Exam 1 Study Guide
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
Ancient Egypt History of Mental Illness
- Treatment of mentally ill begins to change
- Mental hospitals
- Hysteria
- Methods to cure mentally ill (opium for visions, rituals, sleep therapy)
- Health of the soul -> mental healthcare is a priority for 1st time
Middle Ages History of Mental Illness
- Inhumane era
- Mentally ill people are possessed by demons
- Mental illness -> witchcraft
Sterilization Programs and Continued Reform
- Eugenic compulsory sterilization programs
- Mental illness -> a defect, due to hereditary
Radical Medicine
- Electroconvulsive therapy
- Insulin shock therapy
- Frontal lobotomy
Practical Domain of IDD
- Self-Management (personal care)
- Job Responsibilities
- Money Management
- Recreation
- Organizing School and Work Tasks
Role of an Individual's IQ Score in IDD Diagnosis
IQ score of 70 or below diagnoses IDD
Mild Level of IDD
Can live independently with minimum levels of supports
Example of Beck's Cognitive Therapy
Distressing or unrealistic thoughts -> negative interpretations and feelings -> negative actions or behaviors
Behavioral Techniques for Cognitive Behavioral Therapy
- Graded Task Assignments
- Activity Scheduling
- Behavioral Experiments
- Modeling
- Behavioral Rehearsal (Role Playing)
- Coaching
- Scripting
- Brief techniques (thought-stopping techniques)
- Breathing Exercises
- Cognitive Homework
Diagnostic Criteria for IDD from DSM-5
- Deficits in intellectual functions
- Deficits in adaptive functioning
- Onset of intellectual and adaptive deficits during the developmental period
Prehistoric History of Mental Illness
- Mental illness stems from magical beings that messed with your mind
- Tribes have spells/rituals to try and cure mental illness (exorcisms, trepanation)
Renaissance History of Mental Illness
- Insane Asylums (poor treatment)
- Torture entertainment; people could come watch treatment
- Patients are "lunatics"
- Mental Illness is a disease
Moral Reform (1942-1947)
- Abuse in psychiatric hospitals is exposed
- Eleanor Roosevelt became sponsor for National Mental Health -> helped advance to humane treatment of patients
Influence of Medicine & Concept of Remedicalization
- Psychopharmacology begins
- Chloropromazine: first psychiatric medication available
- Antidepressants & muscle relaxants for ECT to treat depression and more
Institutionalization
- Lots of people being admitted to mental hospitals -> overcrowded
- Mental illness treated in inpatient settings
- Overcrowded institutions
- Community mental health movement (1960)
- Forced isolation of people with disabilities
- Deinstitutionalization -> patients being released
- Increased homeless due to less low-income housing options (80s)
How were "severely disturbed" individuals being treated during 1920-1950s?
Institutionalized in psychiatric hospitals
Recovery Model
Conceptual model of psychiatric illness that focuses on individuals improving their health and wellness, living a self-directed life, and striving to reach their full potention
Major Dimensions That Support A Life In Recovery
Health
Home
Purpose
Community
Health Dimension of Recovery Model
Overcoming and managing one's disease and symptoms
Home Dimension of Recovery Model
Stable/safe place to live
Purpose Dimension of Recovery Model
Meaningful daily activities and the independence, income, and resources to participate in society
Community Dimension of Recovery Model
Relationships and social networks that provide support, friendship, love, and hope
Wellness Recovery Action Plan
Individualized, self-designed and self-help system used by individuals with mental illness to promote self-recovery
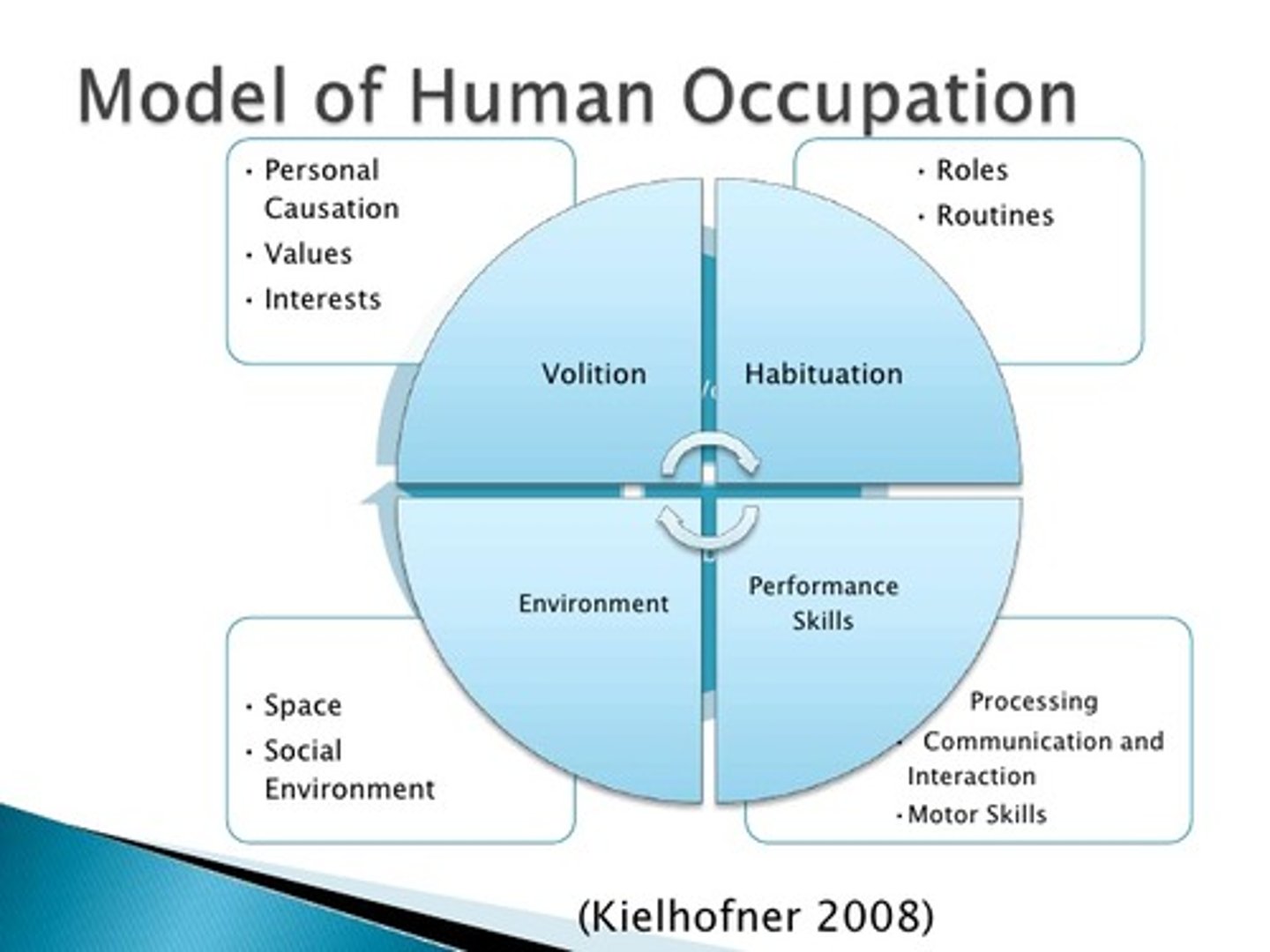
Model of Human Occupation
This model views occupation as a dynamic and systemic process influenced by the person's volition, habituation, performance capacity, and the environment.
Person-Environment-Occupation-Performance (PEOP)
Helps therapists analyze occupational performance through the lens of the person, their environment, and the occupations they engage in, focusing on the interaction of these factors to optimize performance.
Canadian Model of Occupational Performance and Engagement
This model emphasizes the dynamic interaction between the person, occupation, and environment. It highlights spirituality and engagement in occupation as a core element of health and well-being.
Kawa Model
Focuses on understanding the individual’s life context within their social and environmental conditions and working collaboratively to restore or enhance flow.
Purpose of DSM-5
Guides the diagnoses of mental health disorders
DSM-5
Diagnostic and Statistical Manual of Mental Disorders
DSM-5 Major Changes
- Modifications of spectrum disorders
- Replacing terminology (mental retardation -> intellectual disability)
- Improvement methods of assessments
- Disorders on a spectrum (ASD, SA)
Categories of Mood Disorders
- Depressive
- Bipolar and Related Disorders
Bipolar Disorder I
Manic-depressive disorder that can exist both with and without psychotic features
Criteria for Bipolar Disorder I
- At least one manic or mixed episode
- No need for a prior depressive episode
- Can't be better explained by a schizophrenia spectrum disorder
- More severe, easier to diagnose
Bipolar II Disorder
Depressive and manic episodes which alternate, are typically less severe, and do not inhibit function
Criteria for Bipolar II Disorder
- At least one hypomanic episode
-At least one previous major depressive episode
- Can't be better explained by a schizophrenia spectrum disorder
- Less severe; more difficult to diagnose
Brain Stimulation Techniques to Treat Mood Disorders
- Transcranial Magnetic Stimulation
- Electroconvulsive Therapy
- Deep Brain Stimulation
Transcranial Magnetic Stimulation
Non-invasive magnetic stimulation to the scalp
Electroconvulsive Therapy
- Under anesthesia
- Low-voltage currents administered to one side of the brian via electrodes are activated and create a permanent lesion
- FDA approved for Parkinson's Disease
Symptoms of Manic episode
- Elevated/irritable mood for at least 1 week for most of the day
- 3 or more of the following:
Grandiosity
Decreased need for sleep
Pressured speech
Flight of ideas, racing thoughts
Distractibility
Increased goal-direct activity
Excessive involvement in pleasurable activities with high risk
Symptoms of Major Depressive Episode
5 or more symptoms in the same 2 week period:
- Insomnia/Hypersomnia
- Interest (Anhedonia)
- Guilt
- Energy
- Concentration
- Appetite
- Psychomotor
- Suicide
OT Role in Treatment of Mood Disorders
- Observation, interview, and history taking to determine intensity, severity and duration of symptoms
- Life events inventory
- Occupational Profile
- CBT techniques
- Interpersonal Therapy
- Identify areas of occupational performance important to client and set goals
- Assess routines and work with client to reach balance between sleep, self-care, work, and leisure
Interpersonal Therapy
- OT guides client to develop improved communication skills and accurate expression of affect to improve interpersonal relationships
- Builds support for coping with symptoms and life stressors
Three categories of anxiety disorders
- Anxiety Disorders
- Obsessive Compulsive Disorders
- Trauma and Stressor Related Disorders
Diagnostic Criteria for Generalized Anxiety Disorder
At least 3 physical or emotional symptoms:
- Restlessness
- Increased fatigue
- Impaired concentration
- Irritability
- Increased muscle aches
- Difficulty sleeping
Chronic, exaggerated worrying about everyday life that occurs most of the time for at least 6 months
Obsessions
Unwanted, and intrusive thoughts, images, or urges that trigger intensely distressing feeligns
Example of Obsessions
Germ exposure, perfectionism, superstitions
Compulsions
Behaviors an individual engages in to attempt to get rid of obsessions or decrease distress; can be repetitive behaviors
Example of Compulsions
- Showering
- Checking/Re-checking
- Arranging items
- Counting
Repetitive Behaviors
- Can be positive and doesn't interfere with daily life
- Ex: Religious practices, learning a new swkill
Core symptoms of PTSD
Diagnosis requires an adult to have one of each symptoms for at least 1 month"
- Re-experiencing the trauma psychologically (flashbacks, bad dreams)
- Avoiding reminders of the trauma
- Hyperarousal or hypervigilance (easily startled or anger)
- Cognition and mood symptoms
OT Role in Treatment of Anxiety Disorders
- Identify the areas of occupational deficits
- Evaluate (client's routine, environment)
- Relaxation training (breathing, progressive muscle relaxation)
- Expressive activities (journaling)
- Sensory modulation interventions
- Education (time management, lifestyle)
- Complementary Approaches (yoga, animal assisted therapy)
Cluster A Personality Disorders
Social awkwardness, social withdrawal, distorted thinking
Cluster B Personality Disorders
Impulse control and emotional regulation, with a tendency toward dramatic and erratic behavior
Cluster C Personality Disorders
Anxiety and fearfulness
Borderline Personality disorder
Pattern of instability in personal relationships, poor self-image, unstable intense emotions, absolute thinking patterns, prone to angry outbursts, unhealthy coping tools
Positive symptoms of Schizophrenia
- Delusions and hallucinations
- Disorganized speech and behavior
Negative symptoms of Schizophrenia
- Flat affect
- Allogia
- Avolition
- Anhedonia or hypohedonia
Alogia
Poverty of speech
Avolition
Poor initiation of activities and/or inability to sustain goal-directed activities
Anhedonia
Inability to experience pleausre
Hypohedonia
Decreased ability to experience pleasure
Cognitive symptoms of Schizophrenia
- Disorganized speech, thought, and/or attention
- Difficulty with emotional regulation and social cognition
Diagnostic Criteria for Schizophrenia
Characteristic symptoms: 2 or more of the following, each present for a significant portion of time during a month:
- Delusions
- Hallucinations
- Disorganized speech (frequent derailment or incoherence)
- Grossly disorganized or catatonic behavior
- Negative symptoms (affective flattening, alogia, or avolition)
Social/Occupational Dysfunction: for a significant portion of the time since the onset of the disturbance
Some signs of the disorder must be continuously present for at least 6 months
Common Differential Diagnoses for Schizophrenia
- Bipolar Disorder
- Borderline Personality Disorder
- Drug Intoxication and Drug-Induced Psychosis
- Delusional Disorders
- Avoidant Personality Disorder
- Schizotypal Personality Disorder
- Metabolic Disturbance or Systemic Infection
- Syphilis or HIV Infection
- Dissociative Identity Disorder
Borderline Personality Disorder
Emotional instability, fear of abandonment, and strained relationships, often causing intense social difficulties.
Drug Intoxication and Drug-Induced Psychosis
Altered thinking and behavior due to drug use, leading to social withdrawal and impaired interactions.
Delusional Disorders
Strong false beliefs affecting relationships and causing social isolation or distrust.
Avoidant Personality Disorder
Fear of rejection and social inhibition, leading to isolation and difficulty forming relationships.
Schizotypal Personality Disorder
Eccentric behavior and discomfort in social situations, making relationships difficult.
Metabolic Disturbance or Systemic Infection
Physical conditions that cause mental changes, leading to social withdrawal and cognitive issues.
Syphilis or HIV Infection
Illnesses causing cognitive symptoms and stigma, often leading to isolation and emotional strain.
Dissociative Identity Disorder
Shifts in personality causing confusion and relationship challenges.
OT Role in Treatment for Schizophrenia
- Use OTPF to guide eval process and determine how individual's occupations, roles, and routines are impacted
- COPM: guides the interview process and provides observation of client's behaviors while performing occupations
- Cognitive Disability Model Approach
- Assessment of Occupational Performance
- Psychoeducation, Cognitive Remediation, and CBT to support occupational performance.
Conceptual Domain of IDD
- Language
- Reading
- Writing
- Math
- Reasoning
- Knowledge
- Memory
Social Domain of IDD
- Empathy
- Social Judgement
- Interpersonal Communication Skills
- Ability to make and retain friendships
Moderate Level of IDD
Independent living may be achieved with moderate levels of supports (ex: group homes)
Severe Level of IDD
Requires daily assistance with self-care activities and safety supervision
Profound Level of IDD
Requires 24-hour care
Ellis' Rational Emotive Behavior Therapy
- Irrational beliefs lead to emotional distress
- Change irrational beliefs into rational beliefs, leading to healthier emotions and adaptive behaviors
Beck's Cognitive Therapy
States that an individual's thoughts, or personal view of the world, affects how situations are perceived. Occupational functioning is affect when this becomes a pattern
Cognitive Techniques for Cognitive Behavioral Therapy
- Guided Discovery
- Targeting Dysfunctional Assumptions
- Double Standard Dispute
- Catastrophe Scale
- Reverse Role-Playing
- Reframing
Guided Discovery
Socratic Questioning, with a focus on clarification and probing assumptions, evidence, viewpoints, perspectives, implications and consequences
Targeting Dysfunctional Assumptions
Client is asked to provide evidence that supports or does not support personal assumptions
Double-Standard Dispute
Therapist asks the client if they would hold another person they know to the same standard.
Catastrophe Scale
Client is asked to rate something that has been anxiety-provoking or has been the focus of negative energy for the individual.
Reverse Role-Playing
Provides method for the client to argue against the negative assumption or belief that the client possesses. The therapist plays the role of the client and the client becomes the therapist.
Reframing
Technique whereby the therapist works with the client to consider all aspects of a situation
Behavioral Rehearsal
Works well in situations where the client is struggling with verbal interaction (ex: being assertive with someone). Practicing what to say and how to say it can be helpful and can break down negative assumptions regarding personal ability
Cognitive Homework
Client engages in experiential activities and practicing skills at home
Subtypes of Cognitive Behavioral Therapy
- Dialectical Behavior Therapy
- Acceptance and Commitment Therapy
- Mindfulness Based Cognitive Therapy
Dialectical Behavior Therapy
Combines CBT with mindful awareness and distress tolerance practice
Acceptance and Commitment Therapy
- Goal is to increase psychological flexibility (ability to accept your reactions and be present, to choose a valued direction, and take action
- Emphasizes the relationship we have with our thoughts rather than changing (controlling) the content of one's thoughts
Mindfulness Based Cognitive Therapy
- Used as a relapse-prevention treatment for people with depression
- Combination of CBT and mindfulness meditation practice
Thinking in Shades of Gray
Instead of thinking about our problem or predicament in an either-or polarity, evaluate things on a scale of 0-100. When a plan or goal is not fully realized, think about and evaluate the experience as a partial success, again, on a scale 0-100.
Examples of Cognitive Behavior Therapy Tools
- Journaling
- Breathing
- Progressive muscle relaxation
- Challenging though distortions
- Mindfulness
- Positive distraction
- Activity scheduling/ Time management
- Goal setting