Heart failure
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
what is heart failure
heart cannot pump blood efficiently
symptoms: breathlessness, ankle swelling, and fatigue that may be accompanied by signs (elevated jugular venous pressure, pulmonary crackles, and peripheral oedema)
It is due to a structural/functional abnormality of the heart → elevated intracardiac pressures/inadequate cardiac output at rest/during exercise
what are the causes of heart failure
arrhrythmias
hypertension
ischaemic heart disease
cardiomyopathy (walls of the heart chambers have become stretched, thickened or stiff)
congenital heart disease
valve disease
viral infection
medicines
cardiac output equation
Cardiac Output (CO) L/min = Stroke Volume X Heart Rate
stroke volume = Volume of blood pumped out of left ventricle
mean arterial pressure (MAP) equation
MAP = CO x TPR
Cardiac output
total peripheral resistance
what is the pathophysiology of heart failure
reduced cardiac output → activation of RAS and SNS → salt and water retention / vasoconstriction / tachycardia / arrhythmias / myocyte changes
body tries to compensate for compromised cardiac output with activation of different neurohormonal pathways
renin-angiotensin system (RAS)
sympathetic nervous system (SNS)
Although this seems logical, the net effect is increased heart workload with increased preload (venous return) and afterload (arterial resistance)
what changes in the heart occur in heart failure
Cellular and extracellular changes
Myocyte loss
Degradation of extracellular matrix
Replacement by fibrosis (scarring)
Changes in size, shape and function
Left ventricular dilation and increased left ventricular wall stress
Change from prolate ellipse to sphere
decreased contractility
what are other neurohormonal and compensatory mechanisms that cause heart failure
vasopressin hormone → vasoconstriction
natriuretic peptide → affect fluid balance
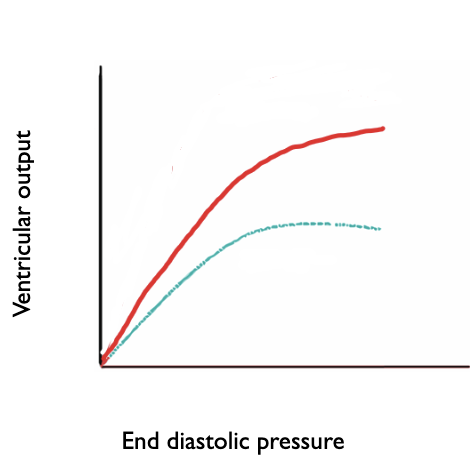
Frank-Starling law mechanism
what is Starling’s law
link between stretching muscle and the force of contraction
Observation that as pre-load increases (more stretching), ventricular output also increases (greater force of contraction)
In heart failure, impaired contractile function means that even higher preload (more stretching) cannot increase ventricular output (force of contraction) to the same extent
how do myocytes lead to arrhythmias and sudden cardiac death
failing myocytes have reduced calcium transients and electrophysiological abnormalities
Reduced size of sarcoplasmic reticulum calcium store (due to reduced expression of sarcoplasmic reticulum Calcium pump)
Upregulated sarcolemmal Na/Ca exchanger
Downregulated Inward Rectifier K+ channel
Prolonged action potential → arrhythmias and sudden cardiac death
• Disruption of the electrical conduction system
how does heart failure progress
Start of heart failure
Compensatory mechanisms
Worsening of HF and development of symptoms
Treatments
Improvement in symptoms
Acute decompensations, some recovery
Gradual decline in quality of life due to worsening symptoms
what is the classification for heart failure
duration → chronic or acute
function → severity of symptoms classed by NYHA Class I–IV or ACC/AHA Stages A–D
side → left: pulmonary symptoms or right: peripheral oedema
direction → forwards: inadequate discharge of blood into arterial system, backwards: inadequate filling of ventricles and discharge of contents, build up of backward pressure
pathophysiology → systolic: impaired ejection or diastolic: impaired filling
ejection fraction: preserved HFpEF or reduced HFrEF
what is ejection fraction
shows how much blood leaves the left ventricle with each heartbeat
expressed as %
normal range is 50-70%
borderline/mildly reduced range is 41-49%
reduced range is less than 40%
estimated using an echocardiogram

what do the different ranges of EF mean
Heart failure reduced EF (<40%)
Ventricles filling with blood but heart not pumping it out very well.
eg.ventricular remodelling/ myocyte damage post ACS, dilation of ventricles
Heart failure with mildly reduced EF (41-49%)
Heart failure preserved EF (50% or more)
Not enough blood coming into the ventricles (despite normal EF)
Eg.Valve issues, poor filling, hypertension, causing hypertrophy HFrEF ((heart failure with reduced ejection fraction) and HFpEF (heart failure with preserved ejection fraction)
what is the NHYA (New York Heart Association) functional classification to asses HF symptom severity
Class I → no symptoms in normal physical activity
Class II → mild symptoms in normal physical activity
Class III → marked symptoms in normal physical activity, asymptomatic at rest only
Class IV → severe symptoms, symptoms even at rest
what are the stage of heart failure according to ACC/AHA
Stage A → at risk of heart failure
Stage B → pre heart failure
Stage C → symptomatic heart failure
Stage D → advanced heart failure
what are the signs and symptoms of heart failure from clinical examination
Raised JVP (Jugular Venous Pressure) → increased elevated right atrial pressure
Tachypnoea → rapid breathing
Hypotension
Tachycardia → fast heart rate
Crepitations on chest auscultation → crackling sounds in lungs
Pallor → paleness
Cachexia → severe weight and muscle loss
Ascites → fluid in abdomen
Peripheral oedema → swelling in legs/ankles
Cyanosis → blueish discolouration of skin/lips
Cold peripheries → cold hands/feet
what are the signs and symptoms of heart failure reported by people
Fatigue
Confusion
Dyspnoea → shortness of breath
Orthopnoea → shortness of breath when lying down that's relieved by standing or sitting up
Paroxysmal nocturnal dyspnoea (PND) → wake up suddenly feeling like you can't catch your breath
Palpitations
Dizziness
Bloatedness/fullness
Weight gain
Reduction in exercise tolerance
Nocturia → frequent weeing at night
how do you diagnose HF according to NICE guidelines
The NT-proBNP (N-terminal pro–B-type natriuretic peptide) blood test is used as an initial screening test for heart failure.
It measures a hormone released when the heart is under stress or strain
NT- pro BNP>2000ng/L → referral for within 2 weeks
NT-pro BNP 400-2000ng/L → referral for within 6 weeks
NT-pro BNP <400ng/L → less likely to be heart failure
what are the aims of treatment
improve mortality
reduce symptoms
reduce time spent in hospital
how can heart failure be managed
Medicines for
HFpEF (Heart Failure with Preserved Ejection Fraction)
HFrEF (Heart Failure with Reduced Ejection Fraction)
HFmrEF (Heart Failure with Mildly Reduced Ejection Fraction)
surgical procedures
Manage any comorbidities or likely causes
what medicines work against compensatory mechanisms
RAS mechanism → ACEI, Angiotensin II Receptor Blockers, Mineralocorticoid Receptor Antagonists
SNS mechanism → beta blockers, ivabradine
Vasoconstriction from vasopressin mechanism → vasodilators such as nitrates
naturetic peptides mechanism → neprolysin inhibitors
Most medicines shown to be beneficial in HFrEF (heart failure with reduced ejection fraction)
Limited medicines with mortality benefit for HFpEF (heart failure with preserved ejection fraction)
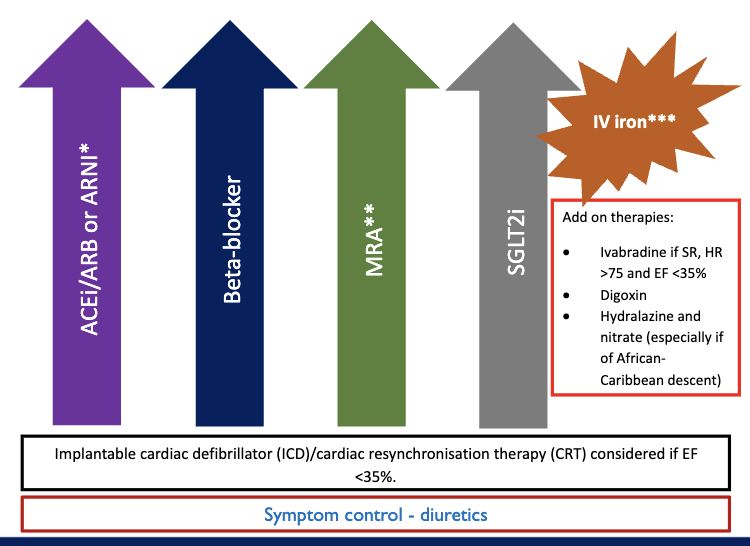
what are the 4 pillar for treatment of Heart Failure with Reduced Ejection Fraction, HFrEF (EF less than 40%)
Angiotensin Receptor-Neprilysin Inhibitors e.g. sacubitril/valsartan considered in symptomatic people despite first line max treatment with reduced EF (<35%)
Mineralocorticoid Receptor Antagonists include eplerenone or spironolactone, but can cause gynaecomastia → consider switch to eplerenone
SGLT2 inhibitors → lower blood glucose by increasing its excretion in urine
IV iron → all HF patients should be regularly screened for anaemia and iron deficiency → given IV iron if appropriate
diuretics → symptom control to remove water → don’t affect mortality
what are lifestyle changes you can change for heart failure
weight management
exercise
cardiac rehabilitation
what are angiotensin converting enzyme inhibitors (ACEIs)
examples: ramipril, analapril, perindopril
mechansim
inhibition of ACE → block conversion of angiotensin I to angiotensin II
Decrease arterial and venous vasoconstriction
Decrease blood volume (no increase in sodium and subsequent water retention from aldosterone)
Decreased compensatory effects of RAAS
effects: trials using enalapril show reduction in CV deaths, worsening HF, reduction in mortality overall
what are Angiotensin receptor blockers (ARBs)
examples: candesartan, valsartan, irbesartan
mechanism
Angiotensin 2 receptor antagonist → blocking the effect of angiotensin II
Decrease arterial and venous vasoconstriction
Decrease blood volume (no increase in sodium and subsequent water retention from aldosterone)
Decrease compensatory effects of RAAS
effects: trials using candesartan and vaslartan showed most benefit seen when taken without an ACEI and more side effects when with ACEI
what are Angiotensin receptor neprilysin inhibitor (ARNI)
examples: sacubitril and valsartan
mechanism of sacubitril
eprilysin breaks down natriuretic peptides
Sacubitril prevents breakdown of natriuretic peptides → increased vasodilation, natriuresis and diuresis
what are Mineralocorticoid Receptor Antagonists (MRAs)
examples: spironolactone and eplerenone
mechanism
Block action of aldosterone, decrease blood volume (no increase in sodium and subsequent water retention)
May affect vasoconstriction
Reduce some of the fibrosis and myocardial necrosis
what are beta blockers
examples: bisoprolol, nebivolol and carvedilol
mechanism:
Beta-selective adrenoceptor blockers, block action of adrenaline and noradrenaline on heart, reducing sympathetic drive and opposing neurohormonal adaptation
Slows heart down → anti-arrhythmic effects
what are Sodium-glucose co-transporter-2 inhibitors (SGLT2i)
examples: dapagliflozin and empagliflozin
mechanism → reduce reabsorption of glucose in kidneys, promoting urinary glucose excretion and reducing sodium reabsorption
mechanism of action is unclear in heart failure, may be beneficial in
diuresis
blood pressure reduction
prevention of cardiac remodelling
what can be used to manage symptoms from oedema
loop diuretics
thiazide and thiazide-like diuretics
what are loop diuretics
examples: furosemide and bumetanide
mechanism:
Alter how kidney handles sodium
Inhibit Na+/K+/2Cl- co-transporter in the loop of Henle in the kidney, preventing sodium reabsorption
Water follows sodium, so without sodium reabsorption water does not follow and diuresis results
what are thiazide and thiazide-like diuretics
examples: Bendroflumethiazide (thiazide), indapamide (thiazide-like), metolazone (thiazide-like)
mechanism:
• Alter how kidney handles sodium
Inhibit Na+/Cl- transporter in the distal convoluted tubule, preventing sodium reabsorption
Water follows sodium, so without sodium reabsorption water does not follow and diuresis results
why is digoxin used in heart failure
mechanism:
Inhibits Na+/K+ ATPase → rise in intracellular sodium, promoting calcium entry → increased force of myocardial contraction (positive inotropic effect)
Impairs atrioventricular conduction (directly and indirectly via vagal activation), slowing heart down and controlling ventricular rate → anti-arrhythmic effects
No mortality benefit, but there is reduction in hospitalisation and is used to improve symptoms
why is ivabradine used in heart failure
reduces heart rate without reducing blood pressure
mechanism
Blocks sinoatrial node pacemaker, sodium and potassium (i-funny (If) or ‘funny current’) currents, reducing heart rate and therefore oxygen demand of the heart
May cause visual disturbance due to retinal If
commence and uptitrate beta blocker therapy to maximum tolerated dose before considering ivabradine
why is hydralazine used in heart failure
Mechanism:
Precise mechanism of action not known, but works as a direct acting vasodilator
Effect is a reduction in blood pressure
Can cause sodium and fluid retention → need to monitor
why are nitrates used in heart failure
mechanism: Vasodilation via the release of nitric oxide (NO)
why is IV iron used in heart failure
patients need to be screened for low iron
UV iron used in those who are sympotamtic and other criteria
what is the treatment for HFpEF, heart failure with preserved ejection fraction (EF ≥50%)
Until recently treatment aimed at:
Symptom control with diuretics
Improved management of co-existing co-morbidities e.g. hypertension, ischaemic heart disease (see other lectures)
However there are now mortality benefits for SGLT2 inhibitors such as Empagliflozin and dapagliflozin
there are reduced hospitalisation for MRAs
what do we need to monitor in heart failures
Medicines → U&Es, FBC, blood pressure, heart rate
Symptoms → important that patients monitor themselves and report any deterioration e.g. breathlessness, oedema, weight
how is acute heart failure managed
IV loop diuretics
Oxygen may be needed
Other specialist treatments eg iv inotropes
Treat any underlying cause
May need to modify existing medicines
Under specialist team
what are non-pharmacological managements for HF
Valve replacement if appropriate
Ablation (if secondary to arrhythmias)
Cardiac resynchronisation therapy (device that can improve pumping function of heart, improve synchronicity of the ventricles)
Implantable cardiac defibrillator (ICD)
Lifestyle: diet, alcohol, smoking, exercise