Female reproductive anatomy
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
3 roles of the female reproductive system
produce gametes
produce hormones
receive, nourish, deliver a developing embryo
How does the female system operate compared to male system
Male system= constant, continuous spermatogenesis, steady testosterone
Female system
operates cyclically: fluctuating hormones, endometrial remodeling, and monthly prep for pregnancy, whether or not it occurs
same HPG axis—but female version adds positive feedback (LH surge)
FSH→ support cells
LH→ hormone-producing cells
In the ovary, granulosa cells also convert androgens→ estrogen
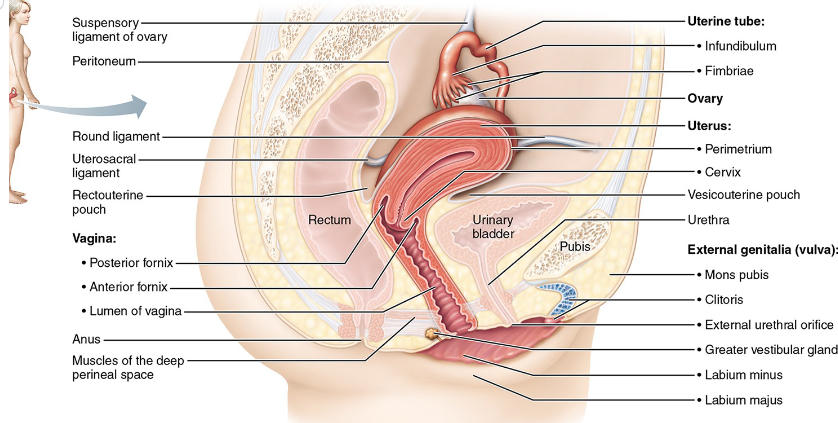
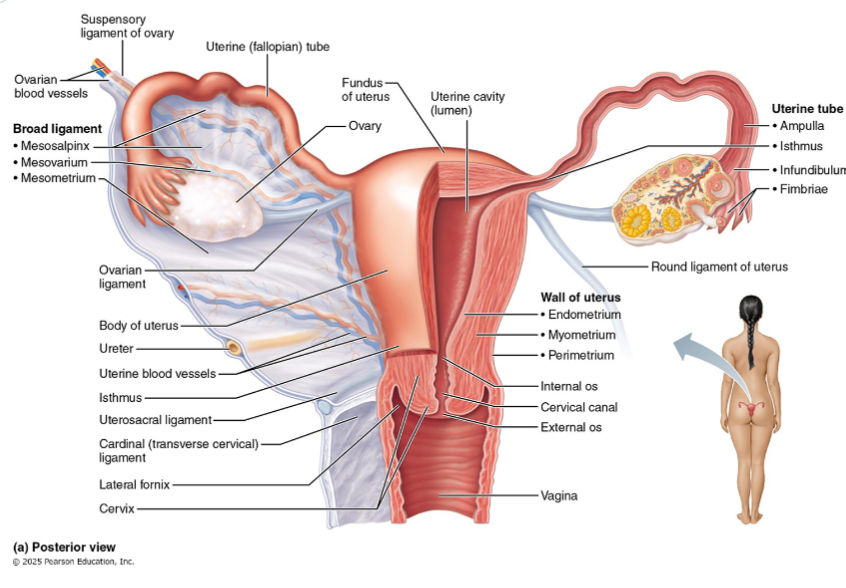
Female Internal genitalia
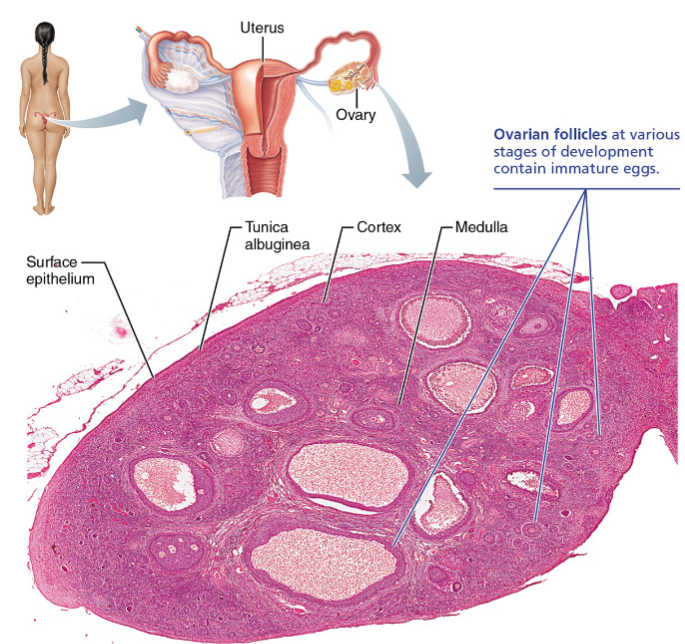
Ovaries
Uterine tubes(oviducts/ fallopian tubes)
Uterus
Vagina
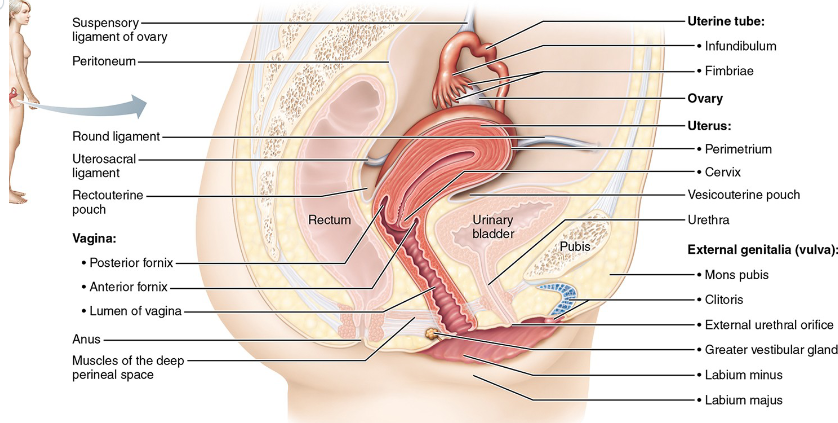
External genitalia
Vulva
(mons pubis)
Labia
Clitoris
Vestibular glands
Ovaries
Paired organs flanking the uterus
almond-shaped(2X size of an almond)
aka gamete factory
Function of ovaries
produce oocytes (gametes) AND secrete estrogen/progesterone (endocrine) — dual function, analogous to the testis
3 supporting ligaments of the ovaries
Ovarian ligament
Suspensory ligament
Mesovarium
Ovarian ligament
Medially attaches ovary to uterus
Short
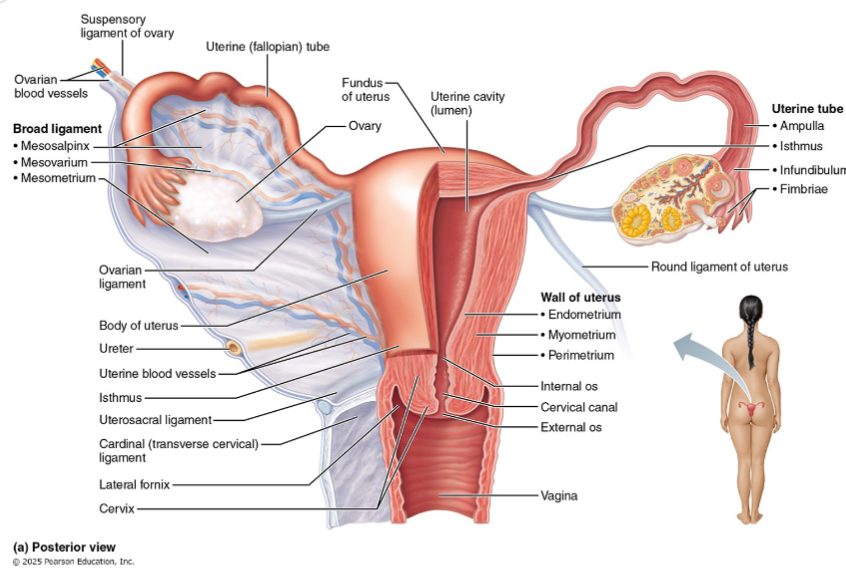
Suspensory ligament
Laterally attaches ovary to pelvic wall
Contains ovarian blood vessels and nerves
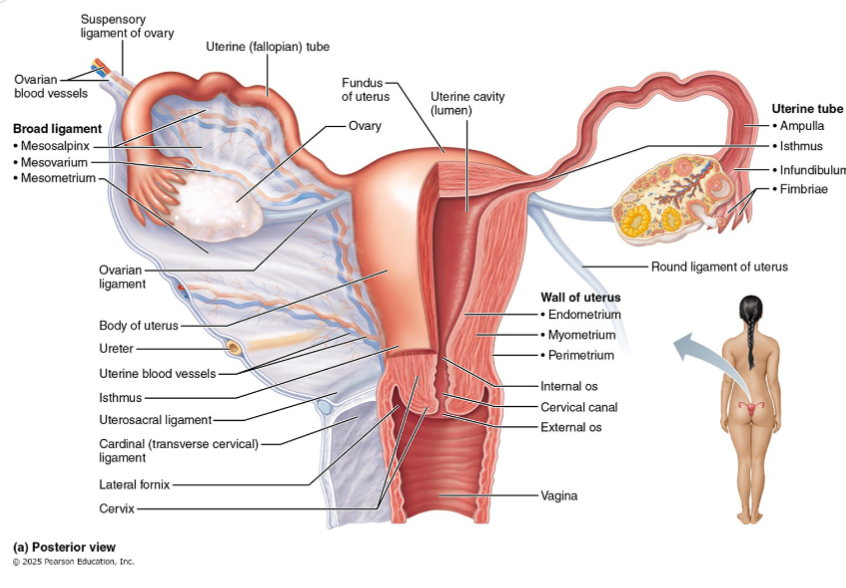
Mesovarium
Attaches ovary to broad ligament
Part of the broad ligament
suspends ovary
-salpinx= fallopian tube
Surface epithelium layer
Is the outermost layer of the ovaries
Consists of simple cuboidal cells
AKA ‘germinal epithelium’ even though oocytes DO NOT arise here
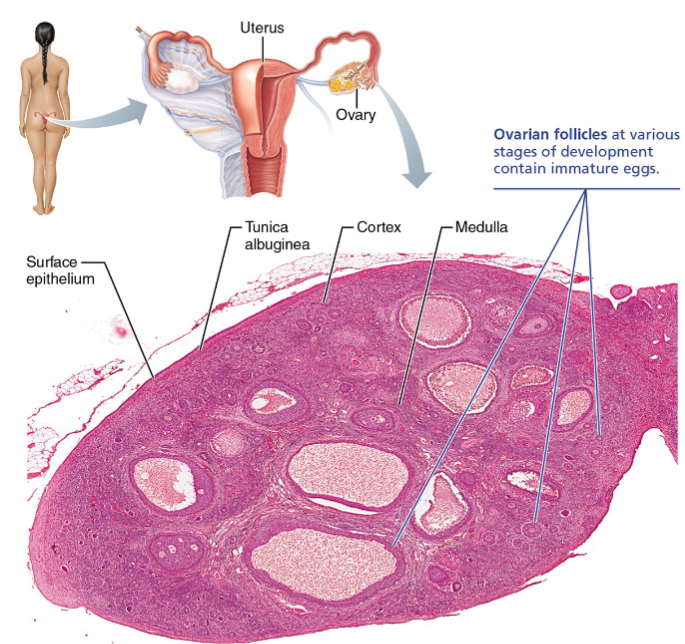
Tunica albuginea layer
Layer beneath surface epithelium
is a dense fibrous capsule
same name as testis covering—homologous structure
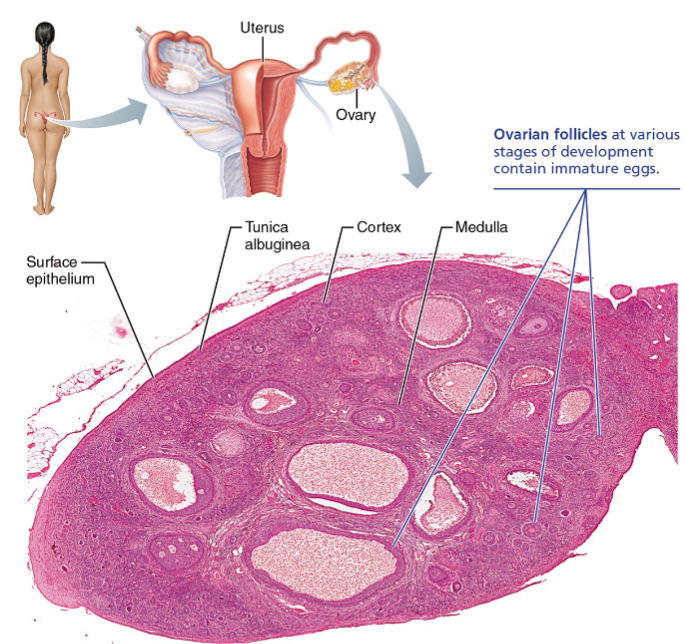
Cortex of ovaries
Outer region layer
Houses ovarian follicles at various stages of development
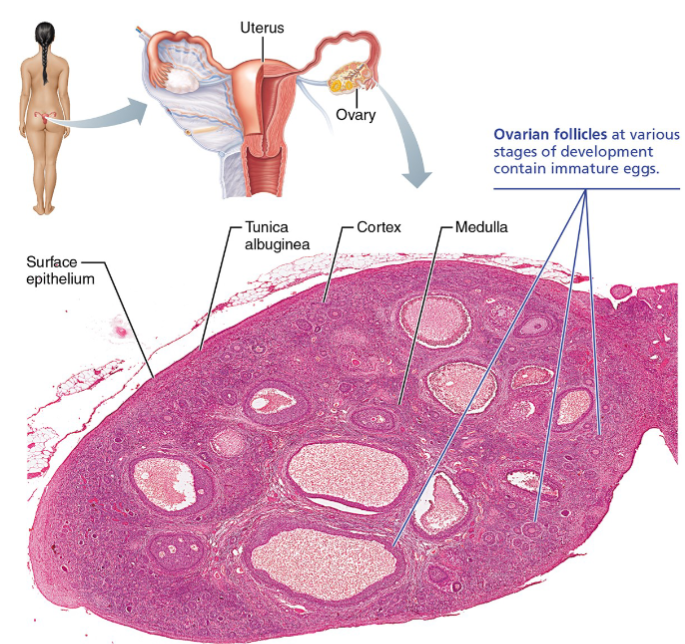
Medulla of ovaries
Inner region layer
Large blood vessels, nerves, lymphatics
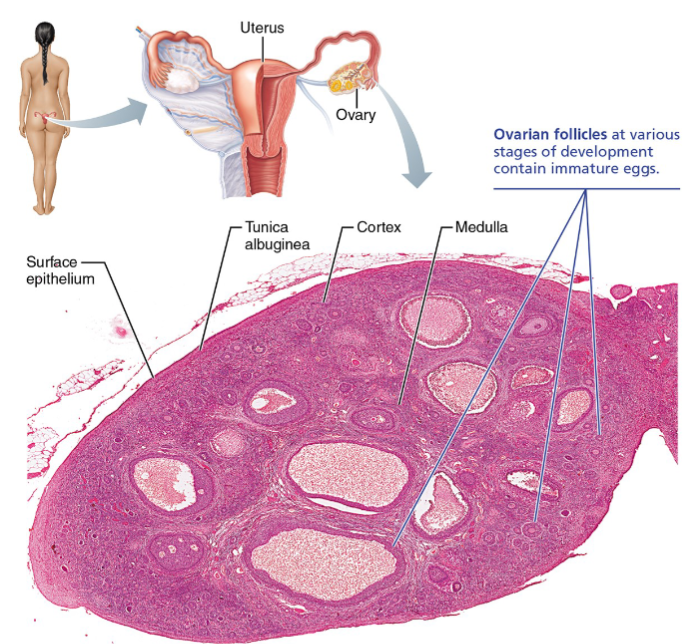
Ovarian follicles
Follicles are tiny sac-like structures in the cortex, each containing:
An oocyte (immature egg)
One or more layers of surrounding support cells
6 stages of follicle development
Primordial follicle
Primary follicle
Secondary follicle
Mature (Graafian) follicle
Corpus luteum
Corpus albicans
Stage 1: Primordial follicle
Oocyte + single layer of flat follicle cells
present from birth
Stage 2: Primary follicle
Oocyte + cuboidal/columnar granulosa cells
zona pellucida appears
Stage 3:Secondary follicle
Multiple granulosa cell layers;
antral spaces forming;
theca cells developing outside
Stage 4: Mature (Graafian) stage
Large antrum (fluid-filled cavity); oocyte on stalk (cumulus oophorus)
ready for ovulation
Stage 5: Corpus luteum
Post-ovulation remnant
temporary endocrine structure producing progesterone + estrogen
Stage 6: Corpus albicans
Scar tissue
remnant after corpus luteum degenerates
Ovulation
Each month, typically ONE mature follicle ruptures at the ovary surface → ovulation
In older females, the ovarian surface is scarred and pitted from decades of ovulation events
Oviducts
Also called uterine tubes or Fallopian tubes
10 cm long; NO direct connection to the ovary (oocyte is released into peritoneal cavity)
Supported by the mesosalpinx (part of the broad ligament)
3 regions of oviducts
From most lateral to medial
Infundibulum
Ampulla
Isthmus
Infundibulum of the oviducts
Funnel-shaped opening to peritoneal cavity; fringed with fimbriae (ciliated, fingerlike projections that drape over ovary)
fringed Fimbriae(ciliated projections) capture oocyte after ovulation
Ampulla of oviducts
Wide middle region; half of tube length
Usual site of fertilization
Isthmus of oviducts
Narrow medial third
Opens into superolateral wall of uterus
Wall composition of oviducts + their function
Smooth muscle layer → peristaltic contractions
Ciliated epithelium → cilia beat toward uterus
Nonciliated secretory cells → provide nutrients for oocyte and sperm
Oocyte capture and transport
During ovulation, fimbriae stiffen and cilia create fluid currents → sweep oocyte into tube
Transport toward uterus by: (a) peristaltic contractions of smooth muscle + (b) ciliary beating of epithelial cells
Transit time: 3-4 days from ovulation to arrival in uterus
Ectopic (tubal) pregnancy
Fertilized oocyte implants in tube (usually ampulla) instead of uterus → dangerous
tube cannot support growing embryo; usually requires surgical intervention
Pelvic inflammatory disease (PID)
Ascending infection (often STI) → spreads to tubes → scarring → blocked tubes → major cause of infertility
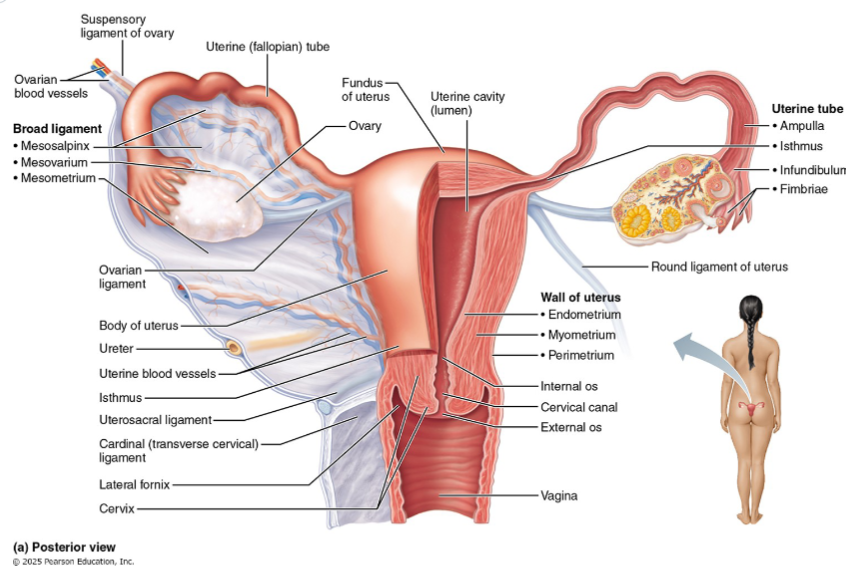
Uterus
Hollow, thick-walled, muscular organ; size and shape of an inverted pear
Location: pelvic cavity, anterior to rectum, posterosuperior to bladder
Position: usually anteverted (tilted forward over bladder); some women have retroverted uterus
4 regions of the uterus
from most superior to inferior
Fundus
Body
Isthmus
Cervix
Fundus of the uterus
Rounded superior portion above uterine tube entry points
Body of the uterus
Major portion of the uterus
Isthmus of the uterus
Narrowed region between body and cervix
Cervix of the uterus
Narrow inferior neck projecting into vagina
Consists of
Internal os: opening from cervix into uterine body
External os: opening from cervix into vagina
Cervical canal: between the two
Cervical glands: secrete thick mucus filling the canal → keeps uterus sterile
At mid-cycle (around ovulation): mucus becomes less viscous → permits sperm entry
Cervical cancer
HPV causes 99% of cases; Pap smear screening; HPV vaccination recommended ages 11-12
4 Ligaments that support the uterus
Mesometrium
Cardinal (transverse cervical ligaments)
Uterosacral ligaments
Round ligaments
Mesometrium ligament
Lateral support (part of broad ligament)
Cardinal (transverse cervical) ligaments
Cervix/upper vagina → lateral pelvic walls (strongest support)
Uterosacral ligaments
Cervix → sacrum (posteriorly)
Round ligaments
Uterus → anterior body wall (through inguinal canals to labia majora)
Peritoneal pouches
vesicouterine (bladder-uterus) and rectouterine (Douglas, rectum-uterus)
Primary support actually from pelvic diaphragm and muscles of deep perineal space
Uterine prolapse
damage to pelvic floor (e.g., childbirth) → uterus descends; cervix may protrude through vagina
3 layers of uterine wall
Perimetrium
Myometrium
Endometrium
Perimetrium layer of uterine wall
Outermost serous layer (visceral peritoneum) — incomplete
A structural covering
Myometrium
Thick middle layer; interlacing bundles of smooth muscle
what contracts during pregnancy and sometimes during menstruation
Endometrium
Inner mucosal lining; simple columnar epithelium + thick lamina propria with uterine glands
2 strata of the endometrium
Stratum Functionalis
Stratum Basalis
Functionalis
Superficial strata and is the disposable layer
Undergoes cyclic changes; proliferates under estrogen; secretory under progesterone; shed during menstruation
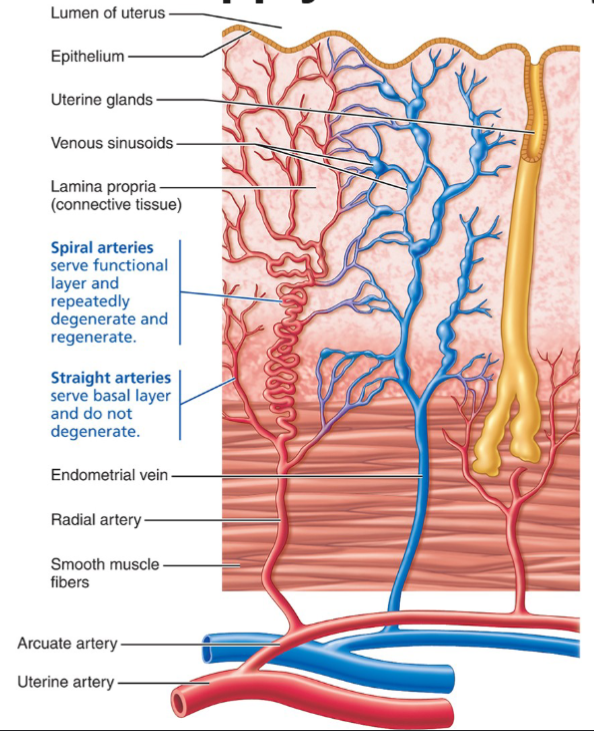
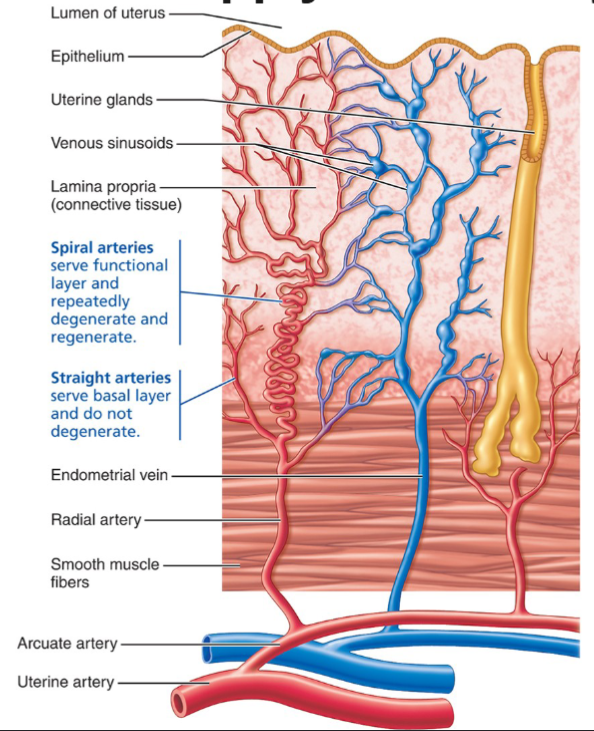
Vascularized by spiral (coiled) arteries
degenerate and regenerate each cycle because they spasm
Basalis
Deep thin strata(permanent, regenerative layer)
Does NOT shed during menstruation; contains stem cells that regenerate the functionalis after menstruation
Vascularized by Straight arteries
stable, do NOT degenerate because they don’t spasm
Vascular key to menstruation
Uterine arteries → arcuate arteries (in myometrium) → radial arteries (into endometrium) → branch into:
Straight arteries → supply basalis (stable)
Spiral arteries → supply functionalis (cycle-dependent)
When progesterone drops at the end of the cycle → spiral arteries spasm → ischemia → functionalis dies and sloughs off = menstruation
Straight arteries are unaffected → basalis survives → regeneration begins under rising estrogen
Vagina
Thin-walled, distensible tube; 8-10 cm long
Location: between bladder (anterior) and rectum (posterior)
No glands — lubrication from cervical mucous glands + interstitial fluid seeping across vaginal epithelium
Acidic pH: epithelial cells store glycogen → shed → metabolized to lactic acid by resident bacteria (Lactobacillus) → protects against infection but hostile to sperm (semen’s alkaline pH buffers this)
Hymen: incomplete partition of mucosa near vaginal orifice; anatomically variable
Vaginal fornix: recess where upper vagina surrounds cervix (posterior fornix deepest)
3 functions of the vagina
Receives penis and semen during intercourse
Passageway for menstrual flow
Birth canal
Wall structure of the vagina
Adventitia (outer layer)
Fibroelastic CT
Muscularis (middle layer)
Smooth muscle
Mucosa (inner layer)
Transverse ridges (rugae)
Stratified squamous epithelium (friction-resistant)
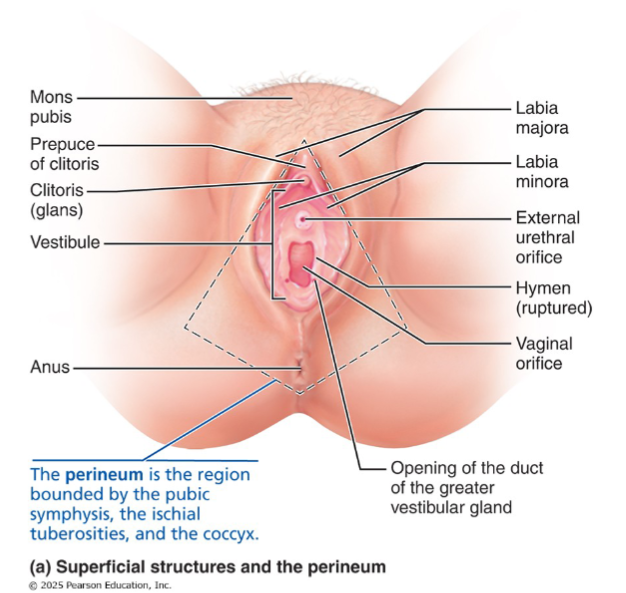
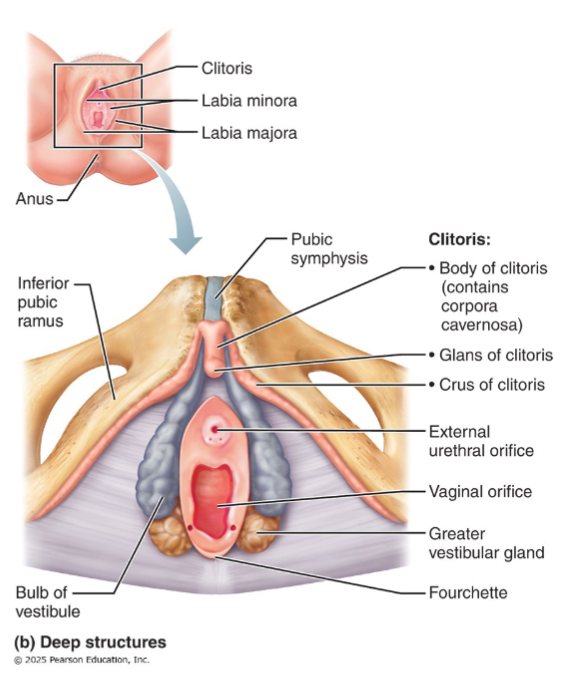
External genitalia (vulva)
Everything external to the vagina, collectively called the vulva:
Mons pubis
Labia majora
Labia minora
Vestibule
Greater vestibular glands
Clitoris
Bulbs of the vestibule
Fourchette
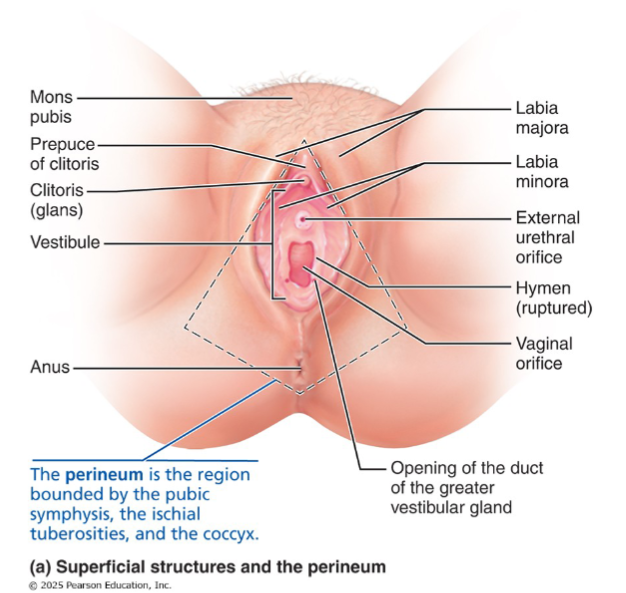
Mons pubis
Fatty mound overlying pubic symphysis; hair-covered after puberty
Labia majora
Elongated, hair-covered fatty skin folds
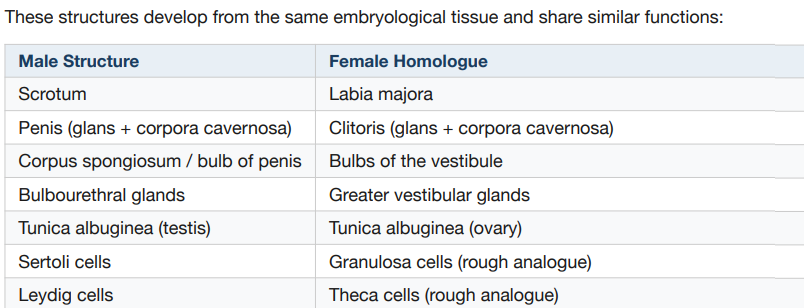
Male homologue= scrotum
Labia minora
Thin, hair-free skin folds enclosed by labia majora
Ventral penile skin (penile raphe)
Vestibule
Recess within labia minora; contains urethral orifice + vaginal orifice
Greater vestibular glands
Flank vaginal opening; secrete lubricating mucus
Male homologue= bulbourethral glands
Clitoris
Erectile tissue; only glans exposed; paired corpora cavernosa;
richly innervated
Male homologue= penis
Only the glans is visible externally; the body extends internally
Contains paired corpora cavernosa (no corpus spongiosum)
Hooded by prepuce (formed by anterior junction of labia minora)
Richly innervated; engorges with blood during arousal
Bulbs of the vestibule
Erectile tissue flanking vagina, deep to muscles
Male homologue= corpus spongiosum/ bulb of penis
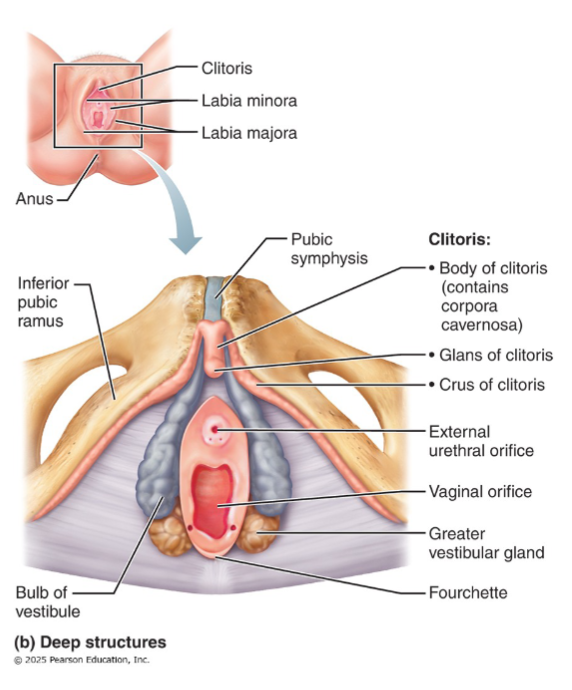
Fourchette
Ridge where labia minora joins posteriorly
Perineum of vulva
diamond-shaped region between pubic symphysis, ischial tuberosities, and coccyx.
Divided into 2 triangles
urogenital triangle (anterior): contains external genitalia + urethral opening
anal triangle (posterior): contains anal opening
Same organization as male perineum
Homologues summary
Why does breast size not correlate with milk production
Pre-lactation breast size reflects adipose content, not glandular tissue. Milk production capacity is similar regardless of breast size