ARDS & Respiratory Failure
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
acute RR failure (type 1) is
PaO2
can’t get enough O2
what pts or disease process do you see with type 1 RR failure
PNA
acute RR failure type 2 is
PaCO2
can’t get enough of CO2
60-70
what pts or disease process do you see with type 2 RR failure
COPD pts
altered gas exchange on ABG
pH <7.30 (severely acidotic)
paO2 <60 (severely hypoxic)
paCO2 >50 (acidotic)
failure of oxygenation
hypoventilation
intrapulmonary shunting ( perfusion, NO VENTILATION) blood is flowing but no air not reaching alveoli (PNA, ARDS, pulmonary edema)
diffusion defects
decreased barometric pressure
LOW CO (non pulmonary hypoxemia)
LOW Hgb (non pulmonary hypoxemia)
failure of oxygenation
hypercapnia (increased CO2)
r/t —> alveolar hypoventilation, decrease in ventilation and hypoxemia
V/Q mismatch
buildup of CO2 since the lungs aren’t moving air in and out effectively or pt is hypoventilation (breathing too slow)
earliest sign of RR failure
neuro changes !!!!
change in LOC
interventions for acute RR failure
maintain patent airway (always thinks ABC’s)
optimize O2 delivery
minimize O2 demand (keep pt sedated enough, paralytics, keep afebrile and cool)
identify and tx cause
prevent further complications
acute RR failure nursing care
• Maintain patent airway
• monitor respiratory status hourly and prn
• Mechanical ventilation/ VAP prevention
• Suction as needed, monitor lung sounds
• Monitor for pneumothorax (a high PEEP may cause the lungs to collapse)
• Obtain ABGs as prescribed and following each vent change
• Continuous ECG monitoring for changes that may indicate increased hypoxemia
• Vitals hourly (BP, MAP, HR, RR, SPO2, pain)
• Manage nutritional needs
• Provide emotional support to the client and family
what is ARDS
acute respiratory distress syndrome
fluid rushes into the lungs (NO BACTERIA)
which can be r/t SIRS (overwhelming response to trauma, pregnancy, pancreatitis)
ARDS meaning continued
NON CARDIOGENIC PULMONARY EDEMA (fluid is in the lungs from increased pulmonary capillary permeability !!!! usually not from L sided HF
ARDS diagnostic criteria
PaO2/FiO2 ratio is LESS THAN 200
BILATERAL INFILTRATES ( white out on both lungs or ground glass appearance)
ARDS pathophysiology
fluid destroys surfactant in alveoli —> no gas exchange
ARDS kills macrophages !!! often leads to a secondary bacterial infection
insult —> SIRS
release of inflammatory mediators
damage to alveolar capillary membrane
increased capillary permeability
non cardiogenic pulmonary edema
ARDS patho continued
microatelactasis ( no surfactant —> closed alveoli)
decreased compliance (stiff lungs, fill up with fluid)
impaired gas exchange
V/Q mismatch
what type of vent setting will a pt with ARDS need to be on
AC/PC
PRESSURE control
other pressure control settings are
SIMV-P
pressure support
what percentage of O2 can usually cause O2 toxicity
60% in about 48 hrs
causes fibrosis of the lungs and scarring
direct risk factors for ARDS
* gastric aspiration
* diffuse pneumonia
* multi system trauma
fat embolism
near drowning
O2 toxicity
pulmonary contusion
inhalation of toxic gases
INdirect risk factors for ARDS (big insult to the body not r/t bacteria)
• *Septicemia
• *Nonthoracic Trauma
• CABG
• DIC
• Drug overdose
• Eclampsia
• Multiple transfusions
• Pancreatitis
• Leukemia
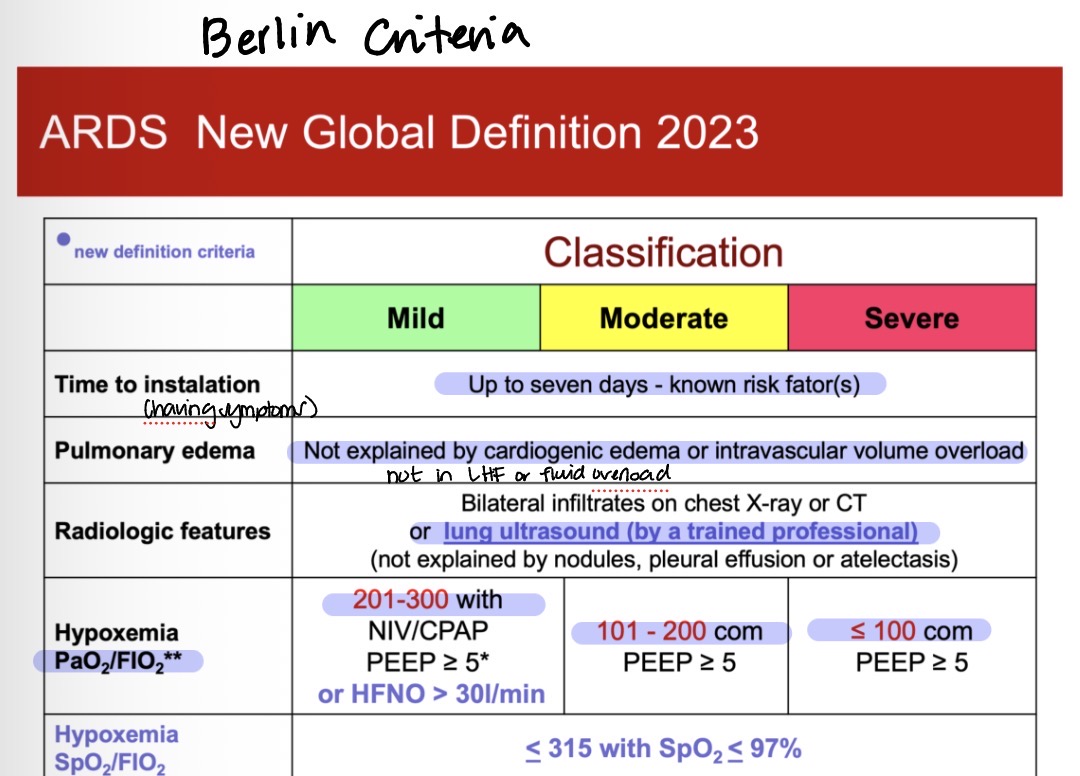
Berlin Criteria is
mild: paO2/FiO2 ratio is 201-300 with PEEP >5
moderate: paO2/FiO2 ratio is 101-200, PEEP >5
severe: <100 paO2/FiO2 ratio, PEEP >5
need to be able to find the PaO2 /FiO2 ratio in order to classify
example” paO2 is 60 and FiO2 is 60 —> make into a decimal
so 60/.60=100 that is SEVERE ARDS
stages of ARDS
insult
acute exudative- SIRS, permeability, leakage, infection
fibroproliferative begins > 24 to 48 hours, fibrosis at 7 days
recovery
early s/s of ARDS
ALTERED LOC
restlessness
refractory hypoxemia (doesn’t get better with supplemental O2)
increased HR and Temp
grunting
normal lung sounds
RR alkolosis from increased WOB
late s/s of ARDS
Severe dyspnea
• increased WOB
• Intercostal retractions
• Accessory muscles
• Pink frothy sputum
• Cough
• Cyanosis
• Increased PIP
• Severe hypoxemia
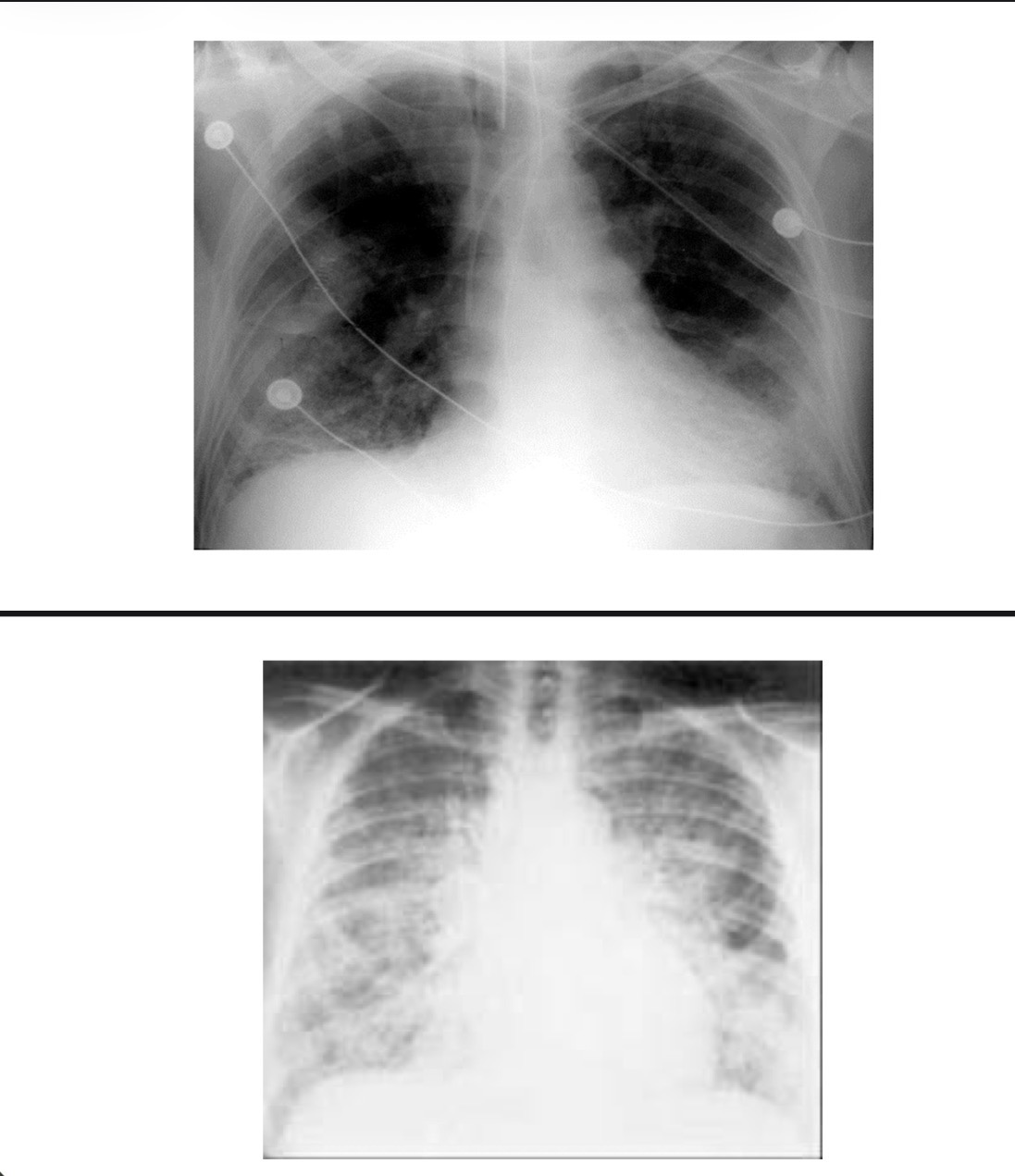
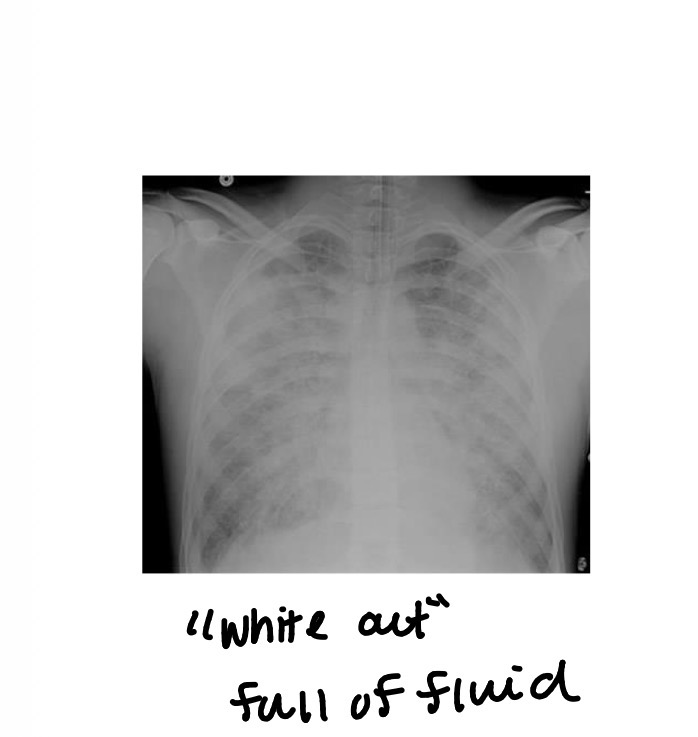
how will the CXR look with ARDS
Interstitial/alveolar infiltrations
• Diffuse, bilateral, symmetrical
• “Ground Glass” or “White-out”
labs for ARDS
• CBC with differential
• Electrolytes
• Sputum culture (r/o)
• Blood culture (r/o)
• Albumin
• Pre-albumin
CXR is best
dont tx with ABX unless secondary infection
ARDS treatment
• Treat the cause
• Oxygenation and ventilation
• Positive end-expiratory pressure (PEEP) (high PEEP can cause Barotrauma and decrease BP)
• Possible nontraditional modes of ventilation: high-frequency, pressure-control, and inverse-ratio
*PRONING helps move fluid around to not obstruct alveoli
treatment goals
• Resolution of hypoxemia
• Normal breathing pattern
• “Normal” ABG’s
• Minimal or no dyspnea
• No complications secondary to treatment therapies evident (can get a pneumo will need chest tube)
oxygenation for ARDS
• Oxygen!!!
• High Flow NC, NIPPV, BiPap, CPAP
• Ventilator
• PEEP
• Low Vt
• Permissive hypercapnia
• Non-traditional modes
• High frequency
• Pressure control
• Inverse I:E ratio
prone position benefits
Alveolar recruitment
• ↑ oxygenation
• Facilitates drainage of secretions
prone position risks
• Loss of airway
• Aspiration
• Corneal injury
• Facial edema
• Impaired skin integrity
pharmacological tx
Diuretics
• Corticosteroids
• Bronchodilators
• Statins
• Antibiotics
• Stress ulcer prophylaxis
• DVT prophylaxis