Behavioral Medicine Lecture 12
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Example: Gender discrimination and mental health
Hackett et al. (2024)
A total of 3081 women (aged ≥52 years) from the
English Longitudinal Study of Ageing provided data
on:T1: perceived gender discrimination
T2 & 3: depressive symptoms, loneliness, quality of life and life satisfaction
Perceived gender discrimination was reported by 282 (9.2%) participants
(cont)
Cross-sectionally, women who perceived gender discrimination (vs. women who did not)
Reported more depressive symptoms & had higher loneliness scores than women who did not perceive gender discrimination.
Reported significantly lower quality of life and life satisfaction
Prospectively, perceived gender discrimination was associated
With greater loneliness scores, lower ratings of quality of life, & life satisfaction independent of baseline values
Gender inequality and brain function
Zugman et al (2023)
Brain develops as a function of interaction with the social world: gender inequality may affect development
Gender inequality is associated with worse mental health and academic achievement in women
Compiled 7,876 MRI scans from healthy adults living in 29 different countries and evaluated them using two combined gender inequality measures
(cont)
Gender inequality is associated with differences between the brains of men and women
In gender egalitarian societies there wasn’t a significant difference between women & men’s brains
BUT in gender inequitable societies cortical thickness of the right hemisphere, (the right caudal anterior cingulate, right medial orbitofrontal) present thinner cortices in women compared to men
These regions have been related to several aspects of emotional control, including resilience to adversity, responses to inequity, or negative social comparisons
Changes in these regions have also been found in pathological conditions where stress is considered a central mechanism, including thinning depression, or reduced volume in posttraumatic stressdisorder
Two hypotheses:
1) Additional stress explained by the minority stress framework
2) Because of gender inequality, women could have lower access to beneficial, enriched environments, which could alter brain structure via higher dendritic branching
1) Racial health care disparities
“The father of gynecology”
James Marion Sims:
Began experimenting on newborn black babies and used an awl to rearrange their skull plates into the “correct position”. Their mothers were blamed for their inevitable death.
In 1849 began performing years of torturous gynecological research on slave women, in particular Anarcha, Lucy and Betsy
These women had all developed fistulas (torn tissues between bladder/anus/vagina resulting in incontinence) as a result of giving birth
(cont)
The experimental surgery techniques lead to terrible infections which never healed, requiring the surgeries to be repeated.
All surgeries were all performed without anesthesia on the Black slaves, but when finally perfected, were performed with anesthesia for white patients.
Sims developed the speculum, and is currently lauded as “the father of gynecology”
It was believed that black people didn't feel pain, which is what led to these experiments
Tuskegee Syphilis study
Tuskegee, Alabama
In 1932 the United States Public Health service began a study to record the natural progression of syphilis in black men; something readily available from centuries of history
The study involved 600 Black men; 399 with syphilis
The study was conducted without the patients’ informed consent, and researchers told men that they were being treated for “bad blood”
In exchange for participating in the study, the men received free “medical exams”, free meals and burial insurance – incentives that were impossible to refuse
“Exams” = painful lumbar punctures disguised as therapy
By 1969 estimates of death from syphilis ranged from 28-100 participants
The Stages of Syphilis
The end stage attacks your organs
Syphilis is often called “the great pretender” since its symptoms look like many other diseases
Primary stage
One harmless sore develops then goes away
Secondary stage
Non-itchy skin rashes and/or sores in music membranes or can also appear on the bottom of feet/palms of hands
Different types: ocular syphilis, neurosyphilis
Latent stage
No signs/symptoms but syphilis remains in the body
Latent syphilis can last for years
Tertiary stage
Can appear after 10-30 years
The virus begins to attack your organs
Gumma
*Image on slides of large sores and a missing nose
Causes swiss cheese brain → the gumma would eat a part of the brain
Tuskegee Syphilis study
Penicillin was discovered and found to be a cure for syphilis in 1943.
The black men in the Tuskegee study were not informed, nor were they given the new drug
In 1972, an Associated Press story about the study was published & an advisory panel concluded that the study was “ethically unjustified” & stopped the study
In March 1973 the Secretary of the Department of Health, Education and welfare was advised to provide all necessary healthcare for the survivors of the study
Later in 1973, a class-action lawsuit was filed on behalf of the study participants and their families, resulting in a $10 million, out-of-court settlement in 1974
It gets worse…
2010: US civilians learned the same research group had deliberately infected hundreds of Guatemalans with syphilis and gonorrhea in the 1940s
Goal? of developing better methods for preventing these infections.
Infected vulnerable populations: prisoners, soldiers, people with mental illness
READ ARTICLE ON BLACKBOARD
**Please read the Tobin (2022) article on blackboard for more information
Not isolated incidents
Other examples of the US government exploiting Black/Brown people:
Late 18th/Early 19th century Grave robbing to meet dissection need
Black corpses were overwhelmingly use for dissection which was considered immoral and irreligious but necessary to advance medicine.
Black men, women and children’s graves were robbed to meet this supply, and some speculate people were murdered to meet this need.
Most of New York City’s dissection tables were full of Black bodies, despite members of the Black community’s accounting for only 15% of the population at the time.
1946 Guatemala STI study funded by US government
5128 vulnerable people, including children, orphans, child and adult prostitutes, Guatemalan Indians, leprosy patients, mental patients, prisoners, and soldiers.
1946-1948, health officials intentionally infected 1308 of with syphilis, gonorrhea, and chancroid and conducted serology tests on others.
Inducing STI involved injecting bacteria (sometimes in the spine), placing bacteria/pus on in eyes, scraping penises with hypodermic needles then applying bacteria, swallowing bacterial solutions
1960s Prisoners (mostly Black) exposed to Dioxin
Study commissioned by Dow Chemicals to see if Dioxin in their herbicides would hurt humans
Lethal in small animals, who developed liver/kidney damage
Despite referring to Dioxin as “highly toxic” by the lead PI, it was applied directly to prisoners’ skin = developed blisters, lesions, acne that remained untreated.
More serious effects, however, have been suspected, including cancer and liver and kidney damage.
Many veterans, among 20,000 who have filed a joint suit against several chemical companies, have attributed a variety of ailments, including birth defects in their children
and malignant tumors, to exposure to dioxin in Agent Orange, a herbicide used in Vietnam.Records were not kept of the tests participants and follow up was impossible
1995: HIV+ women and transmission to babies
Research conducted on 12,211 pregnant women infected with H.I.V. in Africa, Thailand and the Dominican Republic paid for by the NIH and CDC
If H.I.V.-infected women are not treated with the correct dose of AZT ~ 25% of their babies will be born infected
If infected pregnant women are treated with the right dose of AZT the transmission rate falls to 8%
~ 1,000 babies were believed to have contracted HIV/AIDS during the experiment, which was discontinued early because of the controversy surrounding the use of a placebo and lack of informed consent
2021: Prisoners in Arkansas experimented on during the pandemic
A doctor employed at the Washington County Detention Center had been treating COVID-19-positive incarcerated people with ivermectin.
Prisoners were told that they were being treated with “steroids and vitamins”
The FDA has warned that ivermectin isn’t safe or effective for treatment or prevention of COVID-19
Ivermectin’s side effects include skin rash, nausea, vomiting, diarrhea, stomach pain, facial or limb swelling, adverse neurologic including seizures, comas, and even death
The immortal legacy of Henrietta Lacks
Black girl with cervical cancer was brought to a hospital
Cut of a piece of her cells
Her cells never died, they continued to multiply
Her cells spread around the world for important research such as cancer research and the polio vaccine
*article about COVID on slides
Current racial bias
An extensive literature base has demonstrated that unconscious bias contributes to racial inequalities in medical care.
Racial and ethnic minority patients are often perceived negatively by healthcare professionals.
Bias increases further against minority patients vs. white patients when the patient has a lower socioeconomic position.
Racial stereotypes persist in textbooks
The Med Student that Wrote the Book on Diagnosing Disease on Darker Skin
We looked for pictures and clinical descriptors that we could use to define them, understanding that there needs to be a difference in the communication aspect of the descriptors that we use. It was very hard and intense because… there are a lack of images of Black and Brown skin across the internet. Thankfully, we were able to source them and here we are today,” Mukwende said. His work spread worldwide. Since its publication in August, the handbook has been read in 102 countries and added to recommended reading lists at many universities and hospitals in the U.K. (2020)
Web resources
Mukwende created the website “Black and Brown Skin” in hopes of growing the content of the handbook.
The site allows people to submit their own images or personal stories anonymously to build a portfolio of images.
“The aim of the website is to allow people who have been silenced for many years to be able to add and provide resources, which will be collated in one place to a bank of pictures. We also have a feature if they are not able to share their photo, they can share their stories.” - Malone Mukwende
Racial bias in pain assessment & treatment
S1: Participants
92 pps who were white, born in the US, native English speakers
Method
Participants rated the extent to which 15 biological differences between Black and White patients are true or untrue on a six-point scale (1 = definitely untrue - 6 = definitely true)
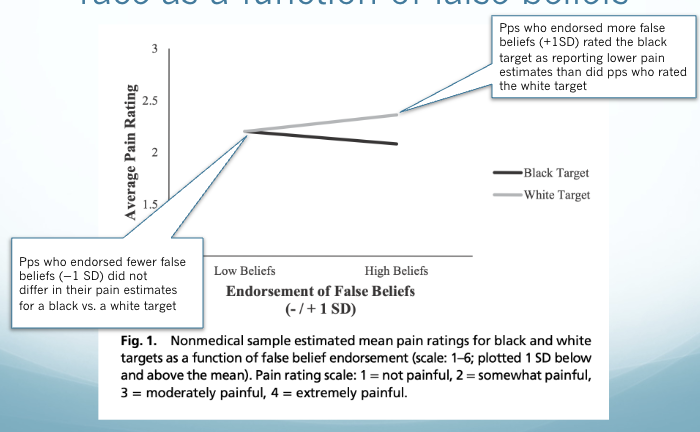
Participants reported the amount of pain they would feel across 18 scenarios and then were randomly assigned to rate the pain of a gender-matched black or white target across the same scenarios
Results
About 73% of the sample endorsed at least one of the false items
Higher false beliefs about biological differences predicted lower pain estimates for black vs. white targets
Non-medical estimates of pain by race as a function of false beliefs
Racial bias in pain assessment & treatment (cont)
S2: Participants
222 medical students and medical residents
Method:
Participants read two mock medical cases about a black and a white patient and made 2 DV ratings:
pain ratings (scale: 0 = no pain-10 = worst possible pain)
medication recommendations (coded 0/1 for inaccurate/accurate)
They completed a measure of beliefs about biological differences between Blacks and Whites as in study 1
Results
On average, participants endorsed 11.55% (SD = 17.38) of the false beliefs.
~ 50% reported that at least one of the false belief items was possibly, probably, or definitely true (Table on next slide)
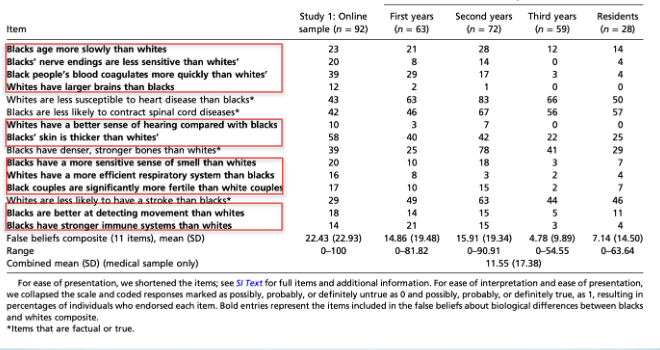
Medical estimates of pain by race as a function of false beliefs
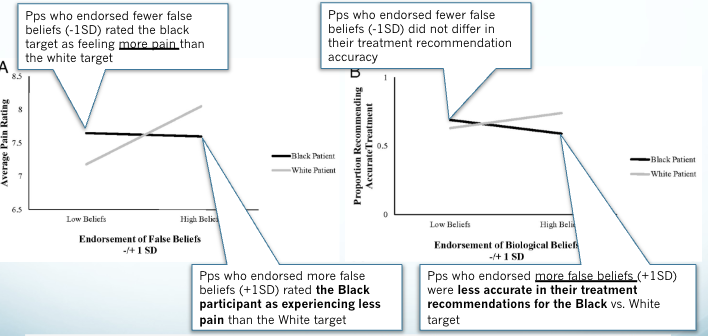
Conclusions
Belief in false biological differences between races by medical students impacted their estimates of pain and accuracy of treatment
Pps who endorsed fewer false beliefs (-1SD) rated the Black target as feeling more pain vs. White target and didn’t differ on their treatment accuracy
Pps who endorsed more false beliefs (+1SD) rated the Black participant as experiencing less pain vs. White target and were less accurate in their treatment recommendations for the Black vs. White target
Racial disparities in ER analgesic prescription
Tamayo-Sarver et al., 2003
Analyzed Black, Latino & White patients from the 1997-1999 National Hospital Ambulatory Health Medical Care surveys
Goal: to compare the rates of opioid prescriptions for the three races/ethnicities for migraines, back pain & long bone fracture
Hypotheses as to why minoritized populations may be less likely to receive opioid prescriptions
They are less assertive/less able to effectively communication with physicians
Minoritized populations are more frequently associated with lower SES
Physician’s perceptions of patients can vary by race/ethnicity
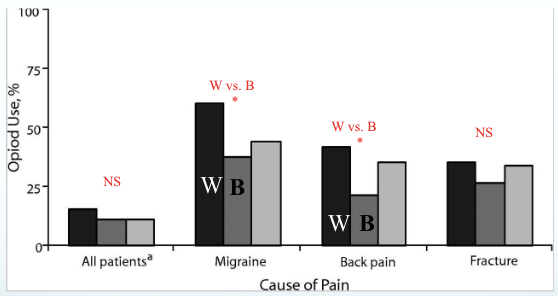
Results
No difference in overall analgesic prescriptions between all ethnic groups BUT physicians were less likely to prescribe opioids overall to Black people
This disparity appears greatest for conditions with fewer objective supports (i.e. migraine/back pain).
Black people were far less likely to receive an opioid for migraine & back pain, but not for long bone fracture
There were no differences in opioid use between White and Latino people for these 3 conditions BUT this may have been limited by the small sample of Latino participants
Proportions of patients who received an opioid analgesic
Racial bias and heart transplant decisions
Participants
422 Heart Failure Society of America professionals i.e. postdoc trainees, nurses, pharmacists, pharmaceutical representative, Nurse Practitioners, physicians
Method
Participants were randomly assigned to read an identical vignette of a man with a complicated Heart failure (HF) history, who was either black or white.
Race was indicated by text, photograph, and ethnic sounding name.
The photographs differed only by race, having similar hairstyle, clothing, and physical build; they were similarly rated for age, attraction, intelligence, health, facial expression, and trustworthiness
DV: Which recommendation did they make for the vignette man?
Heart transplant, future candidate for transplant, not a candidate for transplant
Image
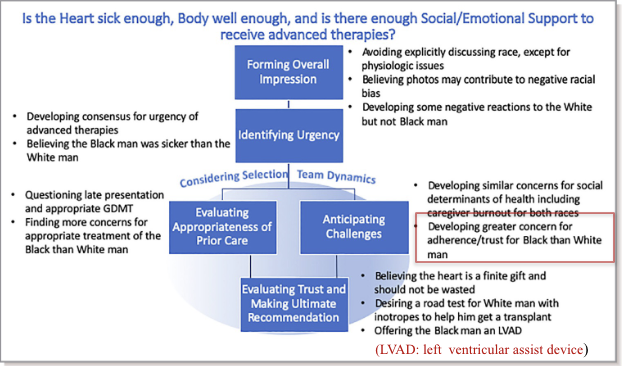
Results
Individually there were few racial differences in participants’ transplant recommendations BUT racial bias was demonstrated when a subgroup of 44 discussed the cases together
This is alarming because the group discussions parallel how the decisions for HF therapies happen in reality
This preference for heart transplants for White men (vs. Black men) increased subtly if the participant was > 40 years of age
Bias against minoritized racial identities increases when the patient has lower SES
In this study the black man was viewed as less adherent to therapy than the white man despite having the same clinical & social history