developmental psychology ch8
1/39
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
40 Terms
The dilemma of Heinz:
If a woman was dying for a rare disease and had no money for one possible cure, because the pharmacist told her to pay 50000 despite him paying 500 (didn’t want to lower it), should her husband steal it?
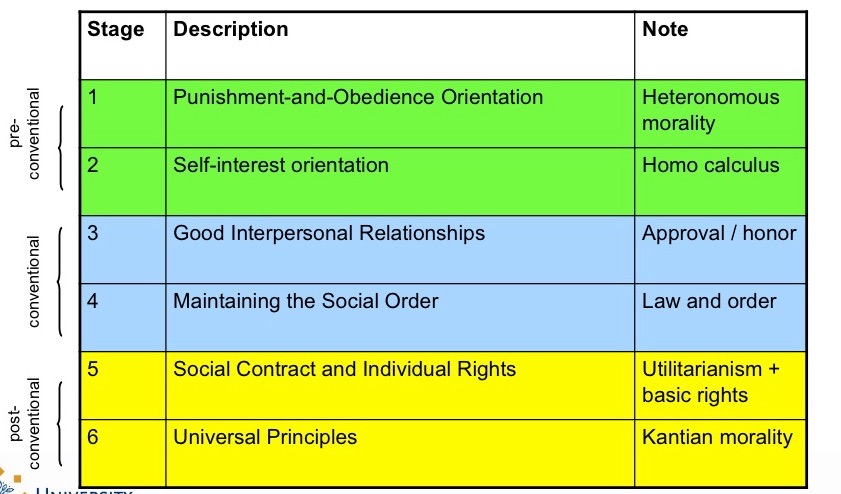
Kohlberg’s moral stages:
Preconventional level: Person operates on punishment and reward mentality (typical at 13):
Stage 1: “Heinz can’t steal it, he’ll go to prison”
Stage 2: “Heinz should steal it because his wife will love him more”
Conventional: Person’s morality centres on the need to obey society’s rules (most 15/16 year olds/adults:
Stage 3: “Heinz has to steal the drug as a good husband”
Stage 4: “Heinz can’t steal it, as other would do it too and laws’d break down”
Post conventional: Person has a personal moral code that transcends society’s rules (few people achieve):
Stage 5: “Heinz can’t steal the drug as that would undermine the scientist’s work”
Stage 6: “Heinz has to steal the drug, because human life is more precious than property rights”
Pre conventional stage:
Person operates on punishment and reward mentality (typical at 13):
Stage 1: “Heinz can’t steal it, he’ll go to prison”
Stage 2: “Heinz should steal it because his wife will love him more”
Conventional stage:
Person’s morality centres on the need to obey society’s rules (most 15/16 year olds/adults:
Stage 3: “Heinz has to steal the drug as a good husband”
Stage 4: “Heinz can’t steal it, as other would do it too and laws’d break down”
Postconventional stage:
Person has a personal moral code that transcends society’s rules (few people achieve):
Stage 5: “Heinz can’t steal the drug as that would undermine the scientist’s work”
Stage 6: “Heinz has to steal the drug, because human life is more precious than property rights”
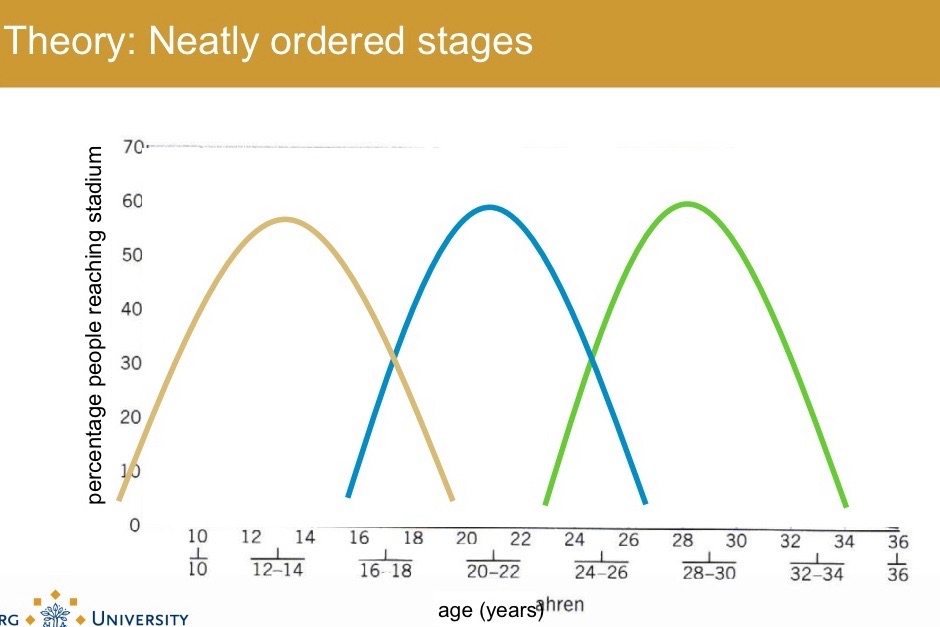
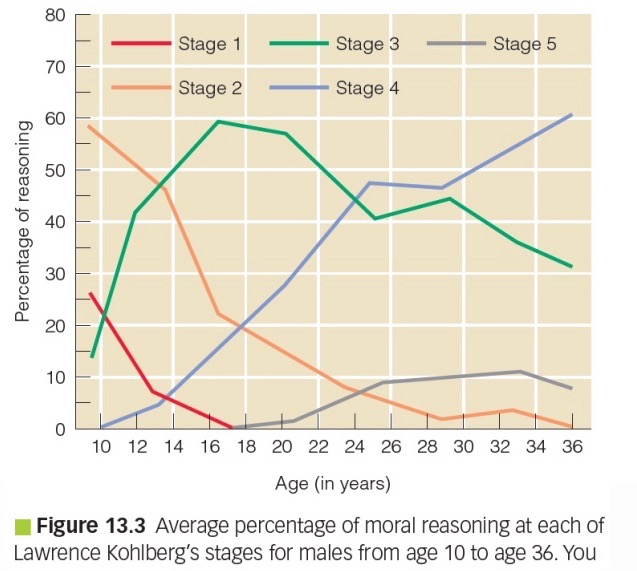
Evaluating Kohlberg’s theory:
Evidence on stage idea:
Children can go beyond punishment/reward mentality
No clear transitions, going back and worth
Stage 3 and 4 dominates (only 10% store higher)
Validity:
Moderate association between moral cognition and moral behaviour
No control for confounds
Association is moderated by motivation and self-control
But; Teens famous for questioning society rules
Alternative theories:
Social learning theory - Bandura:
Moral behaviour affected by: Observational learning, reinforcements, self regulation process, moral disengagement, situational influences
Evolutionary theory - Kerbs, Tomasello:
Humans have evolved not only to be aggressive on occasion, but to have moral and prosocial tendencies to equip them to live cooperatively.
Theory of Mind:
= ability to form ideas about the mental world of yourself and of others and to explain behaviour in terms of mental states.
Basis for: social relationships, empathy, reciprocal conversation, humor lying → important milestine
First social cognitive skills in infancy:
Understanding intentions.
Babies 6-10 months have a “moral compass”
→ Preference for “helping” triangle compared to “annoying” square
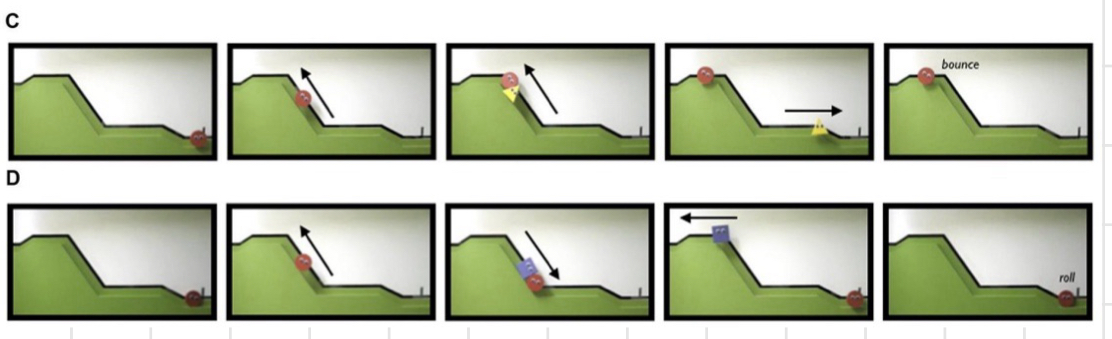
Classic debate in baby and primate research:
Does observed behaviour indicate a deeper understanding or is it just simple associative learning?
Importance and understanding of eye gaze as sign of intentionality.
Joint attention:
= shared attention.
Around 1 year old: important developmental milestone, follows pointing hard/gaze, building block for shared knowledge/experience.
If doesn’t develop, possible autism
Pretend play:
First simple play between 1 and 2 years → distinguish between pretence and reality.
Imitation:
In first year → ability to mentally represent others’ actions + goals
Emotional understanding:
In second year → understanding that other people have emotions and those emotions can be influenced for good/bad.
Desire psychology:
Around age 2, express what they want, explain own behaviour and that of others in terms of wants.
Age 3-4: belief-desire psychology
Understanding that beliefs, true or false, guide people’s behaviour just as desires do.
Theory of Mind: Test
👧 Characters:
Sally has a basket.
Anne has a box.
📖 Story:
Sally puts a marble in her basket and leaves the room.
While Sally is gone, Anne moves the marble to her box.
Sally returns.
❓ Question:
“Where will Sally look for her marble?”
🧠 Interpretation:
A child with Theory of Mind will say: “In the basket” — because that’s where Sally falsely believes the marble still is.
A child without ToM (typically under ~3/4 years old) will say: “In the box” — because they know it was moved and assume Sally knows it too.
Theory of Mind and Piaget:
Counter to what Piaget thought, children in preoperational phase can take others’ perspectives.
Explicit Tom: Sally-Anne test (need verbal skills, explicit questions)
Implicit Tom Tests: Implicit cues (gaze), children of even 15 months show it
Theory of Mild: Criticism of False Belief Test
You need more than TOM to pass it - language, executive functions etc.
TOM is more than passing this one test, it’s just the beginning.
Development of social cognitive abilities:
Age 5-7: Further improvement understanding others, not oneself.
Late elementary school: understand complex second-order belief statements
School kids have to learn to understand sarcasm.
Middle and late childhood: Beliefs can be false, but also one event can be open to interpretations.
Social cognitive skills continue to improve after adolescence.
First order vs second order beliefs:
First-order belief: What Person A believes about the world.
→ “Sally thinks the marble is in the basket.”
Second-order belief: What Person A believes about Person B’s belief.
→ “Sally thinks that Anne thinks the marble is in the basket.”
Development of social cognitive abilities: adults
Better maintained during adulthood than nonsocial cognitive skills.
In older age, improves further: taking multiple perspectives and compromise.
People use social cognitive abilities every day and accumulate expertise → highest skills in socially active older adults in meaningful social roles.
Yet decline in some social cognitive tasks, ex. sarcasm and adult TOM tasks. Especially if they overload basic cognitive capacities bc of fast info processing/executive control.
Types of empathy:
Affective empathy → feeling with someone, emotional connection, compassion, concern, contagion.
Cognitive empathy → rational understanding → taking someone else’s perspective → theory of mind
Development of empathy: Newborns
Newborn baby - emotional contagion.
Distinction between self and other is crucial → Development of empathy mainly between 1 and 2 years.

Development of empathy: Prosocial behaviour in infants
Instrumental helping (12-14 months): Helping with a goal-directed action.
Empathetic helping (18-24 months): Prosocial response to someone’s sadness/pain.
Children struggle helping if they need to:
Reflect on others’ emotional state
Give something up
Cues are subtle
Development of empathy: Prosocial behaviour in children:
Association between cognitive and social development: Prosocial behaviour occurs more often in concrete operational - product of ToM.
Middle childhood: prosocial behaviour requires information-processing skills.
School children tailor their prosocial behaviour to whether they can effectively help, preoperational offer sth useless.
Who is more prosocial?
Individual differences (relatively stable)
Gender difference:
→ Boys more to stand up to a bully
→ Girls comfort the bullied
Small difference in sharing.
Culture difference in modesty about prosocial behaviour:
Japanese kids are more modest about prosocial behaviour
Dutch kids expect praise
Aggression:
Causing (physical/emotional) pain in others.
It is associated with motor and cognitive development.
Aggression types (based on motive for behaviour):
Reactive (impulsive) aggression: direct response to threat/frustration, not well thought.
Proactive (instrumental) aggression: with intent to reach a goal.
Other types of aggression:
Direct aggression: directly visible - most occurring form is physical, peaks around 2.5 years and declines in middle childhood.
Indirect aggression: not directly visible (most common is relational aggression - harming social status), sophisticated social skills needed, peaks around early adolescence.
Aggressive behaviour: Gender differences
Boys show more physical aggresion
Same relational aggression
Overt physical aggression restricted in girls, so mainly relational
Impact of relational aggression bigger for girls.
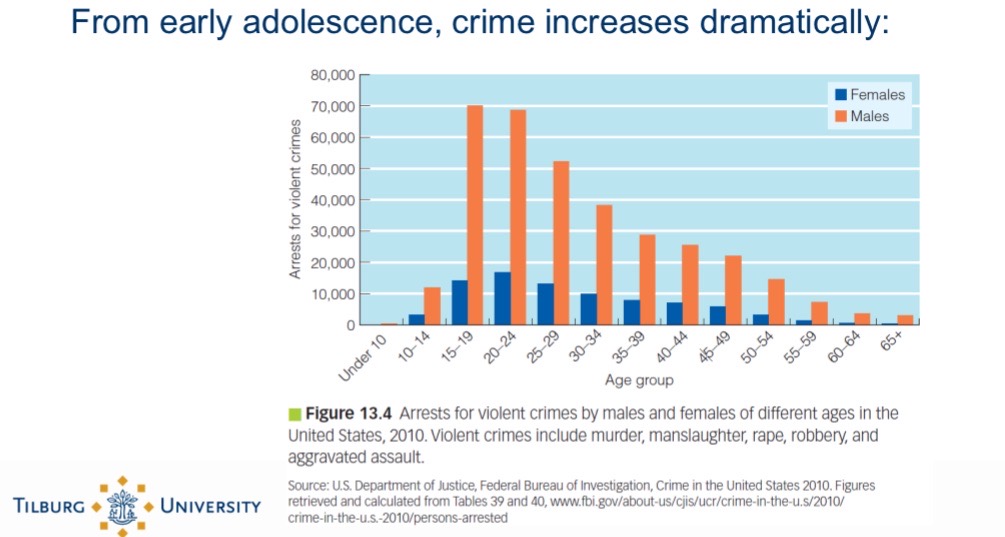
Adolescence: crime rates
Factors affecting juvenile delinquency: Early onset
Family & Environment
Criminal background of parents
Strict/inconsistent discipline
Mental health problems of mother
Alternating caregivers & single parenthood
Low socioeconomic status
Neurocognitive & Developmental Factors
Early neurological impairments
Low motor skills & IQ score
Reading and memory problems
Behaviour and Social Factors
Hyperactivity & self-control problems
Rejection by peers
Interactions with delinquent peers (risk factor late onset)
Additional Factors
Behavioral difficulties in early childhood
Family conflicts
Young age of mother with first child
… but not that they have lost their theory of mind or empathy
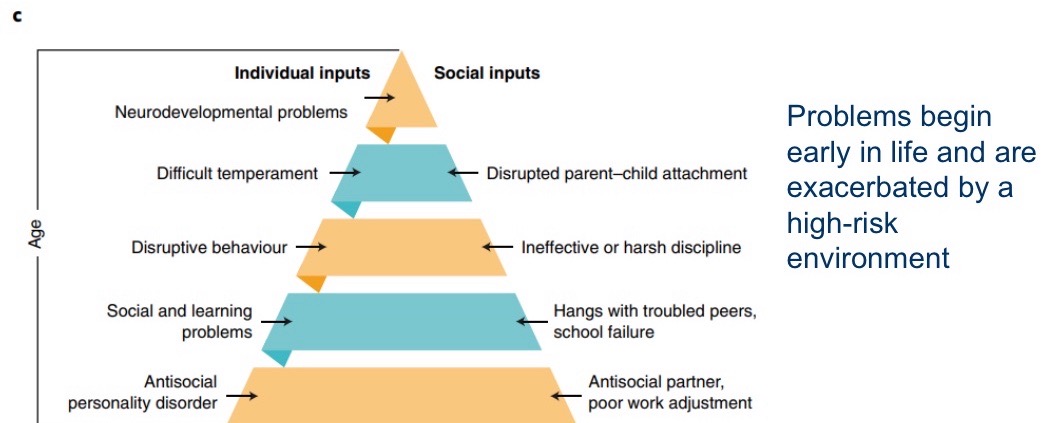
Antisocial and risk behaviour - Moffitt’s theory on 2 types of antisocial behaviout:
Early-onset (life course persistent):
Small % of the population (5), often with neurocognitive deficits, high long-term stability (recidivism), growing up in difficult families/neighbourhood.
Late onset (adolescence-limited): Majority of adolescence demonstrates anti-social behaviour - normative, disappears after puberty, appears to imitate life-course group.
→ same behaviour, different motivations.
Vicious cycle: early onset antisocial behaviour
Why do adolescence in the late onset group copy early onset?
Brain maturation
Age-maturity gap
Brain development:
Self control < emotion!
Increase in levels of neurotransmitters, mainly dopamine → increased risk taking + reward seeking.
Brain is still growing:
Limbic system: almost completely developed in early adolescence
Prefrontal cortex: maturation not finished until adult yeats
Age-maturity gap:
Cognitive and physical maturation
Budding maturation: sexual, autonomy, statue
Social limitations: financial dependence, adult supervision, lack of adult status, societal age restrictions.
Additional considerations:
Not every adolescent demonstrates risk. behaviour, risk behaviour isn’t necessarily an error in calculation - it can be functional: individuation, experimenting, bonding with peers.