Foundations - Chapter 55 - Care of the Patient with an Immune Disorder + Practice NCLEX Questions (with Rationales)
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
What is Immunology? What is the Immune system? (1967)
Immunology - an evolving science that essentially deals with the body's ability to distinguish self from non-self - the body makes this distinction through a complex network of highly specialized cells & tissues that are collectively called the immune system.
The immune system - AKA "the host defense system" - provides a function to the human body that allows for the survival of the entire system. The body has specialized organs, tissues, and cells working to protect it, and the overriding function of the system is the protection of the body from disease and compromise. The body produces specialized cells that detect and destroy harmful pathogens from the body and remove damaged cells from the body.
The immune system also triggers temperature elevation and mucous production.
The nurse outlines the functions of the immune system as those actions which: (Select all that apply.) A. Prevention of hemorrhage. B. Protection of the body's internal environment. C. Maintenance of hemoglobin level. D. Maintenance of homeostasis by removing damaged cells. E. Destruction of growth of abnormal cells.
B. Protection of the body's internal environment.
D. Maintenance of homeostasis by removing damaged cells.
E. Destruction of growth of abnormal cells.
Rationale - The three main functions of the immune system are to protect the body's internal environment by destroying antigens and pathogens, maintenance of homeostasis by removing damaged cells, and the destruction of abnormal growth in the body.
What is immunocompetence? (1967)
The immune system's ability to mobilize and use its antibodies and other responses to stimulation by an antigen. If the immune system is either too weak or too vigorous, homeostasis is disrupted and the system malfunctions - this is called immunocompetence. With this lack of balance, a number of diseases can develop.
Examples of inappropriate immune responses are in 4 categories:
A. Allergies - caused by hyperactive responses against environmental antigens (medication allergies, dust, mold, pet dander)
B. Immunodeficiency - includes AIDS and therapy-induced immunodeficiency from treatments such as chemotherapy and immunosuppressant medications given to prevent a reaction to organ transplantation. Some are born with immune deficiency disorders.
C. Autoimmune disorders - SLE, celiac disease, thyroid disease, inflammatory bowel disease, type-1 diabetes, multiple sclerosis, myasthenia gravis, psoriasis, rheumatoid arthritis, etc.
D. Attacks on beneficial foreign tissue - organ transplant rejection and transfusion reactions.
Which of the following is an example of immunocompetence?
When the symptoms of a common cold disappear in 1 day.
Rationale - Immunocompetence is demonstrated by the immune system responding appropriately to a foreign stimulus and the body's integrity is maintained as with cold symptoms that resolve with residual illness.
Which are autoimmune diseases? (Select all that apply.) A Lupus erythematosus. B. Glomerulonephritis. C. Polio. D. Rheumatoid arthritis. E. Thrombocytopenic purpura. F. Osteoarthritis.
A. Lupus erythematosus.
B. Glomerulonephritis.
D. Rheumatoid arthritis.
E. Thrombocytopenic purpura.
Rationale - Autoimmune diseases such as systemic lupus erythematosus, glomerulonephritis, myasthenia gravis, thrombocytopenic purpura, rheumatoid arthritis, and Guillain-Barré syndrome are treated with plasmapheresis.
A 25-year-old male patient with severe rhinitis asks the nurse what is causing his nose to run. The symptoms are caused by a reaction to a substance, usually a protein, that causes the formation of an antibody and reacts specifically with an antibody called a(n)
Antigen.
Rationale - An antigen is referred to as an allergen (a substance that can produce a hypersensitive reaction in the body but is not necessarily inherently harmful) when symptoms of allergy occur.
What is innate (natural) immunity? (1968)
The body's first line of defense - providing physical, mechanical, and chemical barriers to invading pathogens and protecting against the external environment. It includes intact skin and mucous membranes, cilia, stomach acid, tears, saliva, sebaceous glands, and secretions and flora of the intestines and vagina.
The first line of defense provides non-specific immunity to the individual. Innate immunity also includes the response of phagocytes, such as neutrophils and macrophages. Phagocytes also migrate through the bloodstream to the tissues for the body's second line of defense against disease. Phagocytes engulf and destroy microorganisms that pass through the skin and mucous membrane barriers, also assisting in the immune response by carrying antigens to the lymphocytes.
The first line of defense is innate (natural) immunity. Which is part of that protective mechanism against the external environment? (Select all that apply.) A. Skin and mucous membranes. B. Lungs. C. Heart. D. Tears and saliva. E. Natural intestinal and vaginal flora. F. Stomach acid.
A. Skin and mucous membranes.
D. Tears and saliva.
E. Natural intestinal and vaginal flora.
F. Stomach acid.
Rationale - The innate system is composed of the skin and mucous membranes, cilia, stomach acid, tears, saliva, sebaceous glands, and secretions and flora of the intestine and vagina. These organs, tissues, and secretions provide biochemical and physical barriers to disease.
What is Adaptive (acquired) immunity? (1969)
If innate/natural immunity fails to prevent invasion or to destroy a foreign pathogen, an adaptive immune response will assist in the battle and is the body's second line of defense against disease. Adaptive immunity provides a specific reaction to each invading antigen and has the unique ability to remember the antigen that caused the attack.
It is composed of highly specialized organs, cells, and tissues, including the thymus gland, the spleen, bone marrow, blood, and lymph. It includes humoral and cell-mediated immunity and the system's specificity results from the production of antibodies in the cells. Antibodies develop naturally after infection, or artificially after vaccinations.
The nurse stresses that when a person produces his own antibodies against a specific antigen, that process of immunity is _____ immunity?
Active acquired.
Rationale - When a person's immune system produces specific antibodies against an antigen, that process is an active acquired immunity.
To provide examples of an active acquired immunity, the nurse uses the example of a person who has acquired immunity from measles because that person has had: (Select all that apply.) A. Chickenpox and mumps. B. Measles. C. An extremely healthy immune system. D. An inoculation against measles. E. Maternal antibodies against measles.
B. Measles.
D. An inoculation against measles.
Rationale - Active or acquired or adaptive immunity occurs from having had a disease or having had an immunization against that specific disease.
What should be known about Lymphocytes and Lymphokines? (1969)
Lymphocytes include T and B cells as well as natural killer (NK) cells - 70-80% of lymphocytes are T cells. Activated T cells release compounds called lymphokines - these attract macrophages to the site of infection/inflammation and prepare them for an attack. T and B cells cooperate to produce antibodies but don't produce the antibodies themselves.
T cells are responsible for cell-mediated immunity, protecting the body against viruses, bacteria, fungi, and parasites. They also provide protection in allografts (tissue transfer between two genetically dissimilar individuals of the same species), and against malignant cells.
B cells - roughly 20-30% of lymphocytes - they trigger the production of antibodies, proliferating in response to a particular antigen (a substance recognized by the body as foreign and that can trigger an immune response). Antigens are usually a protein that causes antibody formation and a reaction specifically with that antibody. B cells migrate to peripheral circulation & tissues and are eventually filtered from the lymph and stored in the lymphoid tissue of the body.
Initial B cell formation doesn't require antigen stimulation or any environmental stimulus - B cell proliferation depends on antigen stimulation. B cells are responsible for humoral immunity, and produce antibodies that protect against bacteria, viruses, and soluble antigens.
What is B-cell proliferation dependent on?
Antigen stimulation.
Rationale - Antigen stimulation is the sole focus of B-cell proliferation.
What is the term for transplantation of tissue between members of the same species?
Allograft.
Rationale - The allograft is the transplantation of tissues between members of the same species, such as a graft for full-thickness burns.
What is the substance released by the T cells that stimulates the lymphocytes to attack an inflammation?
Lymphokine.
Rationale - Lymphokines help attract macrophages to the site of the inflammation.
The nurse has held a unit conference on the specific immune response. Which statement by a colleague indicates an understanding of cell-mediated immune response? "Cell-mediated responses are
The direct attack of T-cell lymphocytes.
Rationale - Cell-mediated immunity (the mechanism of acquired immunity characterized by the dominant role of small T cells) results when T cells are activated by an antigen.
What is Humoral Immunity? (1970)
This is a form of immunity that responds to antigens and is mediated by the B cells. B cells produce antibodies in response to antigen challenge. On first exposure to a given antigen, the primary humoral response is initiated. It's generally slow, compared with subsequent antigen exposures.
When a second exposure occurs, memory B cells quickly respond, regardless of whether the first exposure was to an antigen or to immunization - immunization is the process by which resistance to an infectious disease is induced/increased.
T lymphocytes include T-helper and T-suppressor cells - the helper cells coordinate the immune response by activating phagocytes and other T cells and by stimulating B cells to produce antibodies, while suppressor cells maintain the humoral response at the level appropriate for the stimulus.
The antibodies produced by one's own body are said to provide active immunity and develop as the body defends itself from the presence of an active infection or from immunizations against infection, while temporary/passive immunity is provided by antibodies formed by one person in response to a specific antigen and administered to another person.
Passive immunity occurs as antibodies pass through the placenta or through breast milk, as well as when antivenom is given after a snake bite.
The process of immunity through a controlled exposure to an attenuated organism to stimulate the production of antibodies is?
Immunization.
Rationale - The process of immunity through controlled exposure to an attenuated organism to stimulate the production of antibodies is immunization.
What is humoral immunity based on? (Select all that apply.) A. Production of antibodies by B cells. B. T cells are activated by an antigen. C. The body's response to an antigen. D. Sensitized T cells destroy the antigen. E. Helper T cells activate phagocytosis.
A. Production of antibodies by
B cells.
C. The body's response to an antigen.
E. Helper T cells activate phagocytosis.
Rationale - Both types of immunity are in response to an antigen, In the humoral response helper T cells activate phagocytosis and the production of antibodies by the B cells. B cells are the main player in the humoral response.
The nurse explains that when the patient received tetanus antitoxin with the antibodies in it, the patient received which type of immunity?
Passive artificial.
Rationale - When a person receives an inoculation of antibodies from another source, as with tetanus antitoxin, it is considered a passive artificial immunity.
What is the etiology of autoimmune diseases based on?
B and T cells produce autoantibodies.
Rationale - Autoimmune disorders are failures of the tolerance to "self." B and T cells produce autoantibodies that can cause pathophysiologic tissue damage. Autoimmune disorders may be described as an immune attack on the self and result from the failure to distinguish "self" protein from "foreign" protein.
What is the antigen-antibody reaction? (1970)
The antigen-antibody reaction results in mast cells releasing histamine, which produces the symptoms of allergy. When these symptoms occur, the antigen is referred to as an allergen (a substance that can produce a hypersensitivity reaction in the body but may not be inherently harmful).
When immunity results, the antigen is referred to as an immunogen (an agent/substance capable of provoking an immune response or producing immunity).
Which person is most at risk for a hypersensitivity reaction?
The 84-year-old receiving penicillin for an annually recurring respiratory infection.
Rationale - The 84-year-old with a deteriorated immune system is a prime candidate for a delayed hypersensitivity reaction.
What is the Complement system? (1970)
Immunology dates back to the 19th century when researchers recognized that blood plasma contained a substance necessary to complete the destruction of bacteria. The complement system includes roughly 25 serum enzymatic proteins that interact with one another and with other components of the innate and adaptive arms of the immune system.
Complement enzymes are inactive in plasma and body fluids, normally, but are activated when an antigen and antibody interact.
The nurse takes into consideration that when the antigen and antibody react, the complement system is activated which?
Attracts phagocytes.
Rationale - The complement system is a group of plasma proteins that are dormant until there is an antigen-antibody interaction. The proteins destroy the cell membrane and attract phagocytes.
What are the effects of normal aging on the immune system? (1971)
With advancing age, there is a decline in the immune system. As the body ages, the response to infection slows, and this delay allows for illness to impair the body more easily. This may be responsible for the increased incidence of cancer, infections, and autoimmune disorders seen in older adults.
They are also more susceptible to infections (i.e. flu, pneumonia) from pathogens that they were relatively immunocompetent against earlier in life. Bone marrow is relatively unaffected by increasing age.
The thymus gland is the largest between infancy and preadolescence, gradually being replaced by fat as the body ages.
The thymic output of T-cells diminishes, increasing the differentiation of T cells in peripheral lymphoid structures, consequently leading to an accumulation of memory cells rather than new precursor cells responsive to previously unencountered antigens. Delayed hypersensitivity response is frequently decreased/absent in older adults.
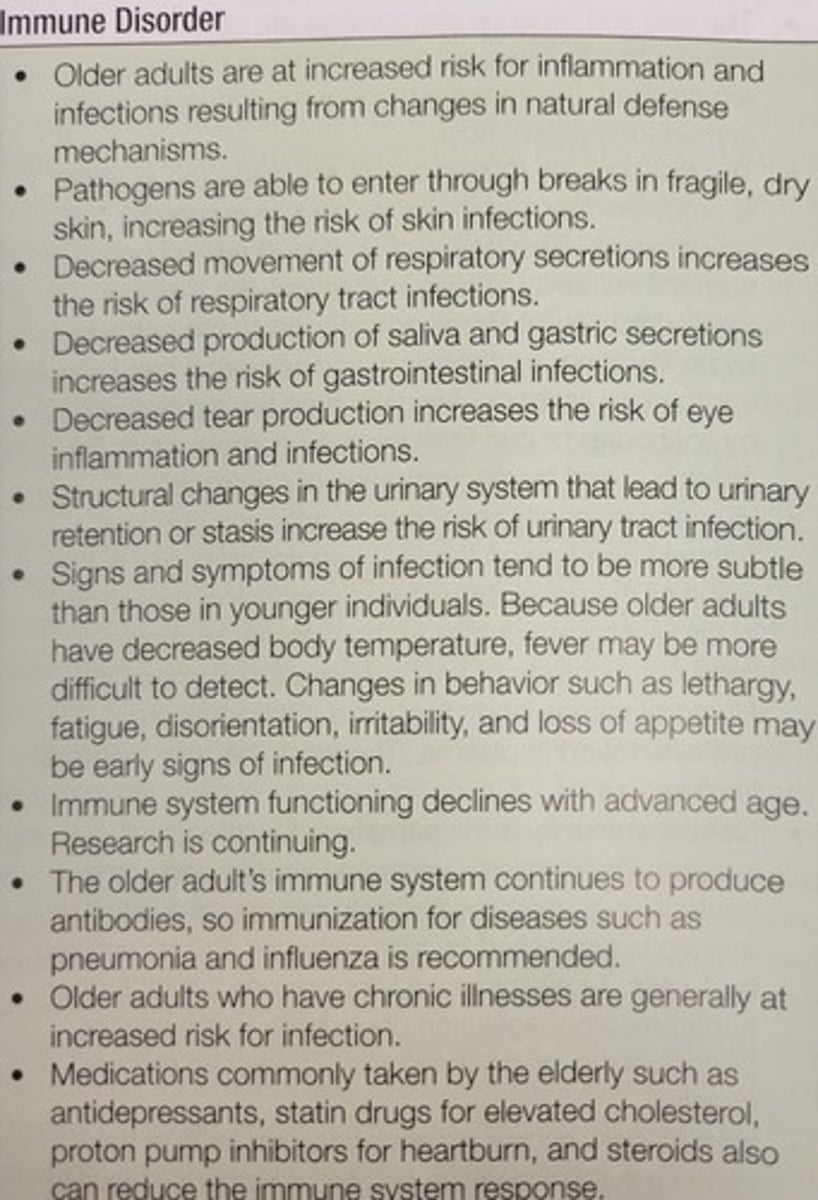
Because the older adult has decreased production of saliva and gastric secretions, they are at risk for?
Gastrointestinal infections.
Rationale - Deficient saliva and gastric secretions make the older adult prone to gastrointestinal infections.
How does normal aging change the immune system?
B cells show deficiencies in activity.
Rationale - Normal aging causes deficiencies in both B and T cell activation, but the bone marrow is essentially uncompromised. The thymus decreases in size.
What are the two ways of helping the body to develop immunity? (1972)
Immunization and immunotherapy.
A. Immunization - the theory behind this is that controlled exposure to a disease-producing pathogen develops antibodies while preventing disease. Vaccines and toxoids are altered, or attenuated (the process of weakening the virulence of a disease organism), to reduce their power without affecting their ability to stimulate the production of antibodies. Immunization allows a greater response from the immune system to a second encounter with an antigen.
Examples: Influenza every year, Td vaccine every 10, Tdap once after age 19, Varicella - two doses if there isn't evidence of immunity to varicella. HPV - for women 19-26 years old. HPV - is recommended for men aged 19-21, and given to men aged 19-26 if having sex with men (unless previously vaccinated). Herpes zoster - two doses for adults 50+. MMR - 2 doses if no evidence of immunity. Hepatitis B - 3 doses if at risk. Meningococcal - 1+ doses if at risk for meningitis.
B. Immunotherapy - AKA Desensitization - a special treatment of allergic responses wherein the patient receives doses of the offending allergens over a 1-3 year period, to develop immunity gradually. A person is injected with a diluted antigen (allergen) to which the person has a type I hypersensitivity. The dilution strength increases weekly until a maintenance dosage is reached. The theory is that immunotherapy assists one to build a tolerance to an allergen without developing fever or increased signs/symptoms.
Immunotherapy may be administered during the allergy season, before allergy season, or year-round (perennial). Perennial therapy is most widely accepted because it allows for a higher cumulative dose, which produces a better effect - this usually begins with a very diluted dose of the allergen, progressively increased weekly over 18+ weeks. Immunotherapy is administered subcutaneously, and the patient should be observed for 20+ minutes after administration as a hypersensitivity reaction or anaphylaxis may occur.
What would the nurse recommend for a 94-year-old home health patient with deteriorated cell-mediated immunity?
Getting pneumonia vaccine.
Rationale - As an older adult loses some of the cell-mediated immunity, especially against pneumonia and influenza, it is recommended that they acquire immunization.
The purpose of immunotherapy is?
Desensitization.
Rationale - The theory behind immunotherapy is to assist the individual to build a tolerance to the allergen without developing fever or increased signs and symptoms. Desensitization is another term used for immunotherapy.
A patient is undergoing immunotherapy on a perennial basis. With this form of treatment, she receives?
Increased amounts and concentrations in 6-week cycles.
Rationale - Perennial therapy is most widely accepted because it allows for a higher cumulative dose, which produces a better effect. Perennial therapy usually begins with 0.05 mL of 1:10,000 dilution and increases to 0.5 mL in a 6-week period.
What precautionary safety measure should the nurse take for a patient who is receiving first-time intradermal injections for allergy testing?
Have the patient remain for 20 minutes after the injection.
Rationale - The patient must always be observed for at least 20 minutes after administration, because hypersensitivity reaction or anaphylaxis may occur.
What should the nurse do because of the increasing strength of the dose in the injections for immunotherapy?
Observe the patient for at least 20 minutes after administration.
Rationale - The patient should be observed for 20 minutes after the increased dose of the allergen. If anaphylaxis is going to occur, it will do so within that time frame.
A patient has experienced an anaphylaxis reaction and is being monitored to ensure she is stable. A nursing diagnosis for her will be?
Decreased cardiac output.
Rationale - In a patient suffering an anaphylaxis reaction, a nursing diagnosis is Decreased cardiac output.
What are the three categories of Immune response disorders? (1973)
1. Hypersensitivity disorder involves an allergic response and tissue rejection. 2. Immunodeficiency disease involves an altered and failed immune response. 3. Autoimmune disease involves extensive tissue damage resulting from an immune system that seemingly reverses its function to one of self-destruction.
This relates to the 4 "R"s of immune response -
1. recognizing self from non-self - the body normally recognizes its own cells and does not produce antibodies to fight those cells, but autoimmune disorders disrupt the ability to differentiate self from non-self, causing the immune system to attack the body's own cells.
2. Respond to non-self invaders - the immune system responds by producing antibodies that target specific antigens for destruction, with new antibodies produced in response to new antigens.
3. Remember the invader - the ability to remember antigens that invaded the body in the past allows a quicker response if subsequent invasion by the same antigen occurs.
4. Regulate its action - self-regulation allows the immune system to monitor itself by "turning on" when an antigen invades and "turning off" when the invasion has been eradicated. The inability to regulate could result in chronic inflammation and damage to the host tissue.
During a patient history, the nurse notices that the patient has had five upper respiratory infections in the past 18 months. The nurse begins to suspect that the patient may have an immunodeficiency disease because the first evidence of this disease is
Increased susceptibility to infection.
Rationale - The first evidence of immunodeficiency disease (an abnormal condition of the immune system in which cellular or humoral immunity is inadequate and resistance to infection is decreased) is an increased susceptibility to infection.
A 72-year-old female patient is admitted with a diagnosis of immunodeficiency disease. The primary nursing goal would be to?
Reduce the risk of her developing an infection.
Rationale: Unusually severe infections with complications or incomplete clearing of infection may also indicate an underlying immunodeficiency.
What is Hypersensitivity? (1973)
Characterized by an excessive reaction to a particular stimulus. A hypersensitivity reaction is an inappropriate and excessive response of the immune system to a sensitizing agent. These disorders arise when harmless substances such as pollens, danders, foods, and chemicals are recognized as foreign. The body mounts an immune response similar to the way it does to any foreign protein.
Chronic exposure leads to chronic allergy response, ranging from mild to incapacitating signs and symptoms. Exposure to antigens may occur by inhalation, ingestion, injection, or touch (contact). It is believed that these disorders are caused by a genetic defect that allows increased immunoglobulin E (IgE) production as well as the release of histamine and other mediators from mast cells and basophils.
The signs/symptoms of histamine release include vasodilation, edema, bronchoconstriction, mucous secretion, and pruritus. Hypersensitivity reactions may be local (GI, skin, respiratory, conjunctival), or systemic (anaphylaxis). Disorders resulting from hypersensitivity include urticaria, angioedema, allergic rhinitis, allergic conjunctivitis (hay fever), atopic dermatitis, and asthma.
How is Hypersensitivity assessed for? (1973)
Subjective signs: pruritus, nausea, uneasiness. Objective signs: sneezing, excessive nasal secretions, lacrimation (flowing of tears), inflamed nasal membranes, skin rash or areas of raised inflammation, diarrhea, cough, wheezes, impaired breathing, and hypotension.
Obtain a detailed history, including the onset/nature/progression of signs and symptoms, aggravating and alleviating factors, and the frequency & duration of signs and symptoms.
Assess environmental, household, and occupational factors. Common offenders include pollen, spores, dust, food, drugs, and insect venom.
More severe signs and symptoms of hypersensitivity include coughing, wheezing, chest discomfort, breathing difficulties, and shock - this could be followed by cardiovascular collapse and respiratory arrest.
When assessing the patient for hypersensitivity, the nurse should?
Discuss seasonal occurrence of signs and symptoms.
Rationale - Common offenders include pollens, spores, dusts, food, drugs, and insect venoms. Many, but not all, offenders are seasonal in nature.
What is the most effective treatment of hypersensitivity disorders? (1974)
Environmental control - this includes avoidance of the offending allergen. Pollens are seasonal and can be avoided at season peaks with air conditioning and limited time spent outdoors. Mold spores can be reduced by maintaining dry conditions and using air filters. Other offending allergens like food, drugs, chemicals, and stinging insects should be avoided if possible.
A patient comes to the clinic for his weekly "allergy shot." He missed his appointment the week before because of a family emergency. Which action by the nurse is appropriate in administering his injection?
Consult with the physician about decreasing the dosage for this injection.
Rationale - Interrupted regimens may place the patient at risk for a reaction.
A patient has a history of allergic reactions to bee stings. Which actions should the nurse teach to avoid an anaphylactic reaction to bee stings?
Take extra precautionary actions when outdoors where bees may be present.
Rationale - teach the patient avoidance of allergens.
A patient who works in a plant nursery and has suffered an allergic reaction to a bee sting is stabilized and prepared for discharge from the clinic. During discussion of prevention and management of further allergic reactions, the nurse identifies a need for additional teaching based on which comment?
"I will need to take maintenance doses of corticosteroids to prevent reactions to further stings."
Rationale - The nurse's responsibilities in patient education are as follows: Teach the patient preparation and administration of epinephrine subcutaneously. There is no need for the patient to take maintenance doses of corticosteroids because this was a short, rapid reaction.
What is Anaphylaxis? (1975)
The most severe IgE-mediated allergic reaction is anaphylaxis, or systemic reaction to allergens. Anaphylaxis, or anaphylactic shock, is an acute and potentially fatal hypersensitivity (allergic) reaction to an allergen.
These allergens include venoms, drugs (penicillin and aspirin, etc), contrast media dyes, insect stings (bees and wasps), foods (eggs, shellfish, peanuts), Latex, and vaccines. This reaction results in sudden severe vasodilation as a consequence of the release of certain chemical mediators from mast cells. An anaphylactic reaction occurs rapidly after exposure, from seconds to a few minutes.
Skin and GI signs/symptoms may occur, although respiratory and cardiovascular signs/symptoms predominate. A fall in blood pressure, laryngeal edema, and bronchospasm can lead to cardiovascular collapse, myocardial infarction, and respiratory failure, which may be fatal. Urticaria, pruritus, and angioedema may be present in mild and moderate anaphylaxis, while cyanosis and pallor may be seen in severe reactions.
Congestion and sneezing to edema of the lips, tongue, and larynx (with stridor and occlusion of the upper airways) are potential upper respiratory signs, while lower respiratory signs occur soon thereafter, including bronchospasm, wheezing, and severe dyspnea.
GI signs include nausea, vomiting, and diarrhea to dysphagia and involuntary stools. The patient may be tachycardic and hypotensive - these may worsen to coronary insufficiency, vascular collapse, dysrhythmias, shock, cardiac arrest, respiratory failure, and death.
Which is a factor that contributes to the extent of an allergic response to an allergen?
The amount of exposure.
Rationale - The five factors influencing hypersensitivity response include host response to allergen, exposure amount, nature of the allergen, route of allergen entry, and repeated exposure.
The correct nursing intervention for anaphylaxis would be?
Assess respiratory status, including dyspnea.
Rationale - Anaphylaxis—If moderate to severe signs and symptoms occur, IV therapy may be initiated to prevent vascular collapse and the patient may be intubated to prevent airway obstruction. Nursing interventions and patient teaching—Assess respiratory status, including dyspnea, wheezing, and decreased breath sounds.
A patient, age 42, develops a severe angioedema involving her face, hands, and feet, with burning and stinging of the lesions. During the assessment, which significant risk factor for allergies does the nurse recognize?
Family history of allergies.
Rationale - A thorough history is the most important diagnostic tool. There is a genetic link to both well-developed immune systems and poorly developed or compromised immune systems.
An anxious patient enters the emergency room with angioedema of the lips and tongue, dyspnea, urticaria, and wheezing after having eaten a peanut butter sandwich. What should be the nurse's first intervention?
Provide oxygen per non-rebreathing mask.
Rationale - Provision of oxygen is the initial primary intervention. Anaphylaxis may advance very rapidly and the patient may have to be intubated. Covering the patient with a warm blanket is not wrong, but not an initial intervention.
A patient comes to the emergency department with dyspnea, wheezing, and urticaria over the arms and face after being stung by a bee. The nurse would begin immediate care for this patient because he or she is having a(n)
Anaphylactic reaction.
Rationale: Fatal reactions are associated with a fall in blood pressure, laryngeal edema, and bronchospasm, leading to cardiovascular collapse, myocardial infarction, and respiratory failure. Early recognition of signs and symptoms and early treatment may prevent severe reactions and even death.
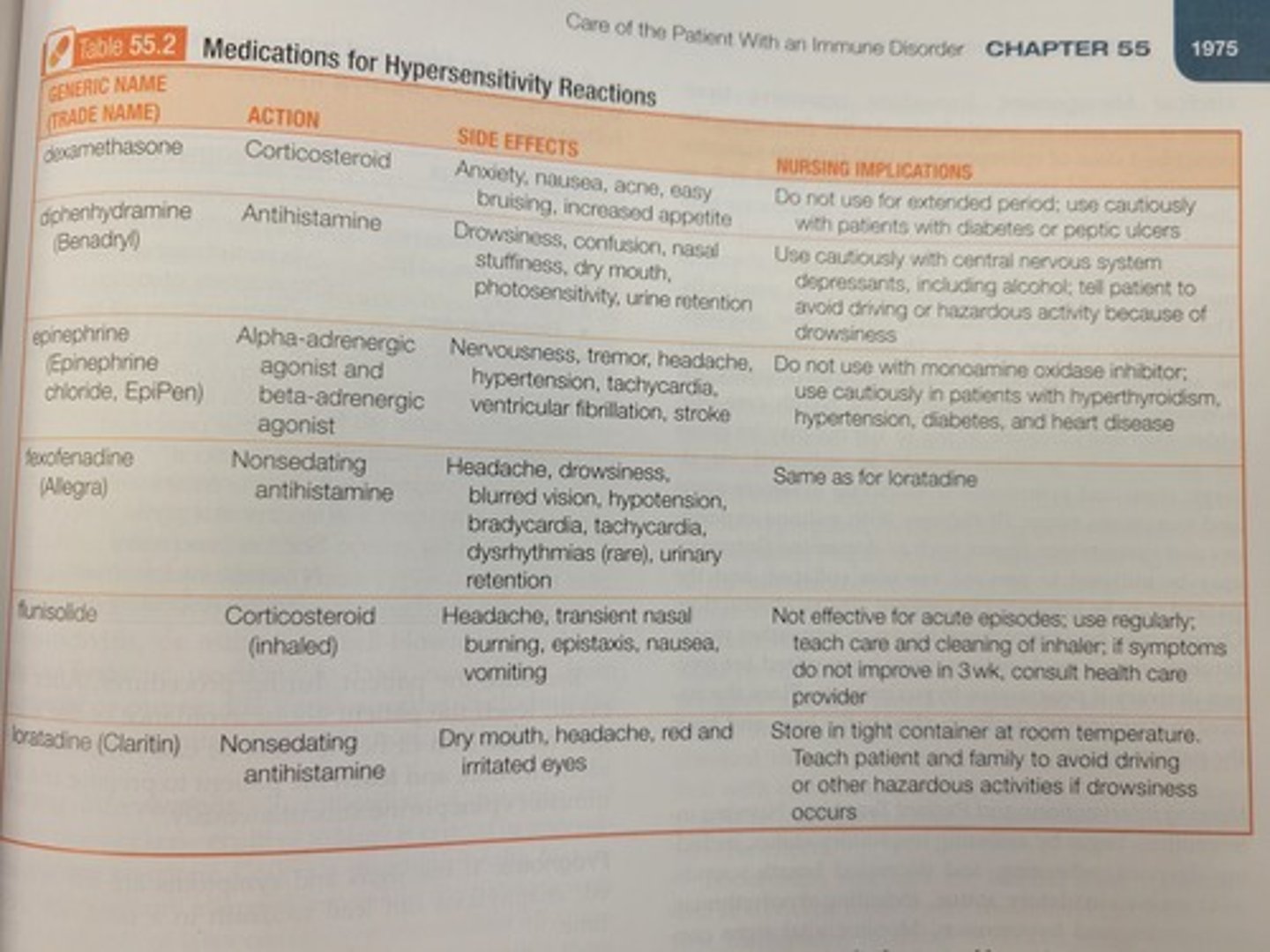
How is Anaphylaxis medically managed? (1976)
Immediate and aggressive treatment is the goal. At the first sign, epinephrine 1:1000 is given subcutaneously for mild symptoms, possibly repeated in 5 to 20-minute intervals.
Epinephrine produces bronchodilation and vasoconstriction, inhibiting the further release of chemical mediators of hypersensitivity reactions from mast cells. Epinephrine 1:10,000 may be given IM or IV for a severe reaction. For allergic signs/symptoms, diphenhydramine 50-100mg may be given IM or IV.
The patient who had an asthma-like reaction to a desensitization shot was medicated with a subcutaneous injection of epinephrine. What effect should the nurse assure the anxious patient this will have?
Produce bronchodilation.
Rationale - The drug epinephrine is given in the case of anaphylaxis because it is a quick-acting drug that produces bronchodilation and vasoconstriction, which relieves respiratory distress. The drug can be ordered to be repeated every 20 minutes. The patient may experience an increase in heart rate.
The nurse recommends to the busy mother of three that the antihistamine fexofenadine (Allegra) would be more beneficial than diphenhydramine (Benadryl) because Allegra:
Does not induce drowsiness.
Immediately after the nurse administers an intradermal injection of a suspected antigen during allergy testing, the patient complains of itching at the site, weakness, and dizziness. Which action by the nurse is most appropriate initially?
Administer subcutaneous epinephrine.
Rationale - Injection of subcutaneous epinephrine should be given at the first sign of an allergy.
After a bee sting, a patient's face becomes edematous and she begins to wheeze. Based on this assessment, the nurse would be prepared to administer:
Epinephrine.
Rationale - At the first sign of a reaction, 0.2 to 0.5 mL of epinephrine 1:1,000 is given subcutaneously.
A patient, age 28, is treated at the clinic with an injection of long-acting penicillin for a streptococcal throat infection. Her history reveals that she has received penicillin before with no allergic responses. When the penicillin injection is administered, which information should be given to the patient by the nurse?
She must wait in the clinic area for 20 minutes before she is discharged.
Rationale - The patient must always be observed for at least 20 minutes after administration, because hypersensitivity reaction or anaphylaxis may occur.
A patient, age 47, is undergoing skin testing with intracutaneous injections on the forearm to identify allergens to which she is sensitive. Immediately after the nurse administers one of the injections, the patient complains of itching at the site, weakness, and dizziness. Which action by the nurse is most appropriate initially?
Give 0.2 to 0.5 mL of epinephrine 1:1,000.
Rationale - At the first sign of a reaction, 0.2 to 0.5 mL of epinephrine 1:1,000 is given subcutaneously.
A patient who has suffered an allergic reaction to a bee sting is stabilized and prepared for discharge from the clinic. During discussion of prevention and management of further allergic reactions, the nurse identifies a need for additional teaching based on which comment?
"I will need to take maintenance doses of corticosteroids to prevent reactions to further stings."
Rationale - The nurse's responsibilities in patient education are as follows: Teach the patient preparation and administration of epinephrine subcutaneously. There is no need for the patient to take maintenance dosages of corticosteroids because this was a short, rapid reaction.
What is important to note about Latex allergies? (1977)
These are an increasing problem - the sharp increase in glove use coincided with an increase in allergic reactions, after OSHA mandated universal bloodborne pathogen precautions and the use of gloves by healthcare workers. 8-12% of healthcare workers regularly exposed are estimated to be sensitized. More frequent and prolonged exposure leads to greater likelihood of developing a latex allergy. Latex proteins can become aerosolized through powder on gloves and can result in serious reactions when inhaled by sensitized individuals.
An allergic reaction to latex may also result in an allergic reaction to some foods - bananas, avocados, kiwi fruit, tomatoes, apples, chestnuts, and melons are common foods to result in an allergy if one is allergic to latex. Two types of latex allergies - type IV allergic contact dermatitis, which is caused by the chemicals used in latex glove manufacturing.
The person typically has dryness, pruritus, fissuring, and cracking of the skin, followed by erythema, edema, and crusting at 24-48 hours. Type I allergic reactions are a response to the natural rubber latex proteins, and occur within minutes of contact with the proteins. These can lead to skin erythema, urticaria, rhinitis, conjunctivitis, or asthma to full-blown anaphylactic shock. Workers with a known latex allergy should wear a medical alert bracelet.
A type IV latex allergy is characterized by?
Contact dermatitis.
Rationale - Type IV latex allergy is that of contact dermatitis, and is a delayed reaction that occurs within 6-48 hours, while type I is a response to the natural rubber latex proteins and occurs within minutes of contact with the proteins.
Health care facilities have reduced the incidence of serious latex reactions by?
Using only powder-free gloves.
Rationale - Powder inside gloves can become aerosolized and cause inhalant reactions.
If a nurse is sensitive to latex gloves, what potential food sensitivities might the nurse develop? (Select all that apply.) A. Peanuts. B. Avocados. C. Milk. D. Bananas. E. Tomatoes. F. Potatoes.
B. Avocados.
D. Bananas.
E. Tomatoes.
F. Potatoes.
Rationale - A person sensitive to latex may also be sensitive to certain foods, including avocados, kiwi, guava, bananas, water chestnuts, hazelnuts, tomatoes, potatoes, peaches, grapes, and apricots.
What are transfusion reactions? (1977)
These are hypersensitivity disorders best illustrated by reactions that occur with mismatched blood. Preventing these reactions requires careful selection of blood donors, followed by careful typing and crossmatching of blood from donor to recipient.
Proper blood storage and adherence to the administration protocol are critical. Blood must be refrigerated at a specific temperature until 30m prior to administration, and it must be administered within 4 hours of removal from refrigeration, and blood components within 6. Donor and recipient numbers are specific and must be thoroughly checked, and the patient must be IDed with an armband. All blood and blood products must be administered through micro-aggregate filters.
Monitor for adverse effects. Reactions can be mild, moderate, and severe. Severe reactions occur within the first 15 minutes, moderate within 30-90, and mild may be late in the transfusion or hours to days afterward.
Mild reactions - dermatitis, diarrhea, fever, chills, urticaria, cough, orthopnea.
Moderate - fever, chills, urticaria, wheezing. With mild/moderate, stop the transfusion continue with saline, and notify the HCP.
Severe reactions - fever, chills, lower back pain, chest tightness, tachycardia, a drop in blood pressure, and blood in the urine. Patients may report a sense of impending doom.
With this reaction, stop the infusion, administer saline to maintain IV access, and send the blood and tubing to the laboratory for immediate testing. Note: an autologous transfusion is the best method for preventing transfusion reactions.
A transfusion using blood from one's own blood is a(n) transfusion, which is the best defense against a transfusion reaction, is?
An autologous transfusion.
Rationale - An autologous transfusion uses blood from one's own body.
Which sign and symptom is a sign of a mild reaction as a result of a blood transfusion?
Urticaria.
Rationale - Mild transfusion reaction signs and symptoms include dermatitis, diarrhea, fever, chills, urticaria, cough, and orthopnea.
Which symptom would be classified as a mild transfusion reaction?
Orthopnea.
Rationale - Mild transfusion reaction signs and symptoms include dermatitis, diarrhea, fever, chills, urticaria, cough, and orthopnea.
The LPN/LVN has arrived at the patient's bedside with a unit of packed cells to be connected to an IV that is infusing. When the RN arrives, what is the first thing the nurses must do?
Do the checks to ensure that the donor and recipient numbers match according to policy.
Rationale - Donor and recipient numbers are specific and must be thoroughly checked and the patient identified with an armband.
The nurse arrives at the bedside of a patient who has had a unit of packed cells infusing in his right arm for 35 minutes. He is complaining of chills, itching, and shortness of breath. The next action for the nurse would be to?
Stop the transfusion and IV administer saline.
Rationale - Mild transfusion reactions signs and symptoms include dermatitis, diarrhea, fever, chills, urticaria, cough, and orthopnea. Treatment includes stopping the transfusion and administering saline.
Once blood is removed from refrigeration, what is the length of time allotted for the blood to be transfused?
4 hours.
Rationale - Blood must be administered within 4 hours of refrigeration, and blood components within 6 hours of refrigeration.
What is transplant rejection? (1978)
Transfer of healthy tissue/organs from a donor to a recipient has been done for many years. The immune system that protects the body from foreign proteins is the same one that's at work in tissue transplant rejection. Medical experts have found a way to control the rejection process.
Autografting - transplantation of tissue from one site to another on the same individual, generally successful as there is a reduced likelihood of rejection.
Allografting - transplantation of tissue between members of the same species, usually used after trauma (i.e. full-thickness burns, reconstructive surgery).
Isografting - transfer of tissue between genetically identical individuals.
- Antigenic determinants on the cells lead to graft rejection via the immune process. Therefore, antigenic determinants in recipient tissue and donor tissue are closely matched if possible before transplantation. Rejection takes several days for vascularization to occur.
Rejection is slowed through the use of chemical agents that interfere with the immune response - corticosteroids, cyclosporine, azathioprine. The administration of these agents is referred to as immunosuppressive therapy - the administration of agents that significantly interfere with the immune system's ability to respond to antigenic stimulation. Infection is a threat to the immunosuppressed patient, so a meticulous aseptic technique is required when caring for these individuals. Prophylactic antibiotic therapy may be advisable, and good skin care is necessary. Bedside visits for staff/family should be limited, and those with infections shouldn't be allowed near the patient.
The transfer of tissue between genetically identical individual (twins) is a(n)?
Isograft.
Rationale - An isograft is the transfer of tissue between genetically identical individuals (twins).
What is the major negative effect of cell-mediated immunity?
Rejection of transplanted tissue.
Rationale - Cell-mediated immunity has the negative effect of rejection of transplanted tissue. Activation of T cells and stimulation of B cells are the positive basis of cell-mediated immunity.
The delayed major process that leads to organ transplant rejection is?
Hypersensitivity.
Rationale - Delayed hypersensitivity reactions occurring 24 to 72 hours after exposure are mediated by T cells accompanied by the release of lymphokines. Tissue transplant rejection is another example.
A patient is recovering from a kidney transplant. He is receiving cyclosporine after surgery. The purpose of this drug is to
Suppress the immune response.
Rationale - Tissue reaction does not occur immediately after transplantation. It takes several days for vascularization to occur. Seven to ten days after the blood supply is adequately established, sensitized lymphocytes appear in sufficient numbers for sloughing to occur at the site. Graft rejection is slowed through the use of chemical agents that interfere with the immune response process.
What are Immunodeficiency Disorders? (1979)
Immunodeficiency is an abnormal condition of the immune system in which cellular or humoral immunity is inadequate and resistance to infection is decreased. The first evidence of this is an increased susceptibility to infection, and the problem can manifest as a recurrent or chronic infection.
Immunodeficiency disorders impair one or more of these immune mechanisms: phagocytosis, humoral response, cell-mediated response, complement response, and/or combined humoral and cell-mediated deficiency.
If immune cells are improperly developed or absent, it is primary, if deficiency is caused by illnesses or treatment it is secondary. Primary disorders are rare and often serious, while secondary are more common and may be less severe.
The basic categories of primary immunodeficiency disorders include phagocytic defects, b cells, t cell deficiency, and combined B and T cell deficiency.
What is important to note about Secondary immunodeficiency disorders? (1979)
Drug-induced immunosuppression is the most common type of secondary immunodeficiency disorder. Immunosuppressive therapy is prescribed for patients to treat a wide variety of chronic diseases, including inflammatory, allergic, hematologic, neoplastic, and autoimmune disorders. Immunosuppressive therapy is also sometimes used to prevent the rejection of a transplanted organ.
Immunosuppression is also a serious side effect of cytotoxic drugs used in cancer chemotherapy. Generalized leukopenia often results, leading to a decreased humoral and cell-mediated response. Secondary infections are common in immunosuppressed patients. Stress may alter the immune response, as well. Hypofunctional immune systems exist in young children and older adults - immunoglobulin levels decrease with age, suppressing the humoral immune response.
Thymic involution (shrinking) occurs with aging, along with decreased T-cells. Malnutrition also alters cell-mediated immune responses.
Radiation destroys lymphocytes either directly or through the depletion of stem cells. As the radiation dose is increased, more bone marrow atrophies, leading to severe pancytopenia and severe immune function suppression. Surgical removal of lymph nodes, thymus, or spleen can suppress the immune response - splenectomy in children is especially dangerous, possibly leading to septicemia. Hodgkin's lymphoma greatly impairs the cell-mediated immune response, possibly leading to death from severe viral or fungal infections.
In which patient should the nurse be most concerned about immunodeficiency disorder?
The patient on long-term radiation therapy for cancer.
Rationale - Radiation destroys lymphocytes and depletes the stem cells. Prolonged radiation depresses the bone marrow.
A cancer patient who has been receiving cytotoxic drugs has been having frequent sinus infections. During planning of his care, the nurse must remember that this frequency of infections is an indication of possible
Drug-induced immunosuppression.
Rationale - Drug-induced immunosuppression is the most common type of secondary immunodeficiency disorder. Immunosuppression is a serious side effect of cytotoxic drugs used in cancer chemotherapy.
A patient is admitted with a secondary immunodeficiency from chemotherapy. The nursing plan of care should include provisions for?
Infection control.
Rationale - Immune-deficient persons are at risk for infection and need to be protected aggressively from contagion.
A liver transplant patient is receiving azathioprine (Imuran). What nursing goal is critical for this patient?
Minimize his risk for infection.
Rationale - Graft rejection is slowed through the use of chemical agents that interfere with the immune response process. Included are corticosteroids, cyclosporine (Neoral, Sandimmune), and azathioprine (Imuran). This chemical therapy is referred to as immunosuppressive (the administration of agents that significantly interfere with the ability of the immune system to respond to antigenic stimulation by inhibition of cellular and humoral immunity) therapy.
What is important to note about Autoimmune disorders? (1979)?
These entail the development of an immune response to one's own tissues - they are failures of tolerance to "self". They may be described as an immune attack on the self and result from the failure to distinguish "self" protein from "foreign" protein.
For an unknown reason, immune cells that are normally unresponsive are activated. Autoimmune diseases tend to cluster, so a given person may have more than one autoimmune disease (i.e. rheumatoid arthritis and Addison's disease).
There is a possible genetic predisposition to autoimmune disease, although the pathophysiology of autoimmune responses is not clearly understood.
Environmental factors - smoking, viral infections, and low vitamin D levels have been found to trigger autoimmune diseases in susceptible people. High salt intake may also be associated with the autoimmune response.
A patient has been admitted with pernicious anemia and has asked the nurse to tell him what type of disorder pernicious anemia is. The nurse tells him that it is an immune disorder that results from failures of the tolerance to one's "self." Responding immunologically to one's own antigens is called a(n)
Autoimmune disorder.
Rationale: Autoimmune disorders are failures of the tolerance to "self." Autoimmune disorders may be described as an immune attack on the self and result from the failure to distinguish "self" protein from "foreign" protein.
What is Plasmapheresis? (1979)
The removal of plasma that contains components causing, or thought to cause, disease. When plasma is removed, it's replaced by substitution fluids such as saline or albumin - thus, the term plasma exchange more accurately describes this procedure. This has been used to treat autoimmune diseases such as SLE, glomerulonephritis, myasthenia gravis, thrombocytopenic purpura, rheumatoid arthritis, and Guillain-Barre syndrome.
The rationale is the removal of pathologic substances present in plasma. Immunosuppressive therapy prevents recovery of IgG production, and plasmapheresis prevents antibody rebound (in which post-treatment autoimmune antibody concentrations exceed their pretreatment level) that often occurs after immunosuppressive therapy.
Plasmapheresis involves the removal of whole blood through a needle inserted in one arm and the circulation of the blood through a cell separator, which divides blood into plasma and its cellular components by centrifugation or membrane filtration. Plasma, platelets, white blood cells, or red blood cells can be separated selectively. The undesirable component is removed, and the remainder is returned to the patient through a vein in the opposite arm. The plasma is generally replaced with: normal saline, lactated Ringer's solution, fresh frozen plasma, plasma protein fractions, or albumin.
When blood is manually removed, only 500 mL may be taken at a time. Apheresis procedures allow for greater than 4 L of plasma to be managed in a 2-3 hour period.
Common complications include hypotension and citrate toxicity. Citrate may cause hypocalcemia, which may manifest as headache, paresthesias, and dizziness.
What should the nurse include to assess for in the plan of care for a patient undergoing plasmapheresis?
Hypotension.
Rationale - Hypotension occurs during plasmapheresis because of the transient volume changes in the blood.
What is the purpose of plasmapheresis in the treatment of rheumatoid arthritis?
To remove pathologic substances present in the plasma.
Rationale - Plasmapheresis is the removal of plasma-containing components causing or thought to cause disease.
A patient with rheumatoid arthritis is scheduled for plasmapheresis. She asks the nurse why they are going to do this procedure. In forming an answer, the nurse must remember that the purpose of plasmapheresis is to?
Remove plasma-containing components that may be causing the disease.
Rationale - Plasmapheresis is the removal of plasma-containing components causing or thought to cause disease.