High-Risk Labor & Birth
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
Induction Or Augmentation
Stripping the membranes, also called sweeping the membranes, is a common way to induce labor. The provider sweeps a gloved finger between the amniotic sac and the wall of your uterus, separating the fetal membranes from the cervix.
This action is done when the cervix is partially dilated. It may cause the release of prostaglandins, which soften the cervix and may cause contractions.
Labor Induction Carries Various Risks
A multifaceted range of factors has been associated with failed induction of labor comprising maternal factors like primiparity, maternal age, poor bishop score, fetal factors like birth weight and gestational age.
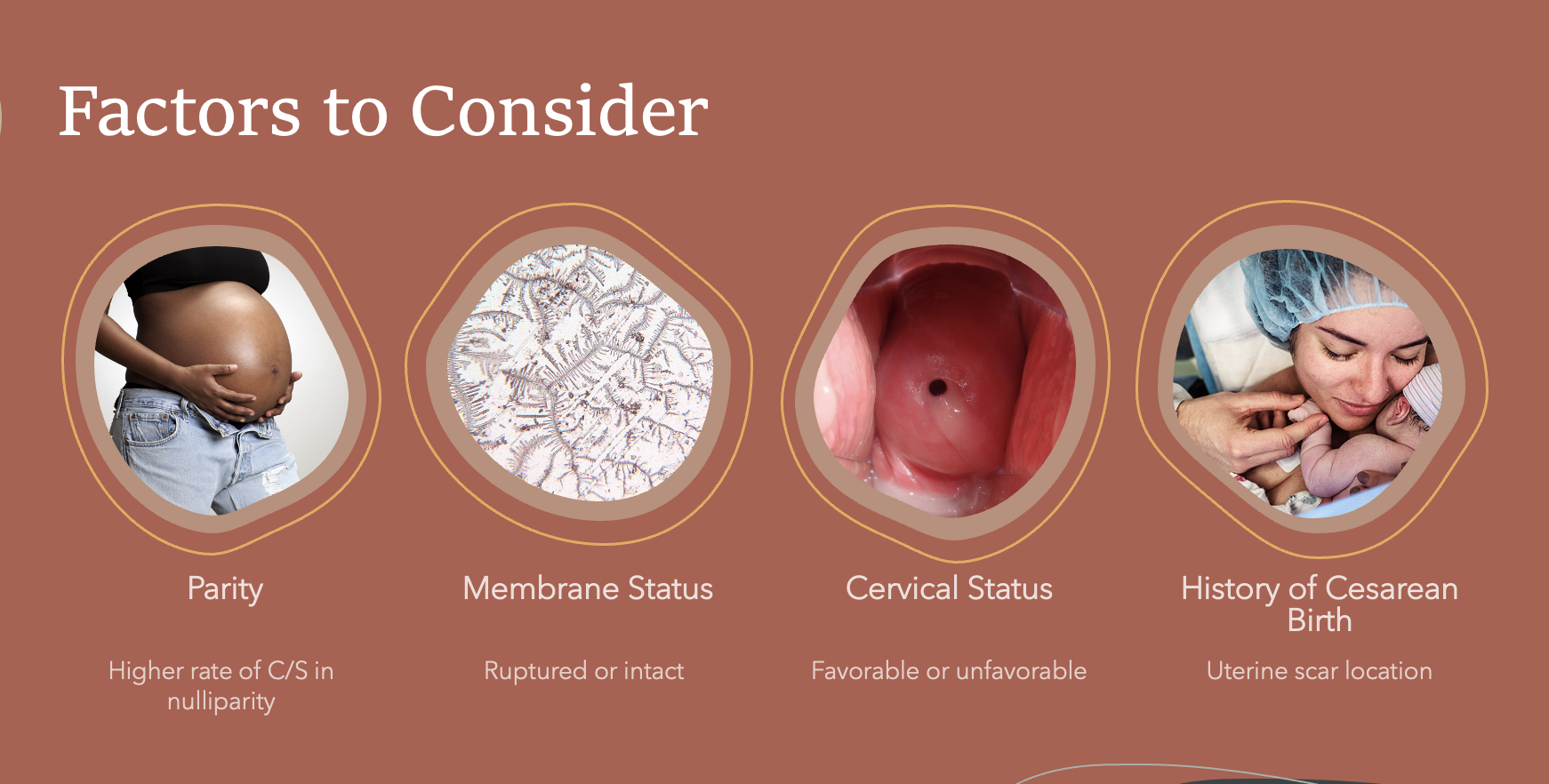
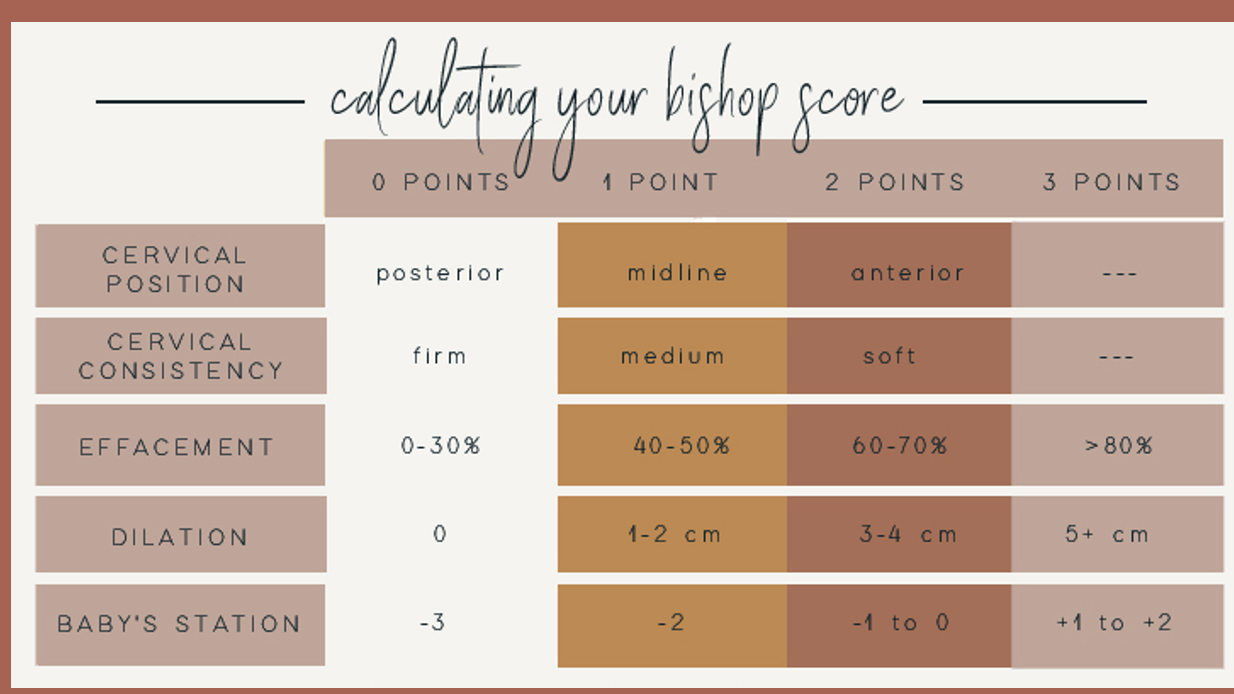
Factors to Consider
A Bishop score of 8 or greater is considered to be favorable for induction, or the chance of a vaginal delivery with induction is similar to spontaneous labor. A score of 6 or less is considered to be unfavorable if an induction is indicated cervical ripening agents may be utilized.
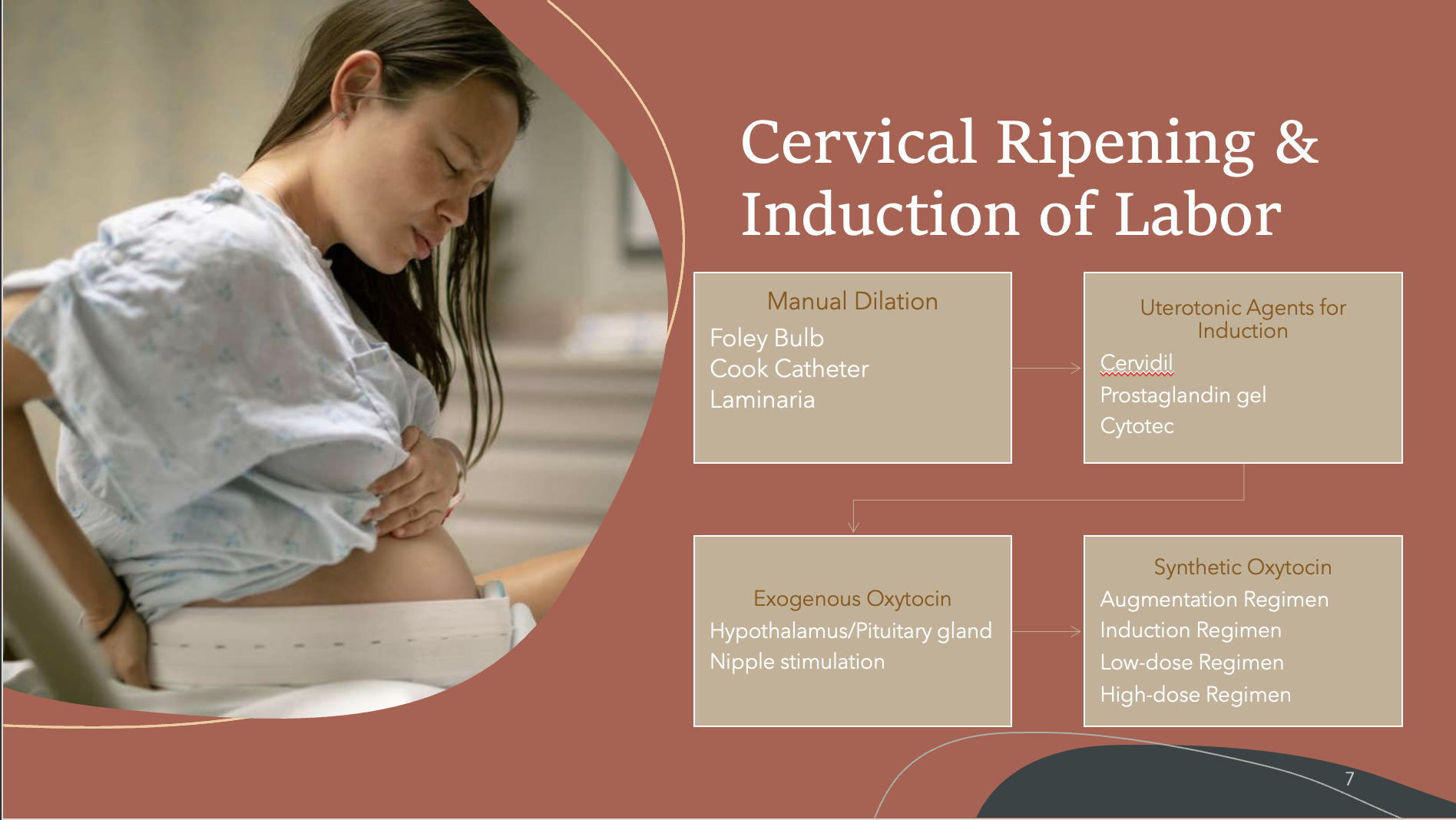
Cervical Ripening & Induction of Labor
Augmentation Protocol
Used to strengthen contractions
Multiparous women
Begin at 0.5 mu/minute, increase to 1 mu Q 30 mins, then up by 2 mu until 5 contractions in 10 minutes
Cannot exceed 30 mu without a physician’s order
Induction Regimen
Used to initiate contractions
Primiparous women
Begin at 1 mu/minute, increase to 1 mu Q30 mins, then up by 2 mu until 5 contractions in 10 minutes.
Cannot exceed 30 mu without a physician’s order
Low-dose Regimen
Used in conjunction with manual dilatation efforts (foley balloon, Cook catheter, laminaria)
Begin fixed infusion at 2 mu/minute
The high-dose oxytocin regimen group will receive a starting oxytocin regimen concentration rate of 6 milliunits/minute that can be increased at increments of 6 milliunits/minute, as per the discretion of their obstetric provider.
Synthetic Oxytocin (Pitocin) Induction
Contraindications
Previous c/section with vertical incision on uterus
History of uterine rupture
Placenta previa of ANY kind
Non-reassuring fetal heart tones (NRFHT’s)
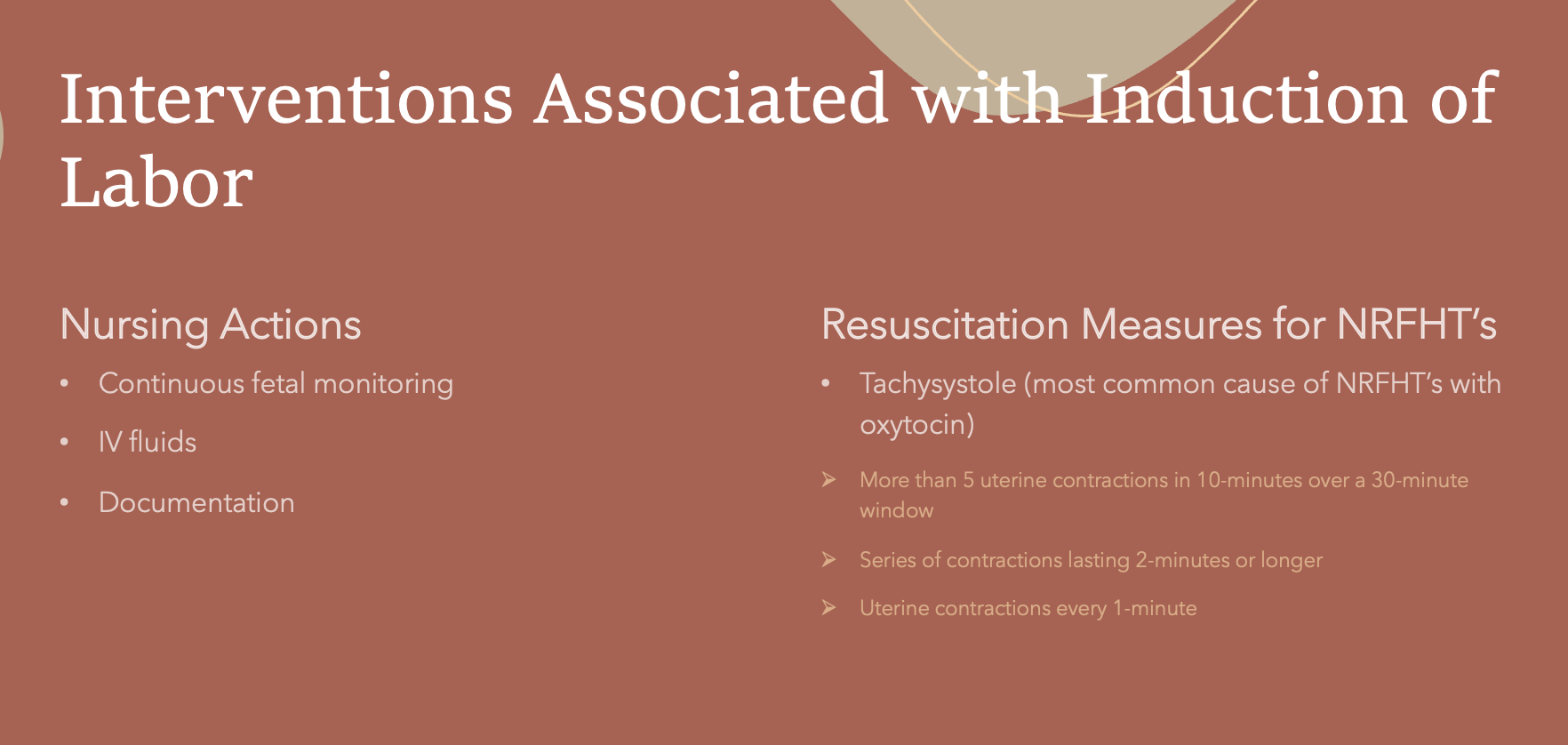
Interventions Associated with Induction of Labor
All patients presenting to Labor and Delivery units at viability should undergo an initial period of electronic fetal monitoring for a minimum of 20 minutes or until fetal well being is assured.
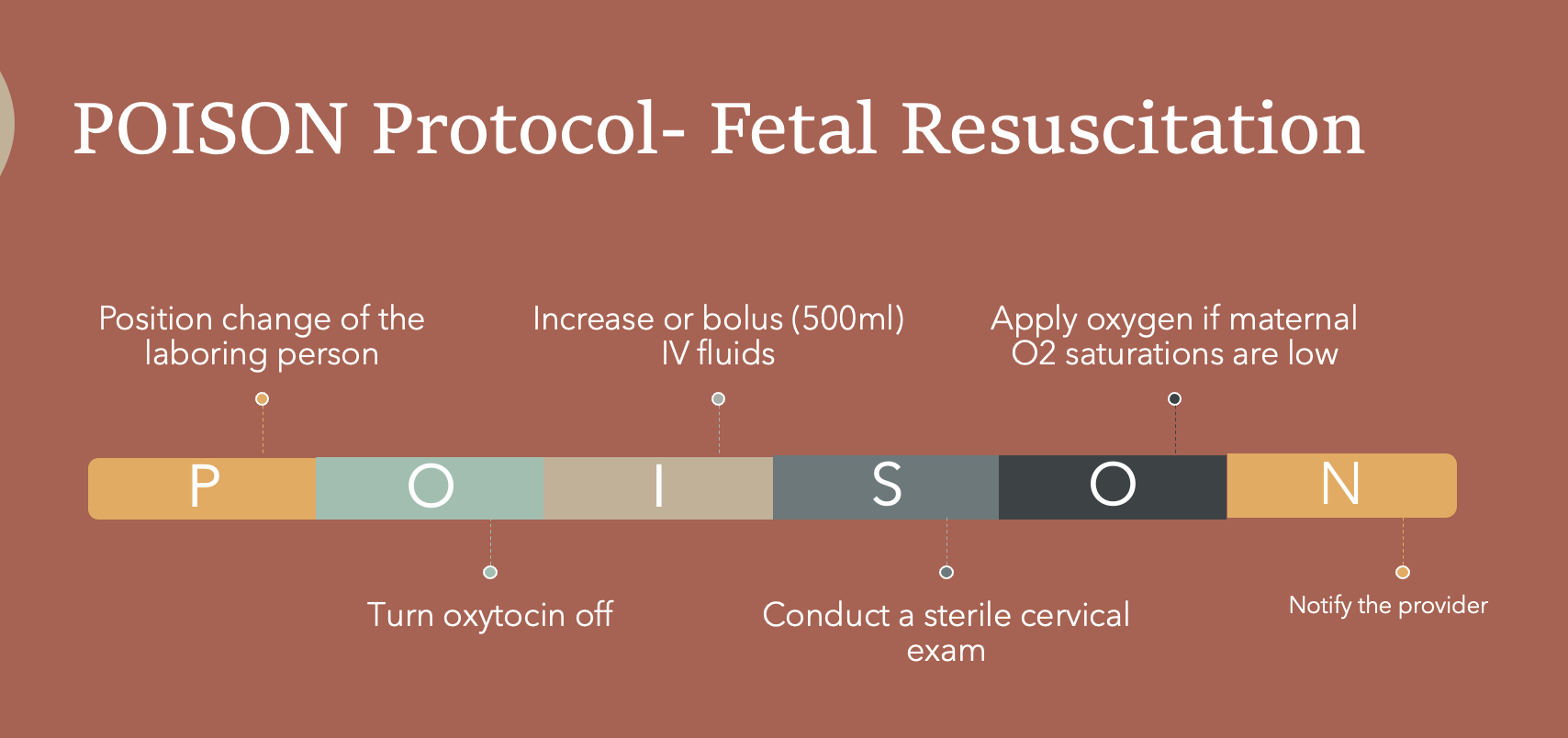
POISON Protocol- Fetal Resuscitation
Complementary Therapies for Labor Stimulation
The action of sexual intercourse in stimulating labor is unclear, it may in part be due to the physical stimulation of the lower uterine segment, or endogenous release of oxytocin resulting from an orgasm or from the direct action of prostaglandins in the semen.

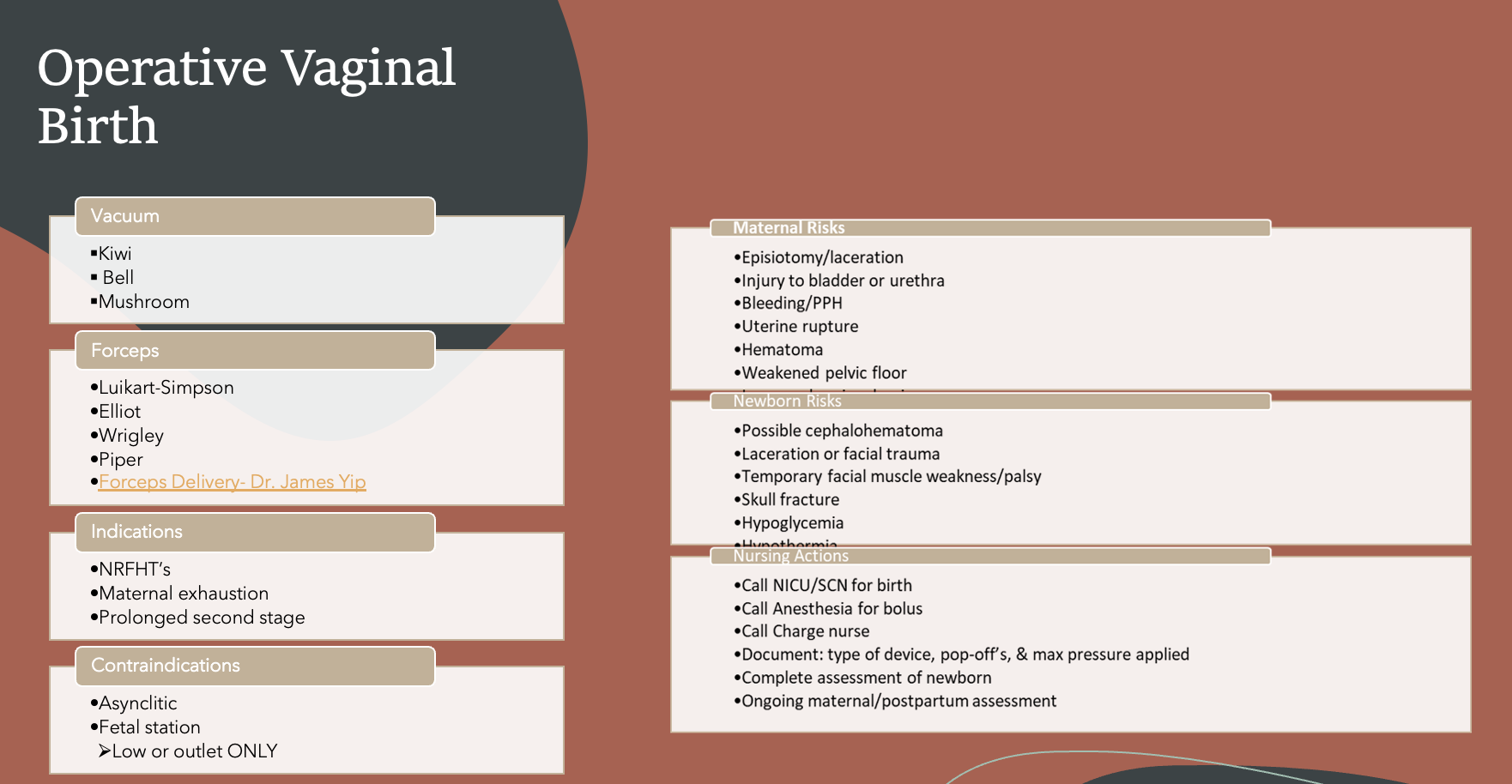
Operative Vaginal Birth
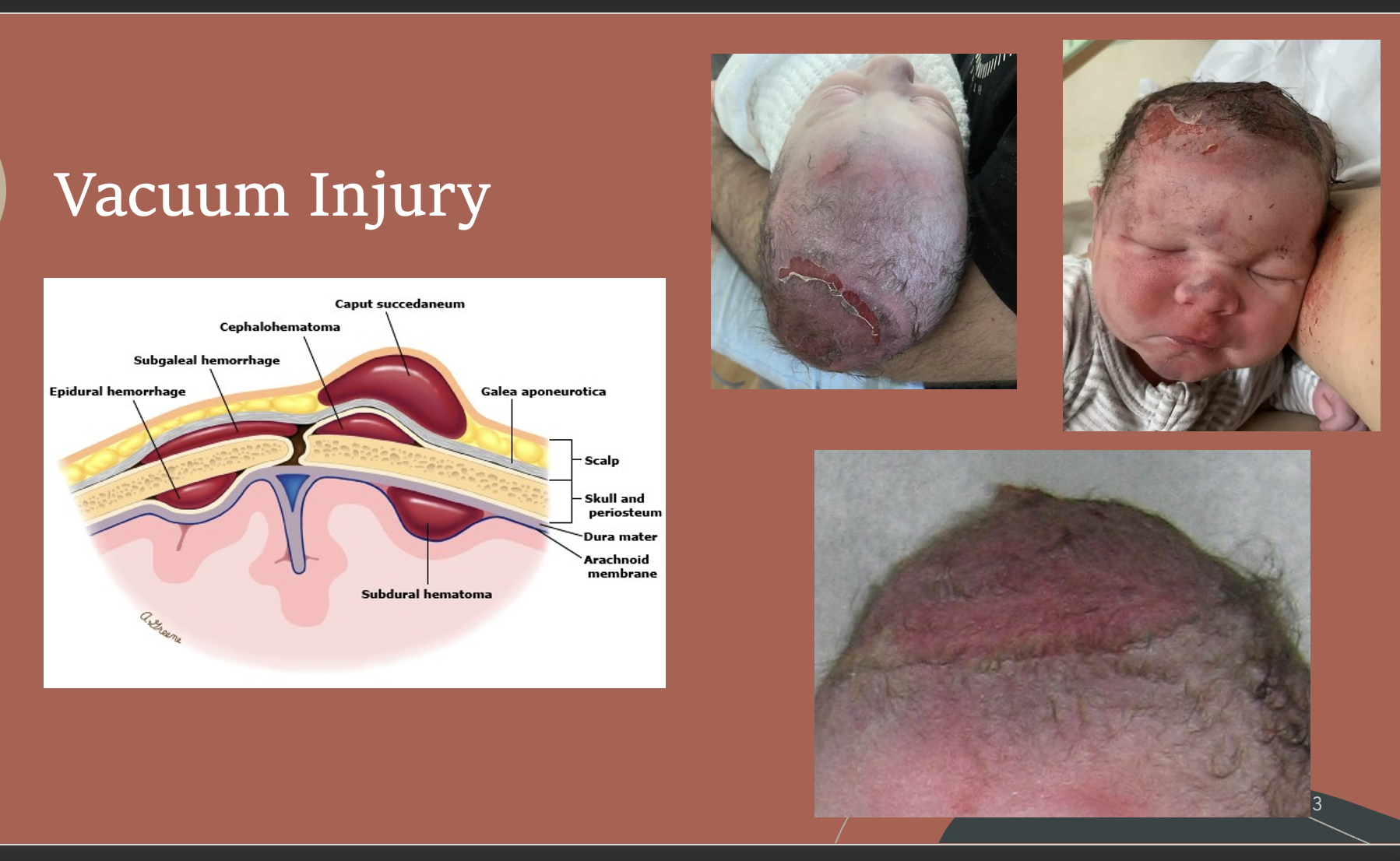
Vacuum Injury
Forceps Injury

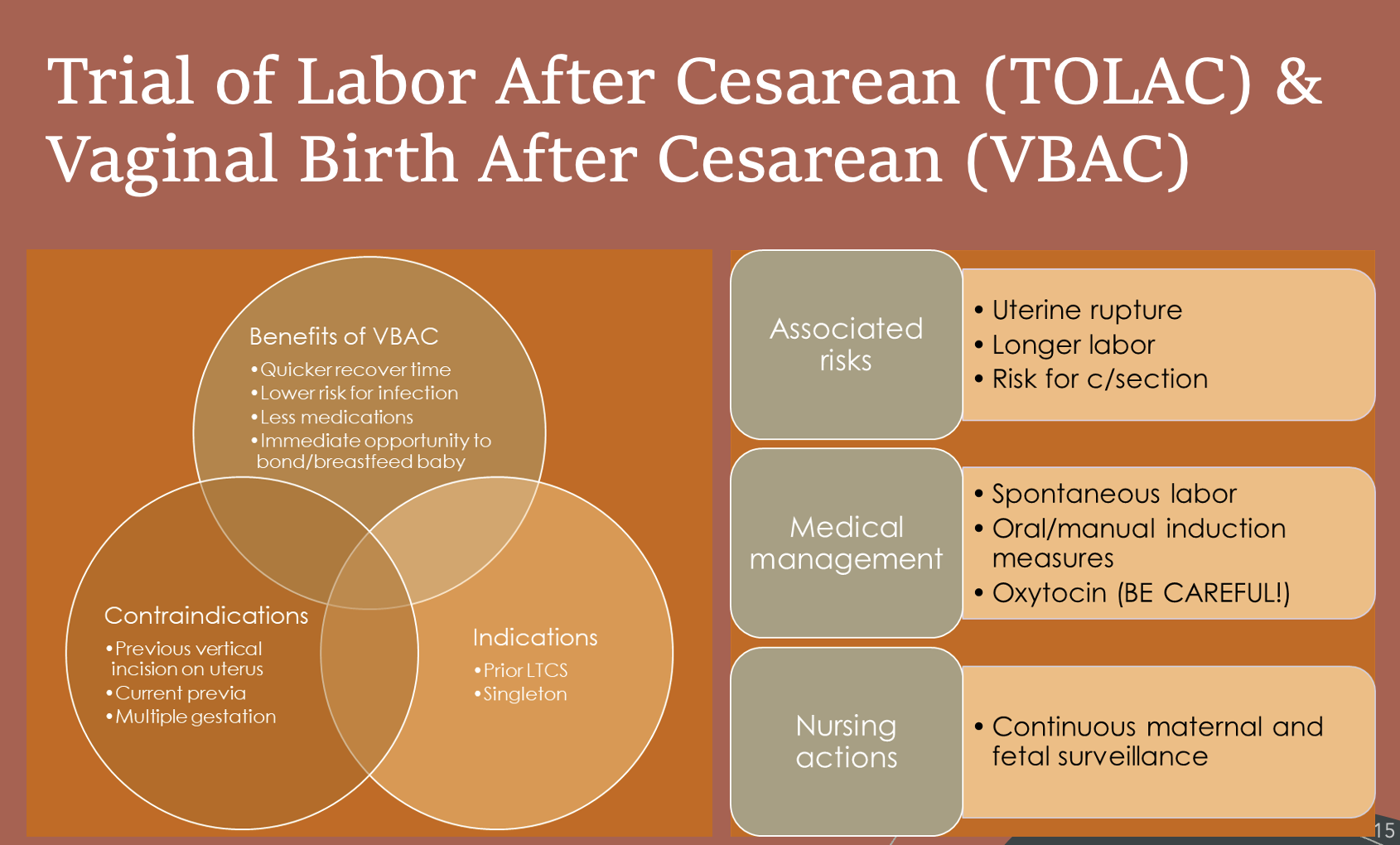
Trial of Labor After Cesarean (TOLAC) & Vaginal Birth After Cesarean (VBAC)
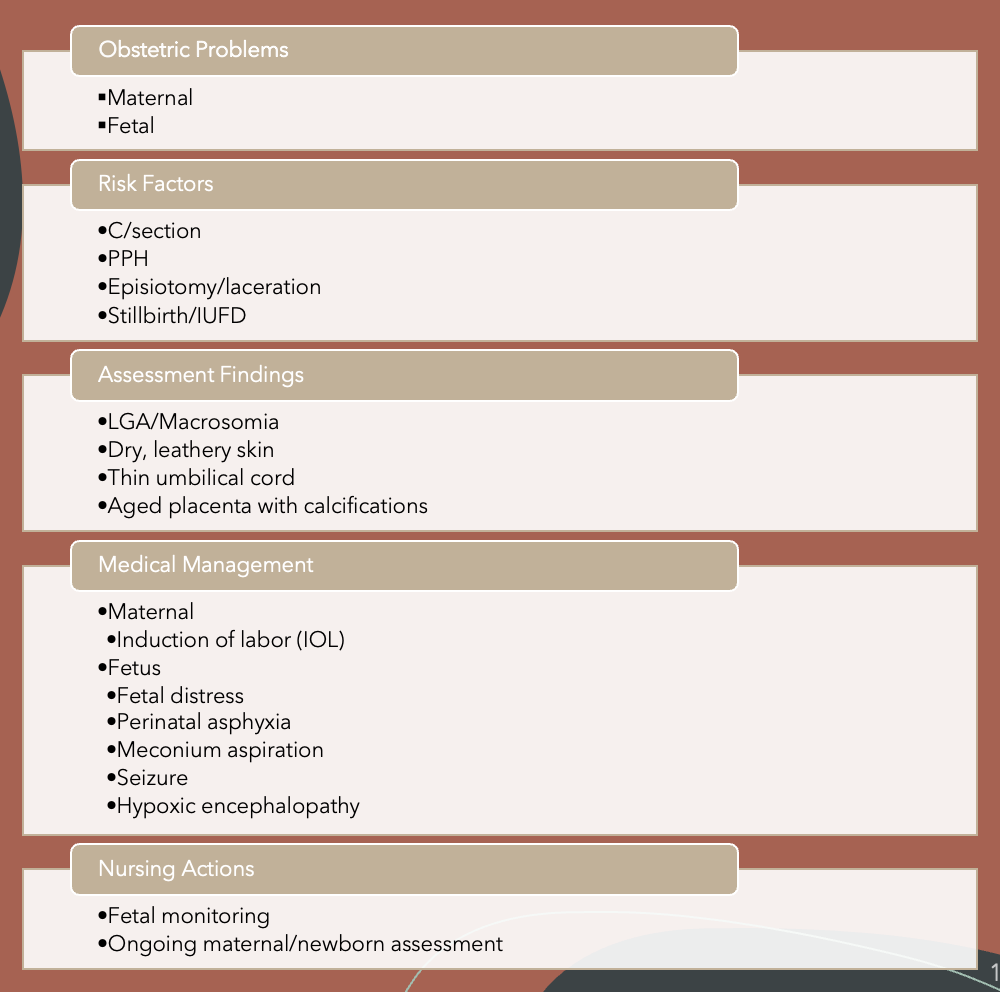
Post-Term Pregnancy (beyond 42 weeks)
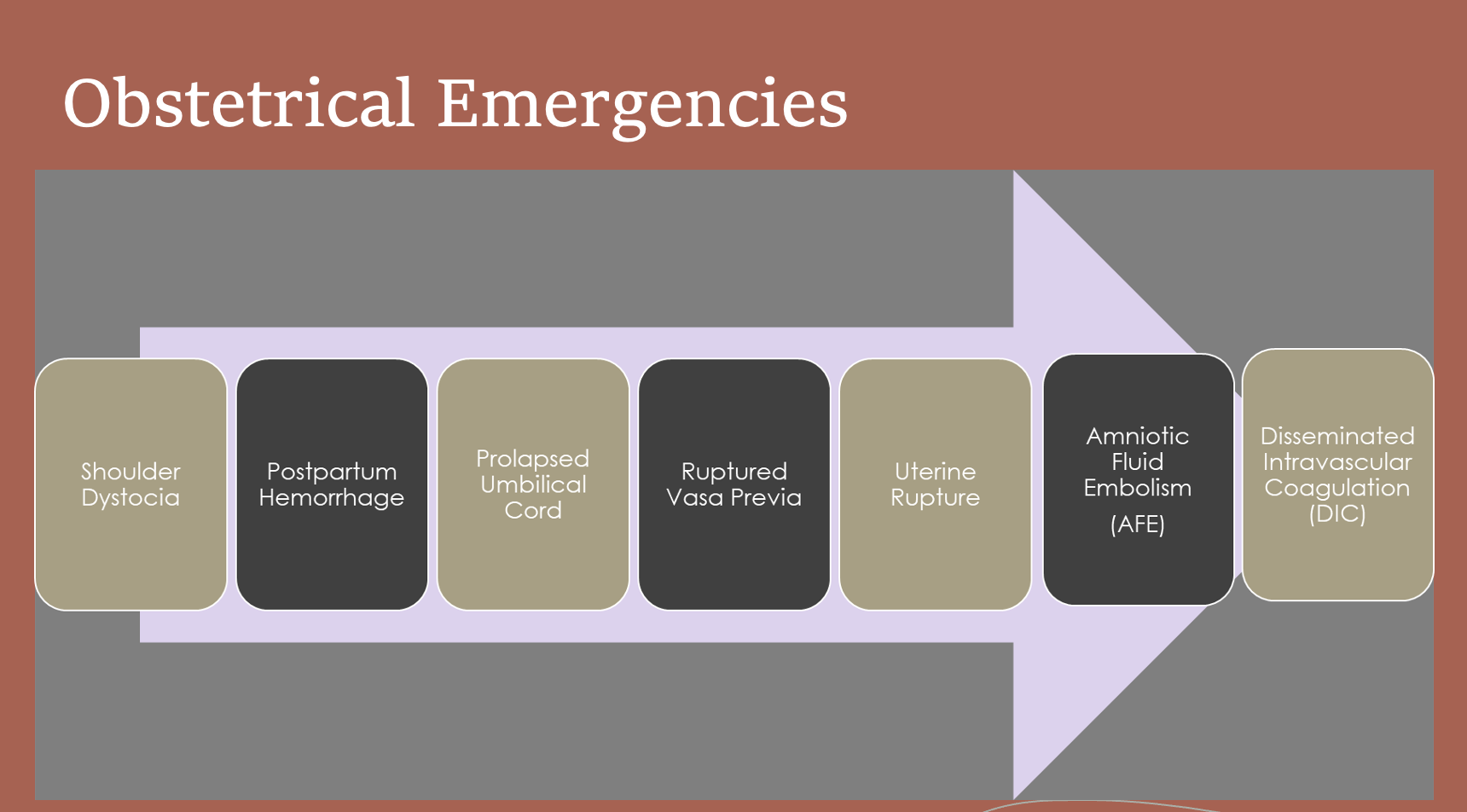
Obstetrical Emergencies
Amniotic Fluid Embolism (AFE) or Anaphylactic Syndrome of Pregnancy is one of the catastrophic complications of pregnancy in which amniotic fluid, fetal cells, hair, or other debris enters into the maternal pulmonary circulation, causing cardiovascular collapse.
Anaphylactic reaction
Etiology largely remains unknown, but may occur in healthy people:
during labor
during cesarean section
after abnormal vaginal delivery
or during the second trimester of pregnancy
may also occur up to 48 hours post-delivery
during an abortion
after abdominal trauma
during amnio-infusion
The pathophysiology of AFE is not completely understood, but providers believe it can stem from a breakdown in the placental barrier. The maternal prognosis after amniotic fluid embolism is very poor though infant survival rate is around 70%.
Symptoms include:
Difficulty breathing
Chest pain
Tachycardia
Hypotension
Hypoxemia
Confusion
Agitation
Seizures
Coagulopathy
Organ failure
Acute pulmonary hypertension
Encephalopathy
The goal is to treat the underlying cause and provide supportive care through intravenous fluids and blood transfusions.
A-OK
(to prevent pulmonary hypertension, systemic hypotension, and decrease coagulopathy)
Atropine 1 mg (vagolysis)
Ondansetron 8 mg (to block serotonin receptors and for vagolysis)
Ketorolac 30 mg (to block thromboxane production) use off label
Some authors have suggested the ventricular dysfunction is secondary to either pulmonary hypertension caused by serotonin and thromboxane or systemic hypotension caused by vagal stimulation. Atropine and Ondansetron may act to block serotonin and vagal stimulation improving cardiovascular function rather than simply providing cardiovascular support. Additionally, the A-OK regimen rather than replacing the consumed factors blocks the proposed cause of coagulopathy by inhibiting thromboxane with Ketorolac
Type 1- Vasa previa with velamentous cord insertion.
Type 2- Vasa previa with vessels connecting lobes of a bilobed or succenturiate placenta.
Intrauterine Fetal Death (IUFD)