Vertical Deviations, Fixation Disparity
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
hyper
Vertical phorias are generally described in reference to the (hyper or hypo) eye. Vertical phorias tend to be VERY SYMPTOMATIC
cover test
Because vertical phorias tend to be very small, ____ is not the ideal test to perform in order to detect them
monocular occlusion for 24 hours
If a vertical phoria is suspected but not detected, _____ and reassessment of the phoria can be performed. Cover test is more likely to reveal the phoria due to long term breakage of fusion. Not a very commonly utilized technique.
Infravergence
fusional vergence compensating for a hyper deviation. Is stimulated with base up
Supravergence
fusional vergence compensating for a hypo deviation. Is stimulated with base down
Increased
increased or decreased vertical vergence ranges suggest a longstanding deviation?
prism, vision therapy
two treatment options for vertical deviations. Treatment is only indicated for symptomatic patients
Associated phoria
the most accurate and readily accepted method of prism correction for vertical deviations
Maddox rod
If associated phoria cannot be determined due to a lack of fixation disparity test, ____ can be used to measure the phoria and can help find a starting point for the amount of prism to prescribe by the amount of prism needed to neutralize the phoria
2 BD OD
(6-2)/2 = 2 PD BD OD
Calculate the prism that should be prescribed
prism flip test
The ______ involves 3 PD vertical prism flipped between BU and BD. The direction for which the images are closer is the type of heterophoria. Prism power is then changed until there is equal separation between images.
down, up
If there is a right hyperphoria during the prism flip test, images will be closer with base ____ over the right eye or base _____ over the left
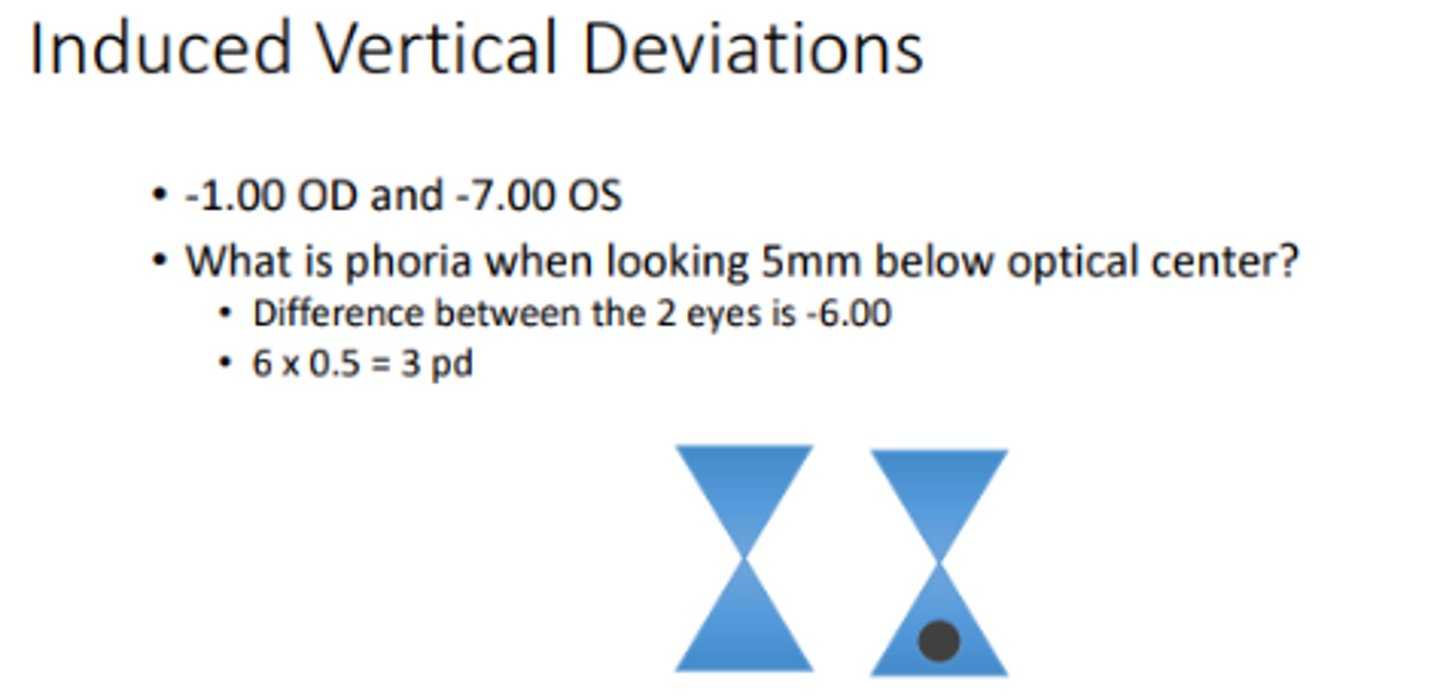
Induced vertical deviations
_____ may occur when there is unequal refractive error between the two eyes and the eyes are pointed downward to read (not in primary gaze). In this case, testing phorias in downward gaze would be helpful to investigate symptoms while reading. I.e) plano OD, +6 OS will appear as a left hyper because it has to move down to track the image after being covered. The right eye will also move down due to yoked muscles, when uncovered it will appear as a hypophoria
slab off prism
Treat induced vertical deviations caused by unequal refractive errors while reading with...
0.752, increases
There is an average of ____ degrees of excyclodeviation at distance that (increases or decreases) with convergence and may produce symptoms at near. Although very uncommon, this can be addressed with a prescription with an alternative astigmatic axis at near.
Fixation disparity
small misalignment of the visual axis occurring between two eyes during binocular viewing. If the magnitude is still within Panum's fusional area then the object of interest will still appear single and a misalignment between the eyes will not be detected with dissociation/phoria testing or cause symptoms
6-10, 0.25
Fixation disparity is usually less than ____ minutes of arc which is less than ____ PD
eso, BO
An overconvergence indicates an ____ fixation disparity which is treated with ____ prism
exo, BI
An underconvergence indicates an ____ fixation disparity which is treated with ____ prism
fast, slow
Initially, ____ fusional vergence responds but dissipates over time due to leaky neural innervation. ____ fusional vergence then takes over in order to maintain the vergence position.
large
Patients having (small or large) fixation disparity tend to be symptomatic and poorly adapt to prism, indicating a defect in the binocular system
small
Patients having (small or large) fixation disparity tend to be asymptomatic and readily adapt to prism, indicating a sufficient binocular system
same direction, larger, fixation disparity
Generally, a patient's disassociated heterophoria should be in the ____ as the patient's fixation disparity, but a ___ magnitude. However, there may be some instances in which this is not true and in this case prescribe the prism that corrects for the ____ (makes more sense to prescribe for the non-dissociated viewing condition because that is how they are normally seeing)
Associated phoria
the amount of prism that is necessary to eliminate fixation disparity during a procedure in which the eyes are associated. Is a good starting point for determining the amount of prism to be prescribed
Bernell fixation disparity (distance)
Mallett fixation disparity (distance and near)
Saladin near point card (near)
3 methods of Measuring Associated Phoria
larger
Patients having strong vergence adaptation will show a ____ magnitude on alternate cover test than unilateral
equal
Patients having poor vergence adaptation will show ___ magnitude on alternate cover test versus unilateral
eso
Placing base in over the eyes will make a patient have a greater ____ fixation disparity. Base in stimulates divergence, but if this does not occur then there is residual convergence error
exo
Placing base out over the eyes will make a patient have a greater ____ fixation disparity. Base out stimulates convergence, but if this does not occur then there is residual divergence error
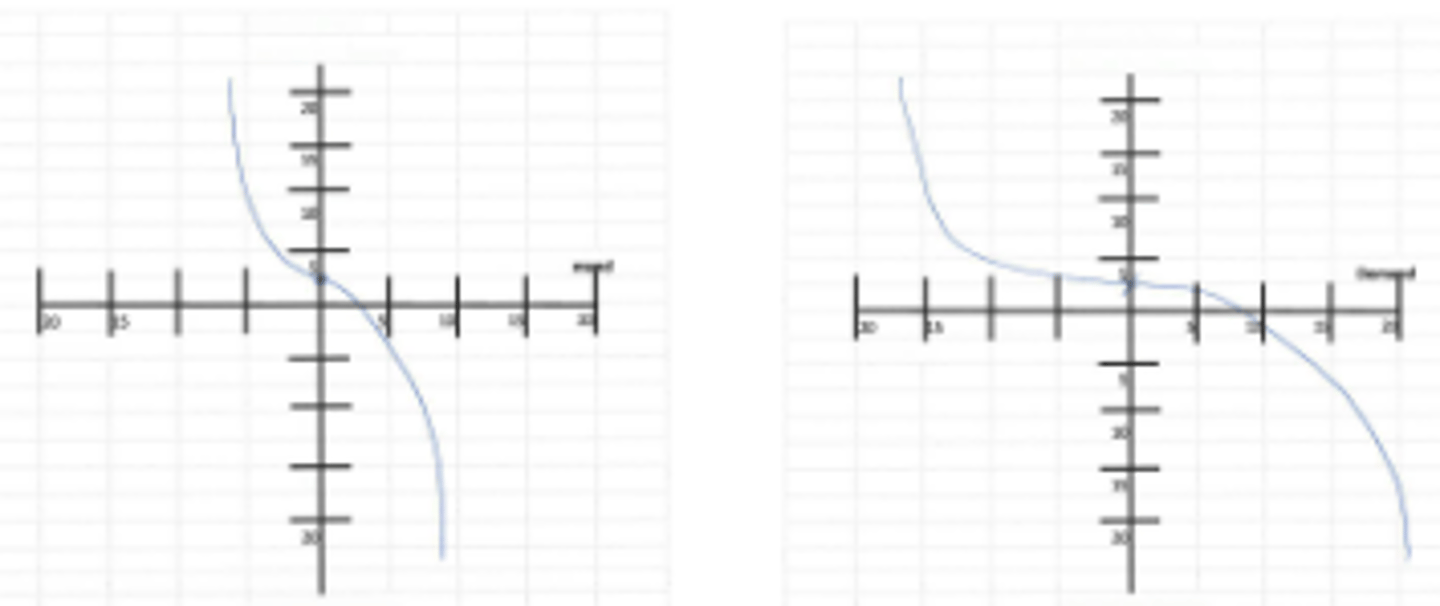
prism demand, fixation disparity
The x-axis on a fixation disparity curve represents the ____, whereas the y-axis represents the resultant ____
y intercept
The fixation disparity with no prism placed in front of the eyes is represented by the ______ on the fixation disparity curve
x intercept
The associated phoria is represented by the _____ on the fixation disparity curve. This is the amount of prism that it took to reduce fixation disparity to zero
better
A flatter slope (<1) on the fixation disparity curve indicates ____ prism adaptation
poorer
A steeper slope (>1) on the fixation disparity curve indicates ____ prism adaptation
prism
Having a center of symmetry (midpoint of the flattest portion of the graph) that is displaced from the y-axis may indicate the need to prescribe...
type I
fixation disparity curve where the slope increases on either side of the y-axis indicating difficulty adapting to both BI and BO. Patient is symptomatic if the slope is steep. Treatment is vision therapy which may flatten the slope or prism based on the center of symmetry or associated phoria
60-70
Type I fixation disparity curves with a flat slope represent ____% of the population. These patients are asymptomatic
type II
fixation disparity curve where the slope is steepest on the BI side of the graph. This indicates a difficulty adapting to BI having greater eso disparity with divergence stimuli. Prescribe prism where the curve begins to flatten over the x-axis on the BO side. Can also prescribe plus lenses at near making the patient less eso
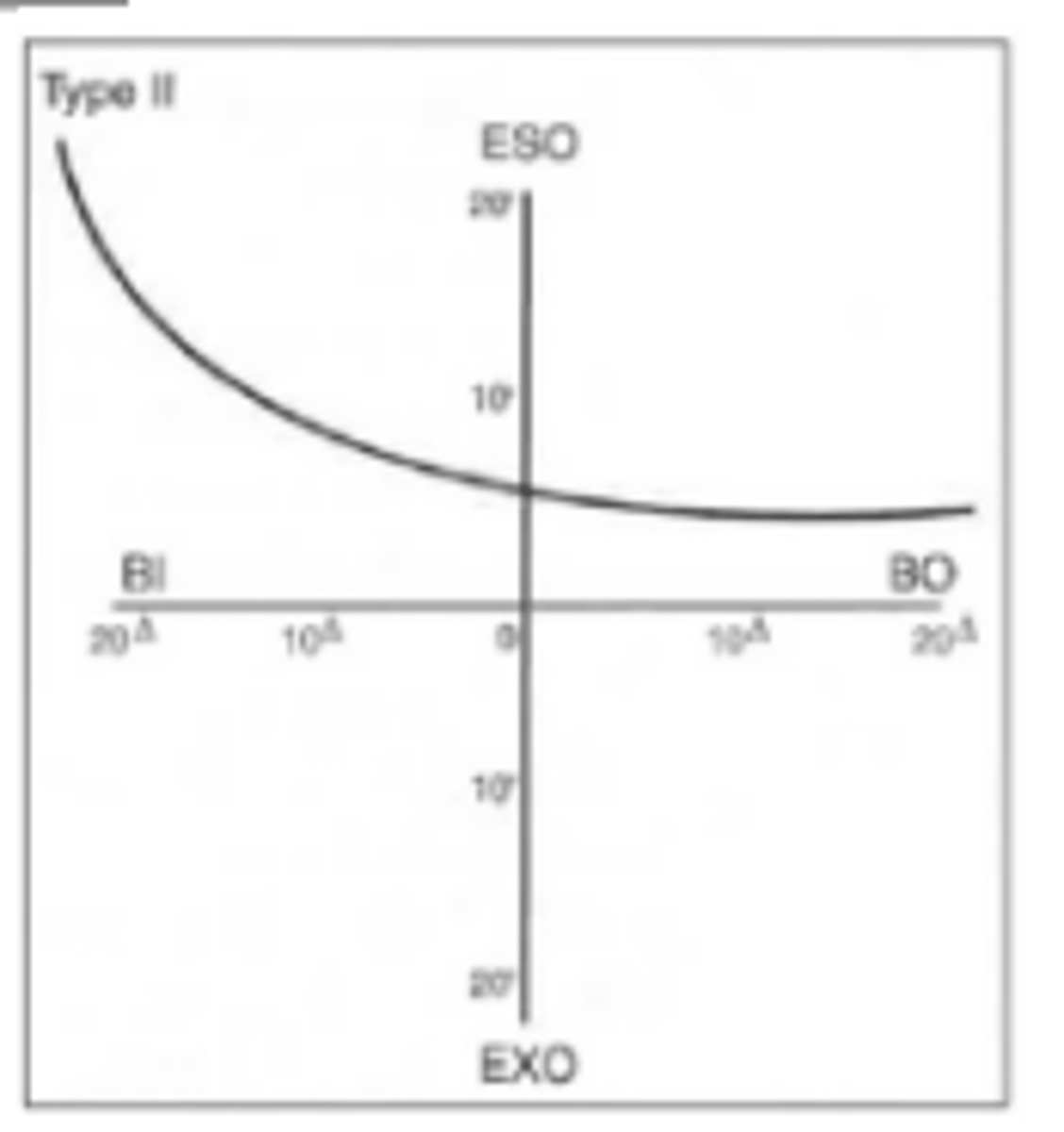
25
Type II fixation disparity curves represent ____% of the population
type III
fixation disparity curve where the slope is steepest on the BO side of the graph. This indicates a difficulty adapting to BO having greater exo disparity with convergence stimuli. Prescribe prism where the curve begins to flatten over the x-axis on the BI side. Can also over minus at distance making the patient less exo
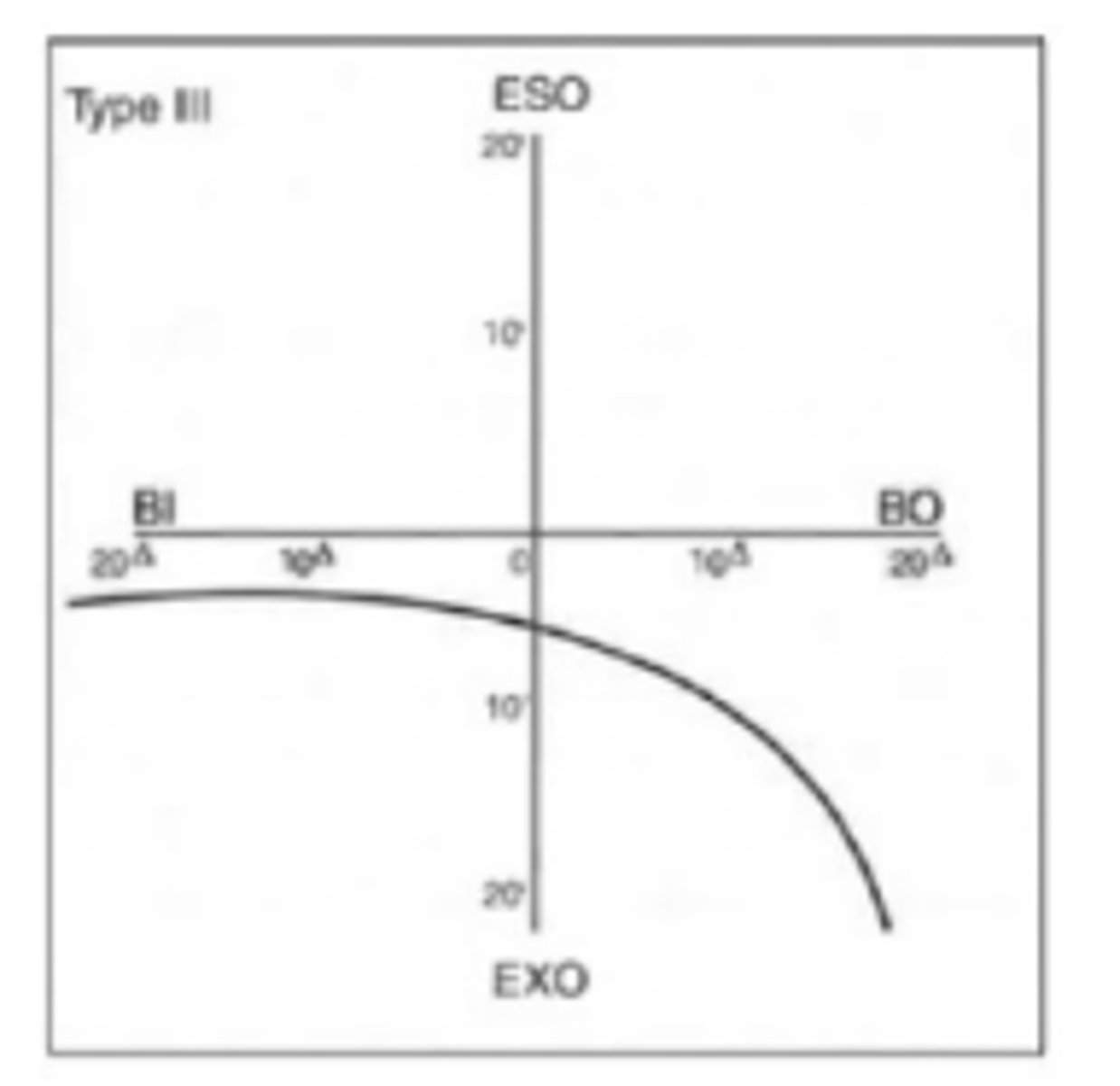
10
Type III fixation disparity curves represent ___% of the population
Type IV
fixation disparity curve where there is relatively constant fixation disparity. Associated phoria may be unstable with no amount of prism neutralizing fixation disparity. Has poor prognosis, vision therapy can be attempted.
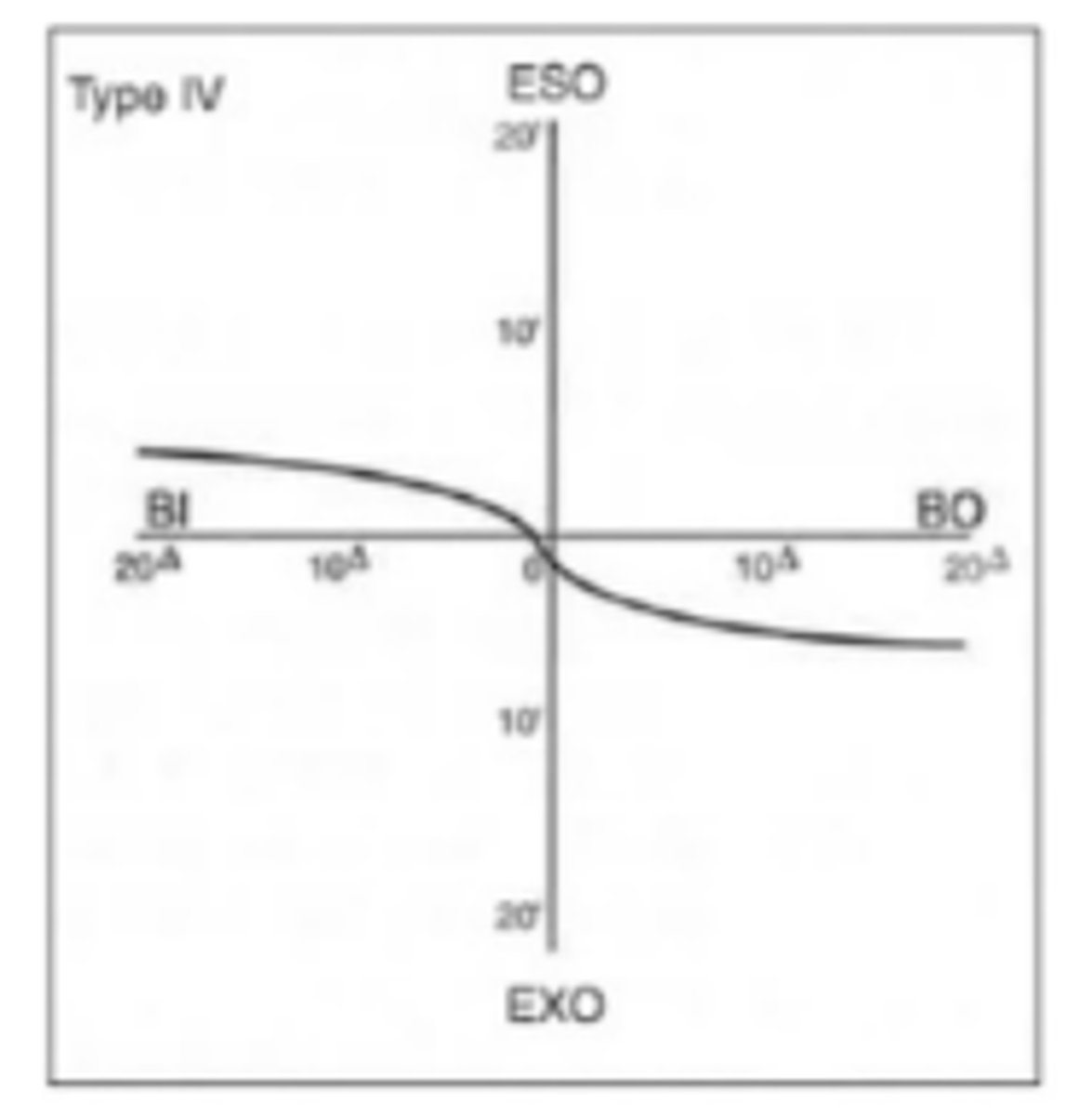
5
Type IV fixation disparity curves represent ___% of the population
accommodative instability
Erratic fixation disparity curves may be due to _____. Vision therapy can be attempted.