3. Panic Disorder
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
What is the study of interoception in terms of an approach to mental health?
transdiagnostic approach to mental health
interoception is implicated in many conditions
potentially a transdiagnostic mechanism
How does the proper functioning of interoception relate to mental health?
allows accurate experience of the body and the self
trust to provide consistent, reliable sensory information
enables engagement in everyday activities
impairment of this is characteristic of many mental health condition
what might the interoceptive deficit be in psychiatric disorders?
different processing on interoceptive signals
bias in reporting interoceptive signals
What did Elliot and Pfeifer (2022) find in their survey responses measuring interoceptive sensibility and anxiety during COVID-19
interoceptive constructs correlate with anxiety
worry, trust, attention regulation
What is measured on the Body Awareness Questionnaire?
attentiveness to normal non-emotive body processes
detect small changes in normal functioning, and ability to anticipate bodily reactions
What did Adams et al (2022) find in meta-analysis of interoceptive accuracy tasks and anxiety?
55 studies using different measures of IA
clinical and subthreshold samples
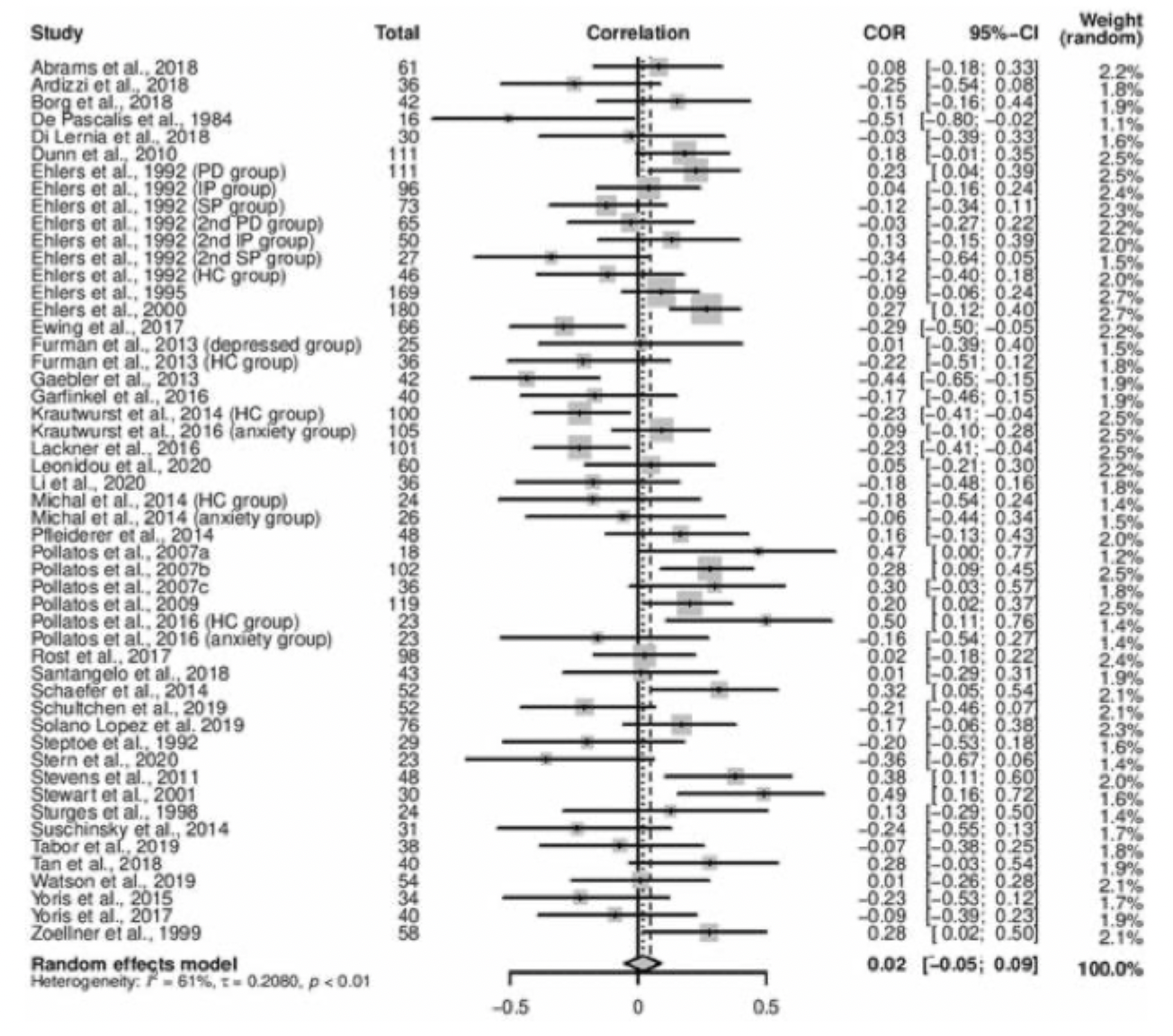
no relationship between IA and anxiety
no effect of task or sample

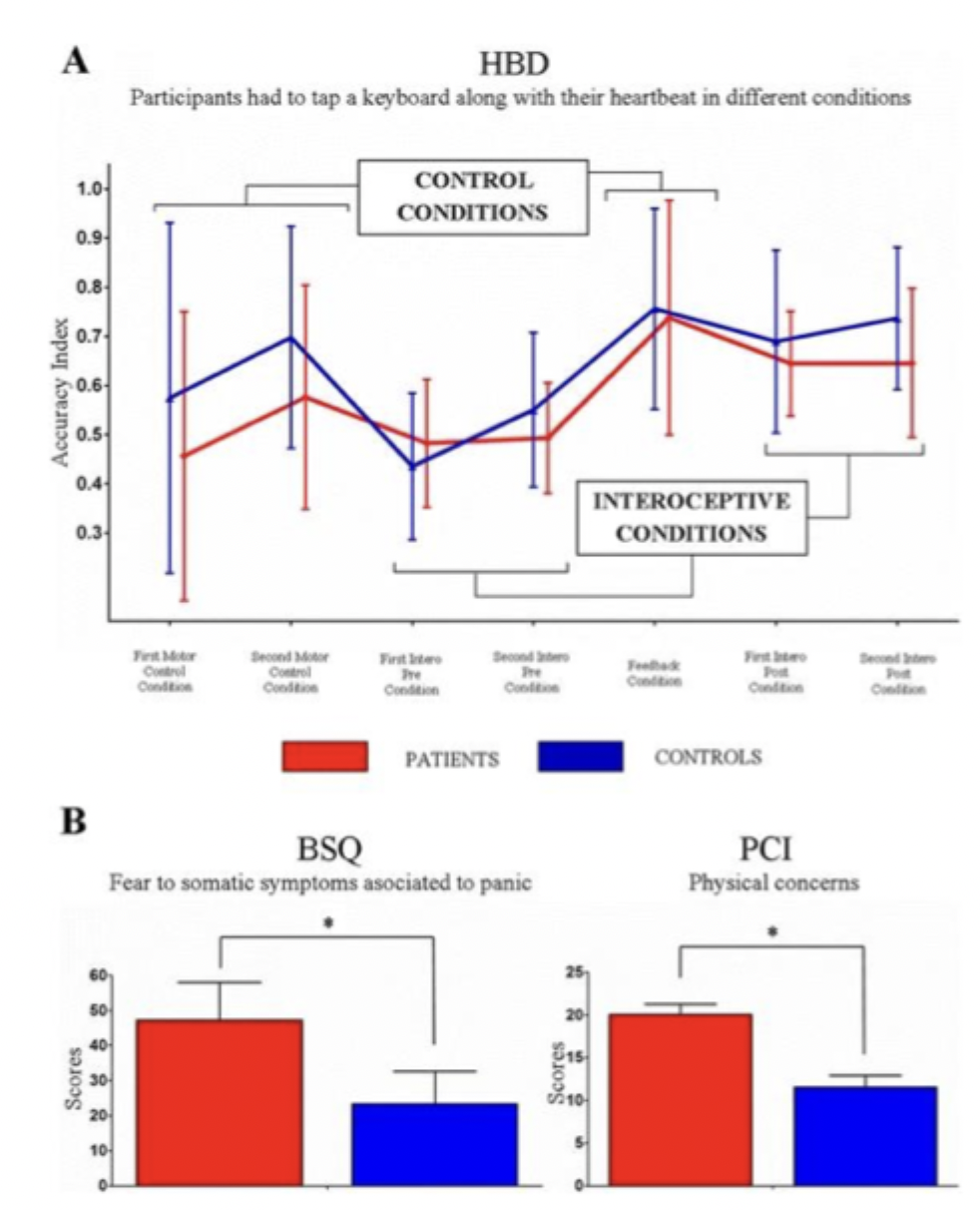
What did Yoris et al (2015) find studying using anxiety and panic attack patients using a heartbeat monitoring task and asking them questions about interoception (metacognition)?
no difference in interoceptive accuracy
but difference in metacognition (threatening beliefs about the body)
not the detection of symptoms different to controls but how they are interpreted
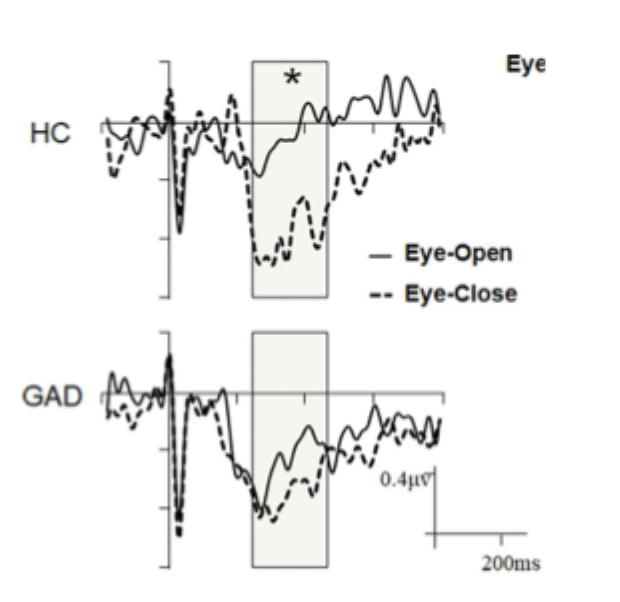
What did Pang et al find comparing patients with GAD and healthy control, examining Heartbeat-evoked potential during resting state?
eyes open (exteroception)/ eyes closed (interoception)
in healthy controls, heartbeat-evoked potentials were greater in eyes closed compared to eyes open at rest
greater focus in interoception with eyes closed
In GAD there was no difference between conditions
higher monitoring of interoception with eyes open - hypervigilance
cortical response to heartbeats greater in GAD
What are the differences in the Insular Cortex in different forms of anxiety disorders
the insula is found to have abnormalities in structure and function across different forms of anxiety disorders
abnormality in perception or interpretation of internal bodily signals
What did Etkin et al 2007 meta-analysis find of brain activation for emotional processing across different anxiety disorders?
social phobia: exaggerated fear of negative scrutiny in social interactions
specific phobia: irrational fear of something that poses little or no actual danger
PTSD: anxiety and flashbacks triggered by a traumatic event
patients with all three disorders demonstrated hyperactivity in the amygdala and insula
this pattern of activation was also noted for healthy subjects experiencing anticipatory anxiety during fear conditioning
an exaggerated fear response - might be reflected in shared neurobiology

How does Interoception relate to self concept?
an important aspect of self is corporeal awareness: the perception, knowledge and evaluation of one’s own body as well as of other bodies
being aware of our internal state modulates our approach and distancing behaviours which, in turn, help us maintain and regain homeostasis
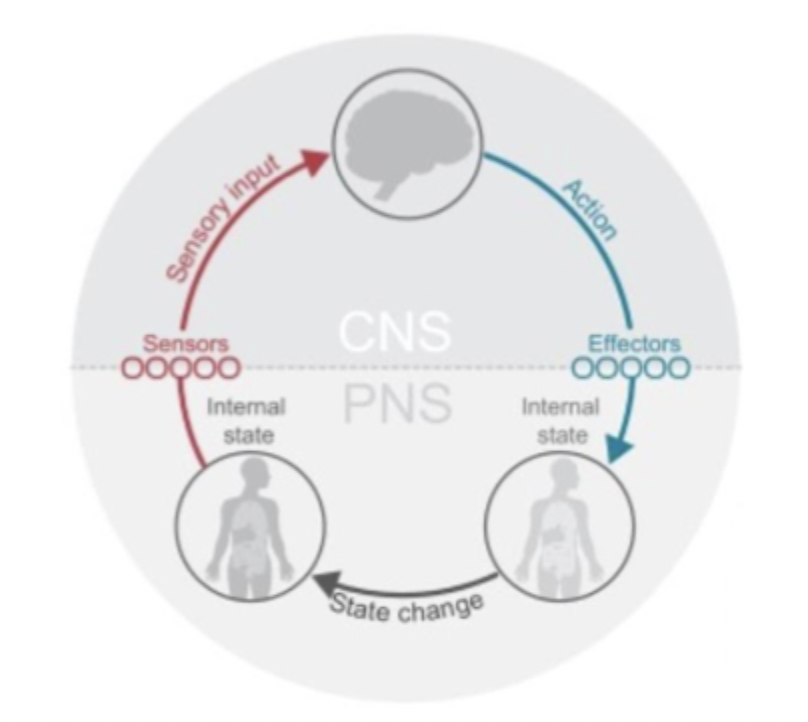
What do the recent models of interoception suggests that contrasts the idea that interoceptive experience is not passively derived from visceral sensations?
interoceptive states are dynamically constructed in the brain using information from sensory predictions and regulatory actions (afferents and efferents)
What does the insular cortex receive and how/what does it control?
receives information about blood pressure and oxygenation, the timing and strength of the heartbeat etc
top down control of autonomic functions such as regulating the heartbeat and blood pressure
How do predictive theories contrast classic theories that cortical regions either reflect stimulus intensity or additive effects of intensity and expectations?
stronger activity = stronger stimulus coming in
predictive theories suggest perception is shaped by the integration of beliefs about the world with mismatches resulting from the comparison of these beliefs against sensory input
What is predictive coding theory in general terms?
because a lot of things in the world are stable (predictable) instead of processing all information we just compare experience to predictions
predictions are faster than direct sensory information
updating predictions through errors helps learning
What is predictive coding theory in terms of interoception? and what can it lead to
links physiological states to behaviours and emotions
prediction errors with interoception can lead to maladaptive emotions and behaviours.
Predictions can be made but may be different to what happens
What is the inaugural moment in the formation of experience of body state?
the initial sensory map from the body without prior experience
How does map of body state exist throughout life?
map modified by life experience - predicted sensory experience of encountering stimuli (internal or external)
insular cortex, amygdala, anterior cingulate, ventral medial prefrontal cortex
experience of body state influenced by cognition (beliefs) often called prior
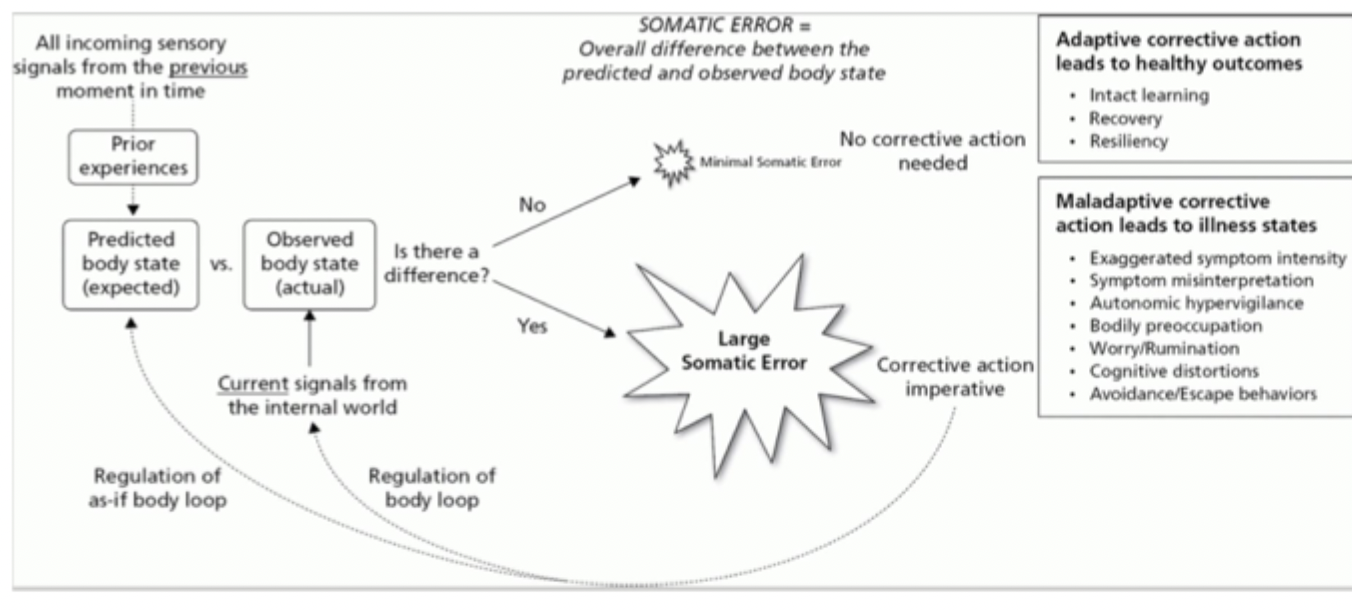
How do prediction errors occur from adaptation and experience of body state?
predicted body state continually updated from afferent information and cognition
this process results in prediction errors - small errors are ignored
large errors are detected regulated to maintain homeostasis
adapt prediction OR adapt physiological state: this aspect thought to be potentially maladaptive
What is the insular cortex anatomically situated for?
detecting errors
neural hub for combining information from visceral organs with cognition, emotion and exteroceptive sensory signals
What do the anatomical connections of the insular cortex lead to, in terms of anxiety?
anatomical connections allow integration physiological state and cognition - linked to two key components of anxiety: sympathetic hyperarousal and worry
association between physiological state, emotions and cognition requires a brain region capable of initiating and maintaining complex representation
altered prediction signal provides a process by which conditioning can occur - pivotal in the development of pathological anxiety
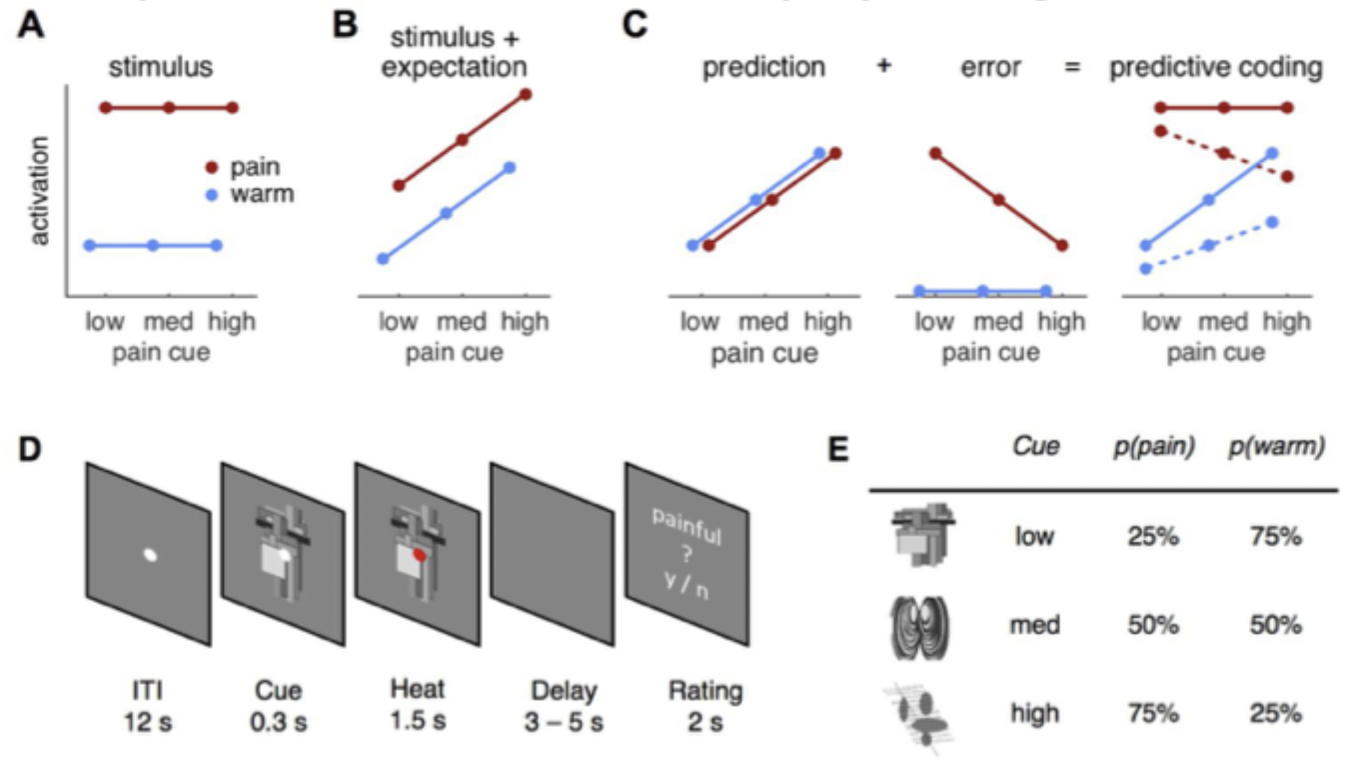
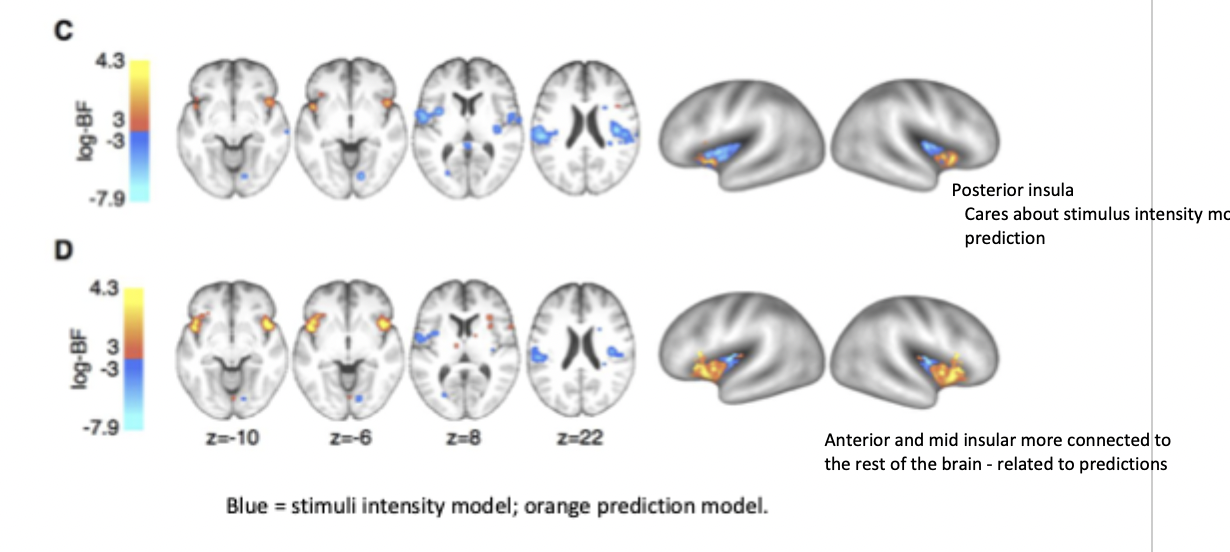
What did Geuter et al (2017) find regarding the heat pain paradigm?
tested models of stimuli and prediction - influence physiological and neural responses
the predictive coding is a weighted sum of two components
posterior insula exhibited neural patterns in line with detecting pain intensity - receives afferents from body (interoception)
anterior insula exhibited neural patterns in line with predictive coding of pain - integrates information with other modalities
these predictions are modality specific (pain) rather than a general expectation of an aversive outcome
How do psychriatric disorders relate to prediction errors?
large uncorrected prediction errors may lead to psychiatric conditions
maladaptive behaviours → e.g. avoidance, withdrawal
maladaptive cognitions → e.g. rumination, worry
What is panic disorder/ a panic attack?
regular sudden attacks of panic or fear
panic attack - a sudden onset of interoceptive signals associated with fear/panic: dizziness, dyspnea (shortness of breath), palpitations, feeling of impending doom or death
What neural structural differences are seen in panic disorder patients compared with healthy controls?
increase grey matter volume in the insula in PD compared to HC

How might misattribution explain panic disorder?
misattribution of symptoms as a heart attack despite physiologically heart is healthy
misattribution of events occurring at the same time as associated (tiggers) - avoidance behaviours
leading to anxiety over bodily signals, maladaptive behaviours and cognitions
What is the viscious circle involved in panic disorder?
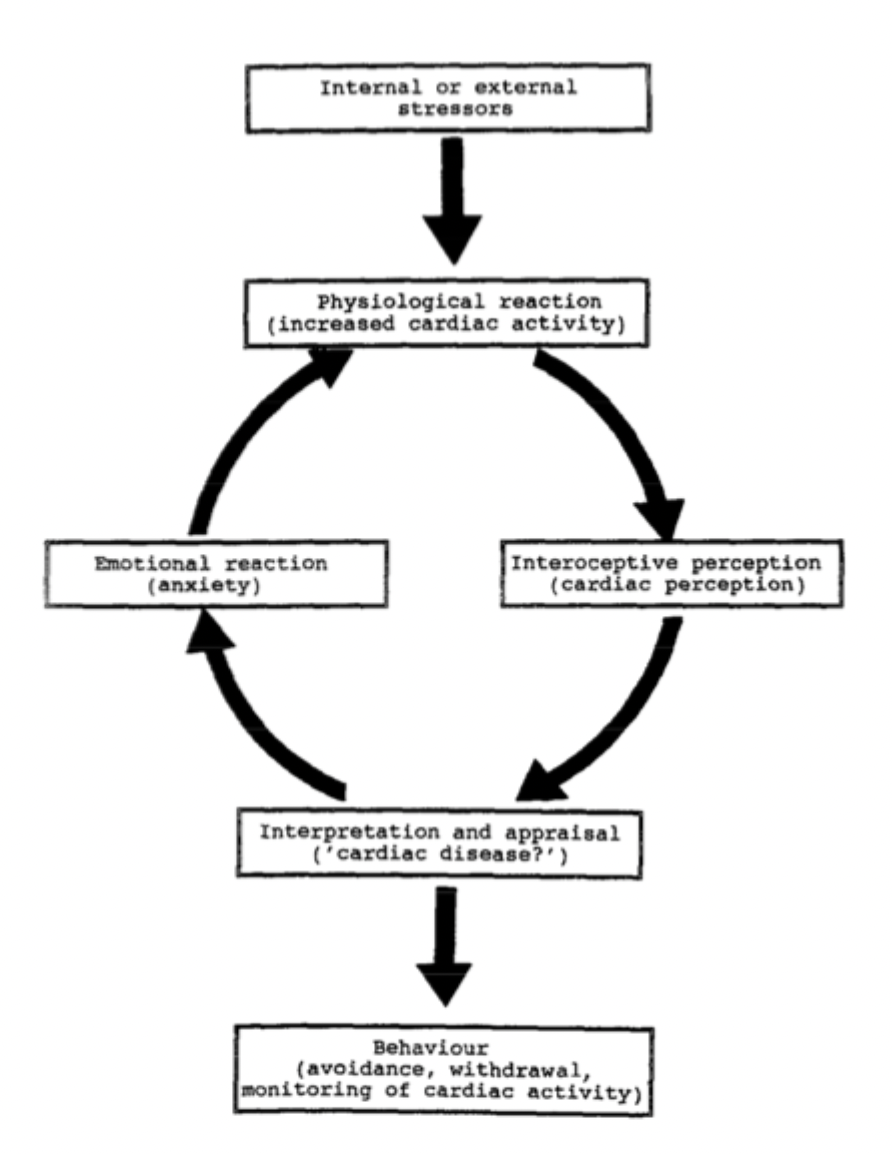
perceiving normal increases in heart rate as potentially catastrophic, experience a mismatch between actual and experienced bodily state
leading to heart rate acceleration and anxiety - body state regulated to minimise the mismatch → raising the heartbeat which further exacerbates anxiety
avoidance behaviours (e.g. withdrawal, agoraphobia)
What did Pauli et al find when patients with Panic Disorder were given 24 hours ECG monitoring (heart rate) and noted cardiac perception, anxiety and activities (not sports)?
Comparing with healthy controls
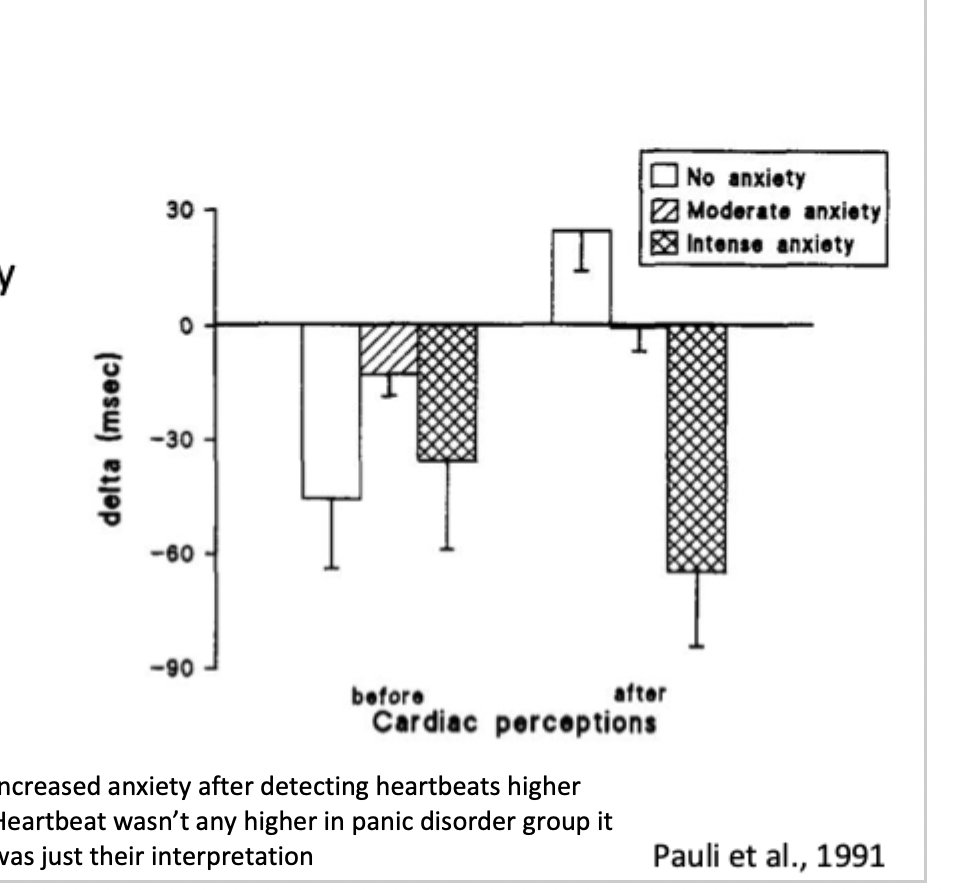
found similar variations in actual heart rate between groups
panic attack patients rated higher anxiety associated with cardiac perceptions
anxiety experienced in relation to heart perceptions related to subsequent shortening between heartbeats
increased anxiety after detecting heartbeats as higher
only difference was PDs interpretation of the heartbeats
How can cognitive states further perpetuate PD symptoms?
the self is a manifestation of past and present cognitive, affective and body state experiences
past experiences can lead to maladaptive cognitions expecting to experience certain physiological states and thus further perpetuate PD and panic attacks
How might beliefs cause the cognitive errors leading to Panic Disorder?
a change in the internal state of the individual, which may be due to an increased attentional biases toward threat
beliefs used to interpret internal body signals
external cues or internal thought generate anticipation of aversive body states that - sets up a body prediction error
How might self processing be associated with the cognitive errors leading to Panic Disorder? with association to relevant brain regions
worrying is associated with increased activity in prefrontal cortex, striatum, and insula
guilt was linked to left anterior insular cortex
sad self-relevant autobiographical memories are linked to the activation of the ventral insula
What is involved in the somatic error hypothesis?
psychiatric disorders, such as anxiety, may be a result of mismatches between anticipated and incoming bodily signals
the compensatory behaviour may come across as the psychiatric symptomology - actions to reduce the discomfort and distress (e.g. agoraphobia)
the brain over regulates the system, predictions become detached from the actual body state
prediction error causes cognitive and emotional symptomplogy → reduced trust in the body signals
What is a somatic error?
when the body state predicted by the brain differs from the afferent signals of the body state
What did Dresler et al find in their study of patients who suffered panic attacks in the fMRI scanner leading to termination of testing?
What were the results for the first patients who was removed at the beginning of discomfort?
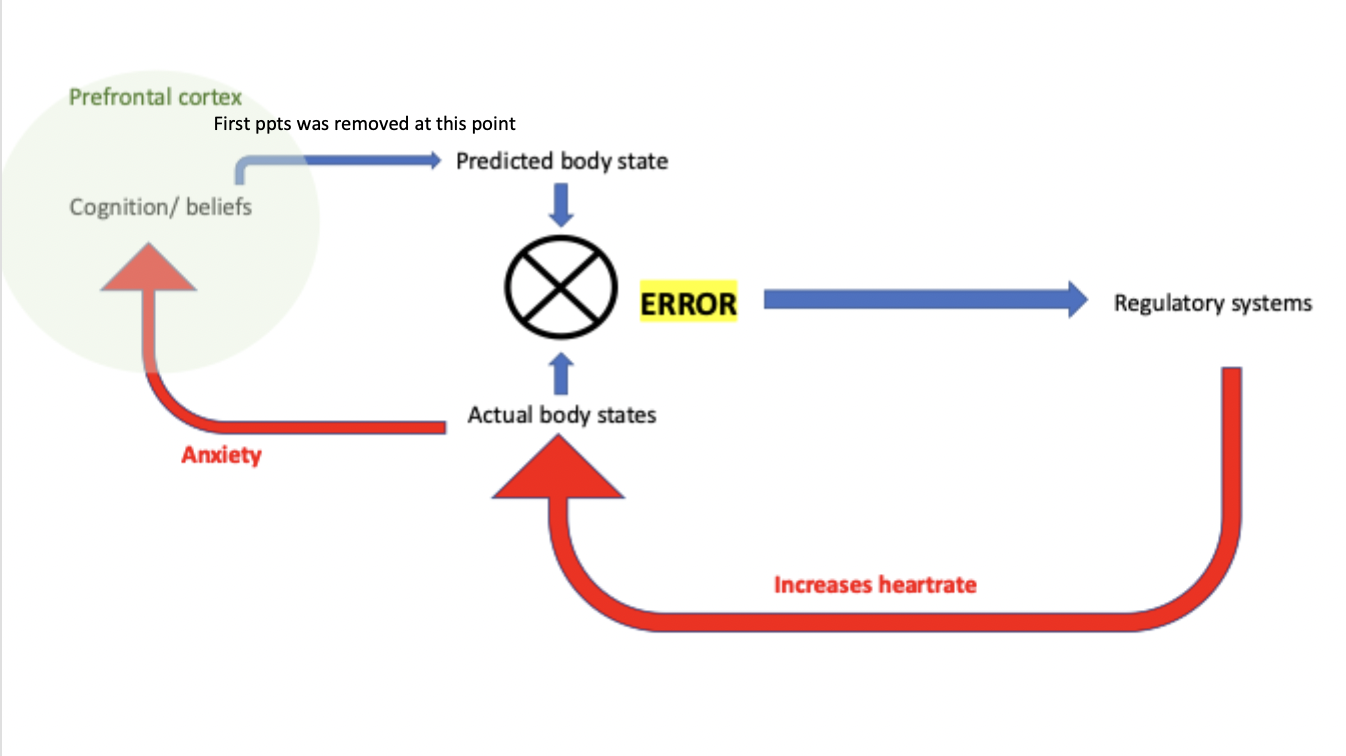
not a full panic attack: only observed a decrease in prefrontal cortex activity
decline in top-down control
suggest there is a top-down cognitive component in the onset of panic attacks
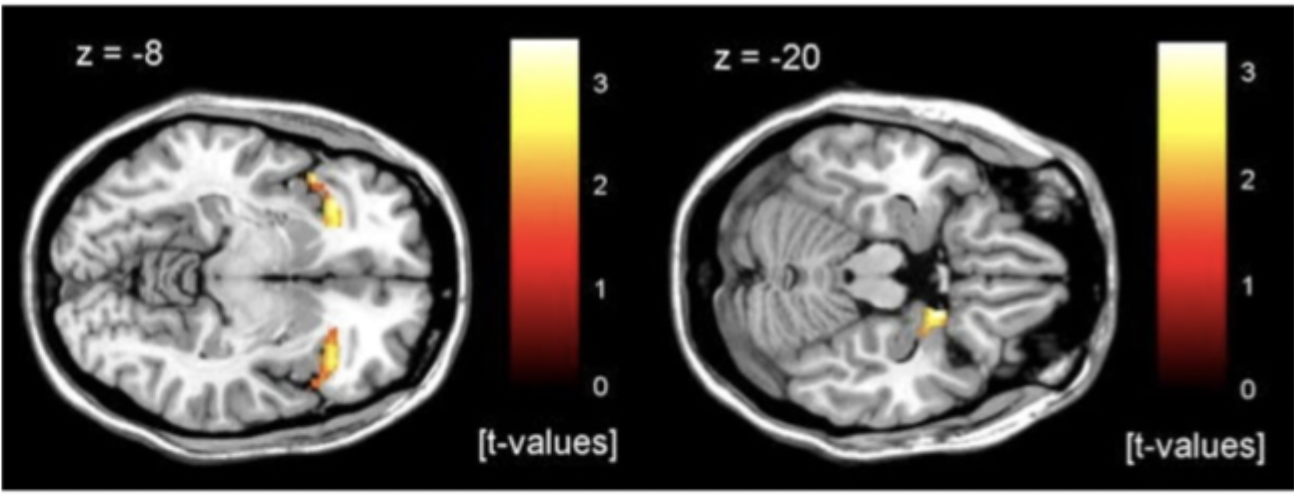
What did Dresler et al find in their study of patients who suffered panic attacks in the fMRI scanner leading to termination of testing?
what were the results for the patients who was in full panic attack before being removed
demonstrated significant insula and amygdala activity
insula activity linked to feelings of discomfort
amygdala related to feelings of panic

In Panic Disorder, maladaptive cognitions may be caused by…
initial deficits in predictive bodily state
How do the initial deficits in predictive bodily state go on to perpetuate the disorder further?
through learned associations and deficits in top-down regulation
Insula is the hub with connections to…
prefrontal cortex, limbic system (including amygdala) and sensory interoceptive afferents
Summaries