2nd/3rd Trimester Placenta and Umbilical Cord (Ch. 56 & 57)
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
T/F: placenta is a multifunctional organ
True—it acts as baby’s lung (supply oxygen), kidneys (filter waste), and GI and immune systems (deliver nutrients and antibodies)
placenta
major role in exchanging oxygenated maternal blood with deoxygenated fetal blood
develops from trophoblastic cells
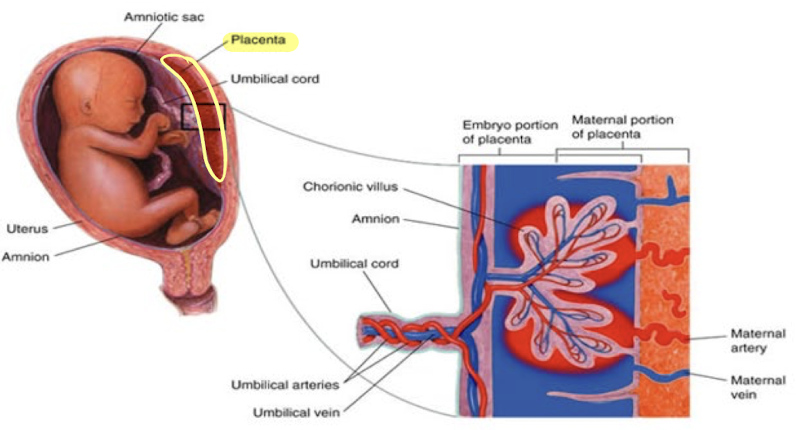
what are the functional units of the placenta?
chorionic villi
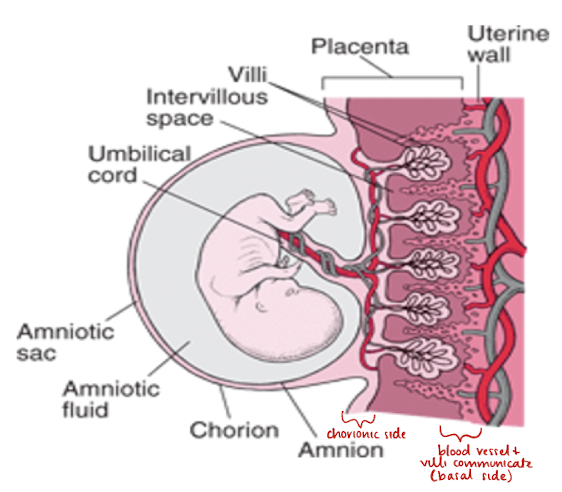
placenta anatomy
divided into 2 parts
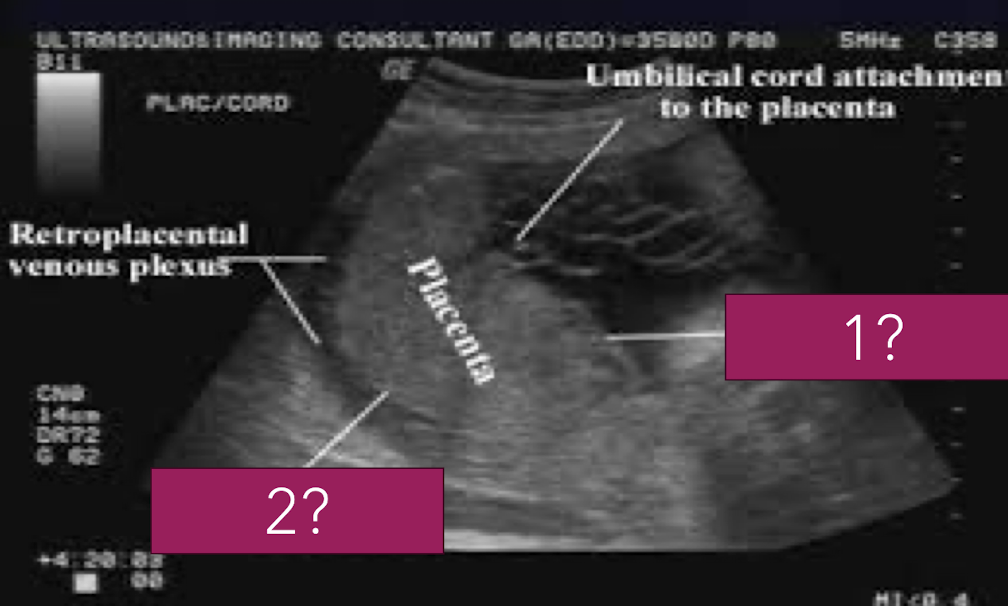
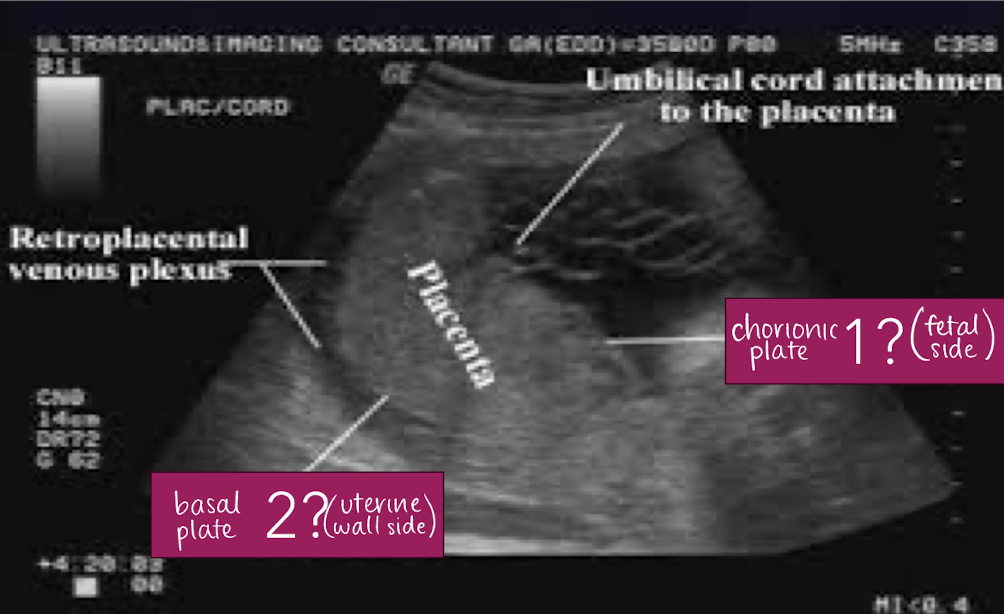
chorionic plate (fetal surface)
surface facing amniotic fluid
continuous with chorion
basal plate (maternal surface)
surface facing uterine wall
continuous with decidua basalis
placenta plate facing amniotic fluid/fetus is called…
chorionic plate
placenta plate facing uterine wall/mom is called…
basal plate
placenta physiology: 3 functions
respiration (supply oxygenated blood to baby)
excretion (remove waste produce and deoxygenated blood)
nutrition
placenta physiology: hormones
placenta produces and secretes:
HCG
estrogen
progesterone
placenta fully develops at __ weeks
15
what is a normal placenta size?
2 to 4 cm AP thickness
measuring technique for placenta
measure in AP dimension
thickest portion perpendicular to uterine wall
DO NOT include uterine wall in measurement
typically measure after 23 weeks

causes for large placenta
diabetes
anemia
hydrops
torch infections

3 causes for small/thin placenta
infection
intrauterine growth restriction (IUGR)
aneuploidy (chromosomal abnormality)
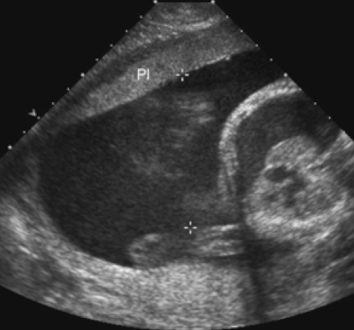
SONO: placenta
homogeneous
pebble-gray—mildly more echogenic compared to uterine wall
may be more echogenic in 1st trimester
smooth borders
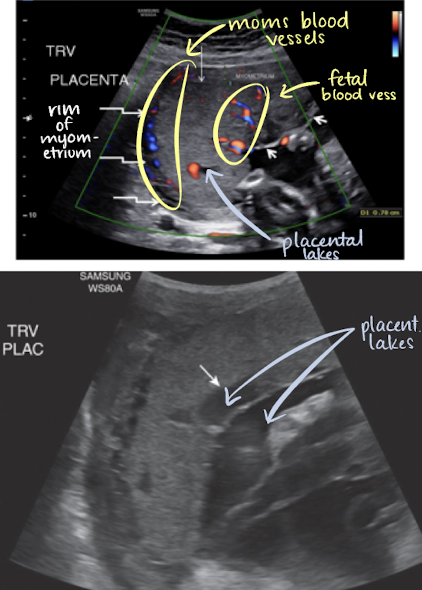
highly vascular structure
rim of myometrium outside placenta should be noted
prominent maternal vessels may be seen posterior to placenta (anechoic tubes)
placental lakes may also be seen in placenta
what to document when evaluating the placenta:
size/shape/position
cord location
abruption
hematoma
location (previa)
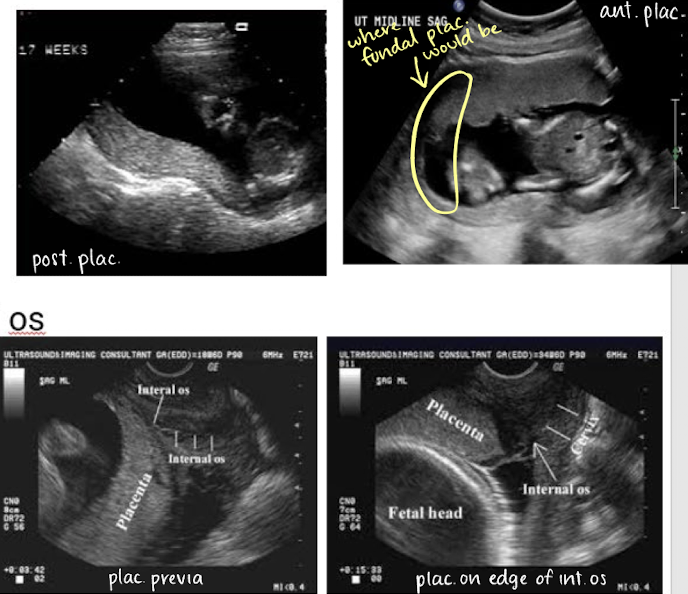
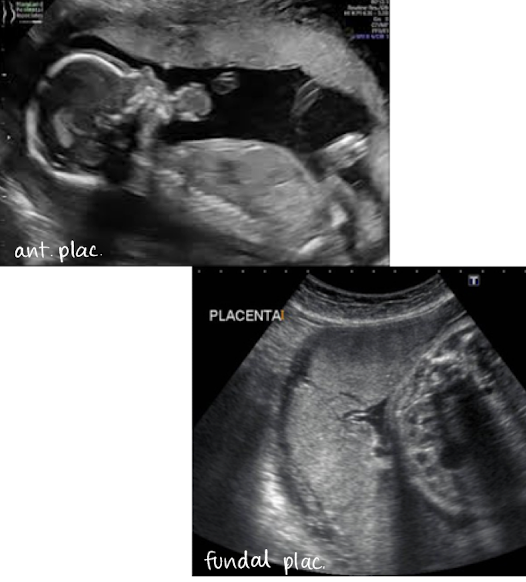
describing placental location in uterus and in relation to cervical os
in uterus
anterior
posterior
fundal (in uterine fundus)
in relationship to cervical os
close to os
away from os
covering os
if covering internal os, that is called previa
3 ways placenta appearance can be temporarily altered
placental migration
distended bladder
Braxton-Hicks contraction
placental migration
refers to when placenta changes position in uterine cavity
primarily explained by 2 theories:
LUS growth theory (when expanding uterus pulls placenta upward)
trophotropism theory (atrophic placenta in areas of low blood supply)
location of placenta can be identified in 1st trimester
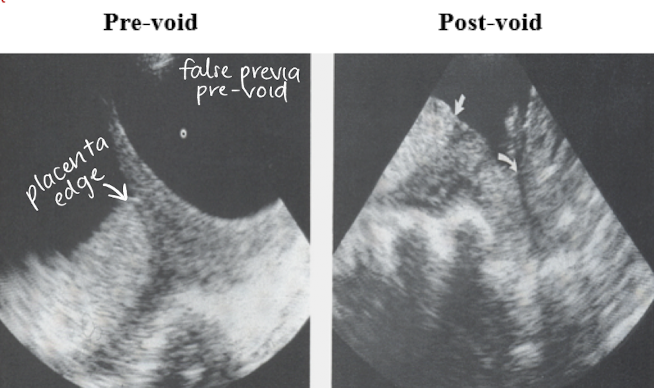
distended bladder
changing bladder shape can create appearance of placental movement or a change in placental shape
full bladder can elongate cervix and give false impression of previa
emptying bladder allows cervix to be in normal position
** have patient empty bladder and reimage if previa is seen
Braxton-Hicks contraction
practice/false contractions
transient myometrial (uterine wall) contraction
created appearance of a placenta mass (distorts placenta shape)

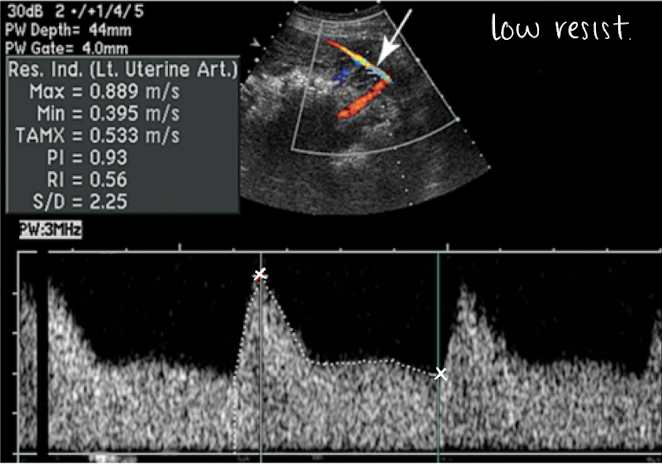
placental PW doppler and SONO evaluation
uterine artery PW (varies based on trimester):
high RI flow pattern in 1st trimester
low RI flow pattern in 2nd trimester
lots of blood flow going through uterine artery to get to placenta and supply baby with oxygen
SONO evaluation:
use optimal gate, gain, scale, placement
measure waveform and RI
4 permanent placental variations
succenturiate lobe
circumvallate or circummarginate
battledore cord insertion
velamentous cord insertion
succenturiate lobe
aka accessory placental lobe
one or more accessory placental lobes
circumvallate or circummarginate
rare (1-2% of pregnancies)
chorionic plate (fetal side) is smaller than normal —> amnion and chorion membranes fold back around the edges of placenta
”double back”
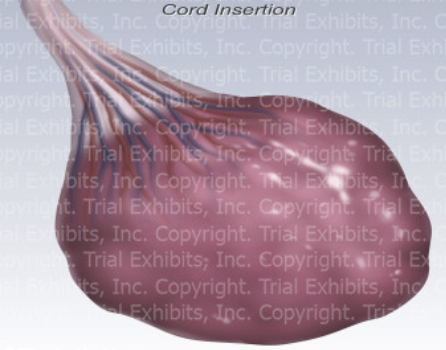
battledore cord insertion
aka marginal cord insertion
cord attaches at edge of placenta
“battledore” means badminton racket —> placenta is woven racket and cord is the handle
7-9% of pregnancies
MC in twins
battledore cord insertion is usually ok, but could lead to…
IUGR (intrauterine growth restriction)
preterm labor
fetal distress during labor
risk of placental abruption
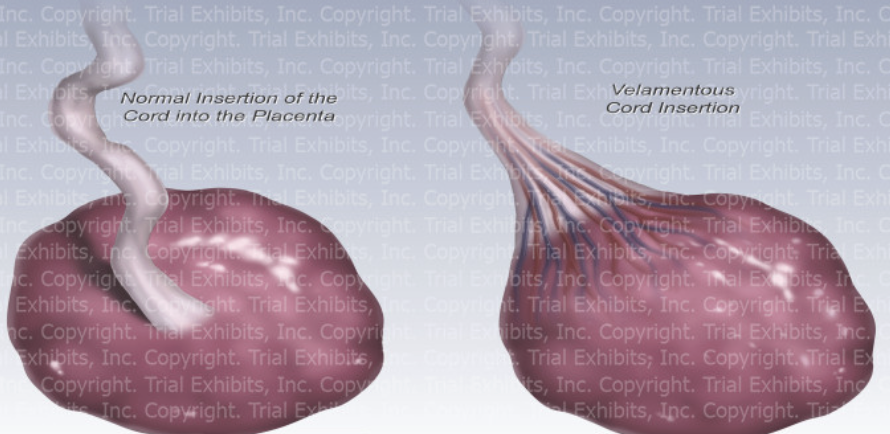
velamentous cord insertion
RARE (0.1-0.8 of pregnancies)
cord attaches to fetal membranes (amnion and chorion) increase of placental disc
fetal arteries and vein are UNPROTECTED by Wharton’s Jelly at insertion
high risk of cord compression, trauma, and rupture—especially during labor
delayed umbilical cord clamping
babies are born with 2/3 of their blood
1/3 of their blood is still in placenta
umbilical cord clamping/cutting is not done immediately after birth
wait 30-60 seconds after birth to allow more blood to transfer from placenta to baby
benefits:
babies have higher hemoglobin
higher iron
better transition to breathing outside
** now a widely recommended as standard care

umbilical cord
connecting yolk stalk and allantois ducts become the umbilical cord
allantois connect to fetal bladder (abdominal/fetal cord insertion point)—becomes belly button
allantoic vessels become umbilical vessels
surrounded by mucoid connective tissue: Wharton’s Jelly
cord covered by amniotic membranes
normal diameter: 1-2 cm
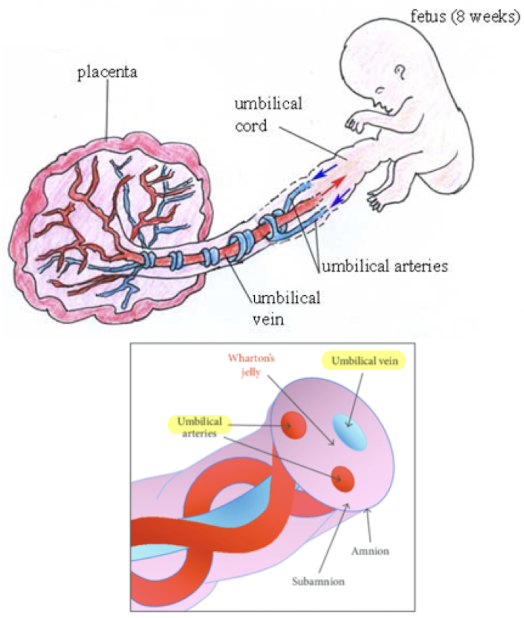
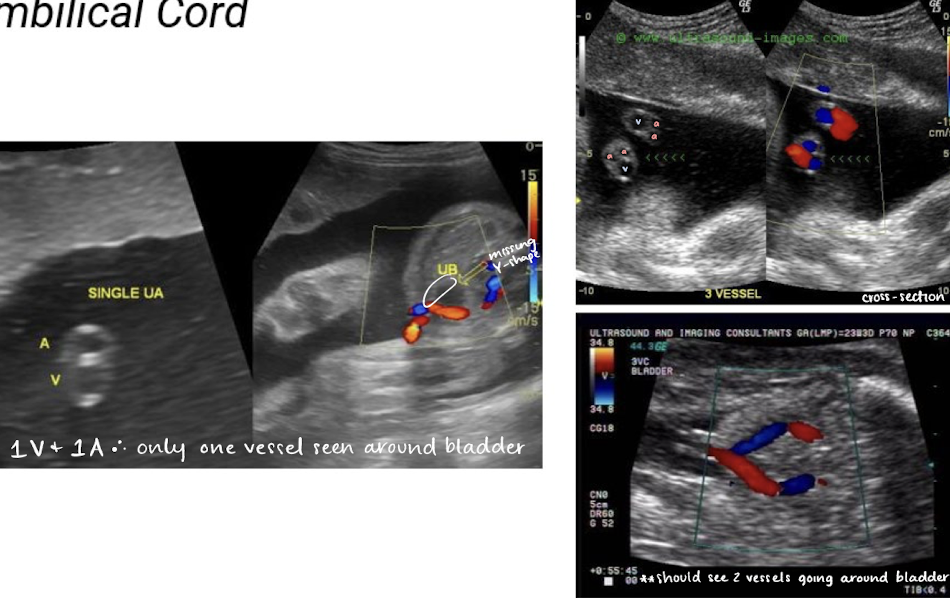
umbilical cords have how many vessels
2 smaller arteries, 1 large vein
single umbilical artery (2 vessel cord) is found in 1% of singleton births
can be isolated
can be associated with congenital malformation
** umbilical arteries and vein functions opposite from typical a. and v.

umbilical arteries
2 umbilical arteries carry deoxygenated blood from fetus to placenta
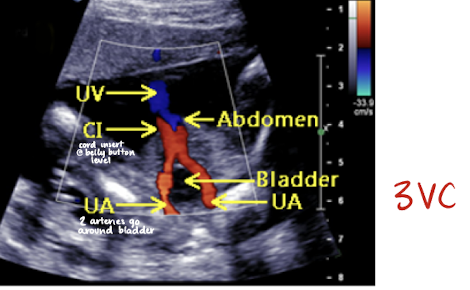
umbilical arteries can be noted on either side of bladder at fetal insertion
umbilical vein
1 umbilical vein carries oxygenated blood from placenta to fetus
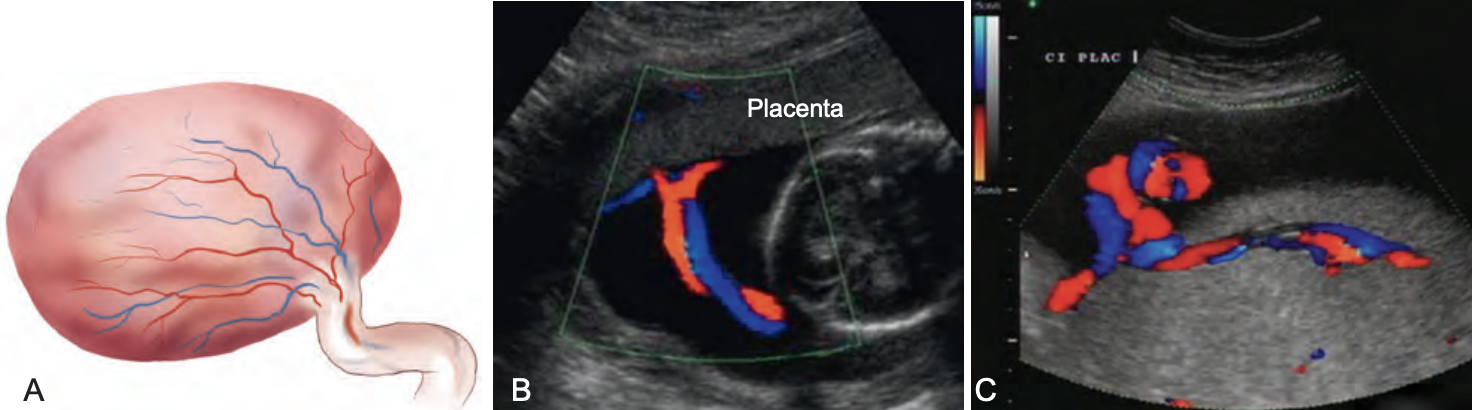
umbilical cord color Doppler
color Doppler is used to visualize umbilical arteries and vein
the bladder, when full, is seen between 2 umbilical arteries
umbilical cord should be images in cross section and with color Doppler at level of bladder to confirm the number of cord vessels
type of placenta?
succenturiate lobe (accessory placenta)

type of placenta?
circumvallate/circummarginate (chorionic plate is smaller than basal plate —> folded membranes)

type of placenta?
battledore cord insertion (umbilical cord attaches to edge of placenta, rather than center)
type of placenta?
velamentous cord insertion (umbilical cord inserts into fetal membranes rather than placenta)
type of placenta?
battledore cord insertion
chorion frondosum
“portion of chorion that develops into fetal portion of the placenta” (chorionic plate)
chorionic villi
“microscopic vascular projections from chorion that combine with maternal uterine tissue to form placenta”
which part of the decidua surrounds the chorionic sac?
decidua capsularis
which part of the decidua unites with the chorion to form the placenta?
decidua basalis
placenta accreta vs. placenta increta vs. placenta percreta
placenta accreta
growth of chorionic vlli superficially to myometrium; not does penetrate through myometrium
placenta increta
growth of chorionic villi deep into myometrium
placenta percreta
growth of chorionic villi through the myometrium to the uterine serosa
Wharton’s jelly
mucoid connective tissue that surrounds the vessels within umbilical cord