Musculoskeletal Alterations
1/155
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
156 Terms
Bone-forming cells
Osteoblasts
Cells that breakdown bone tissue
Osteoclasts
Mature bone cells
Osteocytes
Bone remodeling =
Removal of old bone by osteoclasts
Deposit of new bone by osteoblasts
Attach muscles to bones
Tendons
Attach bones to bones (fibrous connective tissue). Have poor blood supply → slow repair after injury
Ligaments
Gerontological effects of aging on MS system
Functional problemsv (ADLs e.g. walking/get out of bed)
Decreased bone density
Increased r/o osteopenia and osteoporosis
Decreased muscle mass and strength
Decreased flexibility
Increased r/o OA
Decreased height (kyphosis)
Risk for falls
Changes in proprioception awareness of self in relation to environment)
Why do older adults have higher risk for falls?
Changes/decreases in proprioception awareness of self in relation to environment)
Diagnostic test used to check for osteoporosis (measures bone density)
Dual energy X-ray absorptiometry (DEXA)
Preventive teaching for people at high risk for falls
Those with gait instability, vision impairment
Age0appropriate exercise to help maintain muscle strength and balance
Adequate calcium and vitamin D for bone health
Assess living environemnt for safety risks
Soft tissue injuries
Sprains
Strains
Dislocations
Subluxation
Nursing managemnet for sprains and strains
RICE (rest, ice, compression, elevation)
Analgesia (NSAIDs or tylenol)
RICE (management of sprains and strains)
R – Rest: stop activity and limit movement
I – Ice (cryotherapy) on area: 24-48 hrs; 20-30 min at a time
C – Compression: elastic bandage; apply distal to proximal
E – Elevation: above the heart
Why take NSAIDs with food?
To prevent GI irritation and bleeding
Injuries from prolonged force or repetitive movements and awkward posture
Repetitive strain injury (RSI & cumulative trauma disorder)
Those who are at risk for RSI
Those who perform repetitive motions without sufficient muscle rest
E.g. dancers, butchers, athletes, and keyboard operator (gamers), sewing, hair cutters
Caused by compression of the median nerve
Associated with activities that require continuous wrist movement
Compression often caused by trauma, edema, cancer, rheumatoid arthritis, or soft tissue masses, hormones
Carpal tunnel syndrome (CTS)
Which populations have increased incidence of CTS?
Diabetes, PVD, RA, and women
CTS manifestations
Impaired sensation, pain, numbness, or weakness; clumsiness
Tinel’s sign or Phalen’s sign
Late stages:
Atrophy, recurrent pain, and dysfunction of hand
Function of rotator cuff
Four muscles in the shoulder that stabilize humeral head: assist ROM and rotation
Tear may occur with aging, repetitive stress, or injury
Manifestations of rotator cuff injury
Shoudler weakness, pain, and decreased ROM (can’t raise arm up)
Positive drop arm test
Diagnosis of rotator cuff injury
MRI is best
Conservative and surgical tx of rotator cuff injuries
Conservative: Rest, ice, heat, NSAIDs, corticosteroid injections, US, and PT
Surgical (if does not improve): Arthroscopy or acromioplasty, immobilization 6 weeks, passive exercises followed by PT
Conservative tx of rotator cuff injuries
Rest, ice, and heat, NSAIDs, corticosteroid injections, US, and PT
Surgical tx of rotator cuff injuries
Arthroscopy or acromioplasty; affected area is immobilized for 6 weeks, and followed by passive exercises, then followed by PT
Associated with ligament sprains in sports
Rotational stress when knee in flexion and foot planted
Blow to knee causes shearing of meniscus resulting in tear
Also, degenerative tears in older adults and people who squat or kneel at work
Meniscus injury
Diagnosis for ACLs
Positive Lachman’s test
MRI
Inflammation of the bursae from repeated or excessive trauma, friction, gout, RA, or infection
Hands, elbows, shoulders, knees, and hips
Bursitis
S&S of bursitis
Warmth, pain, swelling, limited ROM
Tx of bursitis
Identify and correct cause; rest with immobilization; ice and NSAIDs
Surgery: bursectomy
Risks of skeletal traction
Delayed union, nonunion, or infection at pin sites
Complications of immobility (pneumonia, skin breakdown, DVT, loss of bone density)
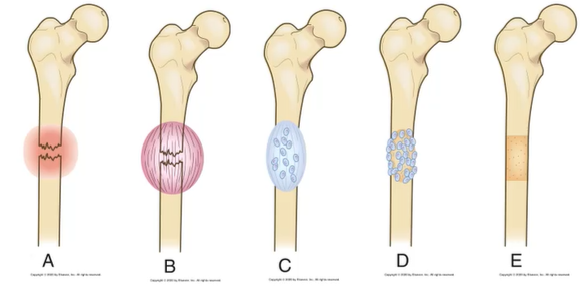
Healing process of fractures
1) Fracture hematoma
2) Granulation tissue formation
3) Callus formation
4) Ossification
5) Consolidation
6) Remodeling
FGCOCR (healing process of fracturos: union)
F – Fracture hematoma
G – Granulation tissue formation
C – Callus formation
O – Ossification
C – Consolidation
R – Remodeling
Factors influencing fracture healing
Displacement and site of fracture
Blood supply
Other local tissue injury
Immobilization (slows healing)
Internal fixation devices (infection)
Infection
Poor nutrition (patient needs protein + hydration)
Age
Smoking
Clinical manifestations of fractures
Edema and swelling
Pain and tenderness
Muscle spasm
Deformity
Contusion
Loss of function
Crepitation
Guarding
Overall goals for fracture care
Anatomic realignment (reduction)
Immoblization to maintain alignment
Restoration of normal or near normal function
Diagnostic assessment of fractures
H&P
X-ray
CT scan + MRI
Management for open fractures
Surgical debridement and irrigation
Tetanus and diptheria immunization (ask patient for immunization hx)
Prophlactic abx therapy (open fractures have high infection risk)
Short-term (48-72 hrs)
Tape, boots, or splints, applied directly to the skin to reduce muscle spasms
For example, Buck’s traction for femor fracture
Traction weighs 5-10 lbs
Skin assessment and prevention of breakdwon imperative
Skin traction
Align injured bones and joints or treat joint contractures and congenital hip dysplasia (bone alignment in fractures)
Long-term pull to maintain alignment
Pin or wire inserted into bone (weighs 5-45 lbs)
Risk for delayed union, nonunion, or infection at pin sites, complications of immobility (pneumonia, skin breakdown, DVT, loss of bone density)
Skeletal traction
What is used for fracture immobilization
Casts
Sling
Temporary after closed reduction
Allows patient to perform ADLs while maintaining immobilizations
Incorporates joints above and below fracture for stabilization during healing
Two most common materials: plaster of Paris; Fiberglass
Casts (fracture immobilization)
Used to support and elevate arm
C/I with proximal humerus fracture
Ensure axillary area is well-[added
No undue pressure on neck
Encourage movement of fingers and non-immobilized joints
Sling (fracture immobilization)
Nursing implications for slings
Used to support and elevate arm
C/I with proximal humerus fracture
Ensure axillary area is well-[added
No undue pressure on neck
Encourage movement of fingers and non-immobilized joints
Fracture assessment
Obtain a brief history of:
Traumatic episode
Mechanism of injury
Patient position when found
Transport to ED ASAP
Thorough assessment and start of tx
Neurovascular assessment
Neurovascular assessment for fractures
Musculoskeletal injuries can alter the neurovascular status of an extremity
Espeically important distal to the injury (e.g. foot injury = watch out for toes)
Assess and document before and after treatment
Compare bilaterally
Palpate pulses
Assess for tingling, paresthesia, numbness
Preoperative care for fractures
Patient teaching
Immobilize injured area
Educate about assistive devices
Expected activity limitations
Assure that needs will be met
Pain meds
Postoperative care for fractures
Monitor VS and S&S of infection
General principles of post-op care (early ambulation, cough, deep breathing, incentive spirometer, monitor for DVT, skin assessment)
Frequent neurovascular assessment (pulse + ask if feeling numb, paresthesia, tingling)
Cast can be too tight or light; cause impingement; swelling can cause obstruction of nerve or blood vessels
Monitor cast if too tight or if swelling is causing tightness
Be attentive to limitations with turning, positioning, or extremity support
Minimzie pain and discomfort
Monitor for bleeding or discharge
Aseptic technique
Blood salvage and autotransfusion (give patient’s blood back to themselveS)
Postoperative neurovascular assessment (fractures)
Assess Pulse + ask if feeling numb, paresthesia, tingling, pain
Cast can be too tight or light; cause impingement; swelling can cause obstruction of nerve or blood vessels
Monitor cast if too tight or if swelling is causing tightness; ask patient if cast is uncomfortable
Nutrition therapy for musculoskeletal recovery
Optimal soft tissue and bone healing
Increase protein (1g/kg of body weight)
Increase vitamins (B, C, D)
Increase calcium, phosphorus, and magnesium
Increase fluid (2000-3000 mL/day)
Increase fiber
Body jacket and hip spica cast patients: eat six small meals a day
They don’t have much room in abd area
Complications of fractures
Majority health w/o complications
Medical emergencies needing immediate attention required with
Open fractures w/ severe blood loss
Fractures that damage vital organs
Death is usually result of:
Damage to underlying organs and vascular structures
Complications of frature or immobility
Infection
Compartment syndrome
DVT
Fat embolism
Rhabdomyolysis
Common complications of fractures
Infection
Compartment syndrome
Venous thromboembolism (DVT)
Fat embolism
Rhabdomyolysis
ICVFR (common complications of fractures)
I – Infection
C – Compartment syndrome
V – Venous thromboembolism (DVT)
F – Fat embolism
R – Rhabdomyolysis
A complication of fractures that is a medical emergency: swelling and increased pressure within a limited space (muscle compartment); compromises neurovascular function of tissues within that space (e.g. patient has cast on arm, then hand becomes tingling/swelling)
Causes excruciating pain not relieved by pain meds
Associated with fractures with extensive tissue damage and crush injury
Most common site = distal humerus and proximal tibia
May occur after knee or leg surgery or with prolonged pressure (limb trapped under the body)
Compartment syndrome
Most common site affected by compartment syndrome
Distal humerus and proximal tibia
May occur after knee or leg surgery or with prolonged pressure (limb trapped under the body)
Compartment syndrome
Clinical manifestations of compartment syndrome
Pain: out of proportion to injury and refractory to opioids; passive stretch (swelling stretches skin and fascia and makes them taut)
Pressure
Paresthesia (numbness/tingling)
Pallor
Paralysis or loss of function
Pulselessness
Six P’s of compartment syndrome
Pain: out of proportion to injury and refractory to opioids; passive stretch (swelling stretches skin and fascia and makes them taut)
Pressure
Paresthesia (numbness/tingling)
Pallor
Paralysis or loss of function
Pulselessness
Early signs of compartment syndrome
Notify HCP if pain unrelieved by drugs and out of proportion to injury
Paresthesia is also an early sign
Relieving the source of pressure may prevent progression (e.g. loosen cast)
Late signs of compartment syndrome
Pulselessness
Paralysis
May require amputation
What NOT to do if compartment syndrome is suspected?
Do not elevate extremity above the heart
Do not apply cold compresses or ice
Why not elevate extremity above the heart nor apply cold compres or ice if suspecting compartment syndrome?
Causes vasoconstriction and reduced circulation to an already comprimised extremity (or it may even lead to compartment)
Treatment of compartment syndrome
Relieve pressure
Surgical decompression (fasciotomy) to release pressure
Amputation (if severe or pulseless)
A complication of fracture; veins of lower extremities and pelvis are highly susceptible to thrombus formation due to venous stasis from muscle inactivity; increased risk with hip fracture, THR, or TKR
Venous thromboembolisms
Interventions to prevent venous thromboembolism (complication of fractures)
Prophylactic anticoagulant drugs for 10 to 14 days
Antiembolism stockings
Intermittent pneumatic compression-devices
Exercises
What veins are at increased risk for forming venous thromboembolisms?
Veins of lower extremities and pelvis are highly susceptible to thrombus formation due to venous stasis from muscle inactivity; increased risk with hip fracture, THR, or TKR
What fractures/procedures causes increased r/o venous thromboembolism
Hip fracture, THR, TKR
A complication of fractures. Systemic fat globules from fracture/broken bone that are distributed into tissues and organs (especially lungs and brain)
Contributory factor in mortality
Fat embolism
What fractures can most commonly cause fat embolisms to develop
Fracture of long bones, ribs, tibia, and pelvis
When does fat embolism occur?
Most common with fracture of long bones, ribs, tibia, and pelvis
May also occur after joint replacement, burns, pancreatitis, liposuction, crush injuries, and bone marrow transplants
Pelvic fracture =
Increased r/o fat embolism
Hip fracture, THR, and/or TKR =
Increased r/o venous thromboembolism
Complication of fractures; syndrome caused by breakdown of damaged skeletal muscle
Releases myoglobin into circulation resulting in obstruction of renal tubules, causing ATN and kidney failure
Rhabdomyolysis
Monitoring for rhabdomyolysis
Assess urine output
Dark-reddish brown urine (cola-colored)
Assess for symptoms of AKI
Most common cause for amputation
PVD, especially related to diabetes
Causes of amputation
PVD, especially related to diabetes
Thermal injuries
Tumors, osteomyelitis
Congenital limb disorders
Complications of joint surgery
Infection
Common organisms: gram-positive streptococci and staphylococci
Loosens prosthesis and causes pain
Prophylaxis: self-contained OR suites, laminar airflow, and abx
VTE
Anticoagulants
Intermittent pneumatic compression
Early ambulation
Preoperative care for joint surgeries
The patients needs to be free from:
Infection
Skin breakdwon
Acute joint inflammation
Explain post-op care:
Early mobility, hydration, VTE, prophylaxis
Assure availability of analgesia
PT visit with practice of exercises and use of assistive devices
Post-op management (joint surgeries + all of musculoskeletal)
Regular neurovascular assessments (important for all musculoskeletal)
Prevent impingement/compartment syndrome
Administer: anticoagulants and abx prophylactically
Teach the patient about continuing meds at home
Monitoring coagulation/WBC studies
Pain management: analgesia
May consider epidural, intrathecal, femoral nerve block, PCA, oral opioids, or NSAIDs
Exercise and mobility (early ambulations); follow protocols
Reduce risk of complications of decreased mobility
Severe infection of bone, bone marrow, and surrounding soft tissue
Can be caused by a variety of organisms; but most common is staphylococcus aureus
Indirect entry (hematogenous) = 20%
Direct entry (contiguous e.g. bone surgery) = 80%
Osteomyelitis
Pathophysiology of osteomyelitis
Microorganisms enter the blood and grow
Increasing pressure in bone leads to ischemia and vascular comprimise of the periosteum
Infection spreads through bone, cortex, and marrow cavity, causing obstruction of blood flow, necrosis, and sequestrum (piece of dead, devascularized bone that has separated from healthy bone)
Clinical manifestations of acute osteomyelitis
Systemic manifestations
Fever
Night sweats
Chills
Restlessness
Nausea
Malaise
Drainage (late)
Clinical manifestations of chronic osteomyelitis
Systemic manifestations are lessened
Local signs of infection are more common
Pain, swelling, warmth
Granulation tissue turns to avascular scar tissue which is an ideal site for microorganism growth because it cannot be penetrated by abx
Conditions takes a long time to heal, and very difficult for abx to reach the bone
Osteomyelitis
Interprofessional care for acute osteomyelitis
Most start IV abx therapy, then switch to oral agents
IV for 4-6 weeks; some need 3-6 months
CVAD requires follow-up from skilled nursing facility or home care
Cultures or bone biopsy before abx
Surgical debridement and drainage of abscess or ulcer
Interprofessional care for chronic osteomyelitis
Surgical removal of poorly perfused tissue, dead bone
Extended use of abx
Oral therapy with a fluoroquinolone for 6-8 weeks
Oral therapy for 4-8 weeks after acute IV therapy is done
Health promotion for osteomyelitis
Control other current infections
Persons at risk:
Immunocomprimised
Have diabetes, orthopedic prosthetic devices, or vascular insufficiency (PVD)
Patient/caregiver education: S&S of osteomyelitis)
Encouarge to call HCP if:
Bone pain, fever, swelling, restricted limb movement
What people are at risk for developing osteomyelitis?
Immunocomprimised
Have diabetes, orthopedic prosthetic devices, or vascular insufficiency (PVD)
Encourage to call HCP if osteomyelitis patient experiences these symtpoms:
Bone pain, fever, swelling, restricted limb movement
Group of genetic diseases characterized by symmetric wasting of skeletal muscles w/o neurological involvement
Gradual loss of strength with increasing disability and deformity
Most common is Duchenne
Muscular dystrophy (MD)
MD treatment
No cure
Corticosteroids → slow progression for up to 2 years; improve survivial
Deflazacort
Disease-modifying drug:
Eteplirsen (Exondys 51)
Treatment goals for MD
Preserve mobility and independece through exercise, PT, and use of assistive devices
Orthotic jacket to prevent spinal deformity or injury
What to monitor for MD?
Cardiomyopathy and HF
CPAP, tracheostomy, and mechanical ventilation
Function of intervertebral discs
Separate vertebrae and help absorb shock
Intervertebral disc disease involves deterioration, herniation, or other problem with intervertebral discs (can involve cervical, thoracic, and lumbar spine)
Loss of fluid leads to loss of elasticity, flexibility, and shock-absorbing capabilities in intervertebral discs
Disc becomes thinner as nucleus pulposus dries out, and load is shifted to annulus fibrosus
Results in progressive destruction as nucleus pulposus seeps out (herniated or slipped disc)
Degenerative disc disease (DDD)