Looks like no one added any tags here yet for you.
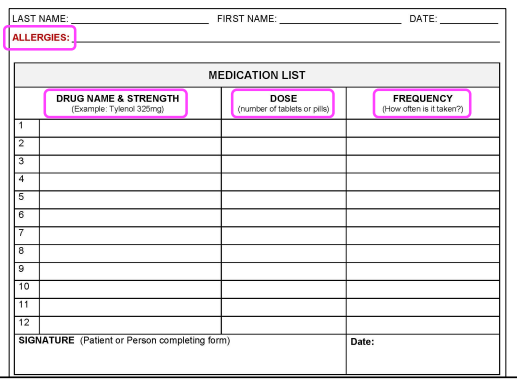
Anatomy of a Medication List
Medication List = Patient Safety Tool
• Allows an Optometrist to:
⎻ Identify the most accurate list of medications a patient is and should be currently taking.
⎻ Reconcile a patient’s current medication history to their medical history and resolve discrepancies with other providers of care.
⎻ Reduce potential/actual adverse drug events
Medication List
Should be viewed as a reflection of the health status of our patients and as a potential tool for population health management.
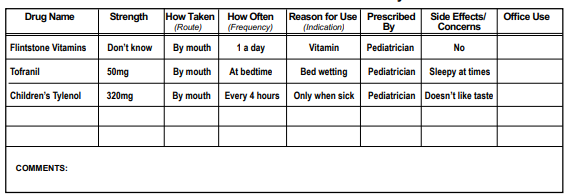
TEACHING CASE: Office Observation/Medication History
Double checl/verify dose of Tofranil and reason for use
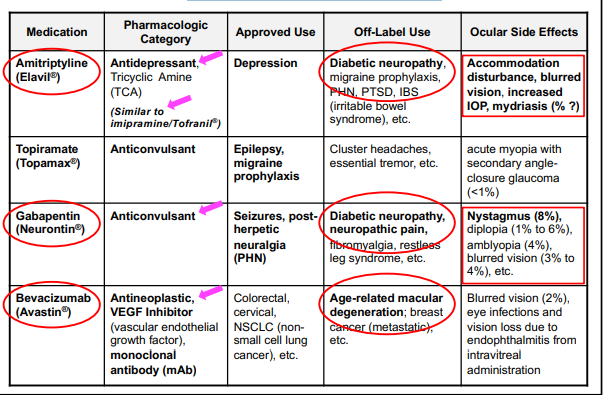
TEACHING CASE: Tofranil® (Imipramine) Drug Information
• Pharmacologic Category – Antidepressant, Tricyclic Amine (TCA)
• Indications (FDA Approved) – Depression and Enuresis
• Off-Label Use – Neuropathic Pain (e.g., diabetic neuropathy)
• Dosing Pediatric (Enuresis – FDA approved indication) – Children ≥6 years and Adolescents: Oral (Initial) – 10 to 25 mg → usually start at low dosages and titrate up as needed
Adverse Reactions of Tofranil
– Ophthalmic: Accommodation disturbance, angle-closure glaucoma, blurred vision, mydriasis
– Central Nervous System: Agitation, fatigue, restlessness
Off-Label Medication Use
Off-label use is not an approved FDA indication and means the medication is being used in a manner not specified in the FDA's approved packaging label or insert.
From the FDA (Off-Label Medication Use): “If physicians use a product for an indication not in the approved labeling, they have the responsibility to be well informed about the product, to base its use on firm scientific rationale and on sound medical evidence, and to maintain records of the product's use and effects.”
Off-Label Medication Use Examples
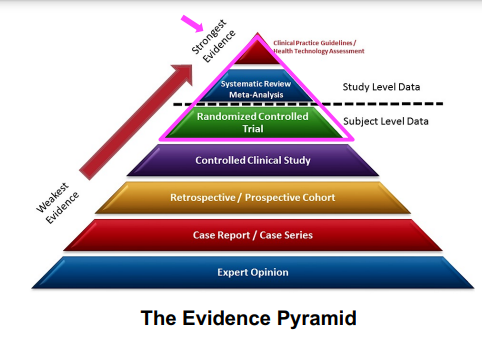
Evidenced-Based Medicine
Evidence-based medicine is the care of patients using the best available research evidence to guide clinical decision making.
• A common approach with guidelines is to grade the strength of the recommendation and quality of the evidence separately.
• Strength (or Class) of Recommendation – Based on Classes (1-3)
o Risk vs Benefit
• Quality (or Level) of Evidence – Based on Levels (A-C)
o Patient Populations