Looks like no one added any tags here yet for you.
The success of hematopoietic cell transplantation correlates with which of the following?
a. duration of immunosuppressive therapy
b. age of the recipient
c. extent of the HLA match
d. age of the donor
c
The drugs administered to transplant recipients predispose them to what types of diseases?
a. malignant
b. infectious
c. autoimmune
d. allergic
a, b
What are the antigen-presenting cells that stimulate acute rejection through the direct recognition?
a. donor B cells
b. donor dendritic cells
c. recipient dendritic cells
d. recipient macrophages
b
The principal type of harmful immune response that occurs in individuals receiving a hematopoietic cell transplant involves reactivity of what component of the immune system?
a. newly synthesized alloantibodies made by donor-derived B cells
b. preformed alloantibodies in the individual
c. mature CD4 and CD8 T cells in the transplant
d. recipient CD4 and CD8 T cells that escape myeloablative therapy
c
In addition to the cornea, which of the following is successfully transplanted in the absence of HLA matching?
a. heart
b. bone marrow
c. kidney
d. liver
d
hat is the name of the type IV hypersensitivity reaction that occurs in an individual after receiving a hematopoietic cell transplant?
a. chronic graft rejection
b. acute graft rejection
c. hyperacute graft rejection
d. graft-versus-host reaction
d
Approximately what percentage of T cells restricted by an individual’s HLA class I or class II allotype have the potential to be stimulated by a disparate allotype of the same locus in a mixed lymphocyte reaction?
a. 0.01
b. 0.5
c. 1
d. 5
d
What does it mean when a hematopoietic cell transplant has engrafted?
a. The transplanted hematopoietic stem cells have been rejected by the recipient’s immune system and killed.
b. The hematopoietic stem cells have been given to the individual intravenously.
c. The hematopoietic stem cells that were transplanted are generating new circulating blood cells.
d. The recipient’s immune system has been destroyed by myeloablative therapy.
c
Before hematopoietic stem cells are fractionated from peripheral blood with anti-CD34 antibodies, the leukocyte population must first be selectively removed from the blood by what process?
a. thrombapheresis
b. leukapheresis
c. leuko-enrichment
d. bplasmapheresis
b
Which of the following hematopoietic cell donors are likely to result in the relapse of an individual’s malignant disease?
a. autologous
b. an unrelated donor with some HLA mismatches
c. an identical twin
d. an HLA-identical, dizygotic twin
a, c
What is the name given to the cellular test for detecting MHC differences between two individuals based on cellular proliferation and killing capacity?
a. cross-match test
b. mixed lymphocyte reaction (MLR)
c. panel reactive protocol
d. HLA identification test
b
Identify the characteristics of acute rejection.
a. a type IV hypersensitivity response
b. managed by conditioning the individual with immunosuppressive drugs before transplantation
c. a response that takes several days to develop
d. primarily a B-cell-mediated response
e. associated with cell surface protein differences
a, b, c
Which of the following are suitable sources of hematopoietic stem cells?
a. autologous bone marrow
b. peripheral blood
c. allogeneic bone marrow
d. small bowel resection
e. umbilical cord blood
f. partial liver resection
a, b, c, e
How would solid tumors benefit from autologous hematopoietic cell-transplant therapies?
a. They would allow for stronger anticancer treatments.
b. They would have the same GVT reaction as liquid tumors.
c. They would allow immune cells to enter immune privileged areas.
d. They would reduce the risk of relapse.
a, b
Beside donor-derived alloreactive T cells, what other donor-derived cells directly cause a GVL effect?
a. dendritic cells
b. NK cells
c. B cells
d. macrophages
b
Why is it important for donors and recipients of hematopoietic stem-cell transplants to share some HLA allotypes?
a. The resulting dendritic-cell pool is a mix of donor and recipient cells that express HLA molecules of both the donor and the recipient.
b. Circulating T cells are educated by recipient HLA molecules but activated by donor HLA molecules.
c. Developing T cells will be negatively selected if HLA allotypes are different.
d. Radio-resistant recipient immune cells will attack the grafted cells if there is no overlap in HLA allotype.
b
What is it called when GVHD proves helpful by eliminating residual leukemia cells?
a. HLA-mismatched effect
b. host-versus-leukemia effect
c. graft-versus-leukemia effect
d. mini-transplant effect
c
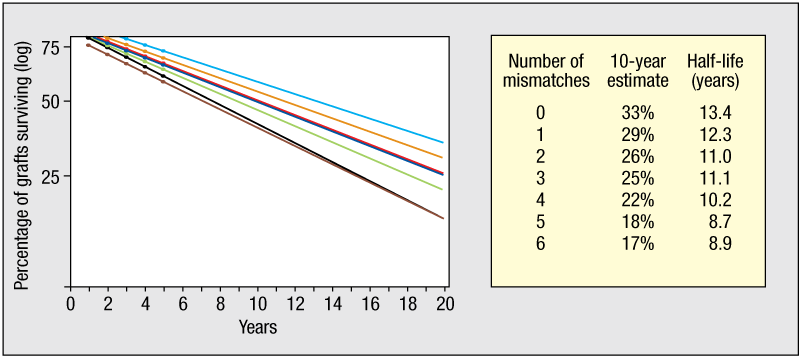
You donate a kidney to your brother. You share several HLA alleles but not all of them.
You:
HLA-A: 2, 16
HLA-B: 4, 8
HLA-C: 2, 2
HLA-DR: 4, 22
Your brother:
HLA-A: 2, 7
HLA-B: 8, 14
HLA-C: 1, 2
HLA-DR: 8, 22
\n Based on the graph and chart, what is the likelihood that the donated kidney will still be around and alive after 10 years?
22%
Identify the correct statements regarding umbilical cord blood as a source of hematopoietic cells.
a. Cord blood is not only a rich source of stem cells, but it also contains fewer alloreactive T cells than peripheral blood and bone marrow sources used for hematopoietic cell transplantation.
b. Although cord blood transplants usually involve combining stem cells from two different donors, the cells from one donor usually dominate in the reconstituted individual over time.
c. More HLA mismatches are tolerated by the individual if cord blood is used compared with bone marrow or peripheral blood stem-cell sources.
d. Cord blood engraftment occurs faster than engraftment from alternative sources of hematopoietic stem cells.
e. Individuals receiving cord blood transplants experience more acute GVHD.
a, b, c
For the GVL reaction mediated by NK cells, the recipient must have how many types of inhibitory KIR ligands compared to the donor?
a. more
b. the same number of
c. an absence of
d. fewer
d
Why are family members often better prospects for kidney donors than the general population at large?
a. Family members are more likely to donate one of their kidneys to kin than to strangers.
b. There are fewer immunogenetic differences in relatives.
c. There is a higher likelihood of blood group compatibility of ABO and RhD antigens.
d. It is easier to contact family members for a kidney donation than to find an unrelated donor.
a, b
In a nuclear family, what is the probability that a given sibling is haploidentical to another sibling?
a. 25%
b. 50%
c. 75%
d. 100%
b
How is prednisolone similar to hydrocortisone?
a. It enters the cell after binding to a cell-surface receptor.
b. It enhances innate immune responses and hastens the clearance of infectious pathogens.
c. It activates the transcription of about 50% of genes and thus exerts multifarious effects, many of which are adverse side effects.
d. It stimulates the synthesis of IκBα and induces anti-inflammatory effects.
d
The regimen carried out on bone marrow recipients prior to transplantation is called what type of therapy?
a. myeloablative
b. conditioning
c. colonization
d. reconstitution
a
Which of the following are true statements regarding acute rejection of organs?
a. Effector TH1 cells migrate to transplanted tissue and activate donor macrophages to cause further inflammation.
b. Effector CD8 T cells migrate to and destroy transplanted tissue.
c. Alloreactive T-cell responses against ‘foreign’ self-peptide: HLA complexes are weak and insignificant.
d. Only naive alloreactive T cells that differentiate into effector cells after transplantation contribute to acute rejection.
a, b
Four grades (I–IV) are used to describe the clinical severity of acute GVHD, with grade I being the least and grade IV being the most severe reaction. Which three tissues are the principal targets of type IV hypersensitivity reactions associated with acute GVHD that factor into the clinical assessment grade?
a. skin
b. gastrointestinal tract
c. liver
d. respiratory tract
e. pancreas
f. kidney
g. urogenital tract
h. spleen
a, b, c
If peripheral blood is used as a source of hematopoietic stem cells, then the donor must undergo treatment with which of the following to mobilize stem cells from the bone marrow to the blood?
a. granulocyte colony-stimulating factor (G-CSF) and granulocyte–macrophage colony-stimulating factor (GM-CSF)
b. IL-7 and IL-15
c. stem-cell factor (SCF) and macrophage colony-stimulating factor (M-CSF)
d. anti-CD34 and anti-cKit antibodies
a
What are H-Y antigens?
a. Antigens only found on stem cells from cord blood.
b. Minor histocompatibility antigens found in all autosomal chromosomes.
c. Antigens that contain histidine-tyrosine motifs.
d. Antigens are encoded on the Y chromosome.
d
Which of the following are correct statements regarding corneal allograft transplants?
a. The lack of vasculature in the cornea is an evolutionary adaptation to suppress inflammation.
b. The development of anterior chamber-associated immune deviation (ACAID) allows the eye to tolerate corneal grafts of all HLA types.
c. Even in the absence of HLA matching or immunosuppression, the success rate of corneal transplants is about 90%.
d. Resident dendritic cells cannot traffic to the secondary lymphoid organs preventing corneal donor-derived antigens from activating immune responses.
e. The cytokine TNF-α exerts suppressive immunomodulatory effects in the eyea..
a, b, c
Which of the following drugs exert their immunosuppressive effect in transplant recipients before transplantation by depleting alloreactive T cells?
a. rabbit anti-thymocyte globulin (rATG)
b. alemtuzumab
c. prednisone
d. cyclosporin
a, b
Which of the following are the most important HLA class I and class II allotypes to match for kidney transplantation?
a. HLA-DR
b. HLA-A
c. HLA-B
d. HLA-C
e. HLA-DQ
f. HLA-DM
a, b, c, d
Transplantation
is the act of transferring cells, tissues, or organs from one site to another
First successful transplantation
entire leg by the 3rd century physicians Cosmos and Damien
History of Transplantation
• During WWII - treatment of burned airmen
• 1954: Joseph Murray performed first successful kidney transplant from living donor (Nobel prize)
• 1960s introduction of immunosuppressive drugs
• 1967: Dr Christian Barnard carried out the 1st human heart transplant
• Improved immunosuppression
• Increased numbers of tissues and organs being transplanted
• Databanks and transplant registry
• Ability to diagnose rejection episodes
• Future? Xenogeneic transplantation
Four properties of blood that makes it good for transplantation
blood can be donated by healthy individuals at regular intervals without compromising their health.
blood transfusion is a simple, inexpensive procedure, involving only the intravenous infusion of a liquid graft.
as blood transfusions are mostly used to compensate for traumatic loss of blood, transfused blood components need only function for a limited time, until a patient’s bone marrow is capable of maintaining homeostasis. This demand is less stringent than that placed on transplanted organs, such as hearts and kidneys, which need to function for a lifetime.
that erythrocytes, the therapeutic cells in a blood transfusion, do not express any HLA class I or class II, the major barriers to transplanting tissues, organs, and other blood cells. Conversely, the leukocytes, which do express HLA antigens, are removed from blood before it is used to transfuse a patient.
First successful kidney transplant from living donor
1954: Joseph Murray
introduction of immunosuppressive drugs
1960s
1st human heart transplant
1967: Dr Christian Barnard
ABO incompatibility
extensive erythrocyte lysis (hemolysis) and leads to fever, chills, shock, renal failure, and even death
Autograft
Tissue is derived from ‘self’, can be transplanted back to the same place or another site
Isograft
tissue transplanted between genetically identical twins
1954 Joseph Murray
bypassed the barrier of rejection by using the patient’s identical twin as the donor of a human kidney transplant
Allograft
Tissue transferred from one individual to another (genetically non-identical, same species)
Allograft examples
✓ Kidney, Heart, Pancreas, Lung, Liver, Bowel (‘solid organ’)
✓ Islet
✓ Bone
✓ Cornea
✓ Skin
✓ Tendon
✓ Cartilage
✓ Stem cell
Xenograft
Tissue transferred from one species to another (eg. Heart valves)
What limits xenografting?
hyperacute rejection
Immunological Privileged Sites
Sites where grafts are not rejected
What is the major barrier to overcome in transplantation?
HLA
Why do heart valves not reject?
biocompatible: tend to be collagen, highly vascularised tissues are more likely to reject
Why is the eye an immunologically privileged site?
Cornea not highly vascularised
Why do corneal transplants require no HLA assessment or immunosuppression?
naturally immunosuppressive environment in anterior chamber of eye and lack of blood vessels in the cornea
HLA
Human Leucocyte Antigen
How many HLA loci are there?
6
HLA class I
A, B, C
HLA Class II
DR, DQ, DP
Purpose of HLA
allow tissue to be recognised as ‘self’ or ‘non-self’ by the host immune system and therefore determine histocompatibility
Function of HLA
serve as recognition molecules in the initiation of an immune response so they are VERY polymorphic
What do HLA antigens present to effector cells of the immune system (mainly T-cells)?
peptides from foreign substances
Why is HLA so polymorphic?
to give individual responses to pathogens
HLA Class I expressed
on nearly all cells
HLA Class II
are only found on immune cells
What do HLA Class I recognise?
pathogens that reside inside the cells (e.g viruses)
What do HLA Class II recognise?
pathogens that reside outside the cell (e.g bacteria)
HLA-A
Defines locus (OUT OF 6)
HLA-A24
Shows the serologically defined antigen
HLA-A*24
asterik denotes that the allele has been defined by molecular methods (low resolution)*
*HLA
Has been determined via molecular methods
Solid organ HLA
Define locus
Serological antigen
Molecular method
HSCT HLA
Define locus
Serological antigen
Molecular methods
need further molecular methods to determine what type of antigen
HLA-A*24**:01**
shows higher resolution, specific allele (required for HSCT)
HLA matching would have…
2 copies of each loci from each parent (A01 and A**33)
HLA A
28 antigens
HLA B
60 antigens
HLA C
10 antigens
HLA DR
21 antigens
HLA DQ
9 antigens
HLA DP
6 antigens
HLA-B alleles worldwide
changes due to variation and migration
HLA*24
10.5% - ENGLAND
26.2% COLUMBIA
HLA B46
1% Vancouver
0% Brazil
29% Thailand
HLA inheritance
Never genetic match to parent, has both HLA but 25% chance to a sibling
Which transplantation due we allow some degree of mismatch?
Solid organ
HLA Typing: Serology
‘Terasaki trays’ used – plates with serum containing anti-HLA antibodies, patient cells and complement added, death occurs in wells where antibody reacts with patient sample (death = positive)
HLA Typing: Molecular methods require the extraction of high quality genomic DNA
• Sequence specific primer (SSP) PCR is often the first step in determining HLA type
• SSP tests consist of multiple different PCR primers specific for known HLA polymorphisms and are supplied in a kit format
• Specific amplicons are produced if the primers are complementary to the sample DNA
SSP results
One band in every well, shows it is working
Double band = HLA type
HLA-B27 (around 8%)
increased risk for ankylosing spondylitis and other inflammatory disorders
95% of AS sufferers are B27 positive
HLA-B57
associated with drug-induced inflammatory disorder
All HIV positive patients in the UK are screened for HLA-B57 prior to beginning Abacavir (reverse transcriptase inhibitor) treatment
Major risk of hyperacute rejection
Anti-HLA antibodies
Anti-HLA antibodies arise
pregnancy, blood transfusion or previous transplantation
CDC crossmatch assays
Complement Dependent Cytotoxicity
used successfully for several years, recipient sera is incubated with donor lymphocytes in presence of complement
Living donors
• Family members/friends can opt donate kidneys or a part of their liver (subject to ABO/HLA compatibility).
• Altruistic donation also sometimes occurs
• Paired/pooled donations are an option when relatives do not match
Cadaveric donors
• Those which are deemed to be ‘brain stem dead’ following appropriate testing
• Donation after ciculatory death (DCD) or non-heartbeating donors, usually occurs after admittance to A&E
Reasons for kidney failure
Genetic diseases
Autoimmune diseases
Diabetes
High blood pressure
Reasons for heart transplants
Ischaemic heart disease due to lifestyle
Idiopathic cardiomyopathy
Myocarditis
Congenital
Peripartum
Pre-transplant crossmatch
• For all transplants, a crossmatch is always performed immediately prior to surgery
• Recipients are screened prior to entry on the waiting list, but their antibody status may have changed (hyperacute risk)
• For heart and lung, logistics may prevent the pretransplant crossmatch, so a virtual crossmatch is performed instead
Issues around consent
• Recent opinion poll study data suggests that 90% of the UK population support organ donation
• In practice, only 68% provide consent in the event of a family member being declared brain dead
• The disparity is likely due to the effects of shock and grief in the situation
• We now have an ‘opt out’ system following Max and Keira’s law
• Even with ‘deemed consent, medics allow family input
For kidney and pancreas, allocation is based on
blood group match and HLA-A, B and DR, 000 mismatch are given priority
Transplantation allocation
Paediatric patients are always prioritised, then sensitization, waiting time, age match and location are also considered
• These factors should prevent a patient waiting for many years, avoid older organs being given to young patients and also reduce cold ischaemic time
For heart and lung allocation
ABO match and HLA-DR
The size of the heart relative to the donor is also important
What HLA is never mismatched?
HLA-DR