Optimising control of T2DM
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Factors to consider for every patient with T2DM
Age and frailty status
Time since diagnosis
Renal function and degree of microalbuminuria – calculate kidney risk
Weight
Occupation and social history
Age of diagnosis
Family history
Co-morbidities and risk factors for CV disease
Polypharmacy - many medications cause a rise in blood glucose e.g. steroids, anti-psychotics
Menopause
Driving status
Is patient able / willing to BG monitor?
Non-pharmacological treatments of Diabetes
Reduce smoking
Reduce alcohol
Physical activity
Weight management
Healthy diet
high veg, high protein, low carb
HbA1c tagrets in T2DM
Diet/Lifestyle ± metformin = 48mmol
SU or insulin = 54mmol
Mild/moderate frailty = 53-64
Severe frailty = 64-75
Clinical Inertia
Where healthcare providers fail to intensify treatment when a patient isn't meeting evidence-based goals
Why is achieving target HbA1c so important in diabetes?
Reduction in micro- and macrovascular complications
Reduce symptoms of diabetes
Reduce risk and episodes of hypoglycaemia
Avoid hospital admissions
Reduce risk of infection
Improve quality of life
Time in Range
percentage of time that a person spends with their blood glucose levels in a target range
(# in range finger pricks/ total finger pricks) x 100
taken over at least 14 days
Non insulin treatments for T2DM
GLP1
SGLT2i
Sulfonylureas
Pioglitazone
SGLT2i
inhibits SGLT2 (Sodium–Glucose Co-Transporter 2) which is a glucose transporter leading to decreased glucose reabsorption and increased glucose loss via urine.
Common SE:
UTIs
Genital fungal infections
Serious SE
euglycaemic DKA
Forneirs Gangrene
Weight Loss: Yes
Hypo risk: Low
Sulfonylureas
Close pancreatic β-cell KATP channels which leads to an increase in insulin secretion
Common SE:
Hypo
Weight Gain
Serious SE:
severe prolonged hypoglycaemia
Weight Loss: No
Hypo risk: High
Biguanides
Decrease the hepatic gluconeogenesis and increase insulin sensitivity. This leads to a decrease in intestinal glucose absorption
Common SE:
GI upset
B12 deficiency
Severe SE:
lactic acidosis
Hypo risk: No
Weight loss: No - neutral effect
DPP4i
inhibit the DPP-4 enzyme which increases the breakdown of GLP-1 leading to an increase insulin release/decreases glucagon
Common SE:
URTI symptoms
headache
Serious SE:
pancreatitis
severe joint pain
Hypo risk = low
Weight effect = neutral
Pioglitazone
PPAR-γ agonist. It increases insulin sensitivity in muscle/adipose
Common SE:
weight gain
oedema
Serious SE:
HF exacerbation
fractures
Hypo risk = low
Weight effect: weight gain
GLP1s
reduce desire for sweet things
cannot be used with DPP4i
once weekly injections
SE:
GI side effects
pancreatitis (rare)
Which antidiabetics have a cardio/renal protective?
Metformin
SGLT2i
GLP-1
Drug safety considerations of Inslulin
Healthcare professionals who handle, prescribe or administer insulin need to receive regular training and demonstrate competence
Over 30 different insulin preparations available!
NEVER STOP insulin in people with type 1 diabetes
Insulin types
rapid acting analogue
onset is in 5-15mins
peak in 30mins-1.5h
lasts 3-5h
short acting human
onset is in 30mins
peaks in 2-4h
lasts 6-8h
intermediate acting
onset is in 2h
peaks in 4-8h
lasts 14-16h
pre-mixed
onset is in 30-60mins
peaks in 2-4h
duration is 12-14h
long acting
onset within 2h
no peak period
duration is 24-42h
Insulin injection sites
Back of upper arms
abdomen
upper buttocks
upper outer thighs
inject into one area no more frequently than every 4 weeks. each injection should be at least 1cm away from the last
Lipohypertrophy
a thickened rubbery lesion of fat tissue that develops in the subcutaneous layer where insulin is repeatedly injected.
Primary causes include incorrect rotation of injection sites or not rotating, duration of insulin use, frequency of injections and needle reuse
Insulin use in T2DM
Insulin therapy should be offered to people with diabetes with inadequate blood glucose control on optimised oral glucose-lowering drugs
Regime should be chosen based on patient lifestyle, preference and risk of hypoglycaemia
First line recommendation is neutral protamine Hagedorn (NPH) insulin injected once or twice daily
How do you change medications when starting injectibles?
Metformin - continue
SU - reduce dose or stop depending on type of insulin
TZD - STOP or reduce dose
DPP-4i - stop if GLP-1 initiated
SGLT2i - continue
What do we need to consider when starting insulin in T2DM?
Any recent changes to dietary intake – does the individual injecting insulin have carb awareness?
Any change in level of physical activity - has the individual injecting insulin taken up any new or extra activities such as going to the gym or have they recently changed work patterns?
Any recent weight change – either planned or unplanned?
SICK DAY RULES
Has any oral diabetes medication been missed recently?
Check injection sites – any lipohypertrophy
How to adjust basal insulin?
reduce insulin by 10-20% if patient is experiencing hypos
How do you adjust BD insulin regimens?
elevated glucose before bed/breakfast = increase evening dose by 10%
elevated glucose before lunch/evening = increase morning insulin by 10%
Smartpens
reusable pens which record time and dose of insulin given to patient
links to smartphone and to CGM apps
allow patients to take control over their diabetes as they can see daily patterns and make associations between good glycaemic control and injection patterns
CGM
Continuous glucose monitors
More often seen in T1D but becoming more common in T2D
Many patients self-funding (if T2DM)
e.g. Dexcom one+ and Freestyle Libre 2 Plus are approved for All Type 1 patients and Type 2 patients on multiple daily insulin injections fitting certain criteria
Sensor changed every 7-14 days depending on type
CSII
Continuous SC insulin infusion or Insulin pumps
Used for T1DM
Two types of pump: tethered and patch
CSII therapy be initiated only by a trained specialist team
Only uses fast acting insulin, delivered as basal (background) and bolus (to cover meals)
Hybrid Closed Loop Systems
Only uses fast acting insulin, delivered as basal (background) and bolus (to cover meals)
Monitoring in T2DM
Annual review including:
a blood test (FBC, U&Es, LFT, eGFR, HbA1c and cholesterol panel)
Foot check
BP
Weight check (BMI)
Urine ACR
More frequent HbA1c, eGFR and urine ACR monitoring if control not optimal or signs of kidney disease / stress
Retinal screening annually
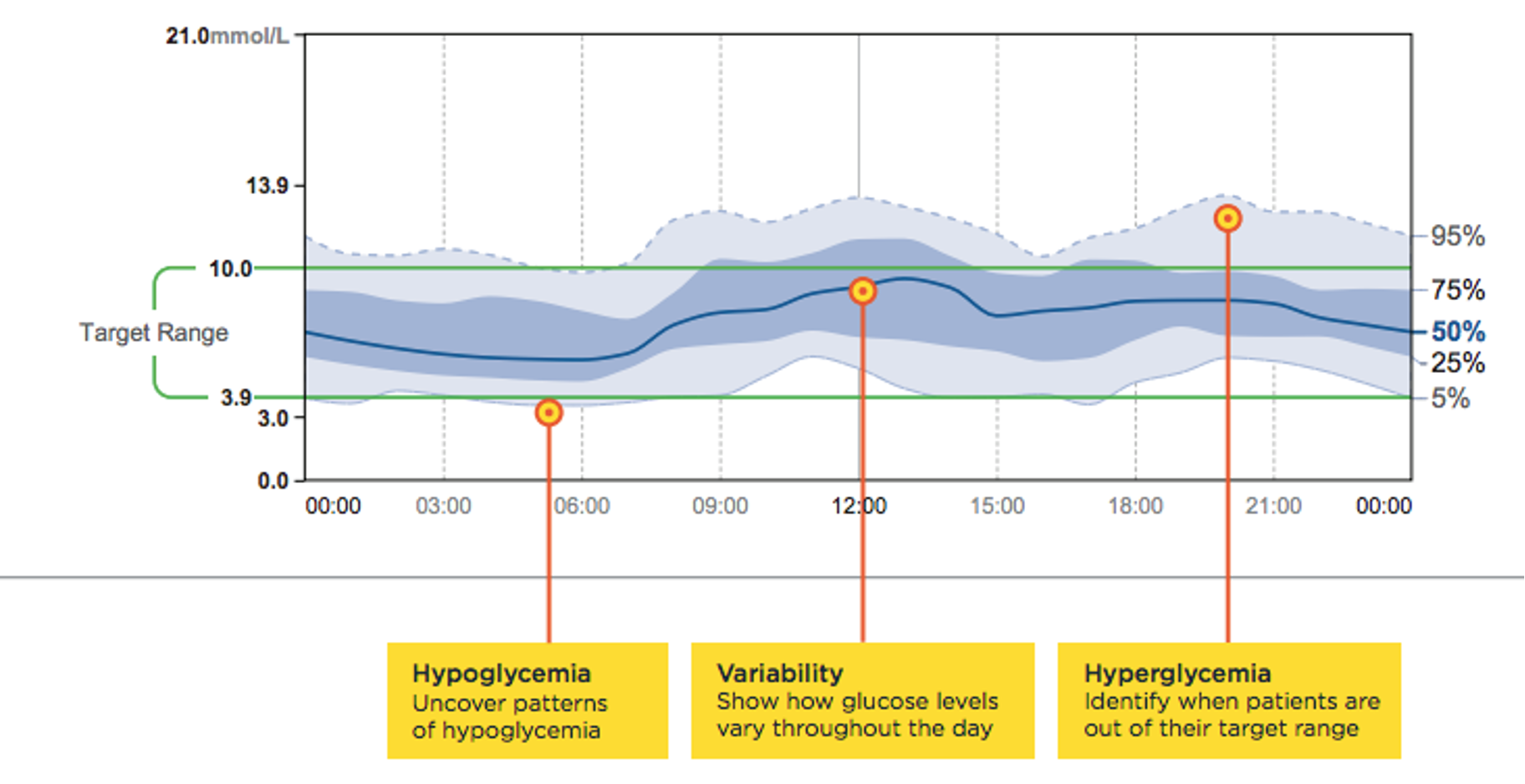
AGP
Ambulatory Glucose Profile
a summary of blood glucose values from the report period with the median (50%) and other percentiles shown as a single day
How to approach reviewing and interpreting AGP?
Get consent for sharing data
Find something positive in data to discuss with patient
Look for a ‘good day’ and try and replicate it
Data should only be interpreted after 14 days of collection
Glucose variability – ideal <36%
Priorities when reviewing AGP
Priority 1: Hypoglycaemia
how often
when
any trend
Priority 2: Hyperglycaemia
Reducing hyperglycaemia (measured by HbA1c) is associated with clinically significant reductions in microvascular complications and long-term macrovascular disease
Priority 3: Glucose variability
important risk factor for CV compliations