Pulmonary Neoplasms - MedPath
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
What does this refer to
______ : are abnormal tissue growths; may be benign or malignant
Neoplasms
What does this refer to
Primary vs. metastatic lung tumors
Lung cancer is the leading cause of cancer-related deaths worldwide
Pulmonary neoplasms
What does this refer to
Benign vs. Malignant
Primary vs. Secondary (metastatic)
Non-small cell lung cancer (NSCLC) vs. Small cell lung cancer (SCLC)
Classification of Pulmonary Tumors
What does this refer to
Tobacco smoke: primary risk factor
Environmental exposures: radon, asbestos, pollution
Genetic predispositions
Etiologic factors
What does this refer to
Most common: Hamartomas (contain cartilage, fat, connective tissue)
Usually peripheral and asymptomatic
Detected incidentally on imaging
Slow growing
Benign Pulmonary Tumors
What does this refer to
They consist of a mixture of normal lung tissue elements, including cartilage, fat, connective tissue, and smooth muscle, with entrapped respiratory epithelium.
Composition of Hamartomas
What does this refer to
They often appear as well-defined, coin-shaped nodules on imaging, sometimes with characteristic "popcorn-like" calcification or fat.
Appearance of Hamartomas
What does this refer to
Non-Small Cell Lung Cancer (NSCLC) ~85%
Small Cell Lung Cancer (SCLC) ~15%
Other: carcinoid tumors, mesothelioma, lymphomas
Malignant Pulmonary Tumors
What does this refer to
Smoking: responsible for ~90% of lung cancer cases
Heavy smokers have 20 times’ greater chance of lung cancer than nonsmokers
Smoking is related to cancers of the larynx, oral cavity, esophagus, and urinary bladder
Environmental or occupational exposures: radon, asbestos, air pollution
Genetic mutations: inherited or acquired
Etiologic factors
What Non small cell lung cancer (NSCLC) subtype does this refer to
peripheral, most common in non-smokers
Adenocarcinoma
What Non small cell lung cancer (NSCLC) subtype does this refer to
: central, associated with smoking
Squamous cell carcinoma
What Non small cell lung cancer (NSCLC) subtype does this refer to
: undifferentiated, poor prognosis
Large cell carcinoma
What does this refer to
Accounts for ~15% of cases
Highly aggressive and rapidly growing
Strongly associated with smoking
Small cell lung cancer (SCLC)
What does this refer to
Driver mutations: EGFR, KRAS, ALK, BRAF (NSCLC); TP53, RB1 (SCLC)
Promote proliferation, evade apoptosis, enhance survival
Targetable mutations guide therapy decisions
Molecular Pathogenesis
What does this refer to
______ mutation → increased tyrosine kinase activity
Downstream signaling: RAS-RAF-MEK, PI3K-AKT pathways
Targeted by _______ inhibitors: erlotinib, osimertinib
EGFR Pathway in NSCLC
What mutation is the following
_______ : associated with poor response to therapy
Found in younger, non-smoking populations
KRAS
What mutation is the following
_______ rearrangement: targetable with crizotinib, alectinib
Found in younger, non-smoking populations
ALK
What does this refer to
Initiation: DNA damage (carcinogens)
Promotion: clonal expansion
Progression: acquisition of malignant phenotype
Multistep Carcinogenesis
What does this refer to
Metaplasia → Dysplasia → Carcinoma in situ → Invasive cancer
Loss of differentiation and architecture
Increased mitotic activity and pleomorphism
Histopathological Changes
What does this refer to
Composed of stromal cells, immune cells, extracellular matrix
Supports tumor growth, angiogenesis, immune evasion
Dynamic and interactive system
Tumor Microenvironment
What does this refer to
Tumors secrete vascular endothelial growth factor (VEGF) to promote blood vessel formation
New vessels are leaky and irregular
Targeted by anti-VEGF therapies (e.g., bevacizumab)
Angiogenesis in lung cancer
What does this refer to
PD-L1 (Programmed Death-Ligand1) expression on tumor cells binds PD-1 on T cells
Suppresses immune response
Checkpoint inhibitors restore T-cell activity
Immune evasion mechanisms
What does this refer to
Tumor cells degrade extracellular matrix via proteases
Enter blood/lymphatic vessels
Seed distant organs: brain, bone, liver, adrenals
Invasion and Metastasis
What does this refer to
Occur due to ectopic hormone/cytokine production
SCLC: SIADH, ectopic ACTH (Cushing), neurologic syndromes
NSCLC: hypercalcemia (parathyroid hormone related protein-PTHrP), hypertrophic osteoarthropathy
Paraneoplastic syndrome
What paraneoplastic syndrome is associated with SCLC
SIADH, ectopic ACTH (Cushing), neurologic syndromes
What paraneoplastic syndrome is associated with NSCLC
NSCLC
What does this refer to
Cough, hemoptysis, wheezing, chest pain, weight loss
Recurrent pneumonia, hoarseness (recurrent laryngeal nerve)
Superior vena cava syndrome in central tumors
Symptoms of Lung Cancer
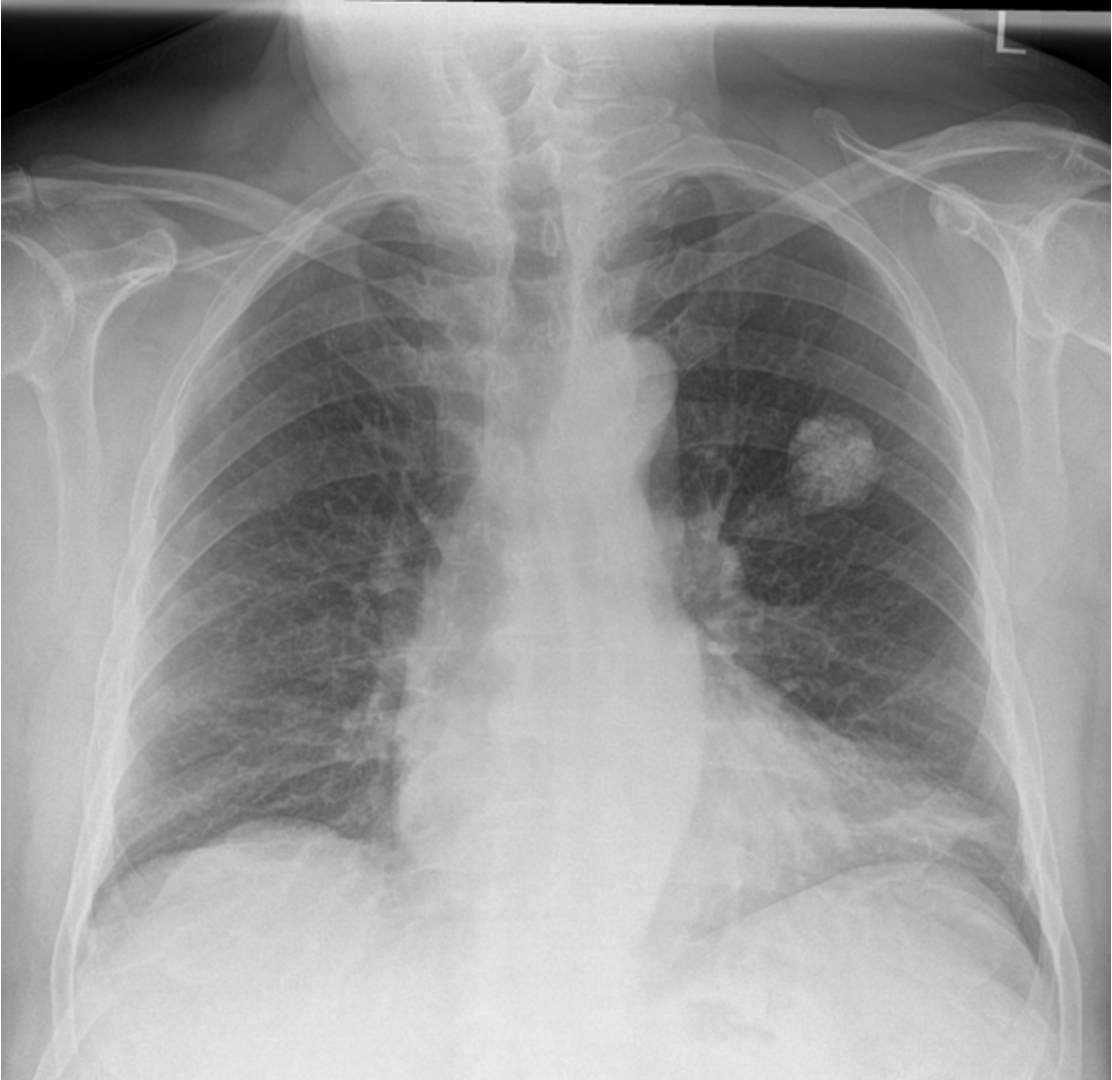
What does this refer to
CXR: mass, atelectasis, pleural effusion
CT: defines size, lymph node involvement, metastases
PET: identifies metabolically active disease
Radiologic Appearance
What does this refer to
Bronchoscopy: visual and biopsy of central lesions
Endobronchial ultrasound (EBUS): guides lymph node sampling
Transthoracic needle biopsy for peripheral nodules
Bronchoscopy and Biopsy
What radiology technique tells you “: mass, atelectasis, pleural effusion”
CXR
What radiology technique tells you “: defines size, lymph node involvement, metastases”
CT
What radiology technique tells you “: identifies metabolically active disease”
PET
What is used to “visual and biopsy of central lesions”?
Bronchoscopy
What is used to “guides lymph node sampling”
Endobronchial ultrasound (EBUS)
What is used for for peripheral nodules
Transthoracic needle biopsy
Given the cytologic and histologic information below, what would you diagnose the patient with
“glandular structures, mucin production”
Adenocarcinoma
Given the cytologic and histologic information below, what would you diagnose the patient with
“keratin pearls, intercellular bridges”
Squamous
Given the cytologic and histologic information below, what would you diagnose the patient with
“small blue cells, nuclear molding, necrosis”
SCLC
What does this refer to
T: tumor size and local invasion
N: nodal involvement
M: presence of distant metastases
Stage guides prognosis and treatment
What does this refer to
Surgical resection (stages I-IIIA)
Adjuvant chemotherapy, radiation
Targeted therapies and immunotherapies for advanced stages
NSCLC Treatment Strategies
What does this refer to
Chemo-radiotherapy mainstay of treatment
Limited stage: curative intent
Extensive stage: palliative, often rapid relapse
SCLC Treatment Strategies
What does this refer to
EGFR, ALK, ROS1 inhibitors for mutation-positive tumors
Improved survival and reduced toxicity
Resistance mutations (e.g., T790M) can develop
Targeted Therapy in NSCLC
What does this refer to
Checkpoint inhibitors (PD-1/PD-L1 blockers)
Effective in high PD-L1 expression
Improves overall survival in NSCLC
Role of Immunotherapy
What does this refer to
Checkpoint inhibitors (PD-1/PD-L1 blockers)
Effective in high PD-L1 expression
Improves overall survival in NSCLC
Surveillance and Follow-Up
What does this refer to
5-year survival depends on stage and histology
Early-stage NSCLC: ~60-70%
SCLC and late-stage NSCLC: <15%
Prognosis
What does this refer to
Rare, aggressive cancer of pleura
Strongly linked to asbestos exposure
Long latency period (20–50 years)
More common in men and older individuals
Asbestos fibers cause chronic inflammation
DNA damage leads to mesothelial cell mutation
Tumor spreads along pleural surfaces
Invades chest wall, diaphragm, and pericardium
Mesothelioma
What does this refer to
Neuroendocrine tumors (NETs) of the lung
Classified as typical or atypical
Less aggressive than small cell carcinoma
May secrete hormones (e.g., serotonin)
Origin from neuroendocrine Kulchitsky cells
Uncontrolled proliferation due to mutations (e.g., MEN1)
Tumor may produce bioactive amines
Can cause carcinoid syndrome if metastasized
Carcinoid tumors
What does this refer to
: asbestos-related, pleural origin, aggressive
Importance of early recognition and pathology
Both require multidisciplinary management
Mesothelioma
What does this refer to
“neuroendocrine tumors, variable behavior, hormone-secreting”
Importance of early recognition and pathology
Both require multidisciplinary management
Carcinoid Tumors