Psychology - MDD
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
MDD terms
Major depressive disorder is most often diagnosed when an individual experiences two weeks of either a depressed mood or a loss of interest and pleasure combined with 4 additional symptoms below.
Feelings of guilt and sadness.
Lack of enjoyment or pleasure in familiar activities or company.
Lack of initiative.
Frequent negative thoughts.
Irrational hopelessness.
Difficulties in concentration.
Inability to make decisions.
loss of energy.
insomnia, or hypersomnia.
weight loss/gain.
Etiologies
The explanation of the cause of a disease or disorder.
prevalence
Prevalence rates are not simply statistical accounts of how many people suffer from a specific disorder.
They also provide us with information about the nature of disorders. For example, we sometimes see that there is a difference in the prevalence rates of a disorder in men and women.
We also see that different cultures have different levels of a disorder.
Point Prevalence rate - proportion of the population diagnosed with the disorder.
Period Prevalence - is the proportion of a population that has the disorder at some time during a given period (year to year)
Onset Age - the average age someone is diagnosed with a disorder.
Depression is more prevalent in women than men.
Point Prevalence: 2015 National survey on Drug use and Health found that one year prevalence rates of depression are 8.5% for women and 4.7 for men.
Clinical biases in diagnosis
There is stigma associated with depression in many cultures so people will not seek help.
Men typically avoid doctors and culturally do not like to speak about emotions.
Psychological symptoms may be expressed as physical pain. (stomach upset rather than relating it to depression)
Classification Systems
Diagnosis of depression is based on classification system of symptoms.
Symptoms have to be present for two weeks.
Recently they added a change to exclude symptoms directly after a death. This would affect overall rates.
study one and year for prevalence
Brown & Harris 1978
Brown & Harris 1978
bg info
aim
sample
method
procedure
BG INFO: The Vulnerability model identifies the predictors of depression.
Protective factors: protect against the development of depression when experiencing stressors.
High levels of closeness with one's husband.
Socioeconomic status.
Meeting of basic needs.
These factors lead to higher levels of self-esteem and the possibility of finding other sources of meaning in life.
Provoking Agents: found to contribute to acute (recent) and ongoing stress.
These stressors could result in grief and hopelessness in vulnerable women with no social support.
Divorce, Loss of job, Loss of loved one.
Vulnerability factors:Long term factors found to increase the risk of depression in combination with provoking agents.
The most significant vulnerability factors were
Loss of one's mother before the age of 11
lack of a confiding relationships
more than three children under the age of 14 at home
persistent unemployment.
AIM: carried out a case study to determine the role of environmental factors in the onset of depression in women
SAMPLE: 498 women were surveyed on their daily life and depressive symptoms using a structured interview process.
The researchers focused on important biographical details - particular life events or particular difficulties faced by the women.
These events were later rated in severity by independent researchers.
METHOD: survey
The researchers identified three major factors that affected the development of depression.
Protective factors found to protect against the development of depression in spite of stressors, e.g. high levels of intimacy with one's husband. These factors lead to higher levels of self-esteem and the possibility of finding other sources of meaning in life.
Vulnerability factors found to increase the risk of depression in combination with particularly stressful life events - called provoking agents in the study. The most significant vulnerability factors were (1) Loss of one's mother before the age of 11, (2) lack of a confiding relationship, (3) more than three children under the age of 14 at home, and (4) unemployment.
Provoking agents found to contribute to acute and ongoing stress. These stressors could result in grief and hopelessness in vulnerable women with no social support.
Brown and Harris 1978
results
connections
8% of all the women - that is, 37 in total - had become clinically depressed in the previous year.
33 of these women (nearly 90%) had experienced an adverse life event (e.g. loss of a loved one) or a serious difficulty (e.g. being in an abusive relationship).
Only 30% of the women who did not become depressed suffered from such adversity.
Only 4 of the 37 women who became depressed had not experienced any adversity.
The study showed that social factors in the form of life stress (or serious life events) could be linked to depression.
The fact that working-class mothers were more likely to develop depression than middle-class mothers showed risk factors associated with social class.
According to Brown and Harris, low social status leads to increased exposure to vulnerability factors and provoking agents, whereas high social status was associated with increased exposure to protective factors and decreased exposure to provoking agents.
Brown and Harris 1978
strengths
limits
strengths
The sample size of the original study was relatively large, making
The study used semi-structured interviews to get an in-depth understanding of the participants' situation as they see it
themselves. This increased the credibility of the results.
limits
self reported symptoms, not able to determine accuracy
Because there is no manipulation of an independent variable, the findings cannot determine cause and effect.
it is possible that biological vulnerability may also play a role in this study
only females were interviewed so the results may not apply to men
prevalence study 2
Nolen-Hoeksama (2000)
Nolen-Hoeksama (2000)
bg info
aim
sample
method
procedure
BG INFO: One theory is that rumination - that is, the focused attention on the symptoms of one's distress.
This is the basis of Nolen-Hoeksema's Response Styles Theory.
There are two components to rumination. First, the individual focuses on the symptoms of distress. Often they will say, " I just can’t concentrate."
They also worry about the meaning of their distress, thinking, "Will I ever get better? Am I a bad parent?"
Rumination contributes to feelings of hopelessness about the future and a negative evaluations of one's self.
Ruminators vacillate between anxiety and depression - uncertainty and hopelessness.
Rumination may prolong negative thinking associated with depressed mood, interfere with good problem solving, and cause friction with friends and family.
AIM: to carry out a prospective study of the role of rumination on symptoms related to depression.
SAMPLE: 1132 adult participants randomly selected from a community sample in the San Francisco area, including San Jose and Oakland by random-digit dialing
METHOD: interviewed two times over a period of one year. + questionnaire
PROCEDURE: All participants interviewed in person in their own homes. The interview consisted of a clinical interview which lasted for 90 minutes.
This included a battery of tests which included the Beck Depression Inventory, the Hamilton Rating Scale for depression, the SCID, and the Beck Anxiety Inventory.
Finally, they were given a rumination and coping questionnaire, designed by the researchers.
asked to rate how often they think, “Why do I react this way”, “I think about how sad I am”, or “I think that I will lose my job if I don’t get better.”
Nolen-Hoeksama (2000)
results
connection
results
Participants who showed signs of Major Depressive Disorder at the time of the first interview had a significantly higher score on ruminative responses than those who did not show signs of MDD.
Participants who had never been depressed had significantly lower rumination scores than the other participants.
In addition, those who had been depressed but improved had lower rumination scores than those who remained chronically depressed.
connection
clearly, there is a connection between those who have experienced depression having higher rumination scores, showing that rumination is a predicting factor of depression, showing that depression is more prevalent in those who ruminant
Nolen-Hoeksama (2000)
strengths
limits
strengths
The research supports Beck's theory that patterns of cognition can have a negative effect on mental health.
The Response Styles Theory is supported by biological evidence - such as Farb (2011)
method triangulation: The study relied on self-report questionnaires as well as diagnosis through clinical interviews.
limits
it was self reported, but they later had clinical interviews
Originally there were 1317 participants. Although there was a small attrition rate, it was those with the strongest symptoms that dropped out which means that there may have been a bias introduced into the study
No information was available on whether the participants living with depression were receiving treatment or how other protective factors may help them to cope with their disorder.
The results may have been influenced by uncontrolled confounding variables.
sociocultural approach terms
The Vulnerability model identifies the predictors of depression.
Protective factors: protect against the development of depression when experiencing stressors.
High levels of closeness with one's husband.
Socioeconomic status.
Meeting of basic needs.
These factors lead to higher levels of self-esteem and the possibility of finding other sources of meaning in life.
Provoking Agents: found to contribute to acute (recent) and ongoing stress.
These stressors could result in grief and hopelessness in vulnerable women with no social support.
Divorce, Loss of job, Loss of loved one.
Vulnerability factors:Long term factors found to increase the risk of depression in combination with provoking agents.
The most significant vulnerability factors were
Loss of one's mother before the age of 11
lack of a confiding relationships
more than three children under the age of 14 at home
persistent unemployment.
Adverse Childhood Experiences study which found:
Negative experiences and stressors in childhood can have long-term effects on health - both mental and physical, as well as on cognitive and social development.
abuse, neglect, and household dysfunction
socul study 1
Brown and Harris 1978
Brown & Harris 1978
bg info
aim
sample
method
procedure
BG INFO: The Vulnerability model identifies the predictors of depression.
Protective factors: protect against the development of depression when experiencing stressors.
High levels of closeness with one's husband.
Socioeconomic status.
Meeting of basic needs.
These factors lead to higher levels of self-esteem and the possibility of finding other sources of meaning in life.
Provoking Agents: found to contribute to acute (recent) and ongoing stress.
These stressors could result in grief and hopelessness in vulnerable women with no social support.
Divorce, Loss of job, Loss of loved one.
Vulnerability factors:Long term factors found to increase the risk of depression in combination with provoking agents.
The most significant vulnerability factors were
Loss of one's mother before the age of 11
lack of a confiding relationships
more than three children under the age of 14 at home
persistent unemployment.
AIM: carried out a case study to determine the role of environmental factors in the onset of depression in women
SAMPLE: 498 women were surveyed on their daily life and depressive symptoms using a structured interview process.
The researchers focused on important biographical details - particular life events or particular difficulties faced by the women.
These events were later rated in severity by independent researchers.
METHOD: survey
The researchers identified three major factors that affected the development of depression.
Protective factors found to protect against the development of depression in spite of stressors, e.g. high levels of intimacy with one's husband. These factors lead to higher levels of self-esteem and the possibility of finding other sources of meaning in life.
Vulnerability factors found to increase the risk of depression in combination with particularly stressful life events - called provoking agents in the study. The most significant vulnerability factors were (1) Loss of one's mother before the age of 11, (2) lack of a confiding relationship, (3) more than three children under the age of 14 at home, and (4) unemployment.
Provoking agents found to contribute to acute and ongoing stress. These stressors could result in grief and hopelessness in vulnerable women with no social support.
brown and harries 1978
resuslts
connection
8% of all the women - that is, 37 in total - had become clinically depressed in the previous year.
33 of these women (nearly 90%) had experienced an adverse life event (e.g. loss of a loved one) or a serious difficulty (e.g. being in an abusive relationship).
Only 30% of the women who did not become depressed suffered from such adversity.
Only 4 of the 37 women who became depressed had not experienced any adversity.
The study showed that social factors in the form of life stress (or serious life events) could be linked to depression.
The fact that working-class mothers were more likely to develop depression than middle-class mothers showed risk factors associated with social class.
According to Brown and Harris, low social status leads to increased exposure to vulnerability factors and provoking agents, whereas high social status was associated with increased exposure to protective factors and decreased exposure to provoking agents.
so like social status affects your depression and the life experiences
brown and Harris 1978
strengths
limits
strengths
The sample size of the original study was relatively large, making
The study used semi-structured interviews to get an in-depth understanding of the participants' situation as they see it
themselves. This increased the credibility of the results.
limits
self reported symptoms, not able to determine accuracy
Because there is no manipulation of an independent variable, the findings cannot determine cause and effect.
it is possible that biological vulnerability may also play a role in this study
only females were interviewed so the results may not apply to men
socul study 2
felitti et al (1988)
felitti et al (1988)
bg info
aim
sample
method
procedure
AIM: The goal of the study was to determine if there was a correlation been negative childhood experiences and adult physical and mental health.
SAMPLE: The sample consisted of 8506 participants - mean age of 56.1 years - with a range of 19 - 92 years old. 43% had graduated with a university degree - and 52.1% were women.
METHOD: correlational study.
PROCEDURE: A questionnaire was sent to people who had completed a standardized medical evaluation at the Kaiser Permanente clinic in San Diego.
it assessed the following 7 ACE factors:
physical, psychological, or sexual abuse.
domestic violence against the mother.
living with a caregiver that was suicidal, a substance abuser, or had been imprisoned.
These seven ACEs were correlated with the health status determined in the clinical evaluation.
Felitti et al (1988)
results
connection
The researchers found that the prevalence and risk increased for smoking, severe obesity, physical inactivity, depression, alcoholism, use of illicit drugs, promiscuity, and suicide attempts as the number of ACEs increased.
researchers also found a strong relationship between the number of childhood experiences and health risk factors.
Persons who had experienced four or more categories of ACE, compared to those who had experienced none, had a 12-fold increased health risk for alcoholism, drug abuse, depression, and suicide.
a 2 to 4-fold increase in smoking, sexually transmitted diseases;
and a 1.4 to 1.6 fold increase in physical inactivity and severe obesity.
Adverse childhood experiences have a dose-response relationship with many health problems.
that there was a strong correlation between the number of ACEs and ischemic heart disease, cancer, chronic bronchitis and hepatitis (linked to sexual and drug behaviours).
experiecnces obciously have an effect on your mdd chances as ACEs increased likelihod of depression
Felitti et al (1988)
strengths
limits
strengths
had a large sample size and
sparked a lot of research that has confirmed and developed the original findings.
limits
It is unclear how the different ACEs interact and contribute to the onset of health problems.
It is also not clear whether it is the presence of an ACE in childhood or the intensity, frequency, or nature of the ACE that impacts adult health.
As no extraneous variables were controlled for, more research is needed.
The study did not focus on the mechanisms that may lead to health issues - for example, cortisol levels were not measured
The data was self-reported and retrospective. However, the rates of abuse were in line with other studies of similar populations
The study is cross-sectional. We do not see changes in health over time.
There is a low number of older participants; it is possible that the elderly participants had simply outlived other older participants who had health issues, making this part of the sample unrepresentative.
cognitive terms
he American psychiatrist Aaron Beck is seen as the founder of cognitive therapy.
He argues that depression is rooted in what he called a patient's "automatic thoughts"- that is, negative self-schemas organized around themes of failure, inadequacy, loss, and worthlessness.
All these personalized thoughts are triggered by particular stimuli that lead to emotional responses that increases the likelihood of depression.
Beck’s theory has 3 components; The Cognitive Triad, Negative Schemas, and Errors in Logic
The Cognitive Triad:
Negative Views of the World: This thinking can generalize the world as a bad place.
It is personalized to thoughts such as “no one in the world likes me”
Negative Views of the self:
Ineptness schema - belief that you are not good at something “I always fail…”
Self Blame Schema - belief that you are to blame for negative events. “Everything is my fault…”
Negative self evaluation “I am worthless”
3. Negative Views of the Future: The belief that nothing will get better; The future is hopeless.
Errors in Logic (irrational thinking)
Many of these self schemas are due to errors; The thinking is irrational
They use absolutes like “always, never”
Use individual events to create a negative identity.
5 types:
Selective abstraction: Drawing a conclusion about yourself based on one incident, ignoring the bigger picture.
Depressed patients look at negative moments and ignore positive.
Magnification: Overthinking the importance of an undesirable event and blowing it out of proportion.
Minimization: Not acknowledging when you do something well or seeing praise for you work as simply flattery and meaningless.
Overgeneralization: When you draw broad conclusions based on a single event and apply it to other areas of your life.
Personalization: Attributing the moods or negative feelings of others to yourself
Arbitrary Inference: Making conclusions without relevant evidence, and this way of thinking tends to focus on the most negative possible outcome.
negative schemas
Ineptness schema - I always fail
Self-blame schema - It is my fault for anything that doesn't work out.
Negative self-evaluation schema - I am worthless.
study 1 cog
alloy et al (1999)
alloy et al (1999)
bg info
aim
sample
method
procedure
BG INFO: The cognitive vulnerability hypothesis argues that there are maladaptive thinking patterns that make a person more likely to develop a mental illness.
Aaron Beck hypothesized that a pattern of negative schemas about oneself, others, and the future play a key role in Major Depressive Disorder.
These negative thoughts about oneself are seen as stable and global - that is, that they are not likely to change and they affect all areas of one's life.
AIM: difficult to resolve bidirectional ambiguity so it is not clear whether negative cognition leads to depression or whether depression leads to negative patterns of thinking. Alloy et al were hoping to resolve this
SAMPLE: used a sample of non-depressed college freshmen with no other diagnosed disorders. Half of the sample had a history of clinical depression; the other half did not. The students with a history of clinical depression demonstrated no symptoms at the beginning of the study.
METHOD: test
PROCEDURE: to begin, the students were given a test to measure their cognitive style.
The students were identified as either High Risk (HR) or Low Risk (LR) for depression based on their thinking patterns.
The researchers carried out follow-up assessments every 6 weeks for 2.5 years and then every 4 months for an additional three years.
The study was based on a combination of questionnaires and structured interviews to identify stressful life events, cognitive style, and symptoms of depression.
Participants also took a test in which they listened to a list of adjectives.
For each adjective, they were asked whether they thought that the word described them.
At the end of the list, they were asked to recall as many words as possible from the list.
alloy et al (1999)
results
connection
The results found that in the group with no prior history of depression, 17% of the HR students developed Major Depressive disorder, compared to only 1% of the LR students.
In addition, 29% of the HR group showed symptoms of minor depression, compared to only 6% of the LR group.
Among the group with a past history of depression, 27% of the HR group relapsed, whereas only 6% of the LR group did.
In addition, 50% of the HR group showed symptoms associated with depression, compared to 26.5% of the LR
In addition, the rate of suicidality was higher in the HR groups (28%) compared to the LR groups (12.6%).
The researchers found that the HR groups showed faster processing and better recall of negative information; and slower processing and worse recall on positive information
It appears that negative cognitive style played a role in both onset and relapse.
alloy et al (1999)
strengths
limits
strengths
The study used method and data triangulation, increasing the credibility of the findings.
The tests used to measure cognitive style are highly standardized and have a high level of reliability.
The use of a pre-test, / post-test design helps to diminish the bidirectional ambiguity.
The theory of cognitive vulnerability has been applied in therapy (CBT) and has been shown to be effective.
limits
However, the study is a natural experiment - that is, the researcher does not manipulate the independent variable. This means that it is not possible to establish a cause and effect relationships.
no control of confounding variables (outside help/ experiences that may have slowed down/ sped up the chances/ development of depression)
The link between cognitive style and depression may be more complex than the study actually proposes. See the second above about domino causality.
cog study 2
Nolen-Hoeksama (2000)
Nolen-Hoeksama (2000)
bg info
aim
sample
method
procedure
BG INFO: One theory is that rumination - that is, the focused attention on the symptoms of one's distress.
This is the basis of Nolen-Hoeksema's Response Styles Theory.
There are two components to rumination. First, the individual focuses on the symptoms of distress. Often they will say, " I just can’t concentrate."
They also worry about the meaning of their distress, thinking, "Will I ever get better? Am I a bad parent?"
Rumination contributes to feelings of hopelessness about the future and a negative evaluations of one's self.
Ruminators vacillate between anxiety and depression - uncertainty and hopelessness.
Rumination may prolong negative thinking associated with depressed mood, interfere with good problem solving, and cause friction with friends and family.
AIM: to carry out a prospective study of the role of rumination on symptoms related to depression.
SAMPLE: 1132 adult participants randomly selected from a community sample in the San Francisco area, including San Jose and Oakland by random-digit dialing
METHOD: interviewed two times over a period of one year. + questionnaire
PROCEDURE: All participants interviewed in person in their own homes. The interview consisted of a clinical interview which lasted for 90 minutes.
This included a battery of tests which included the Beck Depression Inventory, the Hamilton Rating Scale for depression, the SCID, and the Beck Anxiety Inventory.
Finally, they were given a rumination and coping questionnaire, designed by the researchers.
asked to rate how often they think, “Why do I react this way”, “I think about how sad I am”, or “I think that I will lose my job if I don’t get better.”
Nolen-Hoeksama (2000)
results
connection
results
Participants who showed signs of Major Depressive Disorder at the time of the first interview had a significantly higher score on ruminative responses than those who did not show signs of MDD.
Participants who had never been depressed had significantly lower rumination scores than the other participants.
In addition, those who had been depressed but improved had lower rumination scores than those who remained chronically depressed.
connection
clearly, there is a connection between those who have experienced depression having higher rumination scores, showing that rumination is a predicting factor of depression, showing that depression is more prevalent in those who ruminant
cognitive patterns obviously effect development of MDD
Nolen-Hoeksama (2000)
strengths
limits
strengths
The research supports Beck's theory that patterns of cognition can have a negative effect on mental health.
The Response Styles Theory is supported by biological evidence - such as Farb (2011)
method triangulation: The study relied on self-report questionnaires as well as diagnosis through clinical interviews.
limits
it was self reported, but they later had clinical interviews
Originally there were 1317 participants. Although there was a small attrition rate, it was those with the strongest symptoms that dropped out which means that there may have been a bias introduced into the study
No information was available on whether the participants living with depression were receiving treatment or how other protective factors may help them to cope with their disorder.
The results may have been influenced by uncontrolled confounding variables.
bio terms
Genetic heritability of traits such as depression cannot be measured directly but must be studied through
Method | Explanation |
Twin Studies | MZ twins share 100% of their genotype and DZ twins share about 50%. So, MZ twins should have similar behavior compared to DZ. |
Adoption studies | Useful to study the effect of change in environment on children. Can compare similarities and differences of adoptive children with their adoptive parents, biological parents, biological siblings, and other siblings |
Family Studies | Based on family data for several generations and data of relatives compared based on how closely they are related |
Epigenetics/Molecular genetics | Uses genetic mapping (gene -> protein/trait) to investigate how specific genes influence behaviour |
Falconer Model
Used to estimate heritability in twin studies
Phenotype is based on a combination of A (hereditary genes), C ( shared environment), and E (individual environment)
A+C+E=1
Diathesis-stress theories of depression predict that an individual's reaction to stressful events depends on their genetic make-up.
If an individual has a specific genetic predisposition toward a disorder (genotype), then interaction with stressors in the environment may cause these genes to be expressed.
bio study 1
Kendler et al (2006)
Kendler et al (2006)
bg info
aim
sample
method
procedure
BG INFO:
AIM: Kendler and his team wanted to investigate three questions in their study:
Past studies suggest a 35 - 45% heritability of major depression.
Would this be true in a large Swedish sample?
Are there significant gender differences in the heritability of major depression?
Is there evidence that genetic and environmental factors in major depression differ over time?
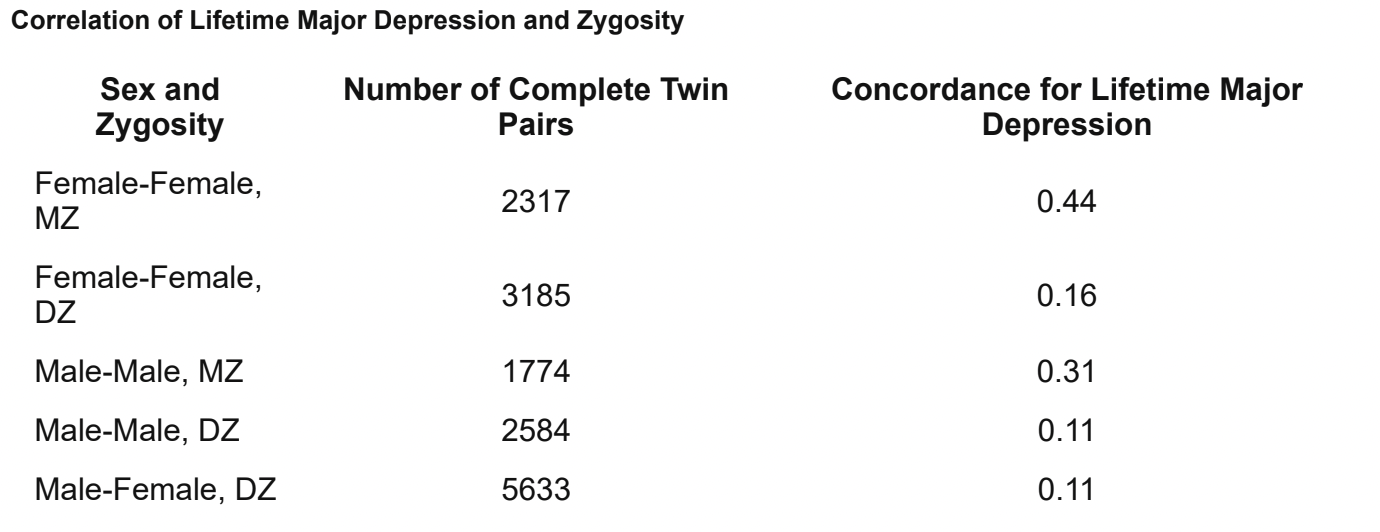
SAMPLE: The sample was made up of 15,493 complete twin pairs listed in the national Swedish Twin Registry. Only twins whose zygosity could be verified were used in the study.
METHOD: interviews
PROCEDURE: used a team of trained interviewers to carry out telephone interviews.
Interviews were carried out between March 1998 and January 2003.
The interviewers assessed lifetime major depression by using modified DSM-IV criteria.
criteria. 8056 twins met the criteria for a diagnosis of major depression at some point in their life - and 322 twins voluntarily discussed a history of antidepressant treatment.
the interviewers also asked questions about the twins "shared environment" - that is, when they were living in the same household - and their "individual-specific environment" - that is, adult personal life events that may make members of the twin pair more susceptible to depression.
Kendler et al (2006)
results
connection
The results indicate that the concordance rates for major depression were significantly higher in women than men.
the correlations were significantly higher in monozygotic than in dizygotic twins.
They also found no correlation between the number of years that the twins had lived together and lifetime major depression.
The estimated heritability of major depression was 0.38, in line with previous research.
There were also no significant differences seen in the roles of genetic and environmental factors in major depression in the three cohorts spanning birth years 1900-1958.
Even when they split the entire cohort into pre and post World War II, there was no significant difference.
This study suggests both that the heritability of major depression is higher in women than in men and that some genetic risk factors for major depression are sex-specific.
In addition, the study confirms the level of heritability of major depression found in other studies, strengthening the reliability of European twin studies.
genes play a role in depression as people with the same genes are predisposed to the same disorder
kendler et al (2006)
strengths
limits
strengths
The study appears to confirm previous research, strengthening the reliability of the findings.
The very large sample size taken from a single population helps to mediate some of the concerns below.
limits
we don’t know that the depression occurring in both twins is due to genes, but it could also be the shared experiences or upbringing
The study is correlational, so no cause and effect relationship can be determined. No particular genes were isolated and tested in the study.
Information about life-events and depressive symptoms was self-reported. men could’ve been less reliable than women to abide to societal expectations of being “strong”
The interviewers did not officially diagnose the twins and they accepted the diagnoses made by clinicians when it was reported by the interviewee;
as we know, clinical diagnoses are not highly reliable and making such a diagnosis by telephone may be considered of questionable validity.
bio study 2
Caspi et al (2003)
Caspi et al (2003)
aim
sample
method
procedure
AIM: to determine whether there is evidence for a gene-environment interaction (G x E) for a mutation of the serotonin transporter gene - 5-HTT.
The serotonin transporter is involved in the reuptake of serotonin in brain synapses.
SAMPLE: 847 New Zealand 26-year-olds.
a cohort that had been assessed for mental health on an every-other-year basis until they were 21.
They were divided into three groups based on their 5-HTT alleles:
Group 1 had two short alleles;
Group 2 had one short and one long allele;
Group 3 had two long alleles.
The mutation of the 5-HTT gene has the shorter alleles. Roughly 43% of people have the shorter alleles.
METHOD: questionnaire
PROCEDURE: The participants were asked to fill in a "Stressful life events" questionnaire which asked them about the frequency of 14 different events - including financial, employment, health, and relationship stressors - between the ages of 21 and 26.
They were also assessed for depression.
caspi et al (2003)
results
connections
People who had inherited one or more short versions of the allele demonstrated more symptoms of depression and suicidal ideation in response to stressful life events.
The effect was strongest for those with three or more stressful life events. Simply inheriting the gene was not enough to lead to depression, but the genes' interaction with stressful life events increased one's likelihood of developing depression.
In a later study by Wilhelm et al (2006), the researchers looked at DNA samples from 127 people who are part of a longitudinal prospective study looking at mental health.
The sample had been monitored for over 25 years. At five-year intervals, scientists recorded any major life events and signs of depression.
They found that 80 percent of those with two short 5-HTT genes became depressed after three or more negative life events in a year, whereas those with two long genes appeared resilient - only 30 percent developed the illness in similar situations.
They also found that childhood maltreatment predicted adult depression only among individuals carrying a short allele and not among those carrying the longer allele.
However, much more research is needed before a clear relationship between a gene and a depression can be
established.
Caspi et al (2003)
strengths and limits
strengths
most of sample comes from same place, so genes can be expected to act similarly
limits
The study is correlational, so no cause and effect relationship can be determined.
The study makes the assumption that serotonin causes depression.
Information about life-events was self-reported. It may be the salience of the negative life events which plays a role in depression - that is, those that recalled them more easily may have a tendency towards depression. Those who are more resilient, may not recall negative life events as easily.
Later studies have not been able to show similar results; low reliability.
There were some participants who did not carry the gene mutation who became depressed; therefore, we cannot say that gene expression alone can cause depression.
ethics?
caspi et al (2003)
they couldn’t consent when they were children
might’ve felt obligated or pressured becasue they’ve been doing it all their lies and they didn’t want to mess up the study
might’ve even contributed to some stress that lead to MDD??
noel-hoeksama (2000)
unfair to bring up these questions to peopel that were already vulnerable
may cause undue stress or harm to think about it
may introduce new insecurities or things to ruminate over
research
idk just reuse the last one?
questionnaire vs longitudinal studiesquestionnaire vs interview!!!!!!