Chapter 20-30
1/113
Earn XP
Description and Tags
20, 21, 22, 23, 24, 25, 29, 30, 26, 27, 28
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
114 Terms
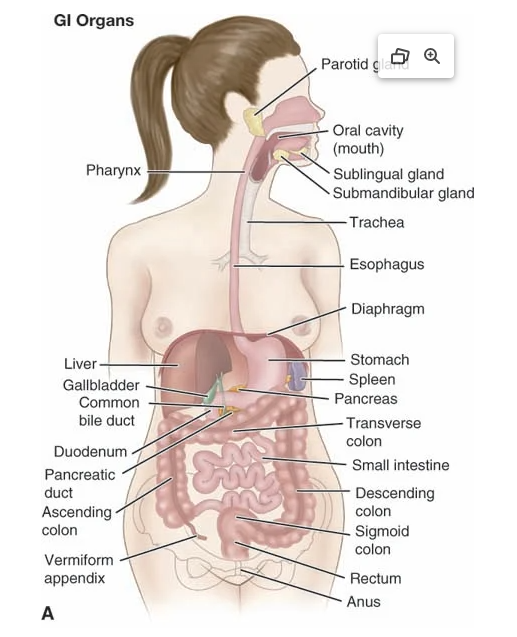
Anatomical Landmarks (GI):
Acscending colon: runs from right to transverse across epigastric area → L descending colon → sigmoid → rectum
Reference Lines:
Use either/or
Most common is 4 quadrants
Now where abdominal organs is in both 4 & 9!!
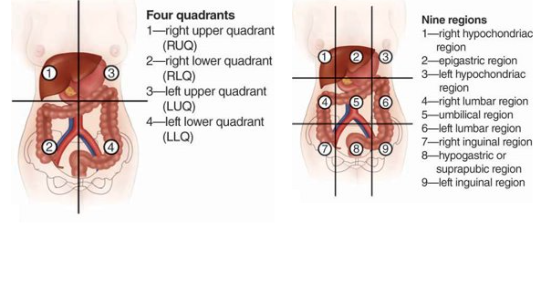
Diverticulitis
Inflammation of Diverticulum within colon
Common Location: Left lower quadrant (LLQ) of abdomen.
Key Symptoms:
Severe LLQ abdominal pain
Nausea and vomiting
Diminished bowel sounds
History of chronic constipation
Fevers/Chills
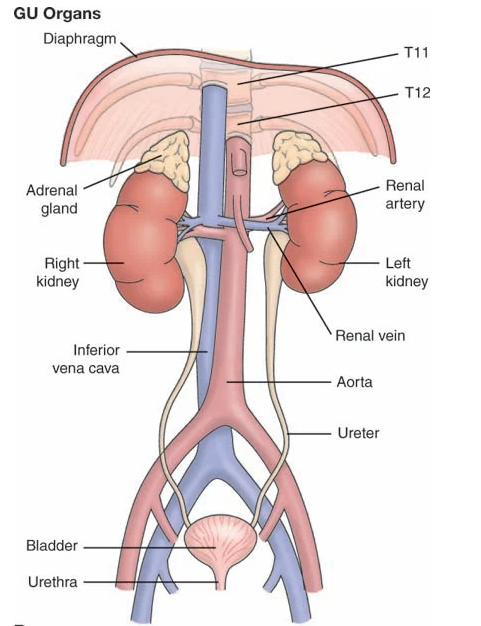
GU organs:
Auscultating lower aorta/iliac/femoral arteries → check for turbulent blood flow or plaque buildup
Spleen
LUQ organ; very vascular
Stores RBCs & platelets
Produces RBCs & macrophages
Activates B & T lymphocytes
Trauma/MVA → rupture → hemorrhage
Abdominal Organs:
Kidneys: controls BP through renin
Erythropoietin -> RBC making
Peritoneum: abdominal cavity; covers & holds organs
Parietal layers; serous membrane
Ex: parietal pleural, pericardium
Tumor can affect it -> a lot of fluid -> compresses organs
Causes ascites (liver cancer)/peritonitis
Mesentery: fanlike structure; from dorsal aorta, supplies blood vessels & nerves to intestines
Ingestion & Digestion
Mechanical digestion: chewing, peristalsis, churning
Chemical digestion: breakdown via HCl, enzymes, hormones
Begins in mouth – food + saliva → bolus
Bolus → oropharynx → esophagus → stomach (peristalsis)
In stomach: bolus + digestive juices + HCl → chyme
Absorption & Elimination
Occurs mainly in small intestine
Duodenum: receives bile + pancreatic juices
Jejunum & ileum: villi absorb nutrients
Undigested food → large intestine
Water & electrolytes absorbed
Remaining waste → feces, excreted in ~48 hrs
Absorption problem with Older Adults:
↓ Saliva & stomach acid → trouble swallowing, digesting, absorbing
↓ Motility & peristalsis → bloating, distention, constipation
Dental changes → painful chewing → diet shift (↓ protein, ↑ carbs)
↓ Muscle mass/tone → worsens constipation
Less pain perception → vague, diffuse abdominal symptoms
Common w/appendicitis → vaguer type of pain
Fat accumulation in lower abdomen → harder physical assessment
Liver: smaller, ↓ function → slower med metabolism → lower dosage
Kidneys: ↓ function → ↓ med elimination → lower dosage
Combined ↓ liver/renal function → lower med effectiveness
↓ Thirst sensation → ↓ fluid intake → ↑ risk for UTIs & constipation
Cultural Variations with Abdominal issues:
African Americans & Hispanic: ↑ sickle cell anemia, G6PD deficiency, lactose intolerance
Sickle cell → splenomegaly, jaundice, abdominal pain, vomiting
Chronic liver disease: leading cause of death in African Americans & Hispanics
Linked to alcoholism, obesity, hepatitis B/C
Obesity (central): fat accumulates in liver -> compresses -> get rids of healthy cells -> take over -> cirrhosis
African Americans: highest hepatitis B rate & higher mortality from hepatitis B/C
Priority Urgent Assessment for Abdomen:
Acute abdominal pain may signal ruptured appendix or diverticula → emergency surgery
Ruptured appendix, rupture abdomen, ruptured fallopian/ ovarian cyst
Nauses, fever, vomiting, dehydrated
Can lead to severe bleeding -> hypovolemic shock
Coffee Ground emesis: trauma, accident
Upper GI; digested blood
Careful with palpation
Bright red blood: Upper GI
Watch out to not rupture spleen when palpating
Esophagus, ruptured ulcer
Colon Bright red blood: → lower GI bleed or hemorrhoids
Black Tarry stool: comes from above (partially digested blood) to -> rectum
Risk factors for Abdominal issues:
s/s of Dehydration:
Vomiting, nauses, no eating, tachycardic, low blood volume, low BP, fatigue, diaphoresis, syncope
Altered mental status, DIZZY
Unintentional Weight loss: never normal
stress, difficulty with ingestion, socioeconomic issues, age-related issues, or dementia.
Anorexia Nervosa
Chronic anti-inflammatories (Advil, Aleve, Ibuprofen): irritate GI tract → inhibit COX enzyme → erosion → gastric ulcers → may cause upper GI bleeding
.
Constipation:
Change from expected pattern
Often due to low fiber/fluid intake or medications (anticholinergics, narcotics)
Assess for diet, meds, activity changes
Diarrhea:
Causes include infection (e.g., C. difficile), food intolerances, or medication side effects
Hidden allergies: gluten & lactose intolerance → GI distress
Past abdominal/pelvic surgery: may cause scarring/adhesions → bowel obstruction → use rest, IV, NPO, surgery
Excessive alcohol: damages GI lining & liver
Lower caloric intake
Recent travel: risk for Hepatitis A (spread via fecal-oral route)
Temporary
Teaching & Health promotion for GI:
Colorectal cancer: 2nd leading cause of death
>45 years
Stool DNA (sDNA) → every 3 yrs
Colonoscopy → every 10 yrs
Hepatitis
Hep A: fecal-oral, more severe in adults, usually resolves <1 yr
Hep B/C: blood/body fluids; can cause chronic disease
Hep B: perinatal transmission common, complications → cirrhosis, cancer; preventable with vaccine
Hep C: high-risk groups → healthcare, IV drug use, penile-anal intercourse; no vaccine; chronic in >50% → fibrosis, cirrhosis, liver cancer
Immunizations:
Hep B at birth
Hep A at 12 months
At-risk adults (blood exposure, travel, healthcare, food services, sex workers)
Common Symptoms related to GI:
Indigestion
Anorexia
nervosa: on purpose
Nausea, vomiting, hematemesis
Abdominal pain
Dysphagia
Odynophagia: pain w/swallowing
Stress, obstruction, GERD, infection, tumor
Constipation
V fluid, fiber, meds, irritable bowel syndrome (from stress)
Diarrhea: C-diff, Stress, food intolerance
CVA; pain = UTI is high up
dysuria, hematuria
r/x for Pyelonephritis
use ulnar edge of the forearm → percuss
Ureteral colic: kidney stones
High pain meds
Immense pain
GI Disorders:
G6PD: low enzyme for RBC making -> anemia
aspirin meds -> hemolysis
Thalassemias: hereditary hypochromic anemias; often confused with iron-deficiency anemia or lead poisoning; do not respond to iron; may show minor pallor & splenomegaly
Lactose intolerance: familial; can develop any age; abdominal discomfort, bloating, belching, diarrhea
Abdominal Assessment:
Preparation:
Warm, private environment; adequate lighting
Patient empties bladder, lies supine, arms at sides
Explain procedure, assess slowly & systematically
Examine painful areas last to avoid muscle guarding
Clinical Significance:
Assessment order: Inspection → Auscultation → Percussion → Palpation
percussion/palpation before auscultation can alter bowel sounds
Inspection: urine, emesis, stool
Auscultation: bowel sounds, vascular sounds
Percussion: kidneys, liver, spleen, bladder
Palpation:
Light palpation
Deep palpation: liver, spleen, kidneys, abdominal aorta, bladder, lymph nodes
Specific things to look at when assessing abdomen:
Cirrhosis
Liver flat edge, enlarged
Bruit
Heard above obstruction
Indicates partial or complete vascular obstruction
Obstruction Assessment
OLDCARTS for symptom analysis
NPO if obstruction suspected → prevents vomiting
No bowel sounds: suggests obstruction
High-pitched bowel sounds in upper regions → early obstruction
CT scan often used for diagnosis
Provider manages care and orders tests/interventions
Most common issues: vomiting, constipation, abdominal distention
Advanced Abdominal Assessment
Bladder Scan
Measures bladder volume & emptying; guides need for catheterization
Male setting if hysterectomy
>600 ml without voiding: abnormal
>200 ml post-void: suggests incomplete emptying
Abdominal Reflex
Superficial cutaneous reflex: stroke abdomen toward umbilicus in all quadrants
Absent in upper/lower motor neuron disease
Ascites Assessment
Detectable after ≥500 ml fluid
Common in cirrhosis or liver tumors
Shifting dullness: percuss supine → lateral positions; dullness moves to dependent area
Fluid wave: patient’s hand midline; tap one side, palpate other for transmitted wave
Peritoneal Irritation
Blumberg sign (rebound tenderness): press 90° and release quickly
Pain on release: peritoneal irritation/peritonitis (appendicitis)
Normal: no pain
Cough test: localized tenderness → peritoneal irritation
Gallbladder Inflammation
Murphy sign: fingers beneath liver border, patient inhales deeply
Positive: sharp pain + inspiratory arrest → cholecystitis
Negative: no pain
Appendicitis
Iliopsoas test: (PSOAS) supine, lift right leg, push down on lower thigh while patient resists
Pain: RLQ, indicates inflamed/perforated appendix
Rovsing:
Test for appendicitis
Press on left lower abdomen, then release
Pain felt in right lower quadrant → positive sign
Bruits
Swishing sounds → turbulent blood flow from vessel constriction or dilation
Hepatic area bruit: may indicate liver cancer or alcoholic hepatitis
Aorta or renal artery bruit: suggests partial obstruction
From smokers & diabetics
GI Diagnostics:
Basic Metabolic Panel (BMP): electrolytes, kidney function, acid-base status
Liver Function Tests (LFTs): assess liver health and damage
H. pylori:
Bacteria that thrives in stomach acids
Causes gastritis, reflux, ulcers
Breath test: detects presence of bacteria
Endoscopy (EGD): can biopsy tissue
Barium Enema: imaging of colon/rectum
Outlines large intestine using barium sulfate
Detects IBD or colon cancer
Colonoscopy: visualizes colon; can biopsy/remove polyps
Assesses colon & rectum, detects polyps, ulcers, tumors
Conscious sedation, scope passed through rectum
ERCP: Evaluates liver & pancreatic ducts, removes gallstones, diagnoses pancreatic cancer
CT Scan / MRI: detailed imaging of abdominal organs
Bones
Living structure: organic matrix + calcium phosphate
206 bones (excluding teeth & small cartilage bones)
Bone types:
Compact bone: shaft & outer layer
Spongy/cancellous bone: ends & center
Shapes: short, flat, irregular, long
Long bones: hollow tube of compact bone, ends = cancellous bone
Growth: lengthen at epiphyses
Functions:
Framework & protection
Mineral storage: calcium, phosphate
Bone marrow: hematopoiesis (blood cell production)
Muscles:
Three types: cardiac, smooth, skeletal
Skeletal muscles: 600 in body; voluntary
Structure: fibers in bundles → attached to bone by tendons
Functions:
Force & movement
Body shape
Heat production during activity
Connective tissue: supports, structures, binds body together
Joints
Definition: where two bones meet; provide mobility
Types by cartilage:
Fibrous (synarthrotic): immovable (e.g., cranial sutures)
Cartilaginous (amphiarthrotic): slightly movable (e.g., costal cartilage, symphysis pubis)
Synovial (diarthrotic): freely movable; major movements:
Ball & socket: hip, shoulder
Hinge: elbow, knee
Pivot: atlas/axis
Condyloid: wrist
Saddle: thumb
Gliding: intravertebral
Joint Real Examples (Read Over):
Temporomandibular Joint (TMJ)
Mandible + temporal bone
Movements: open/close, protrusion/retraction, side-to-side
Palpable: below & anterior to tragus of ear
Shoulder
Humerus + glenoid fossa of scapula (ball-and-socket)
Stability: rotator cuff muscles & tendons
Protection: bursa
Landmarks: acromion, greater tubercle, coracoid process
Elbow
Humerus + radius + ulna (hinge)
Movement: flexion/extension; pronation/supination
Landmarks: olecranon, medial/lateral epicondyles; ulnar nerve (“funny bone”)
Bursa: between olecranon & skin
Wrist & Hand
Wrist (radiocarpal): radius + carpal row (condyloid) → flexion/extension, deviation
Midcarpal: flexion, extension, some rotation
Fingers: metacarpophalangeal & interphalangeal joints → flexion, extension, abduction
Hip
Acetabulum + femur head (ball-and-socket)
Stability: muscles, ligaments, fibrous capsule, femur insertion
Bursae: 3 facilitate movement
Knee
Femur + tibia + patella
Structures: medial/lateral menisci, cruciate ligaments, collateral ligaments, bursae
Palpable landmarks: tibial tuberosity, medial/lateral condyles, patella, femoral epicondyles
Ankle & Foot
Ankle (tibiotalar): tibia + fibula + talus (hinge) → dorsiflexion, plantar flexion
Stability: medial/lateral malleoli & ligaments
Subtalar: inversion/eversion
Weight distribution: metatarsal heads & calcaneus via longitudinal arch
Toes: metatarsophalangeal & interphalangeal joints → flexion, extension, abduction
Spine
33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, 3–4 coccygeal
Intervertebral disks: cushion vertebrae
Palpable landmarks: C7/T1, inferior scapula (T7–T8), iliac crest line (L4)
Curves: cervical & lumbar = concave; thoracic & sacrococcygeal = convex
Functions: absorb shock
Abnormal postures: kyphosis, scoliosis, lordosis
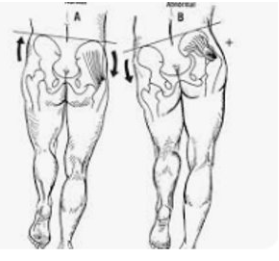
Trendelenburg Sign
Test for: congenital hip dislocation or hip abductor weakness
Positive sign: hip drops on the side opposite the stance leg or in babies, leg elevates when standing/walking
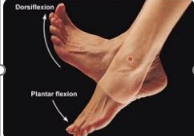
Dorsiflexion & Plantarlexion
Dorsiflexion: Bending the ankle so that the toes move toward the head
Plantar flexion: Moving the foot so that the toes move away from the head
Musculoskeletal Changes with Aging
Bone: osteoporosis = resorption > deposition; rapid loss post-menopause; risk: small frame, smoking, low calcium, alcohol, inactivity; teach: weight-bearing exercise, fall prevention
Bony prominences: more visible → skin breakdown; nursing: reduce pressure
Cartilage: degenerates → stiffness; nursing: warm baths before activity
Joints/ligaments: stiff, lax → ↓ROM; nursing: active ROM, assistive devices for ADLs
Muscle: atrophy → ↓strength after 30, worse after 60; nursing: isometric exercises, nutrition
Posture/spine: height loss (disks & osteoporosis); kyphosis
Fat: ↑abdomen/hips after 40; ↓subcutaneous fat after 80 → prominent bones
Cultural Variations & Health Disparities – Musculoskeletal System
Bone density: more related to BMI & physical activity than genetics
Femur Curvuture
Sex & hormones: testosterone → larger/stronger bones; estrogen ↓ post-menopause → rapid bone loss (≈20% in 5–7 yrs); white women at highest osteoporosis risk
Work risks: heavy lifting → back strain; physically demanding jobs → sprains/strains/fractures; repetitive motion → carpal tunnel, pitcher’s elbow, vertebral degeneration; poor desk ergonomics → musculoskeletal injuries
Musculoskeletal Assessment
Inspection: limb/joint/spine alignment; symmetry in size, shape, position, movement
Swelling/tenderness: → likely strain or sprain
Bone/joint misalignment: bone → fracture; joint → dislocation
Safety: do not attempt to realign; immobilize and keep patient calm
Soft-tissue injury: check swelling, pain, numbness, bleeding; apply pressure if needed; monitor distal pulses, color, temp, capillary refill
GALS screen: gait, arms, legs, spine; 11 tasks + ask about pain/stiffness and difficulty with ADLs (washing, dressing, climbing stairs)
Vital signs, monitoring pulses, assessingcolor, temperature, capillary refill distal toinjury
Neurovascular Test:
Checking for the "5 P's": pain, pallor (color), pulses, paresthesia (sensation/tingling), and paralysis (motor function), along with capillary refill time (<2 secs) and temperature.
Priority assessment btw
R/x for Musculoskeletal issues:
Osteoporosis, RA, OA,
Any high repetitive motion
Use of hands drills, carpal tunnel syndrome, trigger finger
Asks ab complain
Knee, foot, feet (runners)
Musculoskeletal Teaching & Health Promotion
Health History: identify areas needing teaching; link to Healthy People 2030 goals:
↑ osteoporosis screening
↓ hip fractures
↑ physical activity in adults with health problems
Functional Assessment: use Short Musculoskeletal Function Assessment (SMFA)
Lifestyle Recommendations:
Maintain healthy weight
Weight-bearing exercise ≥3x/week
Alternate shoulder bag or use backpack → prevent scoliosis
Use proper body mechanics, protective equipment, seat belts
Exercises to improve strength, flexibility, posture → ↓ fall risk
Bone Density & Osteoporosis:
Calcium + vitamin D important for all ages
Preventive measures: active lifestyle, weight-bearing exercises, joint protection, limit caffeine, discuss risk with provider, bone density test, medications if needed (bisphosphonates, calcitonin, HRT, raloxifene, parathyroid hormone)
Weight-bearing exercise crucial after 30 to prevent bone loss and muscle wasting; walking preferred
Scoliosis Screening (more on females):
Lateral curvature of spine; structural or functional
Early detection in adolescence prevents progression
Severe cases → breathing interference
Screen via hip, scapula, shoulder symmetry; forward bend test
Older adults may present undiagnosed cases
Common musculoskeletal symptoms
Pain/Discomfort: Myalgia (muscle pain), Arthralgia (joint pain)
Weakness: Reduced strength or fatigue
Stiffness / Limited Movement: Contractures or reduced range of motion
Deformity: Visible bone or joint abnormality
Balance & Coordination Issues: Ataxia (unsteady gait, falls)
Crepitus: Crackling or popping in joints (common in shoulder, knee)
Overuse of joint or OA
Specific Joint Deformities
Genu Valgum (“knock knees”): Knees angle inward; medial sides touch, lateral sides apart
diagnosed during school-aged
Genu Varum (“bow-legged”): Knees angle outward; lateral sides apart, medial sides do not touch
Both cause chronic knee pain in the future
musculoskeletal assessment equipment
Goniometer: Measures joint angles and range of motion (ROM)
Tape Measure: Measures limb length, circumference, or deformities
Romberg Test:
Assesses balance and proprioception (sensory input from joints/muscles)
Procedure:
Have patient stand with feet together, arms at sides.
Observe balance with eyes open, then eyes closed for 20–30 seconds.
Initial Musculoskeletal Survey:
Posture: Look for alignment of head, spine, shoulders, and hips.
Gait & Mobility: Observe walking patterns; note any limping, shuffling, or wide-based steps.
Ataxic gait: Uncoordinated, unsteady walking → may indicate cerebellar or sensory deficits.
Balance & Coordination:
Tests: Romberg, heel-to-toe walking, finger-to-nose.
Extremities: Inspect and palpate for deformities, swelling, tenderness, or asymmetry.
Joints & Spine:
Inspect, palpate, assess ROM and muscle strength of each joint and spine.
Fall-Risk Assessment
Tools: Morse Fall Scale, Hendrich II Fall Risk Model
Interventions for high-risk patients:
Encourage supervised walking in the hallway
Provide assistive devices like walkers
Monitor closely for repeated falls
Musculoskeletal Lab Tests:
Muscle Injury:
Creatine kinase (CK), lactate dehydrogenase (LDH), ALT, AST → indicate muscle damage.
Bone Damage:
Alkaline phosphatase → elevated with bone turnover or injury.
Inflammation:
ESR, C-reactive protein (CRP), rheumatoid factor → elevated in rheumatoid arthritis, lupus, and other inflammatory conditions.
Gout:
Uric acid → elevated in gouty arthritis.
X-ray: Detects bone fractures; limited for soft tissue.
CT scan: Shows bone and soft-tissue structures; more detailed than X-ray.
MRI: Most sensitive for soft-tissue injuries (ligaments, tendons) and stress fractures.
Bone Density Scan (DEXA): Assesses osteoporosis risk and fracture susceptibility.
(Musculoskeletal injuries are most painful post-op)
A lot of blood transfusions from bone marrow being taken out
Brain:
Neuron structure: cell body (control center), dendrites (receive impulses), axon (transmits impulses).
Gray matter: cell bodies (outer cortex).
White matter: axons (inner brain tissue).
Synapses: spaces between neurons for communication.
Cerebrum:
Cerebrum:
Two hemispheres:
Left: language, logic, math.
Right: spatial, creative, emotional.
Cerebral cortex: controls motor, sensory, intellect, and language.
Lobes and functions:
Frontal: cognition, personality, motor control, Broca’s area (speech).
Precentral gyrus: Motor control (opposite side of body)
Parietal: sensory perception, size/shape recognition.
Temporal: hearing, memory, behavior, Wernicke’s area (language comprehension).
Postcentral gyrus: Sensory input (temp, touch, pressure, pain) from opposite side
Occipital: vision and visual interpretation.
Limbic (5th lobe): emotion, memory, survival behaviors.
Basal ganglia: modulate automatic movements.
Thalamus: sensory/motor relay.
Hypothalamus: autonomic control (temp, HR, BP, hormones, sleep).
Limbic system: emotions, fear, aggression, affection.
Aphasia Types:
Stroke in right brain → left-sided deficits.
Stroke in left brain → right-sided deficits + language problems.
Wernicke damage: receptive aphasia (can’t understand).
Broca damage: expressive aphasia (can’t speak).
Global aphasia: both receptive + expressive.
Cerebellum:
Coordinates voluntary movement, posture, muscle tone, and balance
Ensures smooth, balanced movement through connections with motor cortex & brainstem
Alcohol impairs cerebellum → loss of balance and coordination
Cerebellum Ataxia: very impaired coordination; bad Romberg performance
Cerebellar Ataxia:
Cause: Cerebral palsy or alcohol intake
Characteristics: Wide-based gait, staggers and lurches side to side, unable to perform Romberg test due to trunk swaying
Reason: Cerebellar dysfunction → poor balance and coordination
Brain Stem
Connects brain and spinal cord; controls vital reflexes.
Components: midbrain, pons, medulla, reticular formation.
Functions:
Medulla: cardiac, respiratory, and vasomotor control; reflexes (swallowing, coughing, sneezing, vomiting).
Pons: regulates breathing rhythm with medulla.
Reticular Formation: Relays sensory info and provides excitatory/inhibitory control to spinal motor neurons
wakefulness, attention, and cortical responsiveness
Cranial nerves III–XII originate here.
Brain Protection:
Protection: Skull and meninges cover the brain
Ventricles & CSF: Fluid-filled cavities circulate cerebrospinal fluid around brain, brainstem, and spinal cord
Cushions brain, carries nutrients, allows fluid shifts
↑CSF pressure → brain herniation → brainstem compression → impaired breathing, ↓LOC, possible death
Spinal Cord:
Extends from brainstem → coccyx
Gray matter (H-shaped, center) = cell bodies: voluntary & autonomic motor neurons, sensory neurons
White matter (surrounds gray) = axons in ascending & descending tracts
Cells Aligned
Ascending Tracts (Sensory):
Dorsal/posterior columns → localized touch, deep pressure, vibration, proprioception, movement → synapse in medulla → cross → sensory cortex
Descending Tracts (Motor)
Motor function & muscle movement (voluntary)
Cranial Nerves:
I. Olfactory (Sensory): Smell & interpretation (stimulates peristalsis, salivation, sexual response).
II. Optic (Sensory): Vision — acuity & peripheral.
III. Oculomotor (Motor): Eye movement (up, medial, down, up/in), raises eyelid, pupil constriction.
IV. Trochlear (Motor): Eye movement — down & in.
V. Trigeminal (Sensory + Motor):
• Ophthalmic — cornea, forehead, nose.
• Maxillary — cheeks, upper jaw, teeth.
• Mandibular — lower jaw sensation & chewing.VI. Abducens (Motor): Lateral eye movement.
VII. Facial (Sensory + Motor): Taste (ant. ⅔ tongue), facial expression, salivary & lacrimal glands.
Bells palsy: unable to wrinkle forehead
VIII. Acoustic / Vestibulocochlear (Sensory): Hearing & balance (cochlear + vestibular fibers).
IX. Glossopharyngeal (Sensory + Motor): Taste (post. ⅓ tongue), swallowing, speech, parotid secretion, sensation (ear & pharynx).
X. Vagus (Sensory + Motor): Parasympathetic control — digestion, defecation, ↓HR, speech & swallowing.
XI. Spinal Accessory (Motor): Swallowing, speech, shoulder shrug, head turn.
XII. Hypoglossal (Motor): Tongue movement.
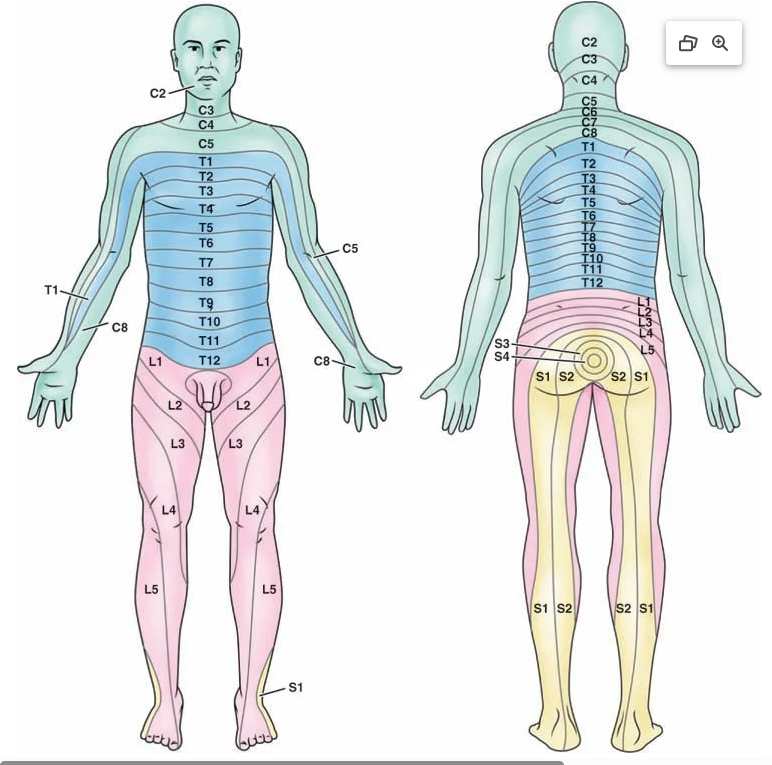
Spinal Nerves:
Arise from: Spinal cord → innervate rest of body.
Composition:
• Afferent (sensory) fibers → dorsal root.
• Efferent (motor) fibers → ventral root.
• Combined = spinal nerve.Total: 31 pairs
• 8 Cervical (C1–C8)
• 12 Thoracic (T1–T12)
• 5 Lumbar (L1–L5)
• 5 Sacral (S1–S5)
• 1 CoccygealDermatome: Skin area innervated by sensory fibers of a single spinal nerve.
Level of injury to the spinal cord affects function at and below the site of trauma
C1-C3: issues with movement of below neck
C4-C6: shoulder & diaphragm; Breathing
C7-C8: fingers & grasping, self care
T1-5: Trunk stability
T6-12: thoracic muscle & upper back → respiratory & transfer strengthL1-2: Legs & Pelvis
L3-L4: Ankle, hamstring
Function: Each level controls motor & sensory activity for specific body regions (head → toe).
Autonomic Nervous System:
Function: Maintains involuntary control of cardiac, smooth muscle, and glands → keeps homeostasis.
Divisions:
• Sympathetic (T1–L2) = “Fight or flight” → ↑ HR, BP, contractility. Neurotransmitter: Epinephrine & Norepinephrine.
• Parasympathetic (Brainstem & S2–S4) = “Rest & digest” → ↓ HR, promotes digestion. Neurotransmitter: Acetylcholine.Receptors:
• Chemoreceptors & Baroreceptors detect changes → trigger ANS response.
Reflexes:
Involuntary, protective responses → tone & posture.
Reflex Arc:
Receptor → Sensory neuron → Spinal cord → Motor neuron → Effector (muscle).Patellar reflex (knee jerk) → tests spinal reflex & muscle strength.
Types:
• Deep tendon (patellar)
• Superficial (corneal, abdominal)
• Visceral (pupillary light)
• Neonatal (rooting, grasp,Babinski (disappears before age of 2): feet go outward
Spinal cord/systematic nervous system injury
Older adults and issues with Nervous System:
Structural brain changes
↓ Brain volume due to neuron shrinkage & fewer synaptic spines/synapses.
Reduction in cognitive abilities
Risk for poor balance, postural hypotension, falls, injury
Light touch, pain sensation reduced
Ventricles enlarge → possible normal pressure hydrocephalus (ataxia, vision problems, gait issues, mild dementia, incontinence).
Peripheral neuropathy: symptom of smth else( Diabetes, B12 deficiency)
-Inspect feet everyday, SHOES,
-Be careful of heating pads
Cultural Variations Regarding Nervous System:
Stroke Risk:
• African Americans = 2× higher death rate (↑ BP, obesity, diabetes, smoking).
• Hispanics & Native Americans = ↑ risk; Asian Americans = ↓ risk.
• Many delay care or stop treatment early → poorer outcomes.Post-Stroke Functional Limitations:
• More common in African Americans & Hispanics.
• Recovery depends on therapy access & support systems.
Priority Urgent Assessment related to Nervous system:
🧠 Acute mental change → restlessness, agitation, confusion
CHECK FOR BASELINE FIRST
😴 ↓ LOC → harder to arouse, unresponsive (not drug-related)
⚡ Seizures
💪 Posturing:
• Flexor (decorticate) – arms flexed, legs extended
• Extensor (decerebrate) – arms/legs extended, plantar flexion👁 Pupil change → size or reactivity altered (one is fixed) BAD PERRLA
👀 Eye deviation (conjugate/dysconjugate)
🦵 Progressive weakness/paralysis (watch for facial droop)
✋ Sensory loss
❤ Vital sign changes:
• ↑/↓ BP → risk of hemorrhage or infarct
• Irregular HR/rhythm (e.g., Afib → emboli/stroke)
• Fever → infection, autonomic dysfunction
• Cushing’s Triad (↑ BP + ↓ pulse + ↓ respirations) → ↑ ICP
• Irregular breathing → brainstem compression
Rapid Acute Neuro Exams:
LOC (Glasgow Coma Scale)
Eye Opening (4): Spontaneous → Voice → Pain → None
Verbal (5): Oriented → Confused → Inappropriate → Incomprehensible → None
Motor (6): Obeys → Localizes → Withdraws → Flexion → Extension → None
Score range: 3 (coma) – 15 (normal)
If <8 → intubation
Pupils: Check size, symmetry, & light response
Motor Strength: Lift each limb vs. gravity & resistance
Face: Check for asymmetry at rest & with movement
Sensation: Light touch on limbs & face (if communicative)
CNs (if ↓ consciousness): EOMs, gag reflex, corneal reflex
Vitals: Monitor for cause/result of neuro change
Act F.A.S.T. for strokes → tissue necrosis → death
-Sudden severe headaches with no cough; blurry vision,
-Cautious with ppl how take blood thinners
Assessment of Risk factors:
Check for past medical history; head-spinal trauma
Chronic Conditions:
Meningitis: fever, stiff neck, drowsiness, photosensitivity
Multiple sclerosis (MS)/Degenerative: weakness, tingling, vision difficulty, elimination issues
Parkinson’s
Infections:
Meningitis
Spider
Ticks → lyme disease
Snakes
Stroke History:
Pts with history may stay with s/s of strokes → not urgent (X code)
Location of issue:
sudden loss of hearing → temporal
obstructive sleep apnea (OSA) → * risk for A fib → stroke
Multiple sclerosis: no known cause (AI)
Teaching & Health promotion for strokes:
Risk factors (modifiable):
Smoking 🚭
Dyslipidemia (high cholesterol)
Hypertension
Diabetes mellitus
Abdominal obesity
Psychosocial stress
Prevention strategies:
Control BP (healthy diet + prescribed meds)
Encourage smoking cessation
Eat low-saturated fat, high-fruit & veggie diet
Weight management & calorie reduction
Regular exercise (vigorous walking 30 min, 3–5×/week)
Chronic Neurological Conditions
Examples: MS, Parkinson’s, Alzheimer’s, ALS, Huntington’s, Epilepsy
Causes: genetic, viral, environmental, or lifestyle factors (often unknown)
Common Symptoms regarding Neuro System:
Headaches: make sure HPI is thorough
-location, quality, severity, progressively worse?
Localized weakness
Generalized weakness (MS)
Involuntary tremors
not all are parkinsons
stress
Balance/coordination issues
Dizziness/vertigo:
-benign paroxysmal vertigo
-may be Meniere disease
Swallowing issues: stroke/Parkinsons
Intellectual changes: Alzeihmeres
Speech/language difficulties
Changes in senses of taste, touch, or smell
Double blurred vision: X normal
Sudden hearing loss: X normal
-Tenitis: does not go away
CVA risk:
Increased age: 2x each decade after 55
Male
African Americans
HTN
Smoking
OSA: affects atrium -> poor conduction -> quiver -> A-fib -> clots are made -> travels to brain -> CVA
Make sure to do a sleep study!
3+ alcohol beverages/day
Equipment for Neurological Assessment:
Penlight or flashlight
Tongue blade
Cotton swab
Tuning fork: is for sensation feeling -> neuropathy risk
- Pt should stop feeling it when nurse does too
reflex hammer
Basic and Advanced Techniques: Neurological System
Dysarthria: slurred speech
Gag reflex; tests vagus for aspiration/swallow patterns
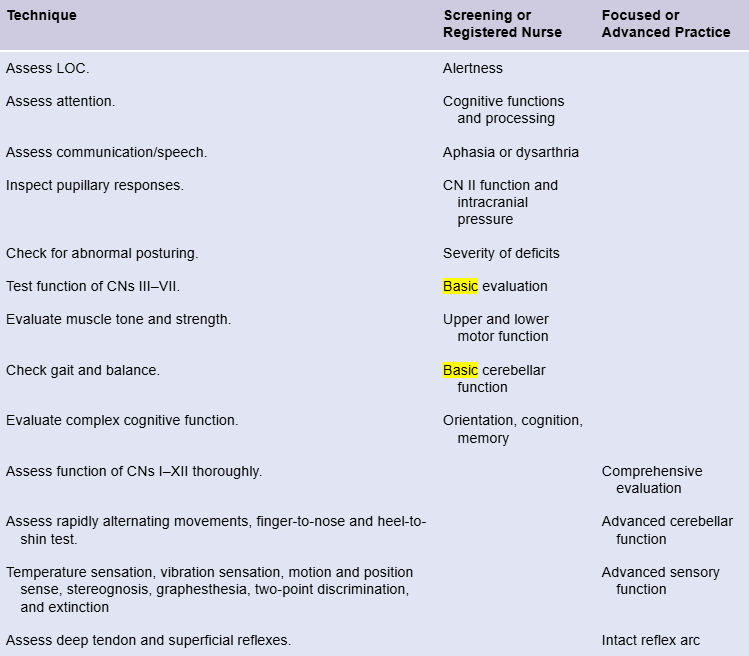
Neurological Assessment: Motor, Cerebellar, and Sensory Functions
1⃣ Motor Function
Assess: Muscle bulk & tone, muscle strength, balance.
Practical tests:
Squeeze nurse’s hands → checks hand grip strength.
Romberg test → patient stands feet together, eyes closed; swaying suggests proprioceptive/vestibular issues.
Abnormal findings: Atrophy, hypertrophy, flaccidity, spasticity, weakness.
2⃣ Cerebellar Function
Assess: Coordination and smoothness of movement.
Key terms:
Ataxia: Unsteady, uncoordinated movements.
Adiadochokinesia: Inability to perform rapid alternating movements.
Practical tests: Rapidly pronate/supinate hands, finger-to-nose test.
3⃣ Sensory Function
Basic senses: Light touch, superficial pain (pinprick).
Advanced senses (specialty/advanced practice):
Temperature sensation
Point localization → can patient identify touch location?
Vibration sensation → tuning fork
Motion/position sense (proprioception) → detect limb movement
Stereognosis: Identify object by touch alone
Graphesthesia: Recognize writing traced on skin
Two-point discrimination: Distinguish two points on skin
Extinction: Detect simultaneous touch on both sides
Practical test for stereognosis: Place a familiar object in patient’s hand.
Reflex Testing & Carotid Arteries Testing
Deep tendon reflexes, superficial reflexes
DTR: bicep, tricep, brachial reflex, patellar, achilles
0- none
1+- diminished
2+- normal
3+-brisk*
4+-Hyperractive, very brisk
Carotid Arteries: carries to brain
-Bruits
- Major cause of Syncopal episode (major cause is cardiac related)
Extra Neuro Assessments:
Meningeal signs for Meningtitis
inflammation, virus check
Brudzinski: flex hip
Lay them down -> flex neck -> significant pain
Kernig Sign: flexing legs at hips
Nuchal rigidity: stiff neck
Intercranial hemorrhage
Dolls eye maneuver:
Turning head to one side -> eyes move opposite way (intact brain stem)
If remain midline or move with head: severe brainstem injury/issue
Glasgow Coma Scale: 3-15; know table!
Eye opening response (4)
Best vertebral response (5)
Best motor response (6)
Labs related to Neuro
Angiography: Inject dye into vessel -> check for every vessels
Helps find very small strokes/aneurysm
EEG: electrical pole activity of brain
Lumbar puncture: collect CSF amount -> lab -> check for meningitis, virus & bacteria in it
Be careful when taking out -> too much = loss of cushion lubricant of spine
Lay them flat in bed due to severe headache
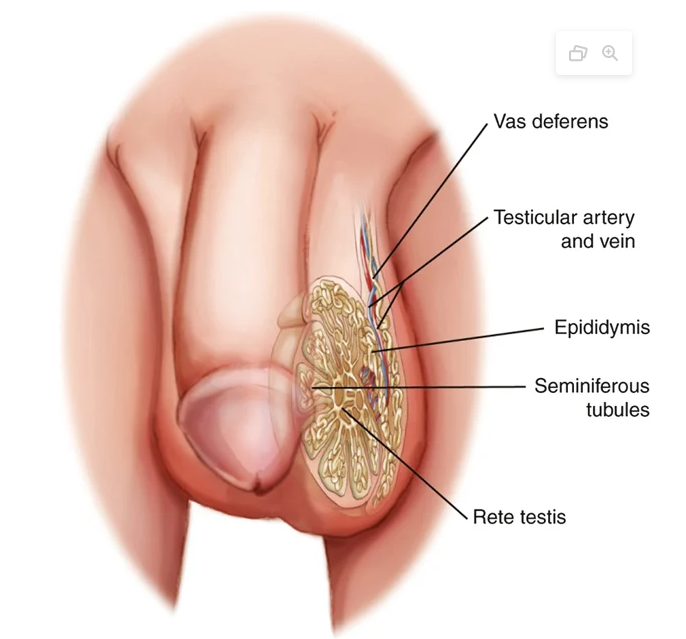
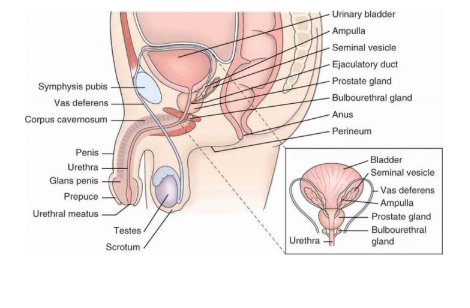
Testicles:
Production of sperm & testosterone
3.5°F (2°C) lower than core body temperature
Prepuce: Foreskin
Full bladder -> penile erection
Epididymis → Vas deferens → Ejaculatory duct → Urethra
Rete Testis: collect sperm from the seminiferous tubules and transport them into the epididymis via the efferent tubules.
Epididymis:.
Functions: storage, maturation, and transport of sperm.
Vas deferens (ductus deferens):
Transports sperm from epididymis to ejaculatory duct.
Along with arteries, veins, and nerves, forms the spermatic cord.
The spermatic cord ascends through the external inguinal ring → inguinal canal.
Joins the seminal vesicle before entering the prostate to form the ejaculatory duct.
Ejaculatory duct:
Passes through the prostate gland and opens into the posterior urethra.
Urethra:
Length: 18–20 cm (7–8 in.), from bladder to meatus.
Divided into three parts:
Posterior
Membranous
Cavernous (anterior)
Seminiferous Tubules
Located inside each testicle.
Consist of coiled ducts where spermatogenesis (sperm production) occurs.
Sperm maturation cycle: approximately every 90 days.
Erection:
Caused by psychogenic or local mechanisms.
Psychogenic erection: triggered by sensory input such as auditory, tactile, visual, or imaginative stimuli.
Local reflex erection: initiated by tactile stimulation.
A full bladder can also induce an erection.
Internal Genitalia, Rectum, Anal Canal,Anus (MEN)
Prostate is below bladder
Enlargement > 50 years
Provide privacy & comfort
Lifespan considerations regarding male genatalia:
Newborns & Infants
Circumcision is a family choice, not a medical requirement.
States that benefits outweigh risks based on:
↓ Urinary tract infections (UTIs)
↓ Ulcerative sexually transmitted infections (STIs)
Uncircumsized → ^ UTI (1st year of life)
Children & Adolescents
Tanner’s Stages of Maturation used to assess puberty and development.
Based on primary and secondary sexual characteristics (external changes).
Older Adults
Rectal changes:
Degeneration of afferent neurons → ↓ sensation of rectal fullness.
Reduced sphincter tone → possible fecal retention or incontinence.
Testosterone declines → ↓ libido and sexual function.
Testes drop lower in scrotum
Benign prostatic hyperplasia (BPH): too big -> obstruction for bladder -> necrosis
Some meds can v psi -> if not then surgery
Erectile Dysfunction: v libido/inability to ejaculate
Do not joke around duh
Piercings and tattoos
Transgender does not change the fact that they have a prostate
Priority Urgent Assessment for Male Genitea:
Torsion -> ischemia; young ppl; familial & can happen again with past torsions
Epididymitis → inflammation
Feature | Testicular Torsion | Epididymitis |
|---|---|---|
Pain onset | Acute, sudden | Gradual |
Nausea/Vomiting | Present in ~50% | Rare |
Fever | Rare | Present in ~50% |
Blue dot sign | Tender blue nodule on testis | Absent |
Voiding symptoms / discharge | Rare | Present in ~50% |
Urinalysis results | Abnormal in 0–30% | Diagnostic in 20–95% |
Relief with elevation | No relief | Pain lessens |
Treatment | Immediate surgery (urologic emergency) | Antibiotics (infection/inflammation) |
Fournier Gangrene:
Severe, rapidly spreading infection of perineal/genital tissue.
Often originates from perianal or retroperitoneal infection.
Common in diabetics.
Symptoms:
Pain, redness, swelling in perineum.
Progresses rapidly within hours.
Tenderness, induration, crepitus (gas pockets).
75% of hospital UTIs are catheter-associated (CAUTI).
Anorectal Disorders
Can cause pain, embarrassment, and delayed care.
Early detection = lower mortality.
Rectal bleeding (Hemorrhoids) → needs rapid assessment.
Colorectal cancer may mimic benign conditions → always investigate; adults
Subjective data collection regarding male genatalia
1. Past Medical History
Ask about chronic illnesses: diabetes, hypertension, neurological disorders, COPD, cardiovascular disease, depression.
→ ↑ Risk for ED, UTIs, epididymitis, proctitis.Age, Gender, Ethnicity
2. Medical & Surgical History
Ask about genitourinary surgeries: prostate, testicular cancer, torsion
Sexual behavior, condoms
Medications used -> erectile dysfunction
r/x for cancer
Sexual History – The “Five P’s”
Partners:
Ask number, gender identity, and new or multiple partners.
Include partner risk factors: injection drug use, known infections, or anonymous encounters.
Practices:
Ask about vaginal, oral, and anal sex (insertive/receptive), and use of sex toys or douching.
Protection:
Ask: “How do you protect yourself from STIs?”
Discuss condom use, testing frequency, and partner communication.
Past History of STIs:
Document specific infections, recurrence, and partner treatment.
Pregnancy Prevention:
Ask, “Are you trying to get pregnant?”
Identify contraceptive methods and family planning goals.
Opportunity to discuss HPV vaccination, HIV PrEP/PEP, and STI prevention.
Teaching & Health promotion regarding male genatalia
Self-examination: more common in young people
Establish a “baseline normal” and detect early testicular cancer.
Recommended monthly for individuals age ≥14 years.
Reduce the prostate cancer death rate.
Increase male participation in family planning and pregnancy prevention.
Increase condom use during last sexual intercourse.
Reduce infection rates of:
Hepatitis (A, B, C)
HIV
Chlamydia trachomatis
Gonorrhea
Family Planning: risk for pregnancy
-r/x for gonorrhea
-r/x for cyphils: primary, secondary, tertiary
primary → discharge ,fevers, rash → goes away → secondary → rash spreads to palm & feet → goes away → tertiary → last for years; lives in aortic valve → aortic rupture & other organ failures
-Trichomoniasis: STI; parasites
Women get green discharge, pelvic pain → ANAs
Viruses:
HPV: causes cervical (woman) cancer; different types/numbers; warts & other s/s
Males can get HPV in other places → oropharyngeal areas
Cancer, warts,
Prostate Cancer Screening: up with BPH & cancer
Ages 55–69 years:
Screening decision should be individualized after discussing risks and benefits.
Potential small benefit: may lower risk of death from prostate cancer
Digital Rectal Exam: Palpate prostate via rectum
- Checks for lumps, indurations, ffoggy?
Common s/s regarding male genatalia issues:
Pain
Difficulties with urination ← BPH
Red urine (hematuria) → infection, malignancy, trauma, or diet (red foods).
Cloudy urine → infection.
Erectile dysfunction (ED)
Curvature of penis during erection (Peyronie disease).
Penile lesions, discharge, rash
Associated pain, itching, burning, discharge, or odor.
Bloody penile discharge → urethritis or malignancy.
Pain with urine
Uncommon for >1yr patients to have UTIs
Scrotal enlargement
varicocele, hydrocele, hernia, epididymitis, tumor, or torsion.
Pain + enlargement → assume testicular torsion until ruled out (emergency).
Older adults
Cultural considerations
Males – Male sex: 1.6-2.3 times more likely → HIV
Higher risk for genital herpes & chiphylis: No use of protection
Comprehensive Physical Assessment regarding Male Genatelia:
Utilize inspection and palpation as appropriate
Groin
Penis
Hypospadias: urethral meatus on underside.
Epispadias: meatus on upper surface.
fixed w/surgery
Scrotum
Sacrococcygeal areas
Perineal area
Fournier gangrene: necrotic tissue or crepitus on palpation (diabetic risk).
Emergency requiring surgical evaluation.
Inguinal region and femoral areas
Inguinal areas: Hernia common -> incarceration (compressed) -> ischemia bowel -> necrosis of bowel part
Additional techniques:
Testicles
Vas deferens
Transillumination of the scrotum
Hydrocele: fluid-filled mass around testis; firm, transilluminates well.
Spermatocele: cystic mass above the testicle, transilluminates well.
Torsion of appendix testis: visible “blue dot sign” on upper pole of testis.
Solid masses (tumor, hernia) do not transilluminate.
Hernias
Sudden impulse or bulge felt → inguinal or femoral hernia.
Perianal and rectal examination: prostate & hemorrhoids
Back pain
Prostate: usually in early stages due to it being slow
Stool:
Look at exudate & lesions
Labs for Male Genitalia:
Colorectal cancer screening:
Begin at age 45–75 years.
High-risk adults (76–85) → continue screening as indicated.
Colon cancer: men > women
smear and culture of exudate or scrapings → lab
Urethral discharge:
Perform Gram stain and culture for gonococci and chlamydia.
Urinalysis → UTI
HIV screenings:
Annual HIV screening for sexually active males who have sex with males (MSM).
High-risk or symptomatic patients:
Consider every 3–6 months screening.
Use of PrEp → prevents HIV
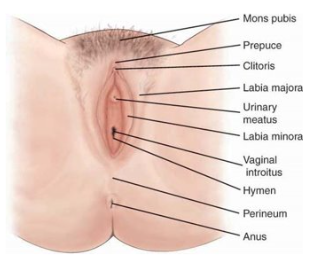
Female Genitalia:
Increased UTI r/x
Skene (antieffective): may secrete clear fluid during climax
Bartholic Glands: secrete clear mucus into the vaginal introitus during sexual arousal and intercourse.
Provide lubrication to facilitate comfort during penetration.
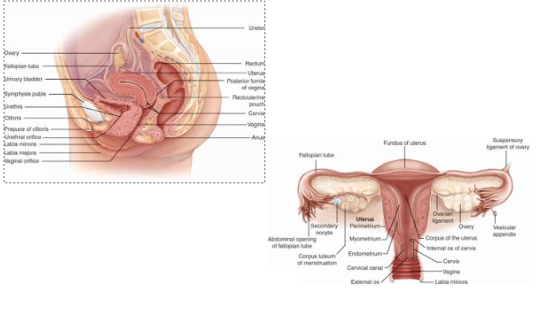
Internal Female Genitalia, Rectum, Anal Canal,Anus
Fallopian Tube: egg becomes fertilized
Ectopic pregnancy: trapped here -> obstruction of flow -> ischemia -> rupture -> shock -> death
Swab is used to check for abnormal cells NOT STI’
Anterior pituitary gland
FSH (Follicle-Stimulating Hormone):
Stimulates growth and maturation of the ovarian follicle.
LH (Luteinizing Hormone):
Luteinizes the follicle → forms the corpus luteum.
Stimulates progesterone production by granulosa cells.
Hypothalamus
GnRH (Gonadotropin-Releasing Hormone): triggers release of FSH & LH.
LnRH (Luteinizing-Releasing Hormone): supports LH release.
Produces Prolactin-Inhibiting Factor (PIF) → inhibits prolactin release.
Acts as the central controller for:
Menstrual cycle regulation
Ovaries
Estrogen:
Regulates secondary sex characteristics (breast, pubic hair, body shape).
Promotes growth of vagina, uterus, and fallopian tubes.
Stimulates endometrial proliferation (lining thickening).
Progesterone:
Secreted by the corpus luteum (post-ovulation).
Prepares and matures endometrial lining for implantation.
Maintains uterine lining if implantation occurs (supports early pregnancy).
If no implantation, progesterone levels drop, leading to menstruation.
Life Span Considerations regarding Females:
Pregnancy:
Ectopic pregnancy:
Fertilized egg implants outside the uterus (commonly in fallopian tube or abdominal cavity).
OB emergency from low HcG — rupture → internal bleeding → life-threatening if untreated.
Vaginal hemorrhage: benign/not
Placenta previa: placenta covers cervical os.
Gestational hypertension / Preeclampsia:
BP ≥ 140/90 mmHg, proteinuria, ± edema.
Can lead to organ damage (kidneys/liver).
Treatment required to prevent eclampsia (seizures, coma).
Preterm labor:
Painful contractions before 37 weeks, especially >6 in 1 hour → immediate evaluation.
Decreased fetal movement:
Always requires professional assessment for fetal well-being.
Infants, Children, and Adolescents
Newborn Assessment:
Pink vaginal discharge in newborn females = normal → caused by maternal estrogen, resolves in 1–2 weeks.
Engorged external genitalia (due to maternal hormones) = normal.
Ambiguous genitalia: opp structure of another gender
Congenital anomaly → adrenal hyperplasia → excess androgens.
Clitoris appears penile, labia fused (scrotum-like).
Puberty:
Sequence:
Breast budding (thelarche).
Pubic hair development.
Menarche (onset of menses) ~2–3 years after breast budding.
Triggered by estrogen release via hypothalamic–pituitary–ovarian (HPO) axis.
Tanner Staging for Female Pubic Hair
Adolescent Examination:
Encourage open communication about sexuality and relationships.
Provide honest, nonjudgmental education.
Annual STI screening for sexually active adolescents.
Establish a trusting, confidential relationship.
Menopausal and Older Adults
Definition:
12 consecutive months without menses.
Average onset: 50–52 years (wide variation).
Hormonal Changes:
Ovaries cease estrogen & progesterone production.
Decreased estrogen →
Smaller uterus and ovaries.
Reduced vaginal secretions → dryness.
Loss of elasticity and fat pad atrophy
Dyspareunia → pain w/intercourse
Health Risks:
Higher risk of endometrial, vaginal, and vulvar cancers.
Require education on warning signs/symptoms (e.g., postmenopausal bleeding).
Cultural variations regarding Female Genitalia:
Median U.S. age at menarche: 12.4 years
Puberty can begin before 8
African American: 5.5 months earlier than peers of other racial/ethnic groups.
Some with greater sexual fluency and candidnessabout sexuality
Sexual activity is personal choice, unrelated toculture and responsibility
Female Circumcision (Female Genital Cutting)
African, Middle Eastern, and Asian cultures despite global opposition.
Cervical cancer checked from swabbing
-HPV
* Prevented with vaccination & protection
Priority Urgent Assessment regarding Female Genitalia:
Severe pain
Acute infection (PID, UTI), appendicitis, pancreatitis, cholecystitis, strangulated hernia ,musculoskeletal trauma (ruptured bladder, spleen, liver), ectopic pregnancy, ovarian cyst
Excessive vaginal bleeding
Change from normal menstrual cycle, occurring outside normal menses, during pregnancy, trauma
Subjective Data collection regarding Female Genitalia:
Past history:
5 Ps
Pregnancy prevention
STI h/x
Any pregnancy:
Gravida: # of pregnancies
Para: delivery past 20 weeks
term: # of pregnancies carried > 37 weeks
preterm: # of pregnancies 20-36 weeks
abortion: loss < 20 weeks
Living: # of alive children
Check for term range
Any abortions
Menopause
Gynecological history
Immunizations
HPV → 11-12 yrs or 9 years
Sexual history
Lifestyle and personal habits
Sexual behavior
Contraception
Sexual transmitted infections
Obesity: ^ Diabetes r/x
Osteoporosis: menopause
Hormonal contraceptive and tobacco use: blood clot; DVT& pulmonary embolism
Medications
Family history
Teaching and Health Promotion regarding Female Genitalia:
Prevention of STIs
Chlamydia -> PID -> potential infertility
r/x in oropharyngeal area; pharyngitis
Trichomoniasis:
Purulent yellow-to-green frothy discharge → foul odor
cervical redness (strawberry looking) contact bleeding
Gonorrhea: yellow vaginal secretions → dysuria & pain with intercourse
Purulent discharge from cervix
Tenderness in pelvic examination
Pharyngeal/anorectal infections
Bacterial Vaginosis (NOT ASSOCIATED W/STI!):
Gray color
Fishy odor
vaginal itching/burning
Flagel med?
Menopause changes
Prevention of HPV and cancer: >100 types
Genital warts, cervix cancer (vaccines only covers this)
Genital self-examination
Elimination of female genital circumcision
Appropriate screenings
Immunizations: HPV vaccine
Common symptoms regarding issues w/Female genitalia:
Pelvic pain
Vaginal burning, discharge, itching
Menstrual disorders
Structural difficulties
Sexual dysfunction
Hemorrhoids
Equipment for vaginal exam:
Sheet or drape
Nonsterile nonlatex examination gloves
Water-soluble vaginal lubricant
Lamp with goose neck or speculum light attachment
Wooden/plastic spatula
Cervical brush
Endocervical brush
Speculum
Swabs
Patient is in Lithotomy position
External genitalia
Inspection
Internal genitalia
Palpate urethra, Skene glands, Bartholin glands
Assess strength of vagina
Speculum examination
Inspect cervix and os
Pap smear and cultures
Inspect vaginal wall
Bimanual examination: lower pelvis palpation; check for masses & ovaries
Rectovaginal examination
Labs for Female Genitalia:
Wet mount analysis, KOH, DNA/RNA diagnostictests, blood tests (LH, FSH, GnRN)
Pap smears: based on case-case
When you start sexual intercourse
stop > 65 years
H/x of hysterectomy: removal of ovaries/fallopian tube
Pregnancy Phases:
Average length of pregnancy: 266 days post-fertilization
from first day of menstruation (28 day-period)
Approximation
Nagele rule:1st day of LMP - 3 months + 7 days
Pregnancy wheel
US (1st trimester) is most accurate way to calculate
Irregular cycle → adjust calculation
Preconception: 3 months before pregnancy
Prenatal, ^ folic acid, exercise
many dont know till 17-56 after conception
most vulnerable during this time
neural tube defects, major brain anomalies, heart defects, limb deficiencies, and various ear and eye defects
miscarriage happens
left & right ovaries ovulate diff cycles → egg → fallopian tube 14 days before next menstrual period → corpus luteum → ^ progesterone
v progesterone → endometrial lining sheds → menstruation
First Trimester (0-13 weeks)
zygote → fallopian tube → fundus → normal small bleed occurs
Second trimester: 13-26 weeks
significant fetal growth; 3in (<30g) → 15in(>1kg)
major organs developed
Fetal survey via US
Third trimester: 26-40 weeks)
Growth but not as fast as 2nd
1kg → 3 ½ kg (7 ½ kg)
Fetal organs grow, ^ muscle size, strength, & protective fat layer
last 4 weeks → mother IgE → aids with fetal immune system
<37 weeks: no IgE immunity boost
Diastasis recti: when fetus grows → abdominal organs spreads → normal tho
Weeks of Gestation:
Term: 37 to 42 weeks (postterm)
Early term: 37 weeks to 38 6/7 weeks
Full term: 39 weeks to 40 6/7 weeks
Late term: 41 weeks to 41 6/7 weeks
Postterm: 42 weeks and beyond
C section/induced
very hard to reach this phase
Nurse role with Pregnancy:
Develop trusting relationship w/patient
bleed, BP issue, prompt mother to go to clinic
If not → majority is outpatient
Dating pregnancy; recording history; obtainingprenatal testing consents; facilitating referrals;orienting client to practice
Triage: check for issues they have (possible UTI)
Nonstress test (NST): 3rd trimester; electrodes → checks babies movements & kicks
Education: Unexpected test results; t/x options, meds, vaccinations
Vaccination: Flu, influenza, T-dap -> pertussis -> negative towards baby (family is vaccinated)
Cultural variations regarding pregnant patients:
Vary throughout the world; U.S. has poorest survival rate due to education & diet
Late or no prenatal care common in teens (<20), African American, Hispanic, and less-educated clients. → infant mortality, still birth, premature delivery
Infant health disparities:
Contributing factors: hypertension, diabetes, obesity.
Gestational diabetes, HTN
Birthing Parent disparities:
stress, bias, attitudes, stereotypes → v affects pregnant client
Midwife contribution → assist in survival rate
Priority Urgent Assessment regarding Pregnancy:
Ectopic pregnancy
Fertilized egg implants outside uterus (often in fallopian tube).
Emergency: rupture can cause fatal internal bleeding.
Pyelonephritis
Untreated UTI → infection ascends to kidneys.
S/S: fever >38°C (100.4°F), severe flank pain.
Requires immediate IV antibiotics to prevent sepsis.
Vaginal Hemorrhage:
Definition: soaking a pad in <30 minutes or showing symptoms of blood loss (light-headedness, dizziness, cold, confusion, anxiety, diaphoresis).
Action: go to emergency department immediately.
Possible causes:
Placenta previa – placenta covers cervical os.
Abruptio placentae – premature placental separation.
DVT
Abdominal emergencies: appendicitis, cholecystitis, pancreatitis, bowel obstruction (esp. 3rd trimester), ovarian tumors.
Gestational Hypertension / Preeclampsia
BP ≥140/90 with proteinuria ± edema.
Organ damage (kidneys/liver) possible.
Treat promptly to prevent eclampsia (seizures, coma).; dip stick too
Delivery leads to rapid recovery.
Preterm Labor
Regular painful contractions before 37 weeks (>6/hour).
Requires immediate evaluation in facility with NICU access.
Decreased Fetal Movement
May indicate fetal distress → requires prompt evaluation.
Kick Count Instructions (Box 25.1)
Start at 26–28 weeks.
Count daily at the same time (often after dinner).
If <10 movements in 2 hours or sudden decrease → call provider immediately.
Subjective Data Collection regarding Pregnancy
Assess for psychiatric h/x → depression & anxiety → unable to take SSRI’s for baby’s health
Eating disorders → screen for it to prevent it when pregnant
Dysmorphic syndrome: see themselves fat even though they not (anorexia nervosa)
Check for folic acid → v neural tube defects
Family h/x: DM, HTN, genetic illness → screen for
Advanced maternal age → Genetic anomalies (>35); miscarriage
freeze eggs to prevent this
Teaching + Health promotion regarding Pregnancy:
Prevent gestational diabetes (preconception phase → 1st → 24-48 weeks).
Promote good nutrition and oral health.
v caffeine → intrauterine growth retardation → v birth weight & baby growth
Encourage healthy lifestyle habits (EXERCISE), mental health, and safety.
Progesterone → v peristalsis → ^ r/x for constipation → hemorrhoids → ^ fluid & exercise
Prenatal and breastfeeding education: best for 1st kid
Stress importance of prenatal visits and monitoring.
v stress, anxiety, & depression
Gaining weight:
10lbs -> first trimester
1lbs -> secondary & third trimester
Common s/s regarding Pregnancy:
Fatigue
Morning sickness: Idiopathic
hormonal, diet, stress; goes away after 1st trimester
some have it/some dont
if not → Hyperemesis gravidarum: vomiting >5% body weight loss, dehydration, electrolyte imbalance → may require IV fluids/hospitalization → fatal
Can continue throught pregnancy
Round ligament pain: 1st trimester; stretching of abdomen → random/sharp pain → indication of growing fetus
Increased vaginal discharge; increased urination (due to ^ progesterone → ^ relaxation)
clear = normal from ^ estrogen
foul-smelling: infection, STI
3rd trimester → mechanical bladder compression
Breast tenderness, discharge: colostrum leaking (3rd) preparing for birth
notify provider to check
Periumbilical pain
Fetal hiccups and other spasms (3rd trimester): when fetus n.s. matures
Braxton Hicks contractions: mimic real contractions
<5/hr; <30 seconds; slight pain
prepare body for labor
Equipment regarding Pregnancy:
Stethoscope; BP cuff; thermometer
Reflex hammer: test for hype reflexive DTR in preeclampsia pt’s to check for eclampsia
+4
Fetal Doppler sonometer: look for fetal HR
Metric measuring tape: measures height of fundus
Urine collection cup and dipsticks
Speculum, light, swabs for pelvic exam
Gown and drape for privacy
Comprehensive physical assessment regarding pregnancy:
General survey & vitals (lungs, heart, baby heart, fundus heigh)
Poor grooming or flat affect → may indicate depression, abuse, or lack of resources → consider social services referral.
Inadequate weight gain/loss
Anemia & IDA → more anemic during pregnancy → supplement them
Pica
Hyperpigmentation: causes distress
Melasma: darker skin pigmentation from hormones → goes away after birth
Epistaxis: vasodilation in nose b.v.
check for hyper/hypothyroidism as it can v affect fetus
2nd trimester → dyspnea during exertion from baby pushing
hard going up the stairs
Systolic murmurs from mother (beginning of the 28 weeks; normal)
Peripheral vascular system: v CO when supine → edema in lower extremities → carpal tunnel syndrome → pain & numb thickness
SMC relaxation → GI & GU stasis → constipation + UTI
Gastric reflux ← fetus compresses & relaxed sphincter
Bad gallbladder bad contractions → bile salts collection → stones
Don’t do anything
If infection → take care
Backaches (2nd & 3rd trimester)
Varicosities: labia; common
Leopold Maneuvers: palpate abdomen to check fetus position
Midwife related
Lab tests regarding pregnancy:
Blood type and antibody screen: check for hemolytic anemia
RhoGam injection avoids attacking Rh factors
Transfusion may be needed
Complete blood count (CBC)
Hepatitis B surface antigen
HIV screening
Rubella titer
Triple or quad screen (maternal serum screening for fetal anomalies) → genetic testing during 1st trimester
Nuchal translucency (ultrasound for chromosomal abnormalities) → check for back cervical spine thickness & neural tube defects
50-g glucose challenge test (screen for gestational diabetes): drink to check sugar lvs after 1-2 hrs
Group B streptococcus (GBS) screening: 3rd trimester
look for bacteria in rectal area → vagina → baby issues
swab vagina & anus → lab → if + → IV ANA (penicillin) during delivery → prevent issues
Total weight gain would be 20-35 lbs throughout pregnancy
Hospital Assessment Types:
Different types, scope, timeframes
Comprehensive/admission: head→ toe
Shift/ongoing
Focused
Urgent/Immediate
Establish baseline (ox stat, vitals)
Use clinical judgment
Assessment begins at admission, continues until client istransitioned to next phase of care.
Cannot delegate main functions of assessment, planning,evaluation, nursing judgment
critical thinking & professional judgment req
5 Delegation rights
Right task
Right circumstance
Right Person
Right direction
Right evaluation (follow-up)
RN assesses basic care activities before delegating
ADLs, assistive devices; nutrition and oral hydration; elimination; personal hygiene; mobility/immobility; rest and sleep; nonpharmacological comfort interventions
RN responsible for delegation
Right task, under right circumstances, to right person, with right direction and communication, under rights supervision and evaluation (5 RIGHTS)
Saferty risks in hospital setting:
Adverse effect: Hospital crew/RN fault
Inaccurate assessment
Delayed recognizing abnormalities
Communicating abnormal/wrong results → provider
Failure to rescue: pt dies cuz RN not fast
Cardiac Arrest, Acute MI, stroke
Safety interventions for hospitalized patients
Improve accuracy of client identification
Improve effectiveness of communication
major issue in adverse events
Improve safety using medications
Reduce harm associated with clinical alarm systems
Reduce risk of healthcare-associated infections
foley caths, C-line
Identify clients at risk for suicide
Prevent mistakes in surgery
time-out: checked verification at the beginning, middle, and end of procedure
Know scope of practice