Neuroradiology
Covers head and axial skeleton
Based off of symmetry
General anesthesia is a must
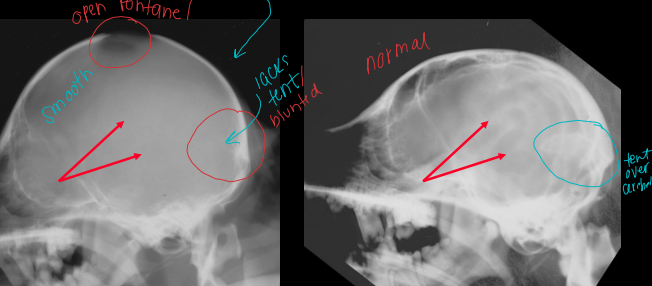
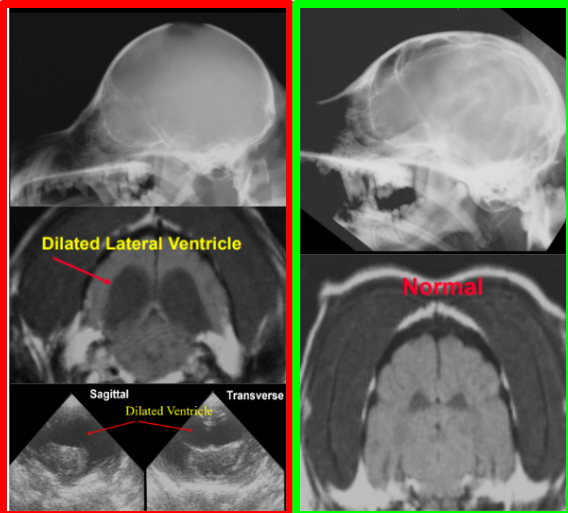
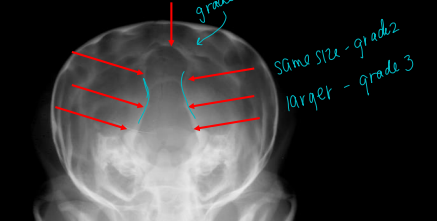
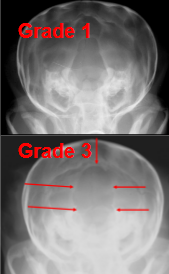
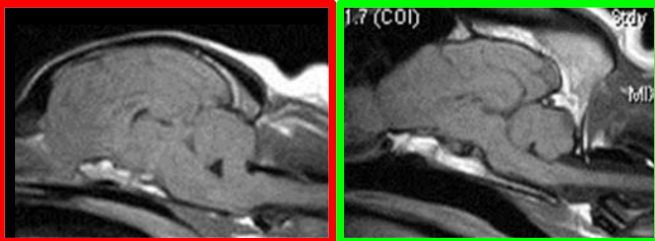
Hydrocephalus
Cause:
Overproduction or obstruction to outflow of CSF: choroid plexus
high production, low absorption
Congenital or acquired
Dome head toy breeds
CS:
dull mentation, seizures, incoordination
Views:
Closed mouth VD and lateral
5% will show x-ray signs
RS:
Open fontanel and suture, caudal osseous tentorium, ground glass look, thin cortex, dilated lateral ventricles
Adults, may look normal
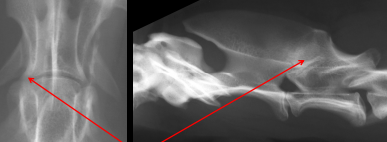
Occipital Dysplasia
Cause:
Congenital defect of foramen magnum
young Dome head toy breeds
CS:
cervical pain, hind limb neurologic deficits
Views:
Lateral, closed mouth VD, slight obliqued VD
Needs MRI/CT scans
RS:
Abnormal foramen magnum with open dorsal extension
“keyhole” shape
herniation possible
Chiari Syndrome
Cause:
King Charles Cavalier Spaniels
CS:
neck pain, mentally dull, ear scratching
RS:
Caudal crowding of the cerebellum with herniation via foramen magnum
Normal X-rays
Cranial Mandibular Osteopathy
Cause:
Unknown but self limiting
Young westies
4-11 months
CS:
Pain, cant open mouth, muscle atrophy, Soft tissue swelling
Views:
Closed mouth VD and lateral view
RS:
Osteoproductive lesion of mandible/TMJ/bulla, NO lysis
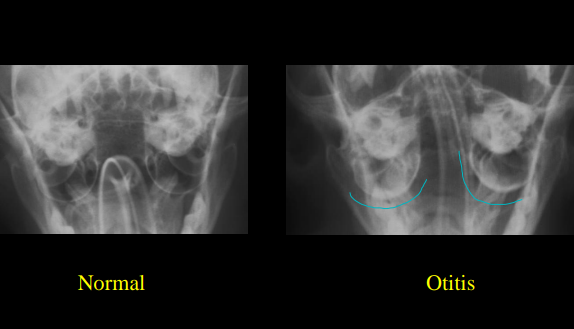
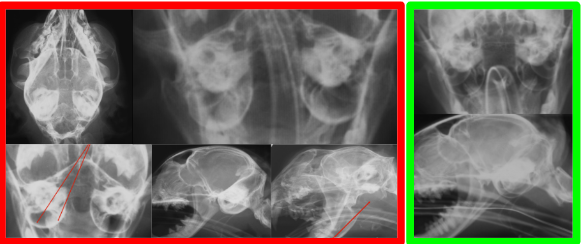
Otitis Media
Cause:
Bacteria mid ear infection
secondary to chronic otitis external
Floppy eared old dogs
CS:
Head tilt, ear pawing, exudate, seizures
Views:
Closed mouth VD, open mouth VD, obliques
CT / MRI is preferred
RS:
Thick osseous bulla with lysis, increased soft tissue density in bulla, mineralization of external ear canals, increased opacity of tympanic bullae, nasopharyngeal polyp
Normal contents of the ear
tympanic bullae
air
external ear
air
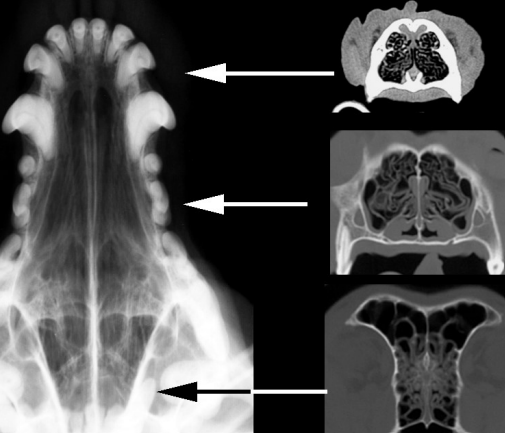
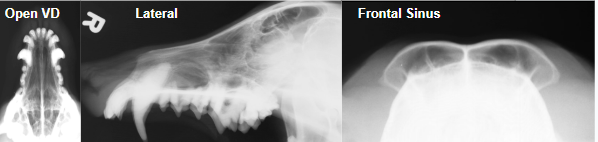
X ray positioning of the head
Done sedated
Open mouth VD
#1 for nasal passages
Closed mouth obstructs passages
Lateral View
Frontal Sinus View
X-rays are insensitive for nasal dx
CT preferred
Destructive rhinitis
Cause:
Neoplastic
Old, Lg dolichocephalic dogs (long)
Adenocarcinoma
Fungal rhinitis
Lg dogs
Aspergillus + blastomycosis
CS:
Mucopurulent to bloody discharge
Neoplastic: Uni to bilateral discharge, facial deformity’s, external masses
Fungal: Uni discharge, facial/external deformities are RARE
Views:
Open mouth VD, lateral, skyline frontal sinus
X-rays insensitive for nasal dx
CT prefered
RS:
Increased nasal passage opacity, turbinate destruction, bone lysis
Non-destructive rhinitis
Cause:
Older animals
Bacti, fungal, viral, FB, allergys, parasites, Kartagener’s
CS:
Serous to mucopurulent discharge
Views:
Open mouth VD, lateral, skyline frontal sinus
X-rays insensitive for nasal dx
CT prefered
RS:
Increased nasal passage opacity, nasal turbinates blurring, NO lysis or septal deviation
Temperomandibular Joint TMJ
Cause:
Congenital or acquired
CS:
luxation, instability of the jaw, weight loss, pain, cant open mouth
Views:
Closed mouth VD, obliques
RS:
irregular articular surfaces, joint incongruity, luxation, DJD
Spinal anatomy
Rib heads
articulate in front of their assigned #
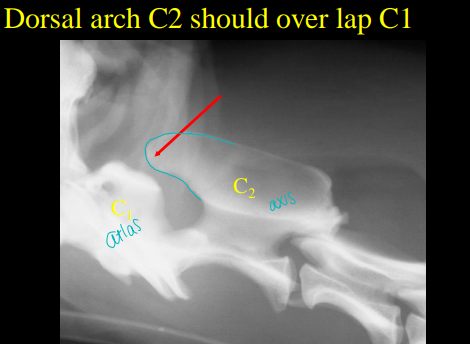
7 cervical vertebrae
C2 dorsal arch over lap C1
C 2-3 narrow disc space
C6 Lg lamina ventral to transverse process
sled runners
C7 dorsal spinous process in Lg
13 thoracic vertebrae
C7-T1 narrow disc space
T10-11 narrow disc space , bulb articular process
T11 anticlinal vertebrae, straight dorsal spinous process
Dorsal spinous process point caudally
Disc herniation are rare cranial from T1-T10
7 lumbar vertebrae
L3 and L4 attach diaphragm
Transverse processes increased opacity
Dorsal spinous process point crainally
3 sacral vertebrae
20-23 coccygeal vertebrae
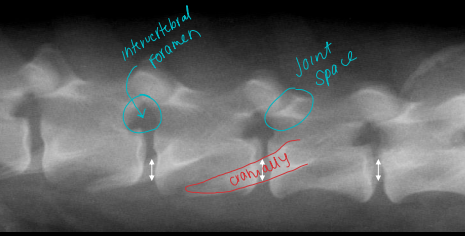
Accessory process
increased disc opacity
overlay the intervertebral foramen and insults in increased opacity within the neurocanal
often not present
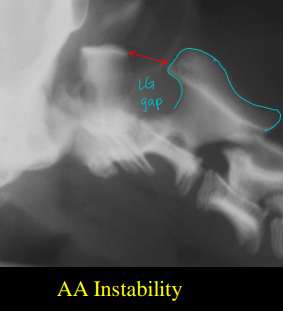
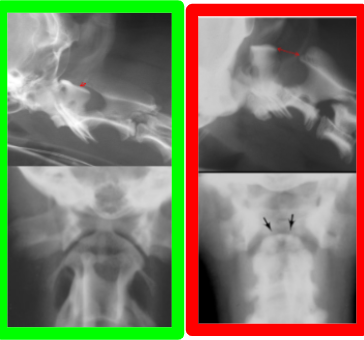
Atlantoaxial Instability
Cause
Congenital (95%)
malformation of dens C2
lig. malformation
Mini dogs
trauma to dens
CS
Ataxia, paralysis, proprioception issues, cervical neck pain, shows up under 1yr old
Views
Straight lateral C-spine, lateral dens view, slightly flexed lateral, VD
RS
C1- C2 large joint space, Sm/missing dens, dens fracture
DDx.
disk herniation, neoplasia, trauma, central CNS dx
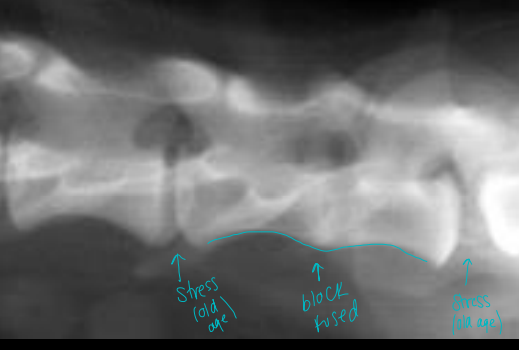
Block vertebrae
@ any location
Cause
Congenital
Boxers, Bulldogs, Bostons, Shar Pei, Chondrodystrophoids, Manx
failure of proper segmentation
CS
stable, incidental, can cause surrounding aging issues
RS
vertebrae fusion, lack of disc
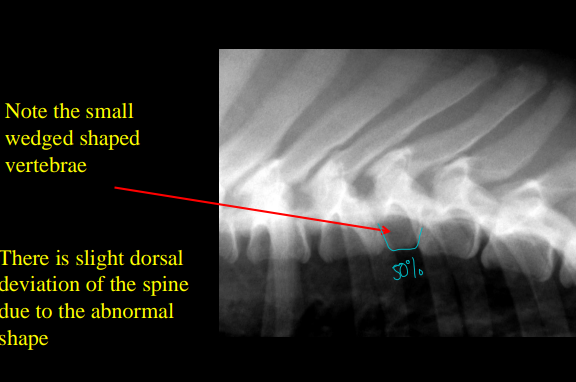
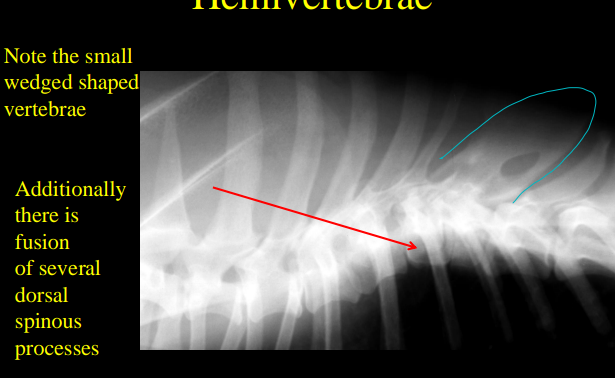
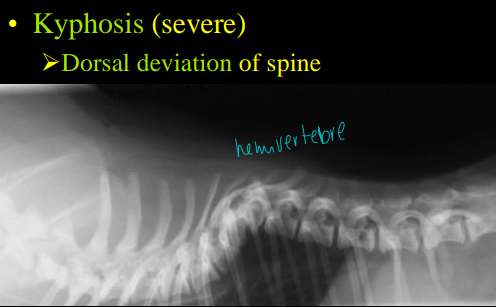
Hemivertebrae
Cause
Congenital
Bostons, bulldogs, pugs
CS
incidental, stable
RS
Abnormally shaped or short vertebra, odd curvature of spine
50% less then other vertebra
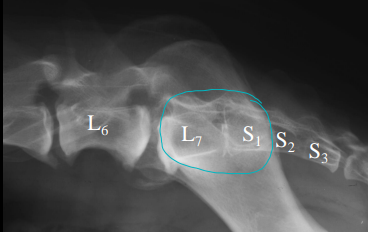
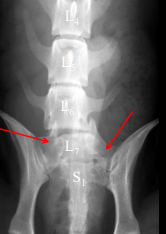
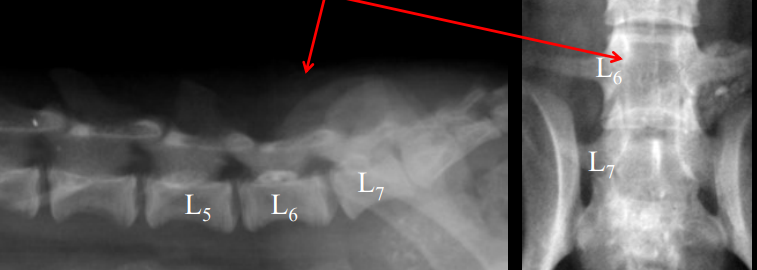
Transitional Vertebrae
Cause
Congenital
Boxers, Bulldogs, Bostons, Shar Pei, Chondrodystrophoids, Manx
anomalous formation of TL and LS junctions
CS
incidental
RS
Sacralization of L7 via illiac fusion
Lumbarization of S1 via transverse process/disc development
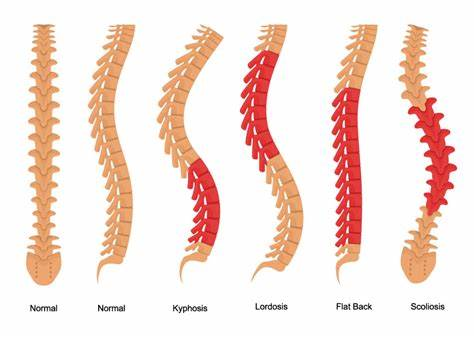
Terms used to describe vertebral curvature
Lordosis
Ventral deviation of spine
looking at the lord
Kyphosis
Dorsal deviation of spine
Scoliosis
Lateral deviation of spine
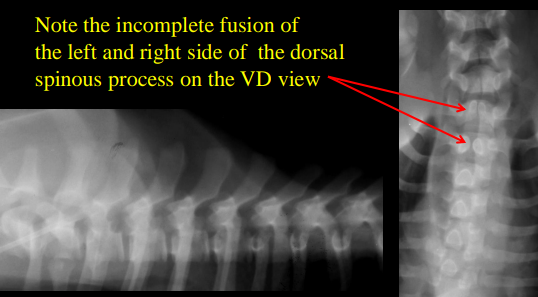
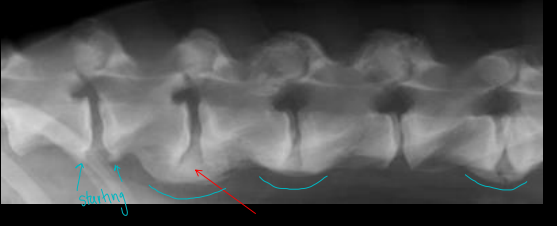
Spina Bifida
Cause
Congenital malformation and failure of fusion of dorsal arches
Bostons, bulldogs, Pug, Manx
screw tails
failure of fusion of dorsal lamina on dorsal arches and spinous processes
CS
Young: clinical
Old: non-clinical
Views
Lateral and VD
RS
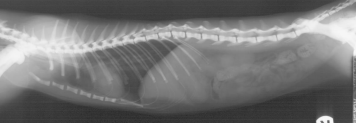
2 paired dorsal spinous processes, missing/blunted L7 dorsal spinous, distended colon or bladder
SB occulta= bony defect
SB manifesta= meninges and spinal cord herniated through bony defect
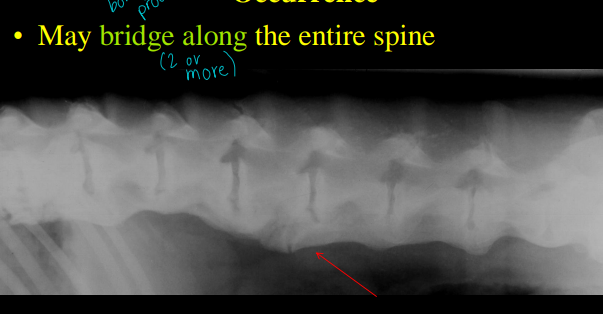
Spondylosis Deformans
Cause
Joint instability, idiopathic
Degenerative
Animals over 1yr
Bone exostosis projecting from the
vertebral endplates
CS:
No CS, incidental
Views
Lateral and VD
RS
Smoothly marginated, bony bridging
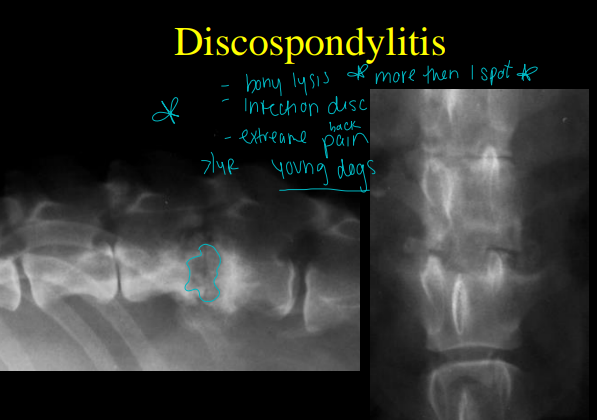
Discospondylitis
Thoracic and lumbar spine are the most common sites
Cause
Bacti infection of discs and end plates
staph, strep, e coli, brucella
Hematogenous infections
can be secondary
septic emboli
GSD, Danes, Males
CS
Young, focal back pain, reluctance to move or ambulate, neuro deficits to limbs, bony lysis
Views
Lateral and VD of entire spine
RS
Osteolytic focal lesion, wide/narrow intervertebral disc space
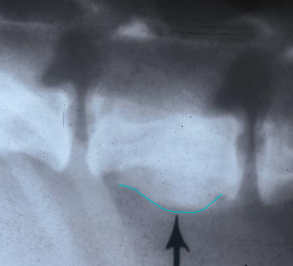
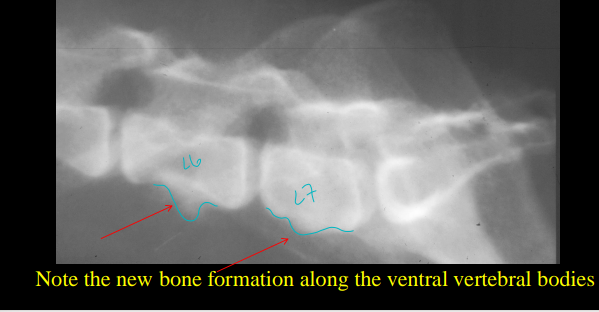
Spondylitis
Cause
Bacti infection of ventral vertebral body
staph, strep, e coli, brucella
Hematogenous infections
can be secondary
septic emboli
CS:
Middle age to older dogs and cats, <2 years most commonly, back pain, reluctance to move or ambulate, neuro deficits to limbs, fever
Views
Lateral and VD
RS
Loss of vertebral body concave margin, bony productive lesion on ventral vertebral body, rough
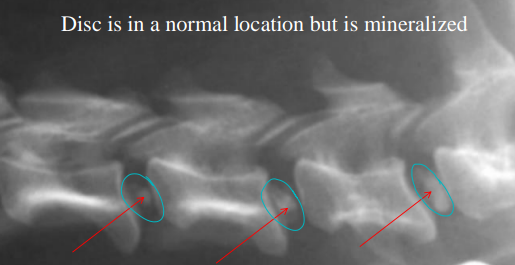
Intervertebral Disc Disease
Cause
disc protrusion or extrusion of nucleus pulposis
Type 1
calcification in situ, acute herniation
chondrodystrophoid dogs
Type 2
Incomplete with slower onset
Rare @ T1-T9 due to intercapital ligament
CS
Older, pain, paralysis
Views
Lateral and VD: cant diagnose
MRI
RS
Narrow disc space, increased intervertebral opacity, mineralized disc
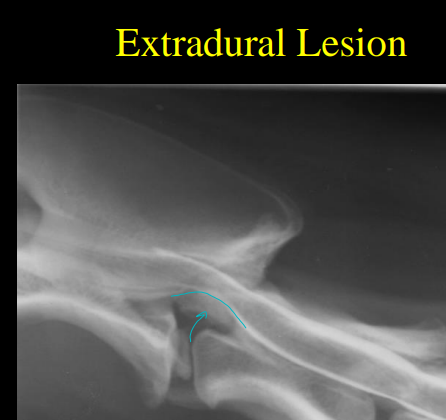
Myelogram
iodinated contrast: agent injected around spinal cord space surrounding (subarachnoid space)
specific nonionic, low osmolar agent
Iohexol or omnipaque
ID areas of cord compression or deviation
Extradural
Lesion outside dura mater
Intradural-extramedullary
Lesion in subarachnoid space
Intramedullary
Lesion in spinal cord
Complications
invasive
seizures, vomiting, bradycardia, exacerbation of neuro issues, death
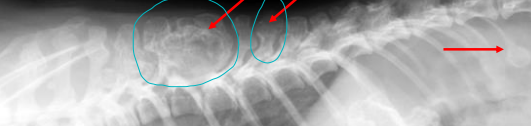
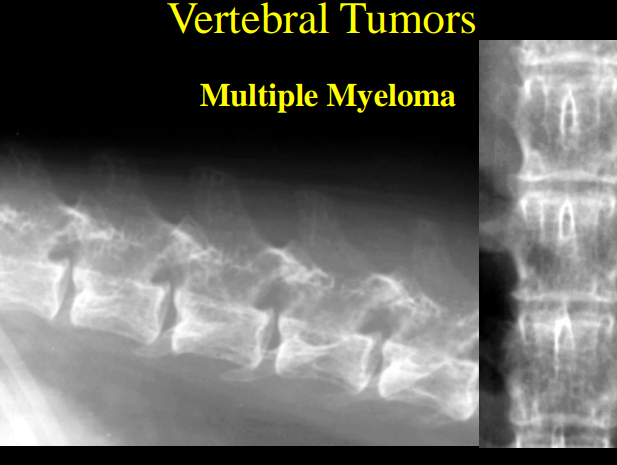
Vertebral Tumors
Primary tumors: stops growing when pet stops growing
usually located in only one vertebral body
Except Osteochondroma or multiple cartilaginous exostoses
Multiple vertebrae and/or ribs
Most are lytic
Osteosarcoma is most common
Metastatic Tumors
multiple vertebral bodies
tumors through body
lytic or periosteal
RS
osteolytic or osteoblastic lesions, compression
MM: multiple areas of moth-eaten diffuse lysis
MCE: bony mass displacing and compressing the Spinal cord
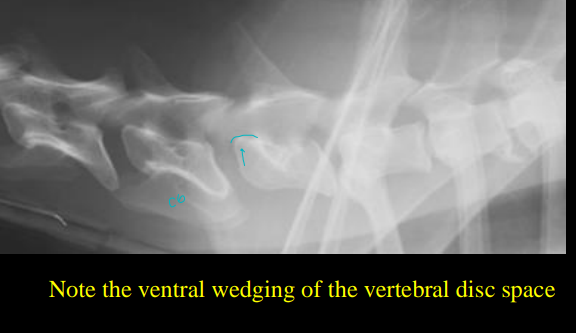
Cervical Vertebral Instability (Wobbler’s Disease)
Cause
Inheritable
Great Danes, Dobermans
cervical disc spaces are unstable, spinal cord interference, dorsally displaced vertebral body, hypertrophy of dorsal longitudinal lig. disc protrusion/extrusion
CS
Old, male, ataxia, cervical pain, hemi to tetraparesis, wide based stance
Views
Straight lateral and VD
myelography and dynamic views
80% can be ID with x-rays (controversial)
RS
Narrowed/wedge disc space, dorsal deviation of vertebral body, spinal mal alignment of C5-6, C6-7, C4-5, cord compression that worsens during neck extension
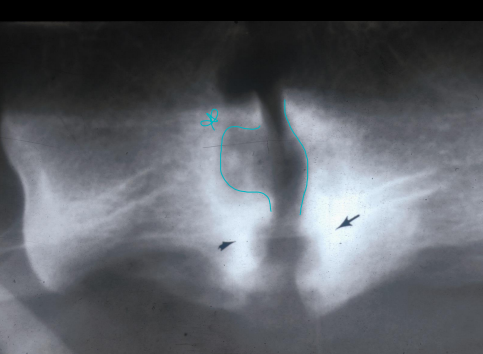
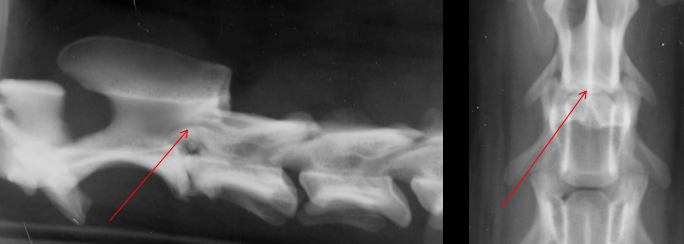
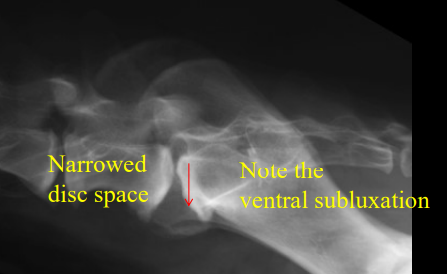
Lumbosacral Instability
Cauda Equina Syndrome
Cause
Instability of L7-S1, disc protrusion or extrusion, hypertrophy of dorsal longitudinal lig.
Transitional vertebrae may predispose
GSD
CS
older, rear limb ataxia, worn dorsal nails, pain during full extension of pelvis, reluctance to position to defecate
Fecal and urinary incontinence
Views
Lateral and VD
Need MRI
RS
Narrowed/wedge, Spondylosis, ventral step lesion at L7-S1
Full colon
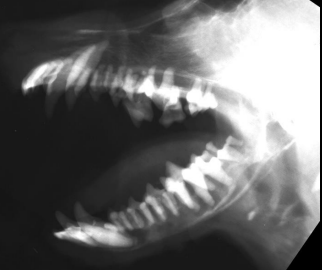
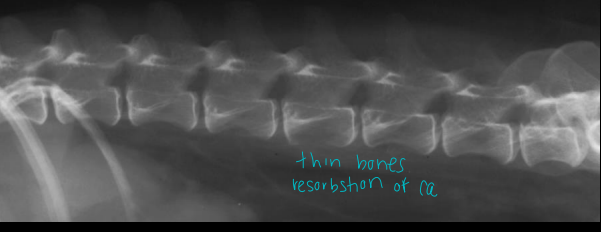
Hyperparathyroidism
Cause
hyperfunctional parathyroid gland
hypercalcemia caused by the elevated PTH.
Primary Hyperparathyroidism from adenoma of the parathyoid gland
Secondary Hyperparathyroidism from diet or chronic renal failure
RS
Skull demineralization, generalized osteopenia with cortical thinning, prominent endplates, prominent teeth opacity
Radiology and skeletal healing
Normally must have 30-50% bone loss prior to seeing it
Lytic changes will not be seen for 7-10 days
Productive changes may not be seen for 14 days
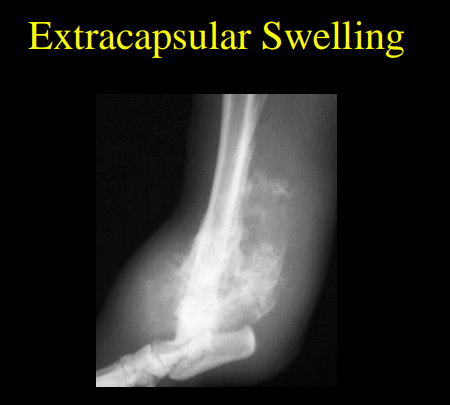
Soft tissue radiology
Extracapsular tissue swelling
Blood, pus, edema outside joint
Not centered around a joint
Intracapsular tissue effusion
Blood, pus, edema within a joint
Centered around a joint space
Soft Tissue Emphysema
Gas inside body
Outside: petrating injury or sx
Bacti sorce: emphysematous bacteria like Clostridia
From body: pneumoarthrogram (cracks)
Soft Tissue Mineralization
Dystrophic
Focal
Dead, dying tissue
Metaplasia to mineral
Normal Ca:P
Metastatic
Diffuse
Abnormal Ca:P
Periosteal Reactions
Healing process in response to injury with Sharpey’s fibers
Solid / Homogeneous
Periosteum is lifted and new bone has filled space beneath it
well defined
Lamellated
alternating opacities
cyclic ongoing processes
Active, aggressive lesions
Osteomyelitis, fungal disease, neoplasia
Spiculated
spicules at right angles with the bone
pus, neoplastic cells between spicules
Form along Sharpey’s fibers
aggressive process
infection, neoplasia, fungal
Amorphous “wispy”
Looks like anything
Aggressive process
neoplasia
Codman’s Triangle
Lifting of periosteum by radiolucent cells at lesion edge
aggressive processes
osteomyelitis, neoplasia
Osteoporosis
Cause
overall decrease bone mass
normal composition just not enough
Old, Cushing’s, hyperparathyroidism, Addison’s, steroids, low calcium
RS
Cortical thinning, bone lucency, prominent trabeculation, “egg shell” vertebral bodies
Osteomalacia
Cause
abnormal matrix, normal mass
“Soft bone”
CKD, low vit D or Ca
Hypophosphatemia
RS
decreased bone opacity, cortical thinning, angular limb deformities
Osteopenia
Generalized term to describe focal or generalized decrease in bone density
Osteosclerosis
Cause
increase in bone mass
hormonal imbalance (female birds), metabolic, neoplasia, incidental (cats)
RS
thick cortical thickening, increased marrow opacity
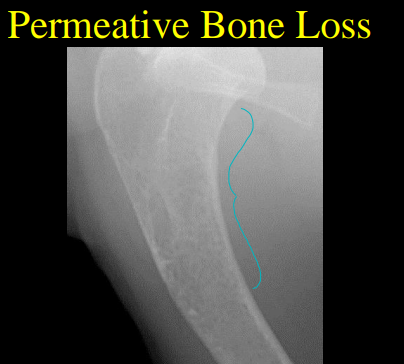
Focal or Regional Bone Loss
Disuse osteoporosis
50% loss before seen
10d “no use”
Geographic bone loss
Focal lytic lesion in bone
Center is necrotic/pus
May be expansile
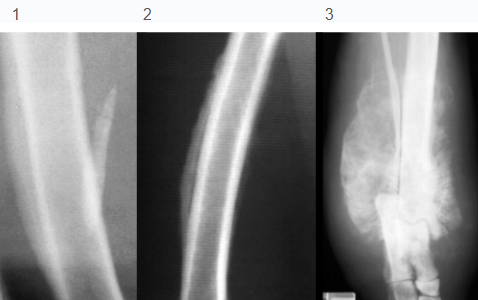
Punctate (permeative) lysis
Multi, sm lysis regions
can coalesce
Indistinct margins
Aggressive process
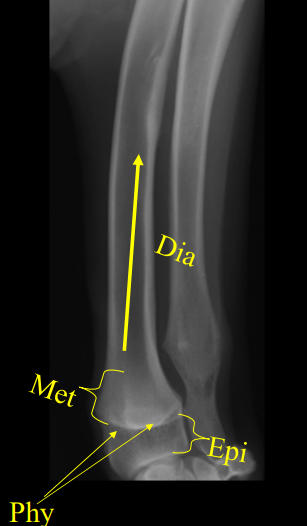
Bone Parts
Epiphysis
end of bone, articular part
Physis
growth plate or line
Distal radial plate
80% of growth, closes 9 mths
Distal ulna plate
85% of growth, closes 10 mths
Metaphysis
widened part between shaft and growth plate
Diaphysis
shaft of long bone
Growth Plate Injuries
Cause
skeletally immature < 10 months
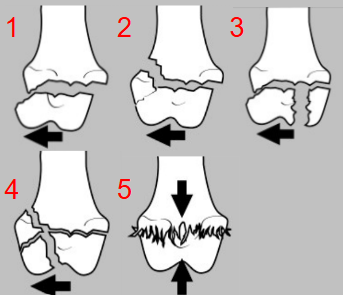
Salter Type I
Separation entire physis
shearing forces
good prognosis
Salter Type II
most common
through physis and metaphyseal
triangular shaped bone frag
good prognosis
Salter Type III
through articular surface, epiphysis and physis
intra-articular shearing force or a torsional force
Fair prognosis
Salter Type IV
through epiphysis, physis, and metaphysis
often older animals
poor prognosis
Salter Type V
through physis
severe crushing forces
poor prognosis
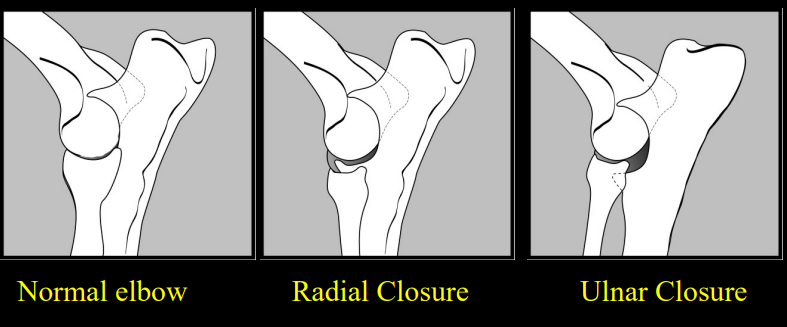
Premature Physis Closure
Distal Ulnar
Short ulna
Radius may bow
Distal radius is subluxated craniomedially from the radial carpal bone
foot deviates laterally
wide humero-ulnar joint
common
Distal Radial
Short radius
Wide radiocarpal and radiohumeral joint space
elbow/carpus degeneration
Fracture classifications
Open Fracture (compound fracture)
exposed to enviro
Closed Fracture (simple fracture)
contained in the body
Incomplete Fracture
partial break
immature animals “greenstick” fracture
Fissure Fracture
incomplete fracture off of a complete fracture
Depression Fractures
multiple fissure fractures
common in skull
Complete Fractures
complete loss of bony continuity
deformed
Transverse Fracture
transverse to the long axis
bending forces
Oblique Fractures
oblique to the long axis
two cortices of each fragment are in the same plane without spiraling
bending forces
Spiral Fractures
fracture line that spirals along the long axis
Comminuted Fracture
+3 interconnected fractures
high energy trauma
Multiple Fracture
+3 not interconnected fractures
Impaction or compression fracture
bony fragment forced into cancellous bone
end of long bones
Avulsion Fracture
violent contraction of a muscle rip off bone
Chip fracture
fragment
Slab Fracture
expansile articular fracture
Pathological Fracture
secondary to disease
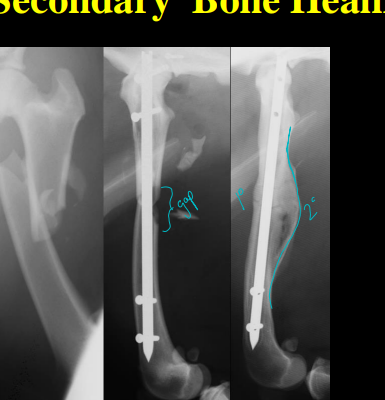
Bone Healing types
Primary
ideal
direct growth of an Haversian system
does not occur across fracture gaps
RS
Lack callus
Gradual decreased opacity and fracture line
secondary
common
when rigid internal fixation does not exist
Factors That Affect Bone Healing
Vascular Integrity
poor blood flow reduces healing
Location
Metaphyseal heal faster
diaphyseal heal slow
antebrachial heal slow
Cancellous bone heal fast
Cortical bone heal slow
Mobilization
rigidity heals fast
Type
complicated heals slow
Postreduction Apposition
good apposition heals fast
Age
young heals fast
Local Trauma
with severe soft tissue injury heals slow
infectsion slows healing
malignancy slows healing
Bone loss
excessive distraction heals slow
Corticosteroids
slow healing
inhibit the differentiation of osteoblasts
Evaluation of fractures
alignment, joints, rotation, fixation
Tx. Sx or casting
6 cortices engaged with screws above and below the fracture site
Complications
Malunion and warping
hard to see in young dogs till mature
Delayed Union
Non Union
no healing for 90d
atrophy of region
Hypertrophic
lysis
Cortical discontinuity
Non bridging callus
angular deformity
Atrophic
Min callus formation
defined gaps
Osteochondrosis
Cause
dysfunction of endochondral ossification
thick weak cartilage
chips off
CS
young Lg breed males
front limb lameness
Location
Shoulder (#1): caudal or caudal-lateral humeral head
Elbow: distal medial humeral condyle
Stifle: distal lateral femoral condyle
Tarsal: medial trochlear ridge of the talus
RS
Calcified flap of articular cartilage, secondary DJD, Joint effusion
DDx
long digital extensor fossa can be confused for an OC lesion
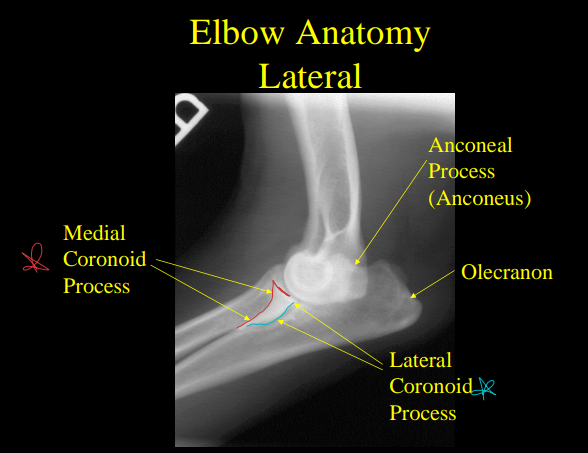
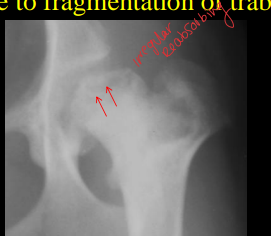
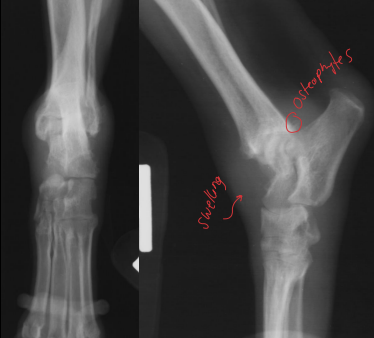
Fragmented Medial Coronoid Process
Cause
Young Lg male dogs
elbow dysplasia
CS
Stiff front end, lameness, elbow pain, DJD in older animals
Rs
osteoarthritis, osteophytes on the anconeal process and radial head, sclerosis of the trochlear notch of the proximal ulna, repair on medial coronoid process of the ulna
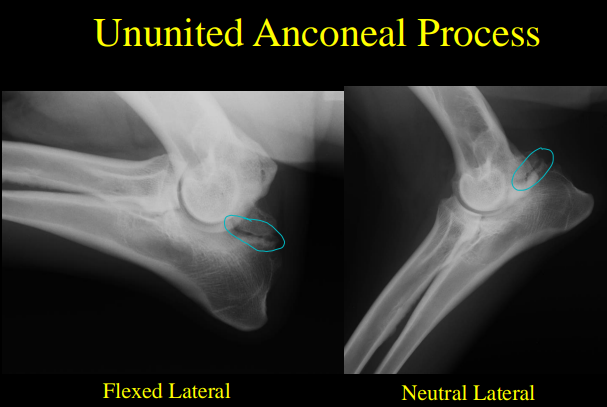
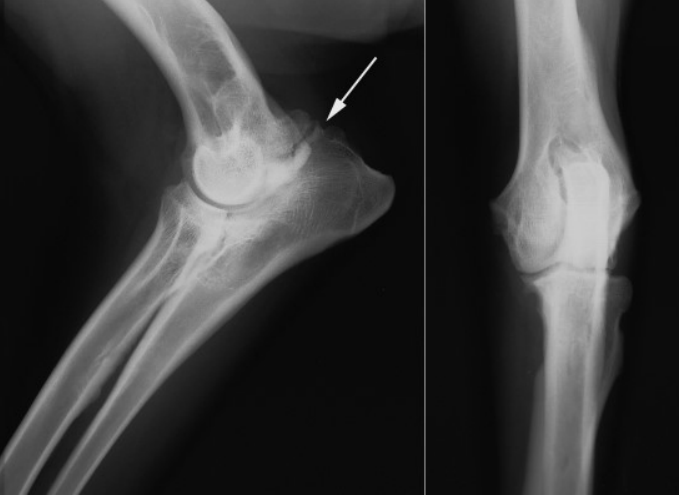
Ununited Anconeal Process
Cause
Anconeal process forms from a separate center of ossifications
unfused
Young Lg dogs
GSD
CS
weight bearing lameness
RS
Irregular radiolucent line cross the anconeal process
Retained Cartilaginous Core
Cause
Young Lg dogs
Unknown
core of cartilage in the metaphysis
issue of osteochondrosis of the distal ulnar physis
cartilage does not transform into bone
CS
self limiting
retard growth of the distal ulnar physis causing angular limb deformity
RS
Conical shaped radiolucent zone extending from the distal ulnar physis into the distal ulnar metaphysis
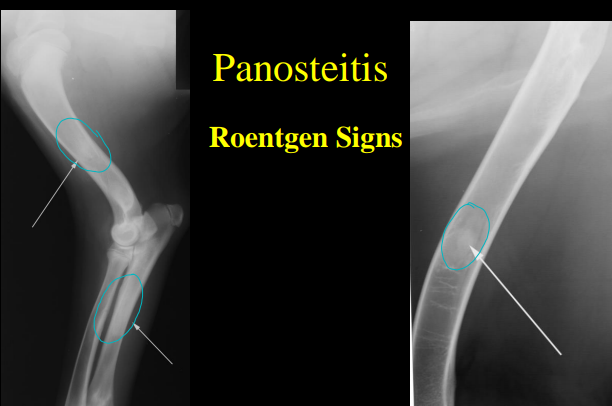
Panosteitis
Cause
Young male Lg dogs
GSD
CS
self limiting, front limb lambess, front limb long bone pain
RS
Increased intramedullary opacity, blurring of the trabecular pattern, patchy medullary opacities, rough endosteal surface
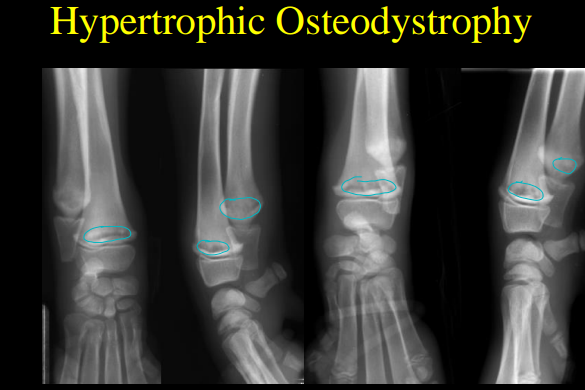
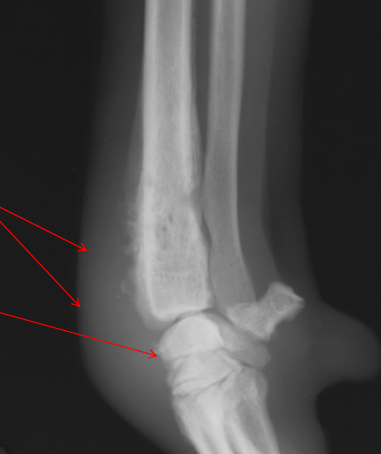
Hypertrophic Osteodystrophy
Metaphyseal flaring – lacy bony appearance around physeal
Cause
Young Lg male dogs
CS
Self limiting, lamness, painful, swelling around long bones, Pyrexia
RS
necrotic marginated line parallel to physis, metaphyseal flaring
Legg Calve Perthes Disease
Cause
Young SMALL dogs
necrosis of the capital femoral epiphysis from poor blood supply
Unilateral
CS
Weight bearing lameness, leg pain
RS
Increased width of joint space and opacity of femoral head, patchy lysis
FHO sx
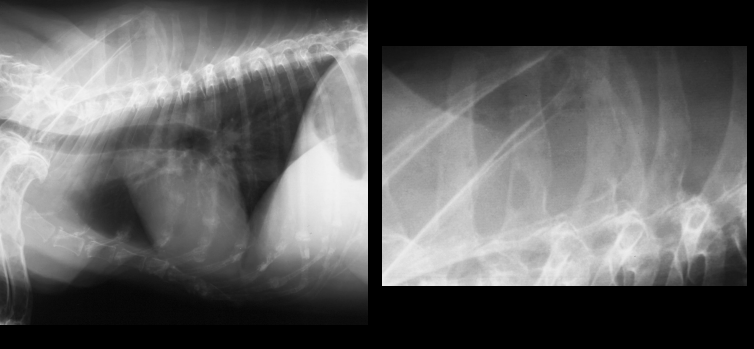
Hypertrophic Osteopathy
Cause
old dogs with lung dx
Hormonal, neural, hypoxia
Begins on the abaxial surface of digit 2,5 and moves proximally
CS
pulmonary dx or masses, 4 limb lameness, distal limb swelling
RS
irregular periosteal reaction of tubular bones and accessory carpal/calcaneous
Degenerative Joint Disease
Cause
multifactorial, non-septic disorder of synovial joints
deterioration of articular cartilage leading to inflammation of joint
CS
slow onset progressive intermittent lameness, work out of lameness with movement
RS
Intracapsular swelling
Increased joint space if acute, decreased size if chronic destruction of the cartilage
articular cartilage proliferation in non weight bearing areas
cartilage proliferation outgrows it nutrient supply
Perichondral osteophytes
Detached pieces of articular cartilage, Joint “mice”
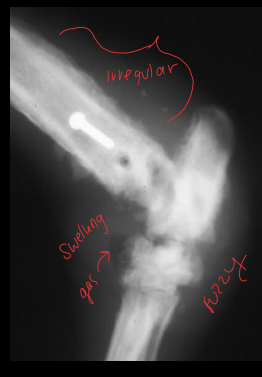
Septic Arthritis
Cause
Adults with penetrating wounds or no wound history in puppies
Joint infection
CS
Severe pain and joint effusion, lameness, fever, anorexia, lethargy, single joint (except puppies)
RS
tissue swelling, chronic bony changes, gas in tissue, lysis, severe subchondral erosion
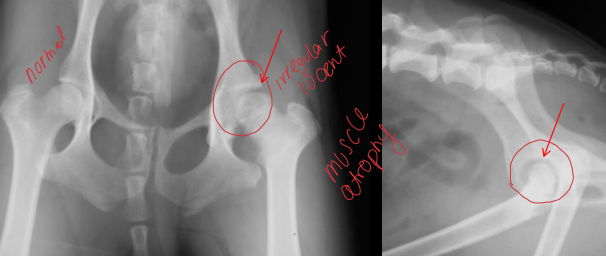
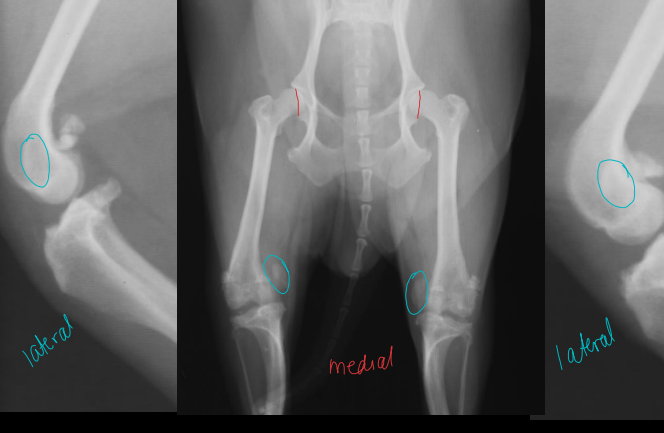
Hip Dysplasia
Cause
High estrogen
Lg dogs
GSD
genetic or environmental
laxity of the coxcombical joint
3 months to 3 years (often worse at 9-11 months) or at old age
CS
lameness, pain, restricted potion, difficulty standing and climbing
RS
cranial joint wedging, <1/2 of the femoral head covered by dorsal acetabular rim, thick femoral neck, shallow flat acetabulum, osteophytes
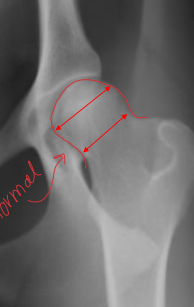
Evaluation
Penn Hip: 4mths
measured distance between the femoral head center and the acetabular center with pressure added
0 = tight
>0.4= high risk
1= luxated
OFA
must be 24m of age or older
extended VD view evaluated by radiologists for subluxation, shallow acetabula, remodeling, osteoarthritis
Excelent = improved
Good= normal
Fair= minor issues
Borderline= marginal issues
Mild= minor dysplastic changes
Mod = defined dysplastic changes
Severe = marked
TX.
Triple Pelvic Osteotomy in young dogs, hip replacement, Femoral Head and Neck Ostectomy as a salvage procedure
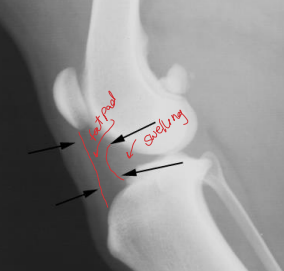
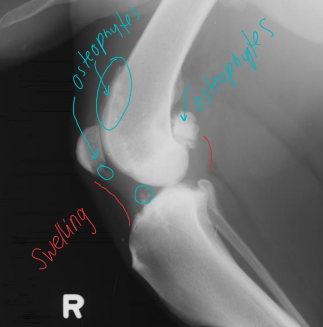
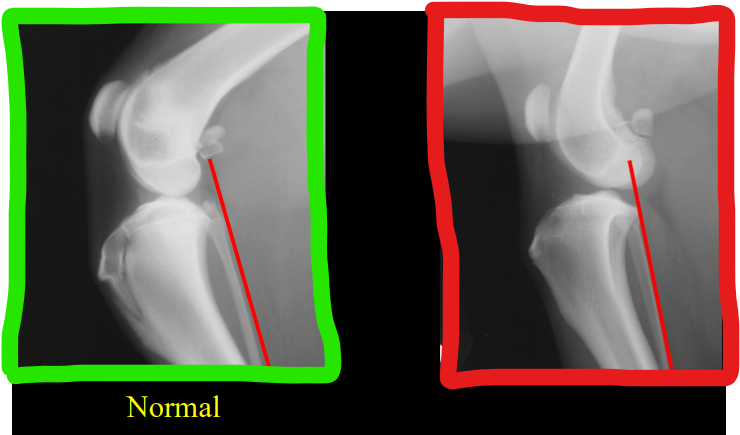
Cranial Cruciate Disease (CCL)
Cause
Young athletic (acute) or fat dogs (chronic)
degeneration, separation, weaking of the lig
CS
Non weight bearing lameness, patellar luxation
RS
cranial tibia displacement, “Rad Drawer sign”, Intracapsular swelling squishing fat pad, joint mice from evulsion fracture, swelling of the medial joint capsule (medial butrus), osteoarthritis
Patellar Luxation
Cause
Medial young sm dogs
Lateral young Lg dogs
congenital or traumatic
CS
lameness
RS
Patella is medial to trochlear groove, lateral bowed distal femur, Medial proximal tibia bowing and quadriceps muscles, shallow tronchlear groove, osteoarthritis
Arthridities
Destructive (erosive)
Lysis and erosion of articular and cortical bone
Narrow joint
Intracapsular effusion
Non-destructive (non-erosive)
no Lysis or erosion of articular and cortical bone
Narrow joint
Intracapsular effusion
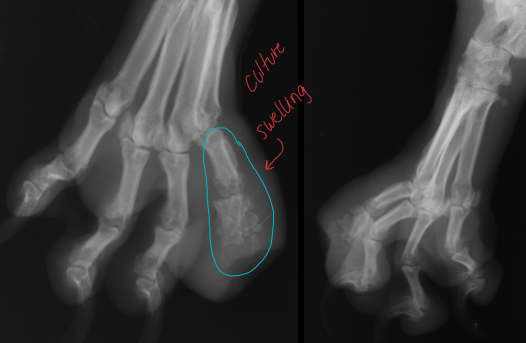
Erosive Polyarthritis
Cause
most common is Rheumatoid Arthritis
carpal and tarsal bones
Middle aged Sm poodles and shelties
granulation tissue invasion, collagenase damages capsule and lig
CS
shifting lameness, low grade, fever, anorexia, and slight generalized lymphadenopathy
RS
lucent, cyst-like subchondral lesions, narrow joints, subluxation and luxation
Osteomyelitis
Cause
Fungal or bacterial infections, often resp invasion
Blastomyces dermatitidis (south)
Coccidioides immitis (west)
Histoplasma capsulatum
Cryptococcus neoformans & Aspergillosis
40% polymicrobial
15% anaerobic
Lg mid age male dogs
working breeds
CS
local swelling, draining tract, lameness, systemic dx
RS
lysis and productive changes, periosteal reaction, sclerosis
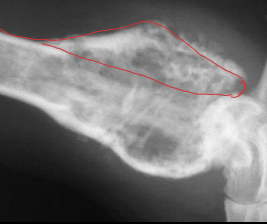
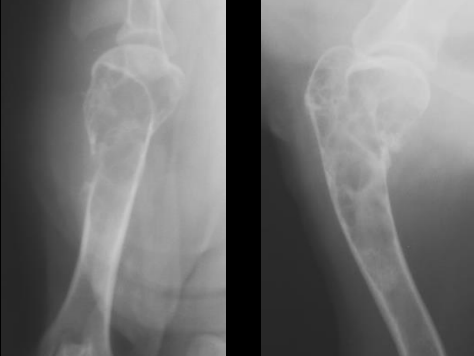
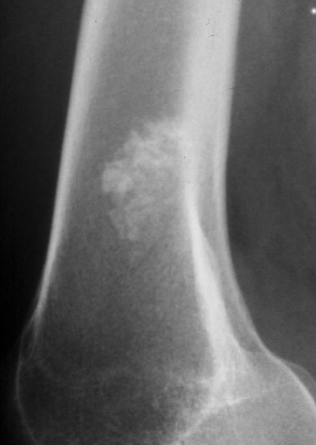
Primary Bone Neoplasia
Cause
Lesion usually solitary in long bones
Osteosacrcoma #1
Signalment
Lg mid age male dogs
CS
Swelling, lameness
RS
aggressive osteoblastic or osteolytic metaphyseal leasons, do not cross joints
“Toward the knee and away from the elbow”
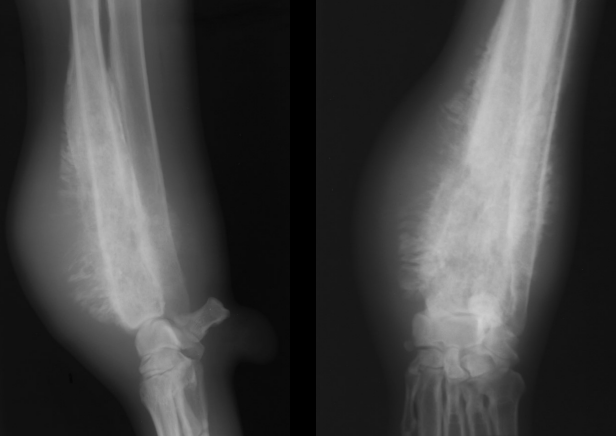
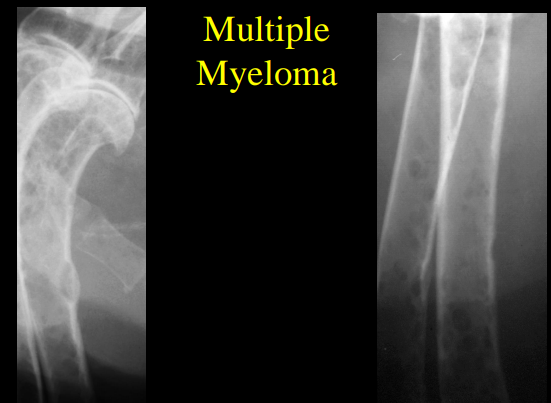
Multiple Myoloma
Purely lytic
“punched out” of flat bones
Little to no periosteal reaction
No bony production
Benign Bone Cysts
Cause
unkown
CS
none, can cause pathologic fractures
RS
Expansile, lucent, bony lesion with decreased trabecular markings, No periosteal reaction, Sharply defined zone of transition, Cortical bone thinning, no lysis
Benign Bone Tumors
Cause
Osteochondroma, osteoma, odontoma, exostosis
Signalment
Old animals
CS
asymptomatic
RS
Sharp transition, min periosteal reaction, no lysis, osteoproduction
Metastatic Bone Neoplasia
Cause
Prostatic adenocarcinoma, transititional cell carcinoma, mammary adenocarcinoma
Signalment
Old animals
CS
generalized bone pain
RS
Diaphyseal reactions
Synovial Cell Sarcoma
Cause
Unknown
arises from tendon sheath or synovial lining
Signalment
Old Lg dogs
CS
joint pain and swelling, lameness
RS
metastasis, lobulated soft tissue swelling, lysis of lg appendicular joints
Next step — Chest xrays!