MRSC1150 DR Methods 1
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
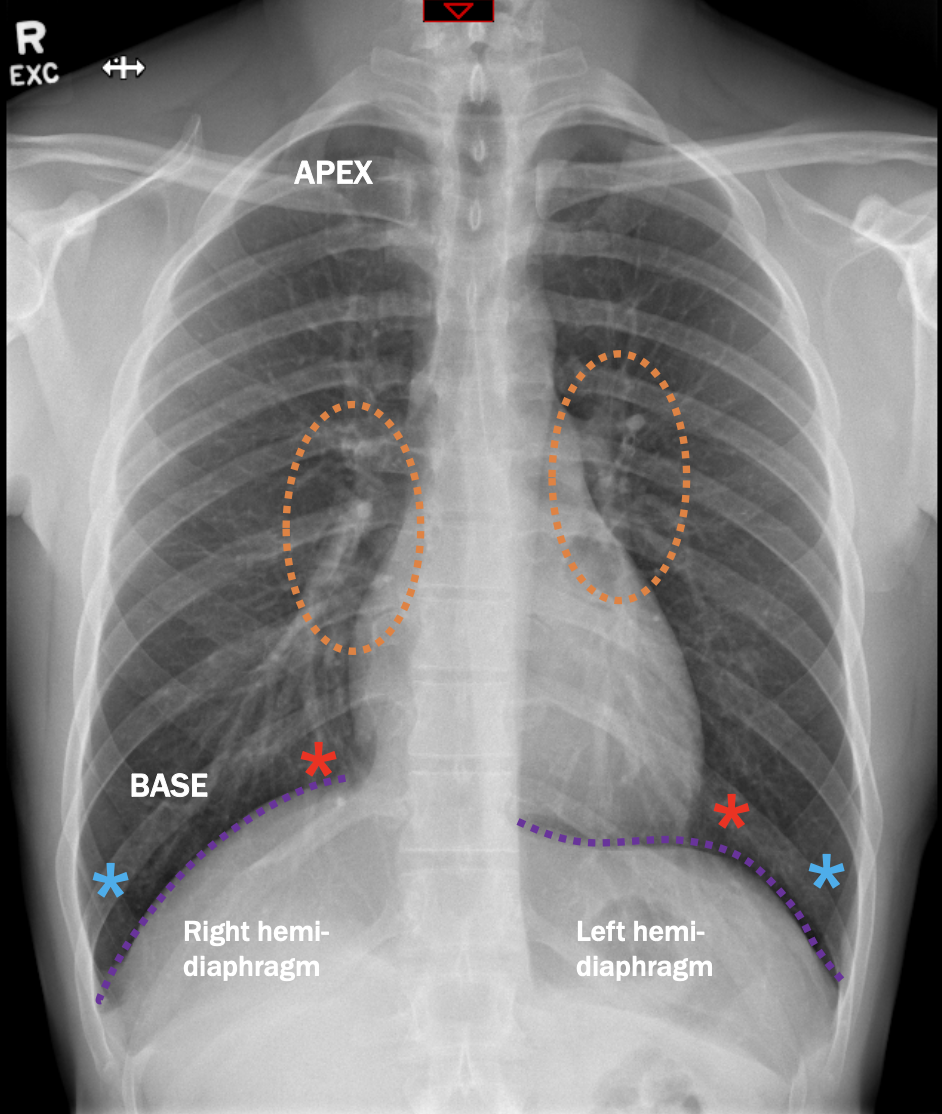
What anatomy is labelled with the blue asterisk?
costophrenic angles
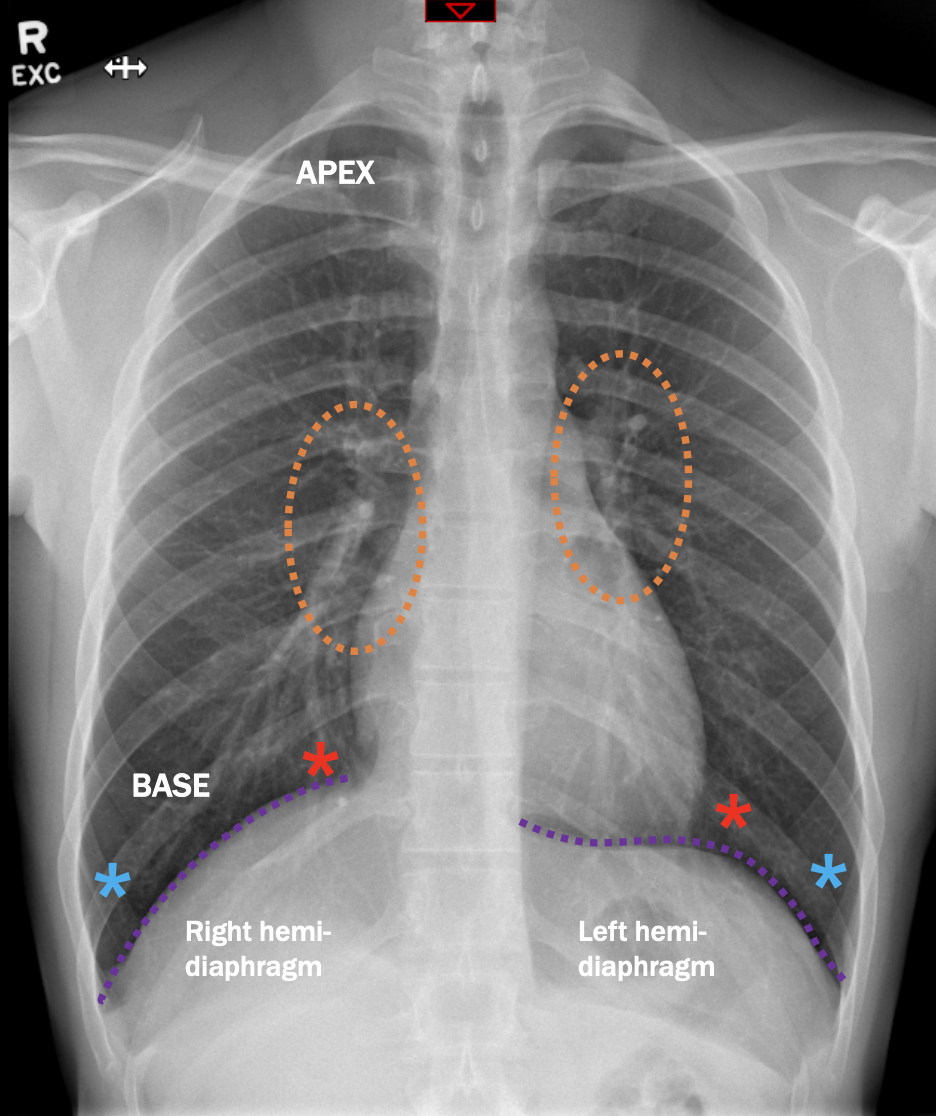
What anatomy is labelled with the red asterisk?
cardiophrenic angles
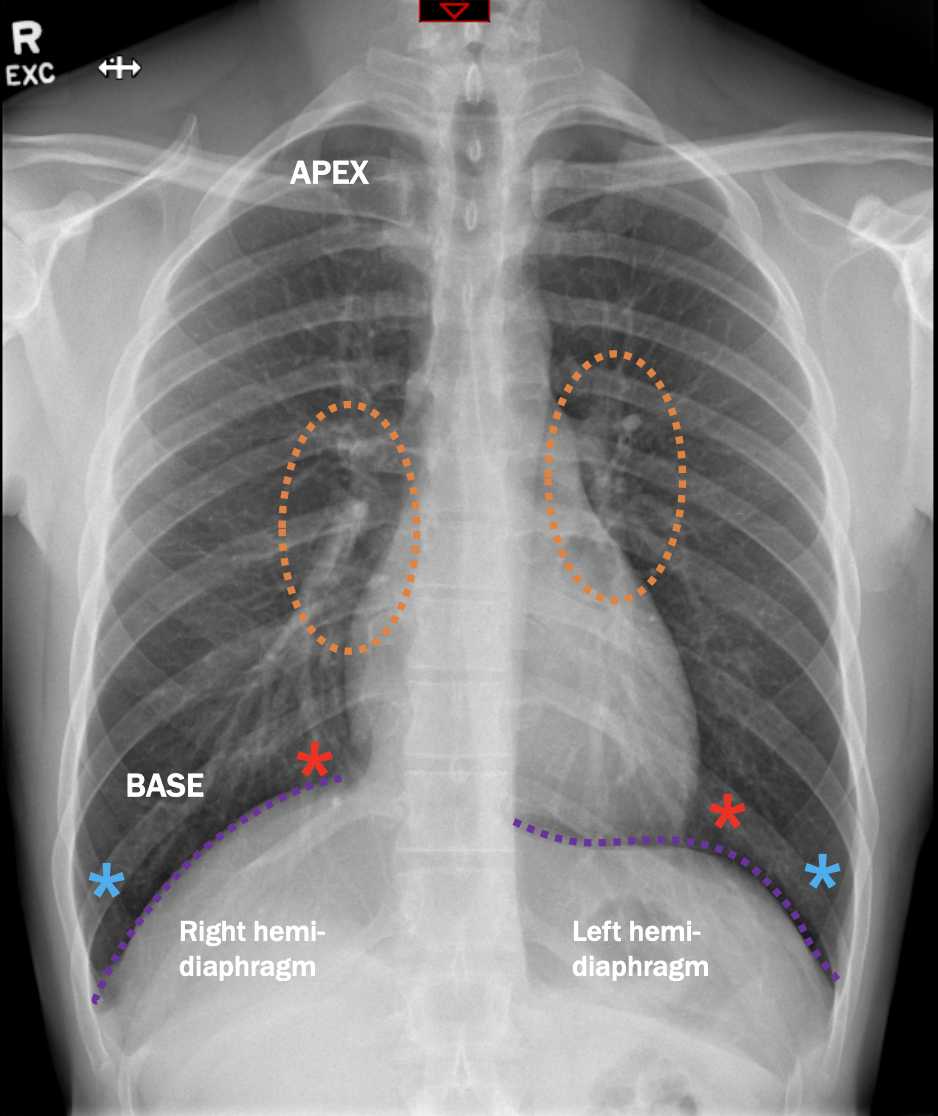
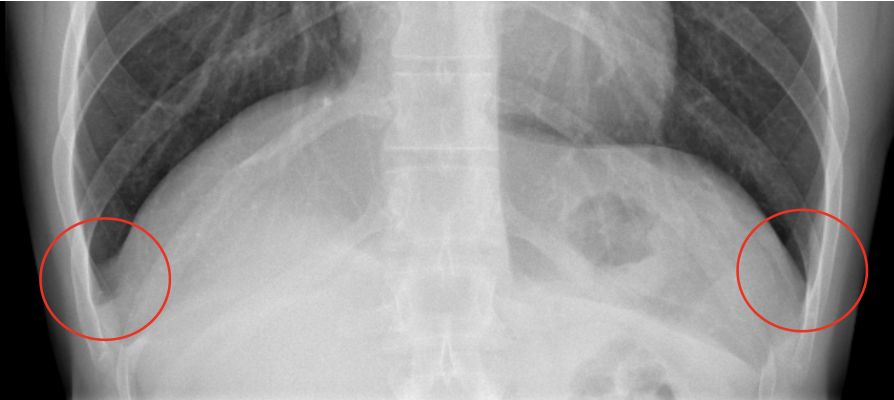
What anatomy is labelled with the orange circles?
Hilum
How do focused grids reduce scatter radiation from a radiograph?
Focused grids have strips which are slightly angles to account for divergent beam. Must be used at a specific distance.
What must you do to the exposure if using a grid?
Increase the exposure (at least doubling mAs)
How does Automatic Exposure Control (AEC) work to control exposure?
An ionisation chamber (which is a hollow cell containing air) is connected to a timer circuit. When the radiation hits the chamber, the air becomes ionised, creating an electric charge. Once sufficient charge has been received, the radiation exposure is terminated.
What is the standard series of radiographs for a chest?
PA and lateral
For a PA CXR, where should the central ray be?
Mid-saggital plane at level of T7 (inferior angle of scapulae)
Distance for a CXR
180cm
Collimation for a PA CXR
Include lung apices to costophrenic angles, laterally to skin border
kVp for a PA CXR
Adult 90-110 kVp
mAs for a PA CXR
Both lateral cells of AEC estimate: 1.2 mAs
Instructions for a CXR
Breathe in and hold your breath (suspended inspiration)
How can you ensure no rotation in a PA CXR (3 points)?
Sternal ends of the clavicles equidistant from the verterbral column
Trachea visible in the midline
Equal distance from the vertebral column to the lateral border of the ribs on each side
How can you ensure proper shoulder rotation for a CXR?
Patient should roll shoulders forward, scapulae should be projected outside of lung fields on radiograph
How can you ensure proper inspiration for a CXR?
10 posterior ribs visible above the diaphragm
What should you ensure about placement of side markers?
Correct placement (correct side) and not over anatomy
How can you ensure that anatomy of interest is assessed adequately for a PA CXR (4 points)?
Apical lung visible above clavicles
Scapulae projected clear of the lung
No rotation (trachea midline and medial ends of clavicles equidistant from the spinous processes)
Good inspiratory effort (8-10 posterior ribs above the diaphragm)
Lateral CXR central ray
Mid-coronal place at level of T7 (inferior angle of scapulae)
Distance of lateral CXR
180cm
kVp for lateral CXR
110-120 kVp
mAs for lateral CXR
Central cell of AEC Estimate: 4 mAs
Where should the hilum be located in a lateral CXR
In the approximate centre of the radiograph
How to ensure correct position and no rotation in lateral CXR (3 points)?
Superimposition of the ribs posterior to the vertebral column
Lateral sternum with no rotation
Open thoracic intervertebral spaces
Where should IR be placed in AP erect CXR?
Behind back approx 3cm above shoulders
What is the appropriate angle for an AP erect CXR?
Caudal angle 5-10 degrees (CR perpendicular to sternum)
Where should IR be placed in AP supine CXR?
Behind back approx 3cm above shoulders
What is the appropriate angle for an AP supine CXR?
Caudal angle 5-10 degrees (CR perpendicular to sternum)
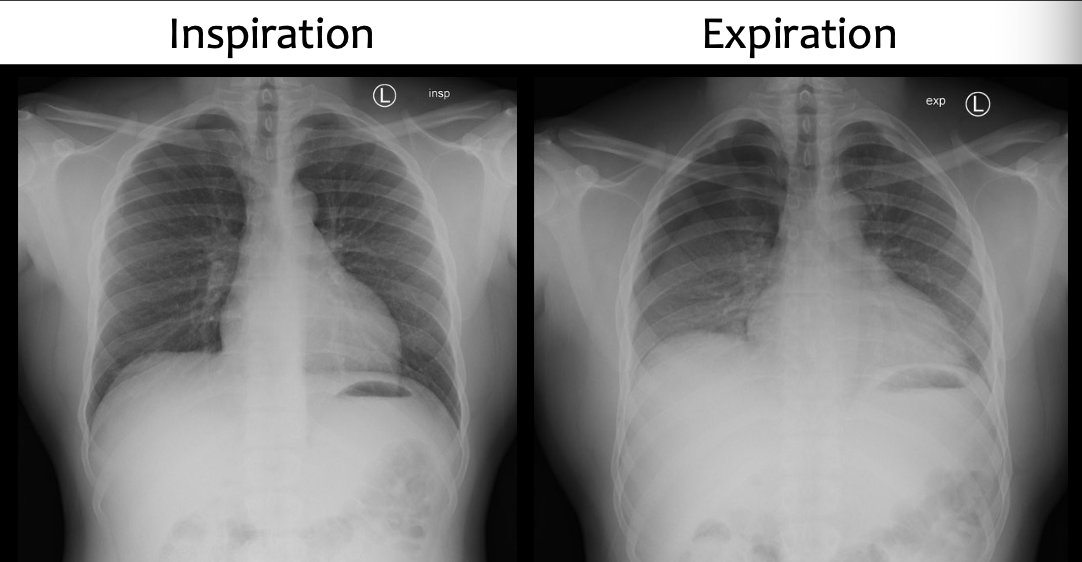
Why would an expiration CXR be performed?
To increase the conspicuity of small pneumothoraces. It increases the attenuation of normal lung, thereby increasing the contrast between lung and pneumothorax.
What should be shown in a lordotic CXR?
Apices in their entirety
Superior lung region adjacent to the apices
Clavicles lying horizontally with their sternal ends overlapping only the first or second rubs
Ribs distorted, with their anterior and posterior portions superimposed

Pathology?
COPD - emphysema (abnormal permanent enlargement of the airspaces and alveolar wall destruction)

Pathology?
Pneumonia (alveolar air replaced with fluid, obscures lung markings)
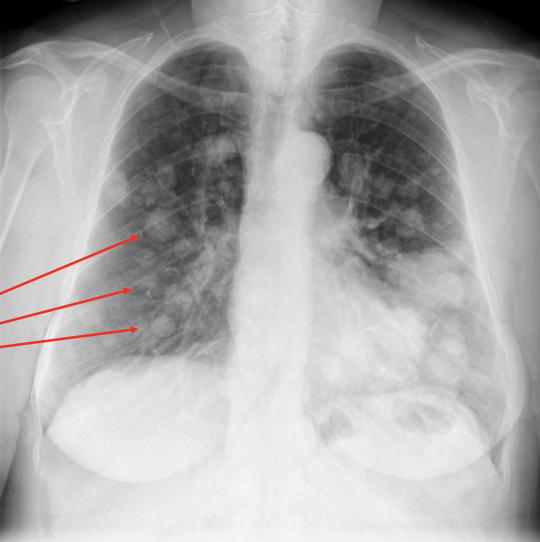
Pathology?
Cancer - metastases
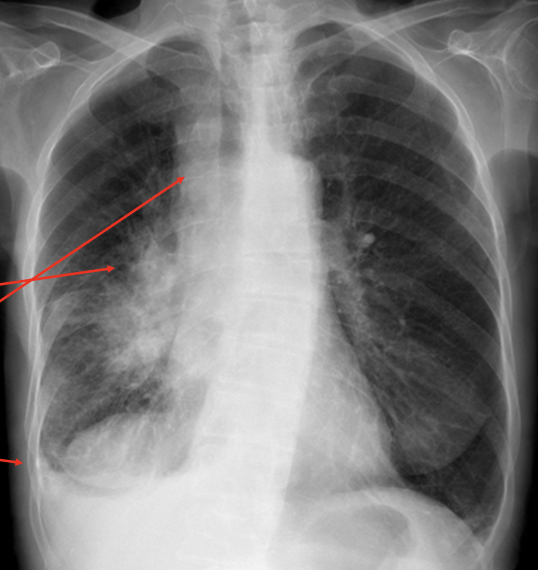
Pathology?
Lung cancer - hilarious mass
Pathology?
Pleural effusion (fluid in pleural space)

Pathology?
Pneumothorax
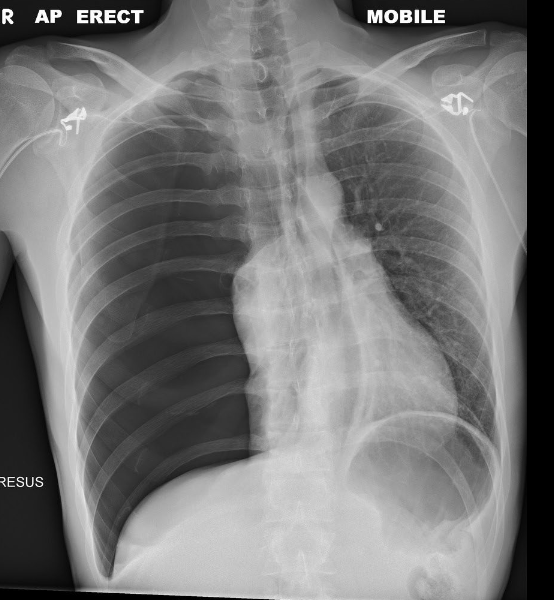
Pathology?
Pneumothorax
Pathology?
Pneumothorax
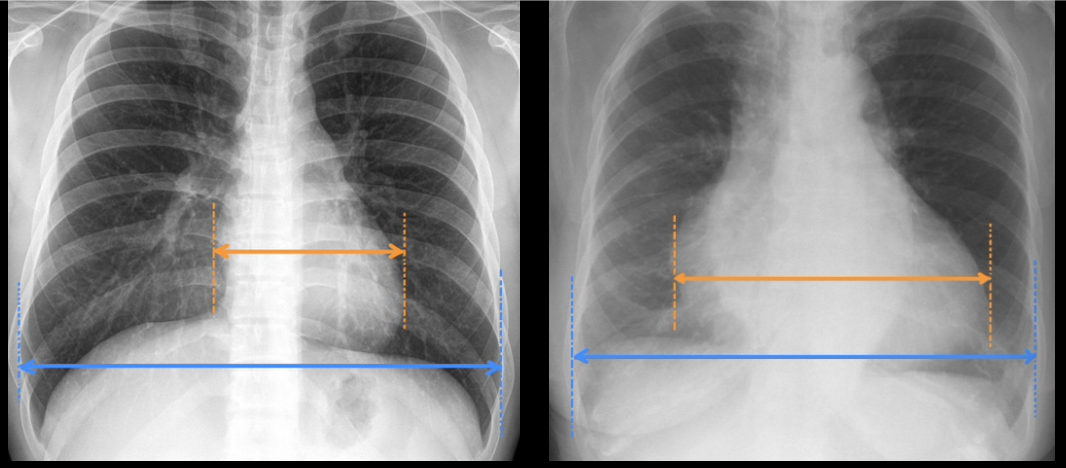
Pathology (in right image)?
Cardiomegaly
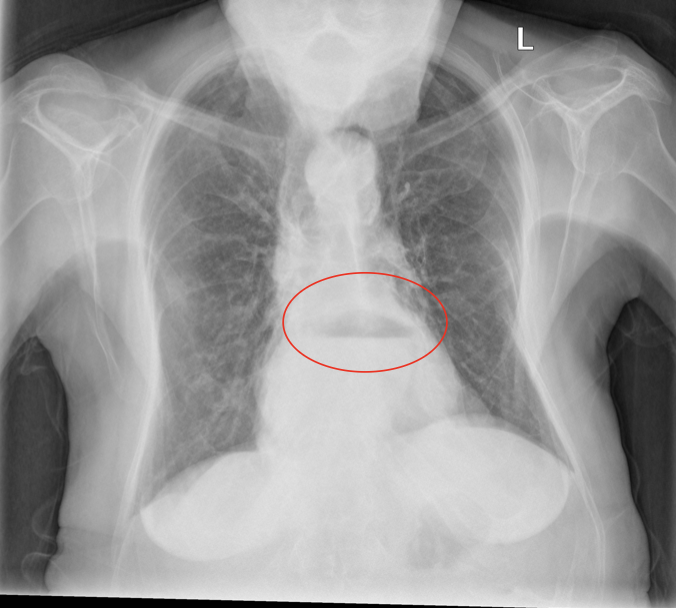
Pathology?
Hiatus hernia (stomach herniates through oesophageal hiatus)
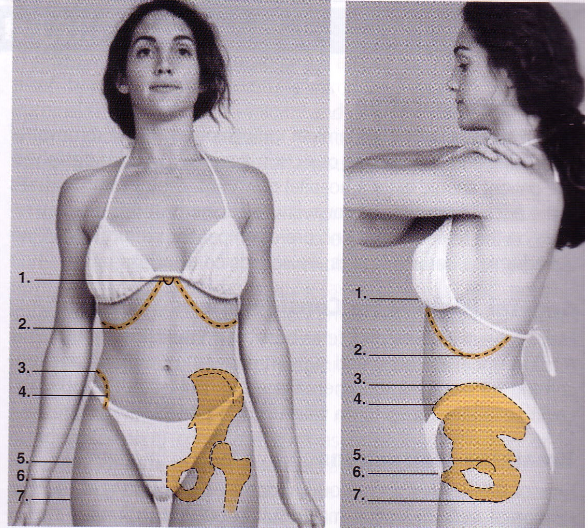
What anatomy is labelled 1 on this diagram?
Xiphoid
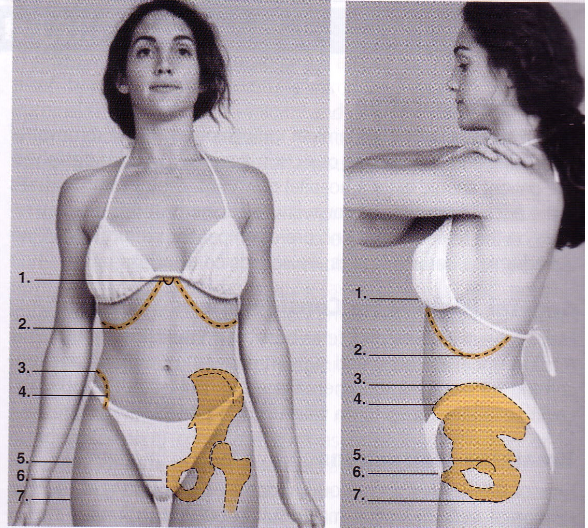
What anatomy is labelled 2 on this diagram?
Inferior costal margin
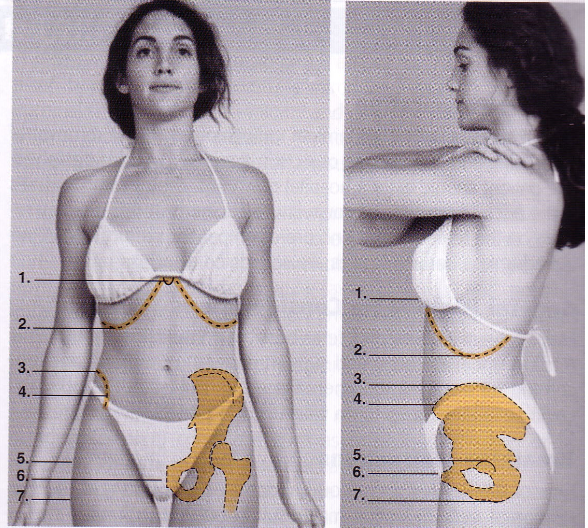
What anatomy is labelled 3 on this diagram?
Iliac crest
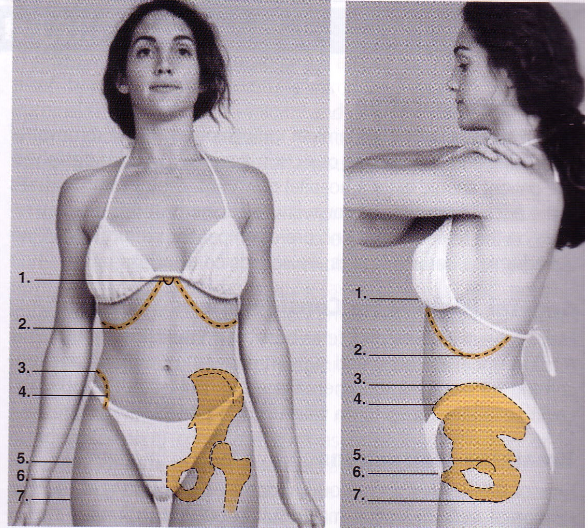
What anatomy is labelled 4 on this diagram?
ASIS
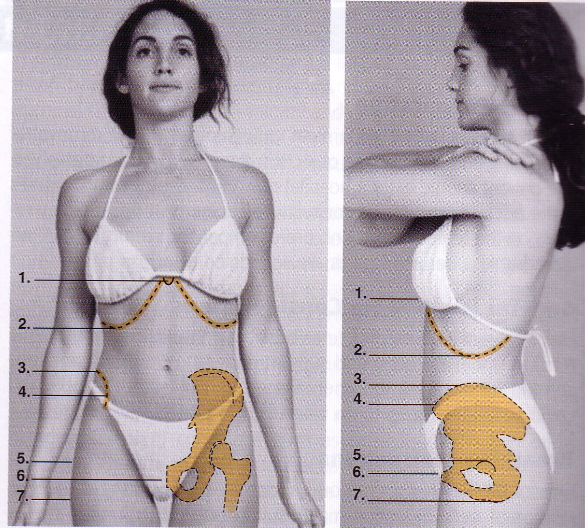
What anatomy is labelled 5 on this diagram?
Greater trochanter
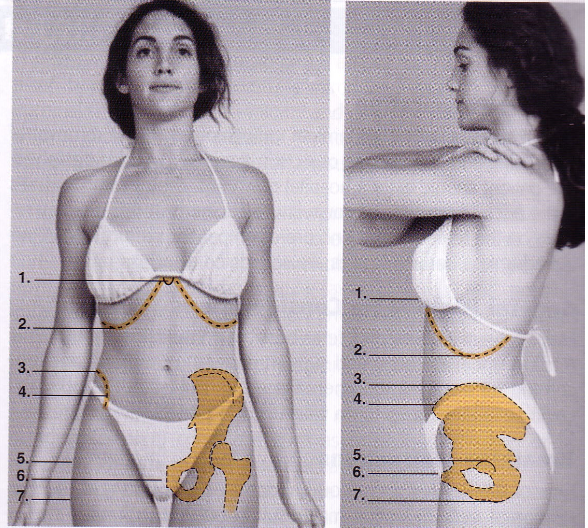
What anatomy is labelled 6 on this diagram?
Symphysis pubis
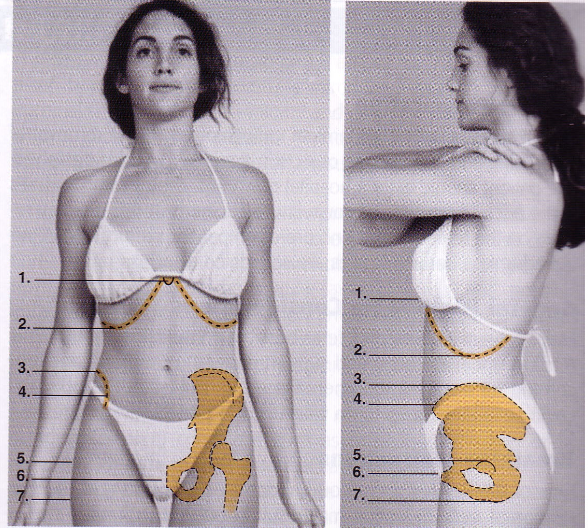
What anatomy is labelled 7 on this diagram?
Ischial tuberosity

What anatomy is outlined in this image?
Diaphragm

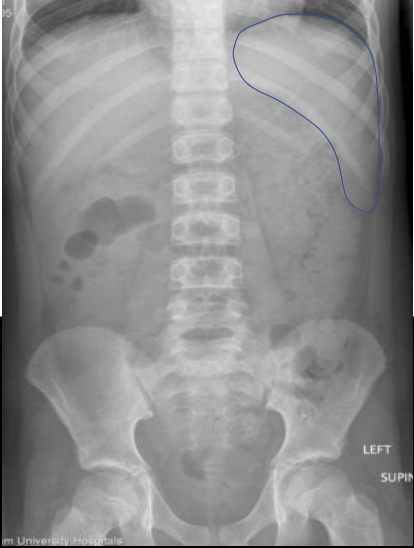
What anatomy is outlined in this image?
Stomach
What anatomy is outlined in this image?
Spleen
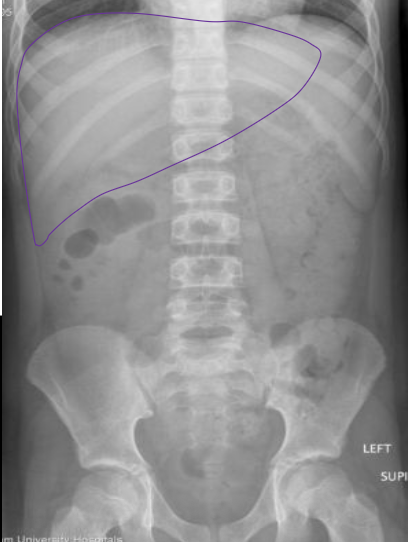
What anatomy is outlined in this image?
Liver
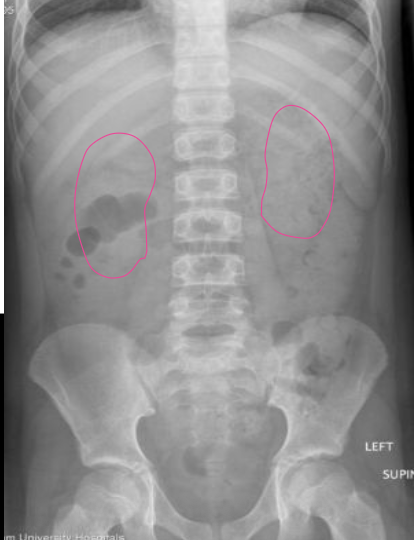
What anatomy is outlined in this image?
Kidneys
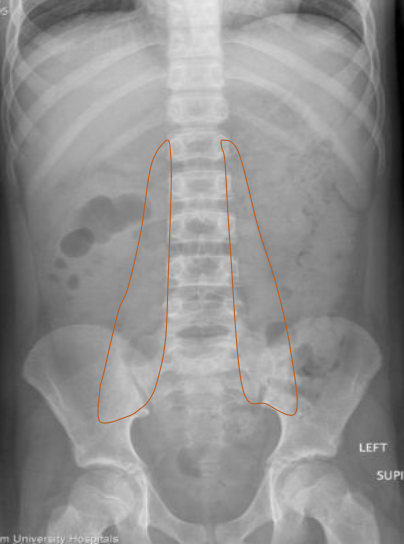
What anatomy is outlined in this image?
Psoas muscle
Standard projections for AXR?
AP supine and PA erect
If a patient presented ?SBO and could not stand, which projection would you take?
Left lateral decubitus (check for air and fluid levels)
Supine AP AXR positioning
Patient on back, on xray table. No rotation, with shoulders and hips equidistant from table
Supine AP AXR central ray
Mid-saggital plane at level of iliac crests
Supine AP AXR distance
100-110cm
Supine AP AXR collimation
Include diaphragm to symphysis pubis, laterally to skin border or receptor size (whatever is smaller)
AXR kVp
Adult 75-80 kVp
Supine AP AXR mAs
Lateral cells of AEC estimate: 30-35 mAs
Grid for Supine AP AXR?
Yes
Breathing for AXR
Suspended inspiration
Criteria for all abdomen radiographic projections (6 points)
As much diaphragm as possible
Mid pubic symphysis included
Psoas muscle seen
Nil rotation (pelvic symmetry)
Wide window width
Markers to indicate side and position
When would a PA prone AXR be done?
Only if a patient is unable to lay on their back. Rarely done.
Erect AP AXR central ray
Mid-saggital plane, half-way between the lower costal margins and the iliac crests
Erect AP AXR mAs
Centre-cell AEC or 30mAs (estimate)
Why would a left lateral decubitus AXR be completed?
To show fluid levels in abdomen, especially if patient cannot stand

Pathology?
Small bowel obstruction (SBO)
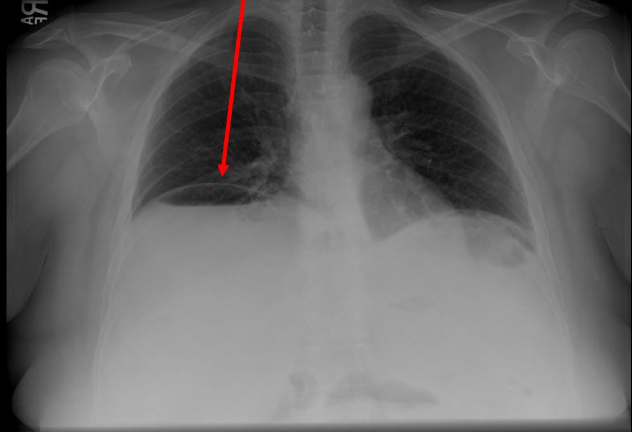
Pathology?
Free air under diaphragm
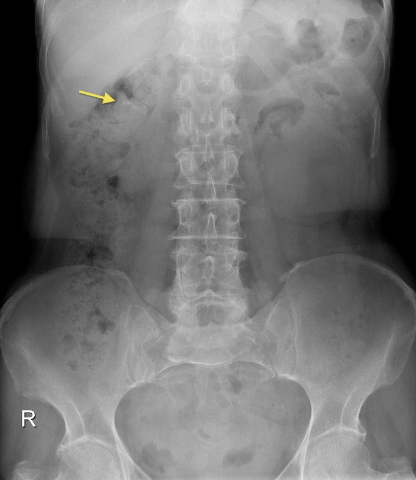
Pathology?
Calcifications
Projections for hand, fingers and thumb
At least two projections of any region
Hand x-ray positioning
Patient seated at end of xray table with legs at right angle to table, hand on image receptor
PA hand central ray
3rd MCP joint
Hand/finger/thumb xray distance
100-110 cm
Collimation for hand x-ray
Four sides of collimation seen to include skin edges of hand
kVp PA hand
50kVp
mAs PA hand
2mAs
Standard hand xray series
PA, PA oblique, lateral
What is an alternate hand projection and when would it be done?
Ball-catchers view (both hands in a ball catching position PA). When suspected rheumatoid arthritis and hands cannot fully open