Ergogenic Aids: Framework and Examples (Part II)
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
if you were to design a new PED, what 2 big things should you consider?
-What type of athlete is it helping?: endurance, speed, or power athlete?
-What physiological mechanism(s) would be affected that result in better performances?
List of ergogenic target sites
-Muscle mass
-Muscle contraction (nerve, EC coupling like at the NMJ)
-Delay fatigue
-Substrate availability (ex: glycogen, creatine)
-Energy availability (more immediate, fat use, or CHO sparring)
-Control muscle soreness or pain (*pain part of brains evol survival instinct)
-Temperature regulation (*more concerned if hot enviornment bc generate a lot of heat)
-Hydration
-Electrolyte balance
-Oxygen delivery (airway, lungs, capillary vasodilation)
Blood volume, Hct, Hb (for thermoreg or O2 delivery), VC, more mito, etc.
Fatigue: Organized around power/speed OR endurance events
Power/Speed events
-muscle mass
-CNS & sympathetic stimulation
-acidosis (*ex: Wingate)
-depletion of PCr
Endurance events
-muscle glycogen depletion
-lactate threshold/accumulation (acidosis)
-low blood [glucose]
-fat oxidation rate
-diminished O2 delivery
-dehydration
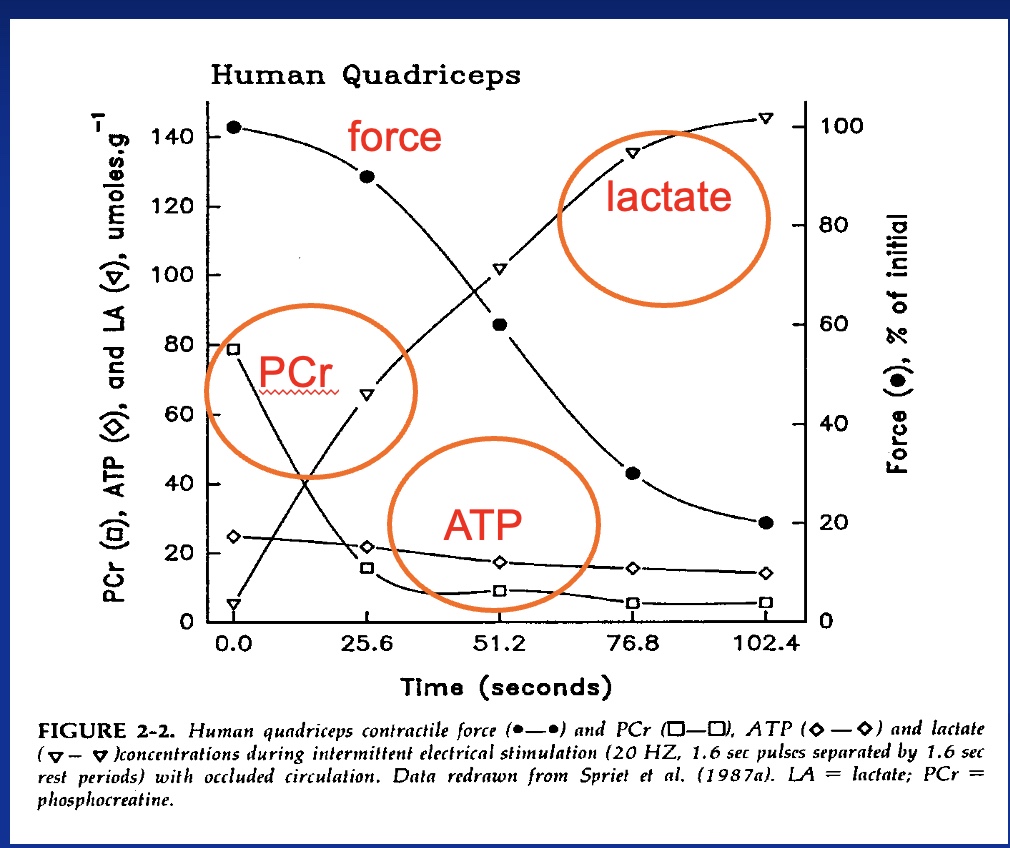
High-intensity exercise effects on muscle metabolites
-Force down
-PCR down
-ATP down (usually constant)
-lactate up
*study: stop blood flow than used electrodes to contract muscles
Endurance training adaptations
-increase VO2max (~15%)
-increase cardiac output (~15%)
-increase mitochondrial volume (2X) (*in slow twith fibers)
-Lactate threshold shifted to higher intensity
-increase ability to use fats (spares glycogen)
*any compound that could mimic these would help
Designing an Aid based on Physiology example: Increase Muscle Mass
We Know
-Requires stimuli (e.g. >75% 1RM and ~8 reps)
-Need increased protein synthesis
Involves mTOR signaling (*promotes growth), DNA, RNA, protein translation
-Need decreased protein degradation
Increase stimuli:
-Training (*periodized program)
-Creatine (*so get 1 more rep out, training volume slightly higher; water retained, gain 1-2lb)
Increase protein synthesis
-Protein (*MPS higher w/ meals)
-Anabolic steroids (*target genes boost PS)
-Insulin (weaker) (*increase after meal to store)
-Growth hormone -> IGF-1 (weaker) (*naturally higher and lower; high in morning)
Decrease protein degradation
-Anabolic steroids (*down regulate genes in MPB)
-Insulin (*goal is to store, so limits breakdown)
Designing an Aid based on Physiology example: Delaying Fatigue (overview)
-FACT: Metabolic acidosis contributes to fatigue
-QUESTION: If you could prevent acidosis, could you do more? (bicarbonate loading…)
effects of acidosis and bicarbonate loading
Intramuscular effects of acidosis
-lower PFK, phosphorylase
-lower Ca2+ sensitivity
-lower cross-bridge force output
-lower ATP turnover
-slows recovery rate
*for all: prod less force
Effects of bicarbonate loading
-higher plasma pH (*which can be transmitted to muscles)
-speeds H+ and Lactate transport from muscle
*CO2 + H20 <-> H+ + HCO3- (*CO2 makes cookies/cake puffy)
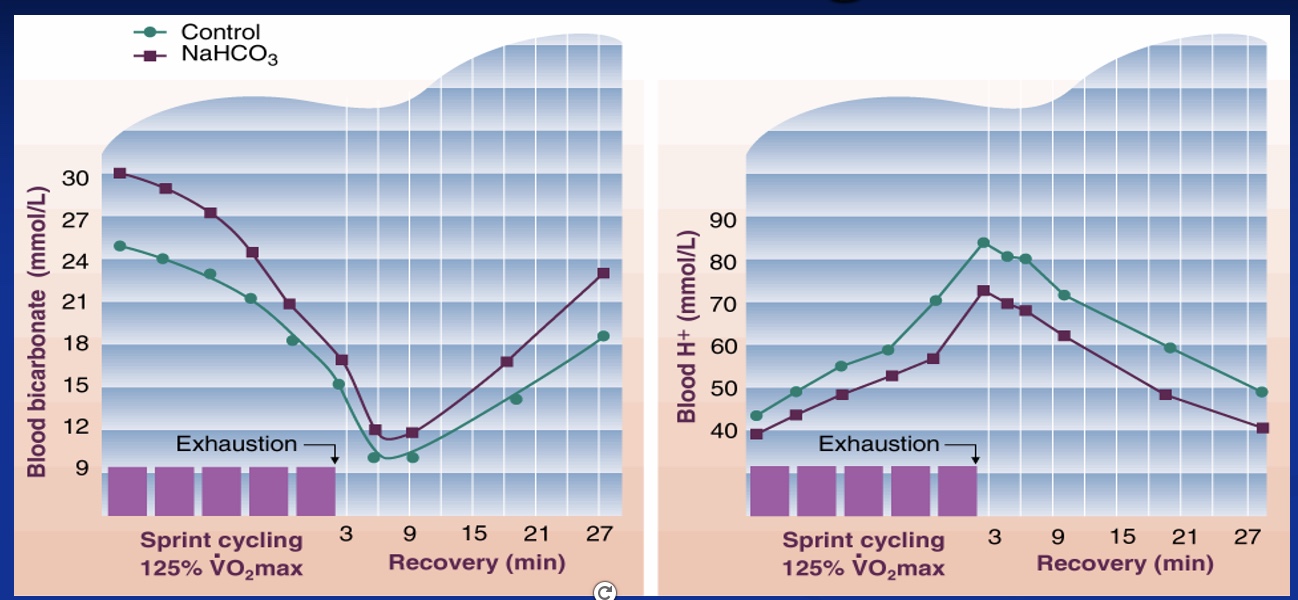
Bicarbonate Loading: Dr. P bicycle sprint test results
-Not all studies report performance benefits
-dependent on dosing
-benefits maximal exercise of 1-10 min
-GI distress (*so likely never would be used bc threw up)
*left graph: bicarb group higher levels but drop bicarb as use it up
*right graph: concentration H+ higher if no bicarb; pH higher if on bicarb
Bicarbonate Loading: lotion research
-no improvement in blood buffering capacity or exercise performance if apply topical sodium bicarbonate
Bicarbonate Loading: 40km bicycle time trail test results
*ingested bicarbonate and carbohydrate gels 2 hours before, then did a 40km time trial; aerobic but above lactate threshold; forms gel and enteric coated so through stomach and get to SI (so no GI distress)
-Intro: useful if short time period/less than 10 min
-Purpose: 40km time trials
-Methods: 14 male cyclists, RCT, double blind, everyone got placebo and product
-Results: if consumed bicarb were 1 minute faster, increased buffering, no GI issues
-Ken’s Conclusion: $18/serving (worth the money?)

Designing an Aid based on Physiology example: Increasing O2 Delivery
*doping dif contexts, but usually means illegal; more useful for aerobic activity
-Blood doping via transfusion (self or donor)
increase RBC concentration (Hct=%blood that is RBC, so higher O2 carrying capacity; iron in center)
RBC live for 4 months; so test RBC age to see if doping (lot of cells the same age=doping)
-Breathing 100% O2
-EPO (Epogen, Procrit)
stimulates RBC production (higher Hct) (*made in red bone marrow)
-Roxadustat:
Brand name Evrenzo, an anti-anemia medication that is a HIF prolyl-hydroxylase inhibitor that increases endogenous production of EPO (*prod more EPO than normal)
-Altitude + training (increases RBC production)
live high, train low (*hard to train well at high altitude, so go lower to train hard)
*perception factor in everything; still affect of altitude indoors
Increasing Energy Supply
-Carbohydrate availability: feeding before/during competition
*in any sport can become carb deficient; likely if over 1 hour
-Creatine: important for energy production during power/speed events
Creatine: Background and benefits
Background
•Non-essential, liver makes it, meat eaters get 50% of need
•Naturally occurring in animal products (primarily meat)
•Supplementing increase cellular levels (95% in muscle, rest in brain and nervous tissue)
Benefits
•Increased volume of training
•Increased muscle mass
•Increased repeat sprint performance (*rebuild PCr inbetween intervals)
•May benefit brain health
Stimulants: use and examples
Use
-For cognition (focus, alertness, fatigue resistance/central govener)
-Improved reaction time
-As sympathomimetics
stimulates SNS (ex: higher HR, mobilized fuels; some golfers/shooters take beta blockers to slow down HR)
Examples
-Amphetamine (inc Adderall)
*for ADHD; going too slow before, match up perception and reality
-Ephedrine(legal)/Pseudoephedrine (not legal; congestion) (Ephedra—Ma Huang: reves up metabolism, like taking meth)
-Methylphenidate (inc Ritalin)
-Cocaine
-Modafinil (aka Provigil)
*ex: Rx for army figther pilots
-Caffeine

Caffeine
-May enhance maximal performance
if < 5 min or > 30 mins (*very short or longer; not good for a 5k)
-May decrease performance due to side effects
insomnia, heart palpitations, tremors, anxiety, nervousness, GI distress
-Addiction possible (*tradeoffs)
Withdrawal symptoms evident (*could periodize)
-Diuretic at higher levels
Heat stroke a concern
*pure caffeine is a diuretic; otherwise having it w/ fluid
*structure: all things made out of the same stuff

is caffeine legal in sports?
-Intake no longer restricted, except by the NCAA (only)
-Urinary concentrations tested
15 mcg/ml of urine (NCAA) (*a lot; for reference ex: 1 soda=50mg; 1 cup coffee=100mg; energy drink=200mg)
Exceeded with 500 mg dose in some 2 hr prior
-Individual variations in metabolism and excretion
-Ergogenic effects are present when urine levels below limits (*don’t need max)
*caffeine effect HR at rest, but not during exercise
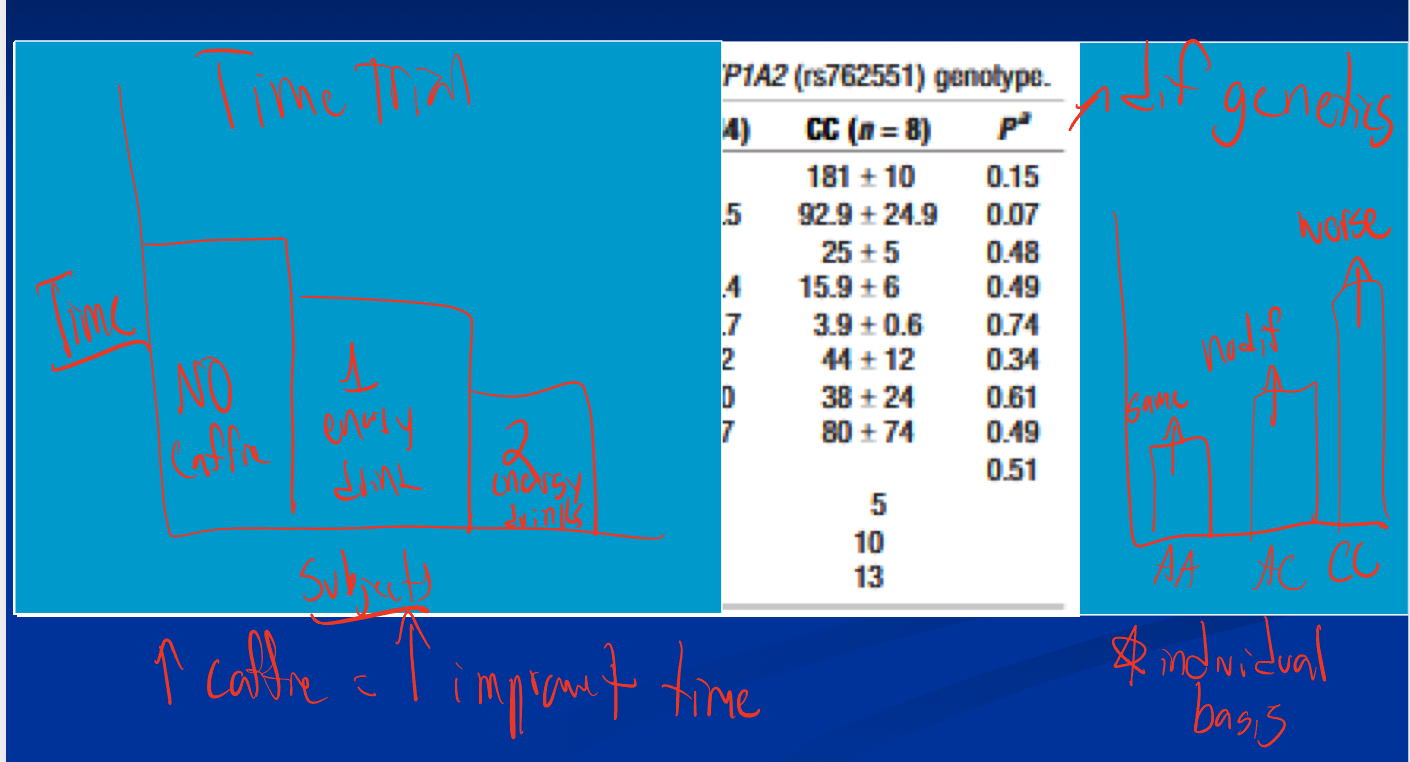
study: caffeine and genotype in endurance performance athletes
*if high intensity and consume caffeine: better reaction time; endurance and caffeine= change perception/RPE (so couple seconds faster each mile)
-Time Trial on own: higher caffeine=more improvement
-Time Trail w/ dif genetics that break down caffeine: CC gene people had worse improvement if took caffeine, most people AA (see improvement) or AC (see no difference)
*shows individual basis
Anabolic Agents: background and examples
Background (*overall=masculine effects)
•Important uses clinically; Includes FDA approved; Veterinary products consumed by humans; Banned in the 1970’s; Popular in anti-aging circles; Black market
Examples
-Anabolic steroids (various androgens)
-Selective androgen receptor modulators (SARMs)
increase # of receptors so more effect
-Growth Hormone (and GNRH)
-Beta-HMB (beta-Hydroxy-beta-MethylButyrate)
prevents lysine from being broken down as easily
Meldonium
-Latvian drug, does not have FDA approval for US usage
-Placed on world anti-doping agency (WADA) list in Jan 2016
-Used to treat coronary artery disease, anti-ischemic; A metabolic modulator, probably increases angiogenesis (*growing blood vessels, increase O2 delivery capacity)
-Appears beneficial on cerebral circulation and CNS, too (ex: hand eye coordination)
-Entire U18 Russian ice hockey team; Boxers, middle and long distance runners, wrestlers, judo, cyclists, biathletes all tested positive recently; Majority were Russian/Ukrainian athletes

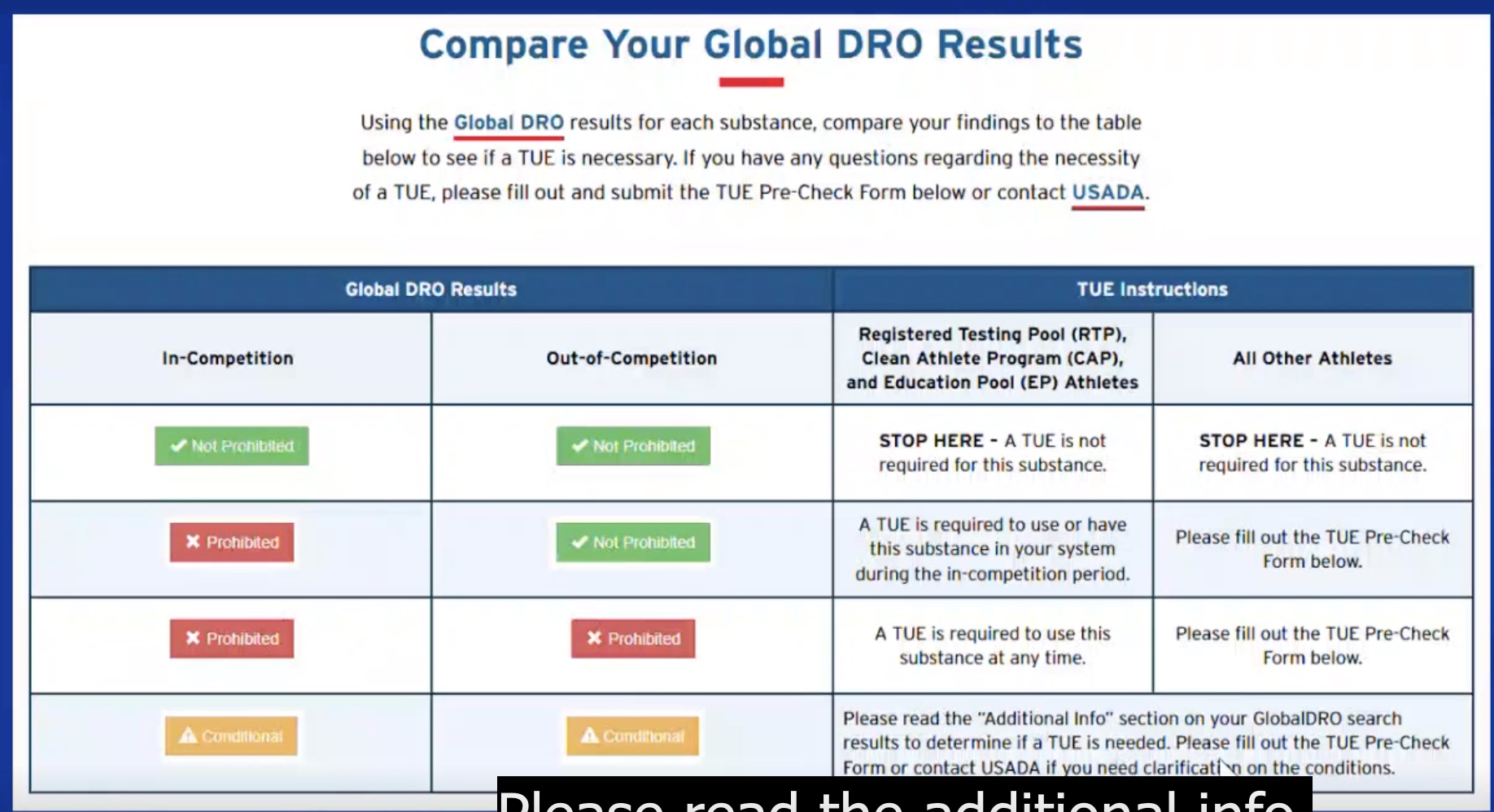
Therapeutic Use Exceptions
-could use something that is banned if have a Rx for a condition
*ex: asthma and inhaler
Evaluating an Ergogenic Aid: Is there any scientific evidence supporting the ergogenic value?
-Are the studies simply basic research done in animals/clinical populations or have the studies been conducted on athletes?
-Were the studies well controlled?
-Do the studies report statistically significant results or are claims being made on non-significant differences or reported trends?
-Do the results of the studies cited match the claims made about the supplement?
-Were results of the study presented at a reputable scientific meeting and/or published in a peer-reviewed scientific journal?
-Have the research findings been replicated at several different labs?
*Major problem in general! (ex: psychology)
-Were the studies done by the company or independent labs? Who paid for the studies?
is the supplement legal and safe? (questions to ask yourself)
-banned?
-long term safety?
-reproductive toxicology?
-side effects?