Equine Medicine
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
42 Terms
What does colic mean
abdominal pain
What can colic range from (in terms of pain)
mild and self-limiting (gas) to life threatening and grave (intestinal obstruction/torsion)
What does founder mean
lay term for “laminitis”
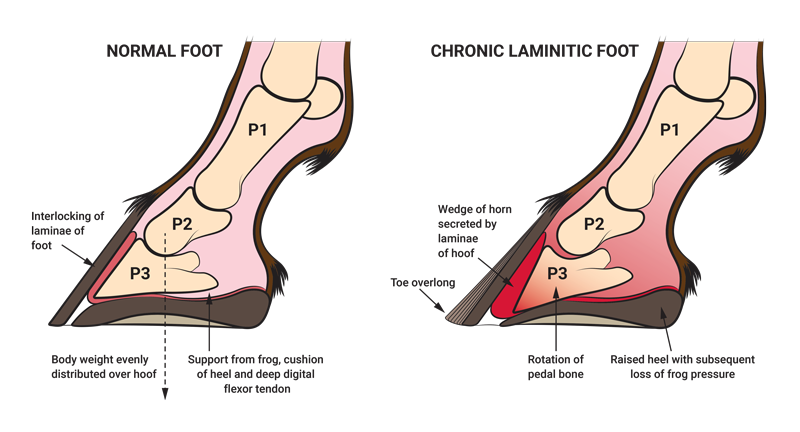
What does laminitis (founder) mean and what is it caused by
inflammation and subsequent separation of the laminae of the hoof
Causes: carbohydrate overload, excess weight bearing, endotoxemia, high temp, anything that offsets the laminae that hold the coffin bone
hallmark clinical sign is severe lameness with bounding digital pulses. P3 rotation or sinking can result from laminar separation
P3 is the coffin bone
usually, the horse will be leaning back on their heels to relieve pressure on their toes
What does the term “off” mean
lame
giving to pressure on a painful limb, quick step
What does tube worm mean
administering dewormer by means of a nasogastric tube
used so the horse won’t spit it up
What does the term “float” mean
Manually or mechanically filing off the sharp points of teeth
horses have hypsodont teeth: teeth that keep growing
sharp edges buccal: superior, lingual inferior
clinical signs when the teeth are way too long are dropping feed/losing weight due to not eating
What does the term “arm” mean
rectal exam
reasons: pregnancy and colic
horses’ rectum are easy to tear
flip sleeve inside out and use lots of tube
gently palpate
don’t want to see blood
What does the term “cut” mean
castrate
What does the term “tying up” mean
myositis/muscle stiffness
happens after working too hard or diet change
Leading a horse
always use a lead rope attached to horse halter
never grasps the halter itself
provides no options if horse were to startle
do NOT coil end of lead rope around your hand
loops could tighten
fold it back and forth and grasp middle of folds
never wrap lead rope or any other line attached to a horse around any part of your body
avoids being dragged
don’t allow horse you’re leading to touch noses w/ unfamiliar horse
can lead the horses to bite or strike another (also applies when you’re mounted)
disease transmission
Tying a horse
tie horse “eye high and no longer than your arm”: tie knot should be at least as high as horse’s eye, and distance from knot to halter should be no more than length of your arm
tie only to safe, solid object, using a quick-release knot or breakaway string
keep fingers out of loops as you tie knot
tie only w/ halter and lead, never w/ bridle reins
Maneuvering around horse
stand near should or next to hindquarters
do NOT stand directly in front of or directly behind a horse when grooming his hand or brushing or braiding his tail
walking behind a horse, go either:
close enough to brush against him, keeping 1 hand on his rump as you pass around
where a kick would have no real force
far enough away to be well out of kicking range
avoid ducking under tie rope
might cause horse to pull back, and you’d be X-treme vulnerable to injury if he did
never kneel or sit on ground when working on distal limbs
remain squatting, so you can jump away in even he startles
be mindful of all 4 feet
Trailering a horse
never fight w/ a reluctant horse to get him into a trailer
seek professional help and retraining, if necessary
once a horse is in trailer, close back door or ramp before you hitch him to trailer tie
unloading: untie horse before opening back of trailer so he doesn’t begin to back out on his own and hit end of rope, causing him to panic and pull back
Turning horse loose
when turning out a horse or pony for exercise or returning him to his paddock or pasture, always turn his head back toward gate
step through gate yourself before slipping halter
avoid his heels in case he kicks them up in delight at freedom
Feeding treats to horses
offer carrot or apple chunks from palm of flattened hand to avoid being accidentally nipped
put treats in a bucket before offering them
Paying attention to horses
stay calm, focused, alert at all times
be aware of surroundings
be mindful of possible spooks
listen to horse
Mucous membranes in horses (physical exam)
pink/moist
CRT < 3 secs
above superior incisors
Skin turgor (physical exam)
pinch skin above eye or lateral neck
not as reliable as mucous membrane
Lung sounds (physical exam)
auscultate all lung fields
clear air movement sounds
barely audible
if we hear crackle, wheezing, or effort, this is abnormal
Borborygmi (physical exam)
gastrointestinal sounds/gurgle sounds of abdomen
all 4 abdominal quadrants
cecum on right side and small intestine on left
regular/consistent
not hyper or hypo motile
Temperature (equine vitals)
98-101F
mild variation depending on ambient temp, activity, anxiety, etc
rectal thermometer
Heart rate (equine vitals)
40 bpm
28-44 bpm
auscultate: place stethoscope on left thorax at elbow
feel pulse: submandibular
Respiration (equine vitals)
8-12 breaths per min
auscultate: place stethoscope on thorax
visualize: movement of thorax and abdomen
Digital pulses (equine vitals)
palmar/ plantar digital vein-artery-nerve bundle
artery will pulse
palmar/plantar axial/abaxial aspects of metacarpal-phalangeal joints
should be faint or absent (otherwise think laminitis, joint infection)
really strong pulse → bad
hoof should feel cooler than body
hot hoof wall → bad
What are the core vaccinations for horse
WN/EWT: West Nile Virus Vaccine
RV: rabies vaccine
What are the risk-based vaccinations for horses
Flu/Rhino
Strangles
EHV: equine herpes vaccine
EVA: equine arteritis vaccine
Leptospirosis
transmitted through urine so if there’s a lot of rain/standing water, this vaccine is def needed
Potomac Horse Fever
Botulism
Venipuncture- IV (horses)
Jugular groove (vein)
brachiocephalicus
sternomandibularis
jugular stays superficial
jugular vein is v close to carotid artery which goes from heart to brain

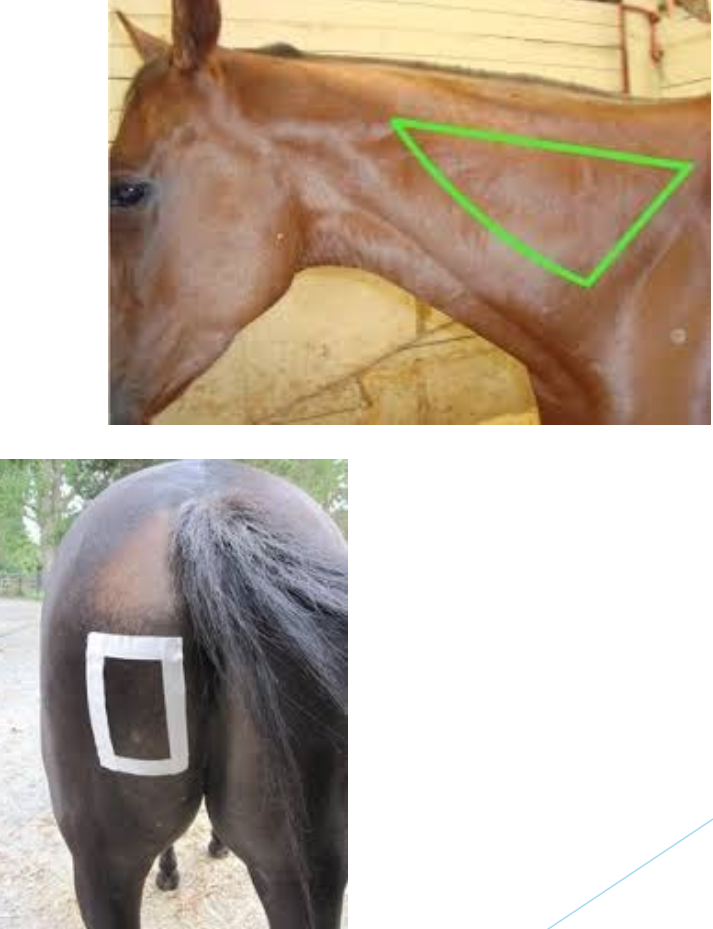
Injections- IM (horses)
Cervical
cervical vertebrae
scapula
nuchal ligament
Rear
semimembranosus
semitendenosus
Layer 1: Wound Dressing (Bandaging)
should be non-stick
if a wound is present, primary or contact layer should be a wound dressing
appropriate dressing may vary depending on type of wound and stage of healing
most commonly used wound dressing is a sterile non-adherent gauze pad
Layer 2: Padding (Bandaging)
intermediate bandaging layer consists of soft, absorbent padding material to cushion and protect the limb, and to help evenly distribute pressure applied by bandage
roll cotton
sheet cotton
combine cotton (knowns as Gamgee)
commercial cotton or flannel “pillow” or quilted wraps
can be washed and reused
smoothed w/ a cling gauze wrap
Layer 3: Bandage (Bandaging)
third and outermost bandaging layer consists of bandage itself, which secures other layers and provides compression
flexible cohesive bandages “Vet Wrap”
3M Vetrap
Powerflex
Co-Flex
Reusable bandages w/ Velcro fasteners
fleece
cotton
polyester knit bandages w/
4 and 6 inches wide
narrower bandage can result in pressure points and general constriction of limb
On top of the layer 3 of the actual bandage, there’s a protective layer. What are 2 things that can used for the protective layer
elasticon
holds bandage in place
prevents slipping
duct tape
waterproof protection
8 principles of bandaging
begin w/ clean, dry legs and bandages
trapped dirt and debris can cause skin irritation/wound irritation
moisture can lead to a fungal infection
apply correct tension
greatest challenge
applied too loose, bandage will fail to provide adequate support, but may slip out of place or come undone
create pressure points on back of leg that can cause damage to tendons (“bandage bow”)
wrapped too tightly will impede circulation in limb and can also result in tendon injury
ideal tension for a correctly applied leg bandage = snug
tight enough to remain securely in place
not too light restrict blood flow in limb
make wraps smooth and even
bandage and padding underneath should lie flat and smooth
no wrinkles, bunches, or ridges that could cause pressure points
leg bandages wrapped in spiral pattern
each wrap made around leg, should overlap preceding layer by about 50%
ensure consistent, even distribution of pressure
provide adequate padding
inadequate amt of padding → construction on limb, inhibiting blood flow and creating pressure points that can lead to injury
layer of padding should be at least one inch in thickness in order to adequately cushion and protect leg
always make sure there’s ~ inch of padding showing above and below bandage
wrap from front to back, outside to inside (counterclock on left legs, clockwise on right)
ensures tension from bandage is applied to front of leg rather than on delicate tendons at back of leg
horse ppl expect this
start wrap over bond at inside front of leg
never start or finish wrap over tendons
may cause damage or over joint as constant movement will loosen bandage and may cause it to bunch or unravel
horse ppl expect this
standing bandages
provide protection, mild support, and warmth to tendons and ligaments in horse’s lower leg
wrap legs in pairs
check leg bandages frequently and re-bandage if necessary
general rule
standing bandages shouldn’t be worn for longer than 12 hrs at time
wound bandages should usually be changed every day
Clinical Signs of Colic
stoic, depressed
laying down (up and down)
inappetent
bruxism (grinding teeth)
biting at abdomen
restlessness
rolling excessively
abrasions over eyes and on hips
violently thrasing
History taken while examining for colic
when was last time horse appeared normal
when did horse last eat
what its usual diet
when did it last defecate? what did stool look like
has it colicked before
are any other horses on property displaying similar signs
reproductive status
deworming history
travel history
history of dental care
primary use of horse
what meds have been administered recently
Physical Exam
abnormal signs w/ colic
Tacky MM
variety of colors like bright red, fuchsia, purple
toxic line = endotoxemia
injected sclera (blood shot eyes)
normothermic
sweating
tachycardia
tachypnea (high respiration rate)
decreased or absent GI sounds
Diagnostics (w/ colic)
NG tube
esophagus is on left side and trachae is on right
you’ll smell and hear the correct side
rectal palpation
abdominocentesis
abdominal ultrasound
clinicopathologic analysis
don’t do radiographs bc waste of time
Surgical candidate or not (assoc w/ colic)
Stabilize
IV cath
IV fluids
Banamine/Bute
no banamine and dex together
butorphanol
xylazine
buscopan
NG tube
oil, epsom salt, H2O
walking
enema
referral
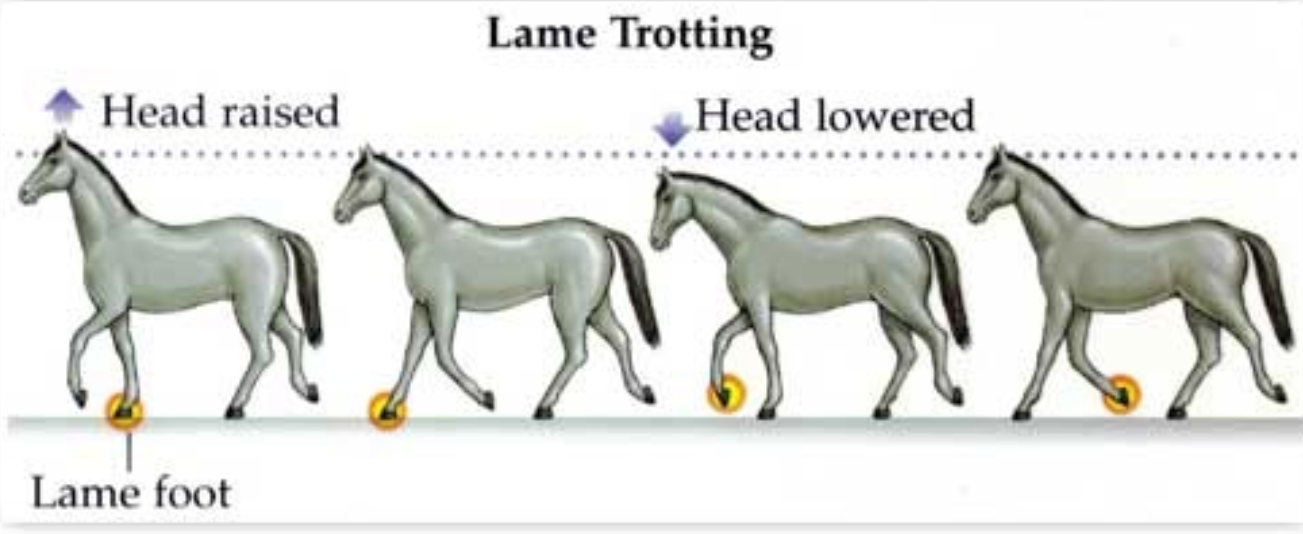
Lameness Exam/ Grades
evaluated at a trot
Lameness on a scale from 0-5
0= no lameness observed @ time of exam
1= lameness difficult to observe and not consistent, regardless of circumstances
2= lameness difficult to observe at walk and trot, but consistent under certain circumstances, such as trotting in a circle
3= lameness consistently observable at a trot in all circumstances
4= lameness apparent at a walk
5= lameness w/ minimal (toe-touching) to non-weight bearing
Flexion Tests (for Lameness Exams)
holding leg in a flex for like 30 secs and let them trot after bc first 3 steps will be worst/show if there’s a prob
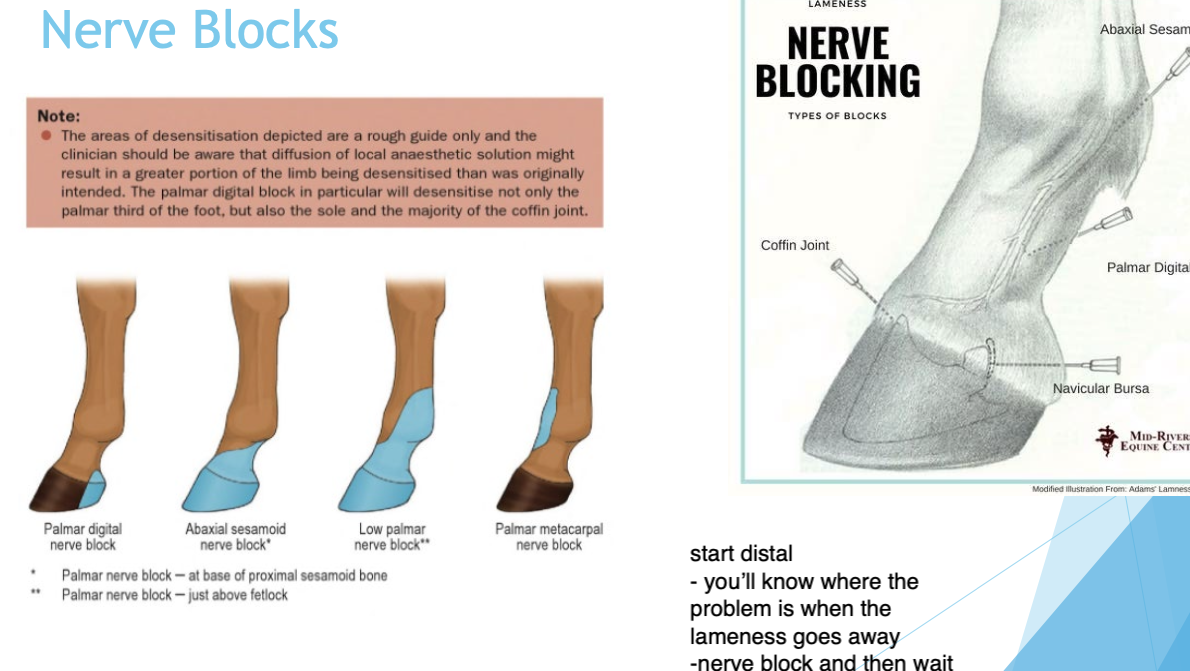
Nerve Blocks (Lameness Exams)
Use carbocaine
Start distal then work your way up the limb (with shot of carbocaine)
you’ll know where the problem is when the lameness goes away
Nerve block shot → wait ~ 10 mins → trot exam