Connective Tissue Disease, Vasculitis and Related Disorders
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
Connective tissue disease triggers
1- Unknown (usually)
2- Sunlight
3- Infection
4- medication

Vasculitis
Vasculitis pathophysiology
- Complex and poorly characterized.
- Antibodies or immune complex-mediated.
- Immune complex deposition at blood vessel wall >> Inflammation >>
Complement activation & inflammatory mediators release >> vasodilatation &
polymorph accumulation >> Leakage so RBC extravasation >> occlusion of blood
vessels >> Ischemia.

Bullous vasculitis with necrosis
Vasculitis clinical presentation:
• General malaise
• Fever
• Abdominal pain
• Arthropathy
• Skin lesions:
- Non-blanching
- Erythematous macular, palpable purpura
- Can become blistering, ulcerated, and necrotic.
- Transient or last for weeks.
- Painful and unpleasant.
- M.c Location: Lower Limbs
Polyarteritis Nodosa Clinical Presentation:
General:
• General malaise
• Fever
• Weight loss
• Weakness
• Arthralgia
• Neuropathies
• Renal involvement (can cause renal failure)
Cutaneous:
• Livedo reticularis (subtle lacy mottled pattern)
• Purpura
• Tender subcutaneous nodule
• Ulceration
• Necrosis
• M.C location: Lower limbs.

Retiform Purpura PAN

Livedo reticularis PAN

PAN Retiform Purpura

PSN Retiform Purpura

PAN Ulceration Necrosis
PAN investigations
1. Angiography
2. Tissue biopsy ( skin, sural nerve, muscle )
PAN management
1. Corticosteroids (oral)
2. Cyclophosphamide in severe cases.
Henoch – Schönlein purpura pathophysiology
Deposition of IgA, complement and immune complexes in small vessels
(arterioles, capillaries , venules) leading to systemic vasculitis.
• Skin, kidney, GI tract, and joints are mainly affected.
Henoch – Schönlein purpura Clinical Presentation:
• Cutaneous:
• Vasculitic rash on the buttocks and lower
legs
• Might be associated with edema of
scrotum/hands/ears
• GI: Abdominal pain, Vomiting
• Joint pains in the knees/ankles
• Hematuria.

Henoch – Schönlein purpura

Henoch – Schönlein purpura

Henoch – Schönlein purpura

Henoch – Schönlein purpura
Henoch – Schönlein purpura Investigations:
1. Hx and P/E
2. Skin biopsy:
-Deposition of IgA on immunofluorescence (support the diagnosis).
Henoch – Schönlein purpura management
• Usually supportive (recovery in weeks)
• Systemic corticosteroids:
-If persistent disease
-Can treat skin, GI, and arthritis symptoms
-Don’t prevent or treat renal disease
Management of cutaneous vasculitis
• Treat any underlying causes.
• Support hosiery should be used and the leg elevated on sitting.
• For mild to moderate cutaneous involvement:
-Potent topical steroids can be applied to the affected skin.
• In severe cases:
-Systemic corticosteroid
-Anticoagulation with warfarin or heparin.
• In persistent cases:
-Alternative immunosuppressants (Methotrexate or Azathioprine) may be
needed.
Raynaud’s phenomenon associated with
Raynaud’s disease, systemic sclerosis, mixed connective tissue disease, SLE, and Cryoglobulinemia.
Raynaud’s phenomenon types
1. Primary: Symmetric, before 30 years old, no skin manifestations, idiopathic.
2. Secondary: Asymmetric, ANA can be +ve, digital ulcerations can occur.
Raynaud’s phenomenon Symptoms:
1- Change in color after cold exposure:
White (Vasospasm) >> Blue (Cyanosis) >> Red (hyperemia).
2- Pain
3- Numbness
• The condition most frequently affects the finger in a symmetrical pattern
• Can also affect toes, nose, and ears.

Raynaud’s phenomenon

Raynaud’s phenomenon

Raynaud’s phenomenon
Raynaud’s phenomenon Investigations:
1- Full blood count
2- LFT and KFT
3- Coagulation profile
4- Thyroid function
5- Serum glucose
6- Creatinine kinase
7- Hepatitis serology
8- Antinuclear antibodies
Raynaud’s phenomenon management
1- Keeping peripheries warm
2- Nifedipine
3- Iloprost (Prostacycline Analogue)
Systemic sclerosis (SSc)
• Excessive sclerosis (i.e. collagen deposition and fibrosis) of
the subcutaneous tissues in the fingers and toes as well as
around the mouth (scleroderma), with similar changes
affecting the internal organs, particularly the lung and
kidneys.
• Blood vessels can be affected, leading to:
- Raynaud’s phenomenon (fingers)
- Telangiectasia (mouth and fingers)
Systemic sclerosis (SSc) classification:
1- Limited systemic sclerosis(lSSc):
2- Disseminated systemic sclerosis (dSSc):
3- Undifferentiated connective tissue disease
4- CREST syndrome
Limited systemic sclerosis(lSSc):
• Raynaud starts many years before
• Anti-centromere antibody
• Skin sclerosis distally does not cross the
elbows and knees
• Slowly progressing
• CREST is an example
Disseminated systemic sclerosis (dSSc):
• Raynaud starts 1-2 years before
• Antibodies ANA, Scl-70 (anti
topoisomerase)
• Sclerosis crosses elbows and knees
• Fast progress with internal organs
involvement ( heart, kidneys, lungs)

Raynaud’s and Telangiectasia associated with SSc
Systemic sclerosis (SSc) Clinical Features:
1- Raynaud’s phenomenon
2- Telangiectasia (mouth and finger )
3- Tethering of skin on the fingers/toes
which become very tight with a
waxy appearance and considerable
limitation of movement.

Tethering of skin on the fingers associated with SSc
SSc Diagnosis:
1- ANA ( 90% of patients with SSc will have at least one +ve ANA)
2- CRP / ESR ( raised)
3- High-resolution CT scan of the lung (thickening of the alveolar walls)
4- PFT (impaired ventilation – perfusion)
5- Skin biopsy (fibrotic changes seen in histology )

Morphaea associated with SSc
Benign form of localized systemic sclerosis in
which there is localized sclerosis with very slight
inflammation.
Morphaea stages
- Early stages: Dusky appearance of skin.
- Late stages: Discolored and Firm skin.

Localized morphea in the frontoparietal area is associated with alopecia and sunken groove of firm sclerotic skin.
CREST syndrome Symptoms:
• Calcinosis Cutis: Calcium deposits in the
skin are seen as chalky white material
which can be painful
• Raynaud’s phenomenon: First complaint
• Esophageal Dysmotility
• Sclerodactyly: Thickening of the skin of
the digit
• Telangiectasia: first seen in the face

CREST syndrome
CREST syndrome Management:
• Psychological support
• Patients should keep themselves warm
• Calcium-channel blockers
• Prostaglandins/prostacyclin analogue.
• Calcitriol (for sclerodactyly)
• Pulsed dye laser (for telangiectasia)
CREST syndrome investigations
• FBC (Full Blood Count)
• ANA
• Anticentromere antibodies
• Scl-70
Lichen Sclerosus pathophysiology
Unknown, but in early lesions there is an infiltrate of lymphocytes with CD3,
CD4, CD8, and CD68 markers.

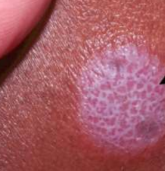
Lichen Sclerosus
Lichen Sclerosus Clinical Features:
• Well-demarcated atrophic patches and plaques
with a distinctive ivory-white color.
• Fibrosis of the underlying tissues with associated
loss of normal genital architecture
• Frequently affects the vulva and perineum, but
may also affect the penis and extragenital skin.
• Children: Acute, resolves
• Adults: chronic, rarely associated with the
development of squamous cell carcinoma (SCC).
Lichen Sclerosus Treatment:
• Intermittent potent topical steroids, which usually
control itching.
• If pruritus is not controlled by potent topical
steroids or soreness develops, you have to rule
out the development of SCC.

Lichen Sclerosus
Lichen Planus Histological features:
Characterized by a band of lymphocytes attacking the basal keratinocytes which
result in edema, subepidermal clefts, and death of some keratinocytes

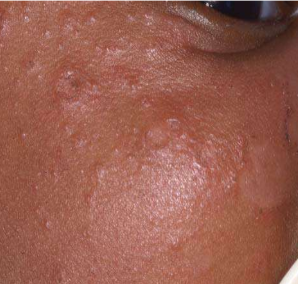
Lichen Planus

Lichen Planus wickham striae
Lichen Planus Clinical features:
• Itchy eruption consisting of shiny purple-colored flat-topped papules (6 Ps: Pruritic polygonal purple planar papules and plaques)
• Appear on the wrists and ankles.
• White lines called Wickham’s striae may appear on the surface of the lesions at any site
• Lesions may appear in clusters or in linear scratches/surgical scars (Koebner phenomenon)
• In patients with black skin, LP may be very hypertrophic and heal with marked post-inflammatory hyperpigmentation.
• Mouth (buccal mucosa), and genitals (erosions on labia minora ) may also be involved
• Distinctive linear ridges may affect the nails.
• Scalp lesions are often scaly with marked follicular plugging that may result in scarring alopecia.
• Severe acute lichen planus can manifest as bullous lesions

Lichen Planus

Lichen Planus erosions in mouth-wickham striae
Lichen Planus wickham striae

Lichen Planus sever with bullous lesions

Lichen Planus sever with bullous lesions

Lichen Planus sever with bullous lesions

Lichen Planus

Lichen Planus sever with bullous lesions
Lichen Planus treatment:
• Potent topical steroid applied to the itchy active lesions
• Occlusion of the steroid for hypertrophic lesions.
• Severe lichen planus can be treated with systemic Corticosteroids, mycophenolate mofetil, methotrexate, or azathioprine
Lichenoid drug eruptions Clinical Features:
• Clinically similar to LP
• Lesions are usually more extensive and oral involvement is rare .
• Lesions only resolve very slowly after the drug is stopped, generally taking 1–4 months to settle and usually leaving hyperpigmentation on the skin.
drugs that cause Lichenoid drug eruptions
Antihypertensives, ACE inhibitors, beta-blockers, nifedipine, methyldopa
Clinical variants of lupus erythematosus
• Systemic (SLE)
• Subacute cutaneous lupus
• Discoid Lupus
• Neonatal Lupus
Systemic Lupus erythematosus presentation
• 75% of patients have skin involvement, most commonly an erythematous ‘butterfly’ distribution rash on the face, Photosensitivity, hair loss, and areas of cutaneous vasculitis.
• As the disease progresses the cutaneous manifestations can become extensive.
• Systemic changes include fever, arthritis, and renal involvement, but there may be involvement of a wide range of organs.
Drugs that can trigger Systemic Lupus erythematosus
chlorpromazine, quinine, and isoniazid.
Systemic Lupus erythematosus Tx
• Prednisolone is usually required
• Sometimes immunosuppressant drugs such as azathioprine as well.

Subacute lupus erythematosus (SLE)
Erythematous annular and serpiginous eruption on the skin
(E.N.A (extractable nuclear antigen) test is positive in 60% and anti-cytoplasmic antibodies are present in 80% of patients.)

Discoid lupus erythematosus (DLE)
Well-defined erythematous lesions with atrophy, scaling, and scarring occur on the face, scalp (alopecia, follicular plugging), and occasionally arms.

Discoid lupus erythematosus (DLE)

Discoid lupus erythematosus (DLE)
DLE Tx
• Potent and super-potent topical steroids to limit
scarring
• Hydroxychloroquine 200mg twice daily can be
effective (ask about eye sx, rare ocular toxicity)
Neonatal lupus erythematosus
Skin lesions characterized by annular scaly and inflammatory lesions on the face/scalp.
• Congenital heart block (which may require pacing).

Neonatal lupus erythematosus
Neonatal lupus erythematosus Treatment:
Skin lesions may require topical steroids and sunscreen but usually resolve spontaneously as the level of autoantibody depletes.

Dermatomyositis V sign

Dermatomyositis shawl sign

Dermatomyositis Heliotrope Rash
Dermatomyositis clinical presentation
• Rash on a photosensitive distribution.
• Characterized by a purple hue (heliotrope) on the upper eyelids, cheeks, and forehead.
• The anterior neck and chest rash is a ‘V’ sign while posteriorly is called a shawl sign.
• The dorsal surface of the fingers may be affected by the erythematous eruption and purplish (Gottron’s) papules may predominate over the dorsal finger joints.
• Ragged cuticles and dilated nail-fold capillaries may also be seen.
• There is a variable association with muscle discomfort and weakness, which is mainly in the proximal limbs but bulbar and respiratory muscles may be affected.
• In adults may precede the diagnosis of an underlying tumor (most commonly breast, lung, ovary, or gastrointestinal tract)

Dermatomyositis Gottron’s papules

Dermatomyositis Gottron’s papules

Dermatomyositis Ragged cuticles and dilated nail-fold capillaries
Dermatomyositis Investigations:
• Labs: Creatine phosphokinase (CK), ESR, Anti-Jo-1 antibody.
• Skin and muscle biopsy.
• Electromyography and MRI can help demonstrate myositis.
Dermatomyositis Treatment
• High-dose systemic corticosteroids (60–100mg daily) or pulsed methylprednisolone (1 g daily for 3 days) helps achieve rapid control of symptoms.
• Pulsed cyclophosphamide, azathioprine, methotrexate, and mycophenolate mofetil.
• Treatment of any underlying malignancy will usually lead to the resolution of these skin signs.
Mixed connective tissue disease (MCTD) Clinical Features:
They usually have Raynaud’s phenomenon, sclerodactyly/swollen hands, arthritis/ arthralgia, Sjogren syndrome, myositis, malaise, oesophageal dysmotility, trigeminal neuralgia, & pulmonary hypertension.
(its a combination of SLE, scleroderma, and myositis)
MCTD Investigations:
Positive antibodies to U1-ribonucleoprotein (RNP) and small nuclear ribonucleoprotein (snRNP)
MCTD Treatment
• NSAIDs are used to reduce pain and inflammation and the newer cyclooxygenase 2
(COX-2) inhibitor celecoxib is increasingly used to help reduced arthritis and myositis.
• Hydroxychloroquine
• For refractory disease low dose of oral corticosteroids and methotrexate