Antibiotic Agents Part 1&2
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
82 Terms
What are the most pervasive bacteria in ocular flora?
Staphylococcus aureus (most common trouble maker)
Staphylococcus epidermidis
Streptococcus pneumonia
All are gram positive bacteria
What are other bacterial species that affect the eye?
Haemophilus influenzae
Large component in peds
Pseudomonas aeruginosa
Common for CL
Chlamydia trachomatis
STD
Neisseria gonorrhoeae
STD
Can penetrate intact cornea
Treponema pallidum
All are gram negative
What are the common targets for antibiotic therapies?
Attack bacteria cell wall
Attack bacteria cell membrane
Attack Folic Acid synthesis (humans must get folic acid from food & environment, bacteria synthesize it themselves)
How do bacteria develop antibiotic/microbial resistance?
Produce an enzyme that deactivates antibiotics
Alter surface cell receptor to reduce or inhibit antibiotic binding to its surface
Block entry of antibiotic into cellular contents
Actively transport Ab out of cell
More/etc.
What prescribing patterns increase risk for developing antibiotic resistance?
Antibiotic is not dosed properly (sublethal dosing)
Rx below minimum inhibitory concentration (MIC)
Shortened course of therapy
Intermittent use of antibiotic
Tapered dosing
Bacteriostatic drugs were used vs bactericidal drugs
Bacteriostatic doesn’t kill bacteria, giving more opportunities to develop resistance
Overuse of antibiotics
Specifically overuse of systemic antibiotics
What are the indications for topical ophthalmic antibiotics?
Active infection: bacterial conjunctivitis, microbial keratitis
Eyelid/surface disease: anterior blepharitis, MGD, or other surface lid disease with bacterial involvement
Prophylaxis: pre‑ or post‑ocular surgery or when the epithelial barrier is disrupted (e.g., corneal abrasion, contact lens–related epithelial defects)
What are the indications for oral (systemic) antibiotics in ophthalmology?
Glandular or deep lid disease: dacryocystitis, preseptal cellulitis, severe blepharitis not responsive to topicals
Ocular manifestations of systemic disease: chlamydial conjunctivitis, gonococcal infection
How do cell wall inhibitors work and what are some examples?
Inhibit transpeptidation of peptidoglycans in cell wall formation.
Are 1 of 2 groups:
Beta-lactam ring subgroups
Non Beta-lactam ring subgroup
What are examples of Beta-lactam ring subgroup cell wall inhibitors?
Penecillins
Cephalosporins
Carbapenems (injection only)
Aztreonam (injection only)
What are examples of Non Beta-lactam ring subgroup cell wall inhibitors?
Bacitracin (only topical ophthalmic agent of all cell wall inhibitors)
Vancomycin (IV only)
What are the 2 main beta-lactam classes of meds relevant to eyecare?
Penicillins and cephalosporins
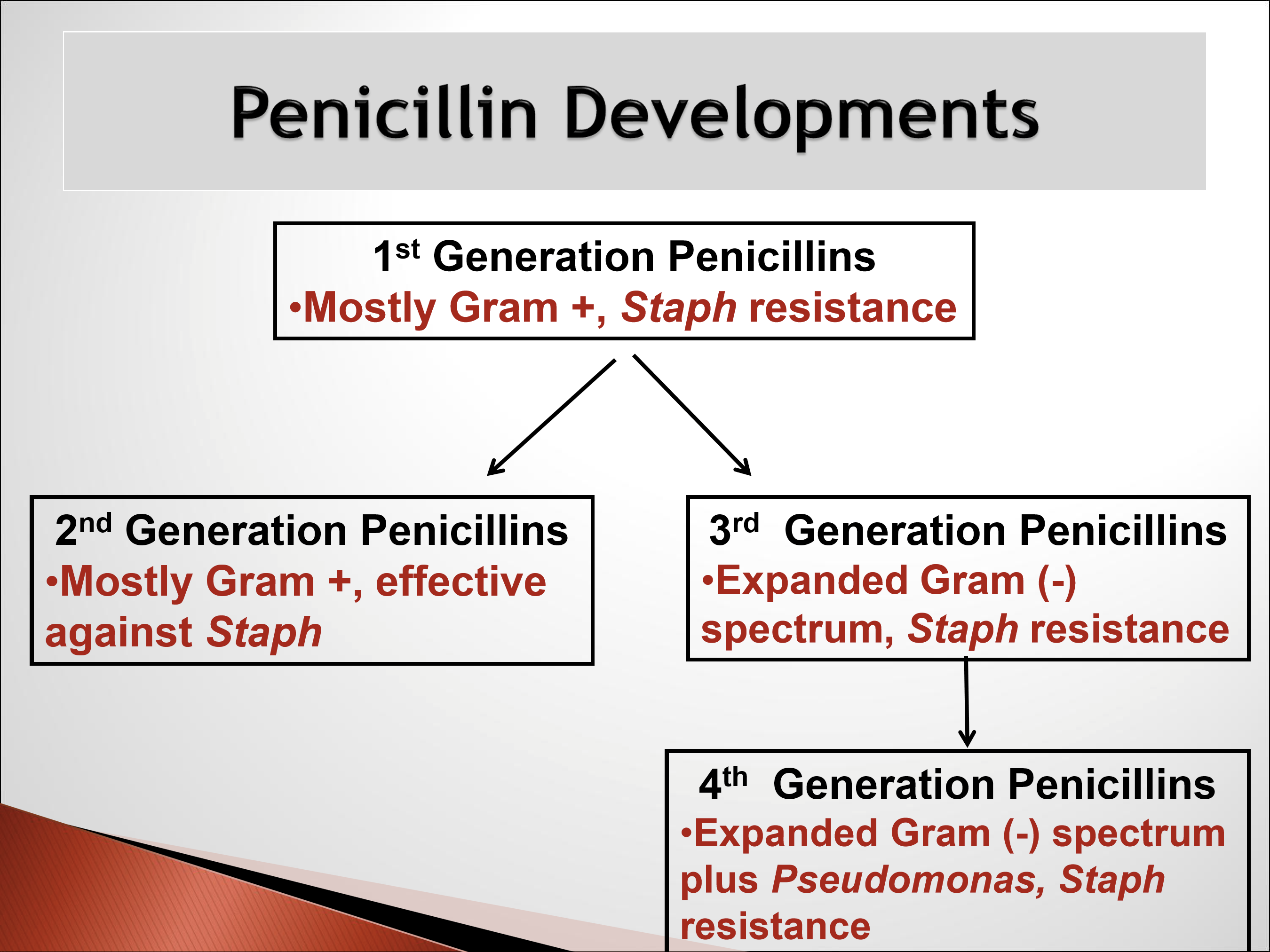
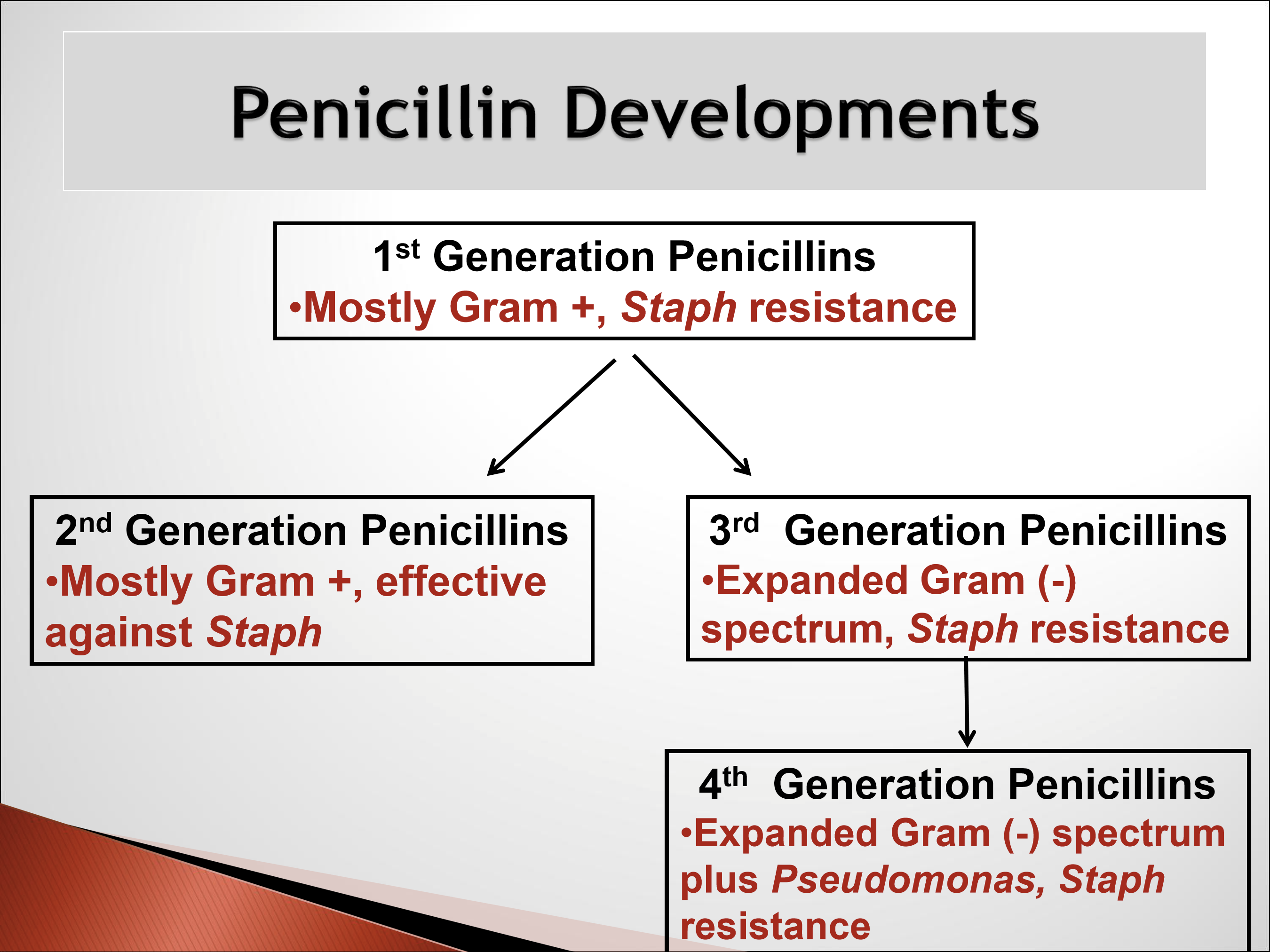
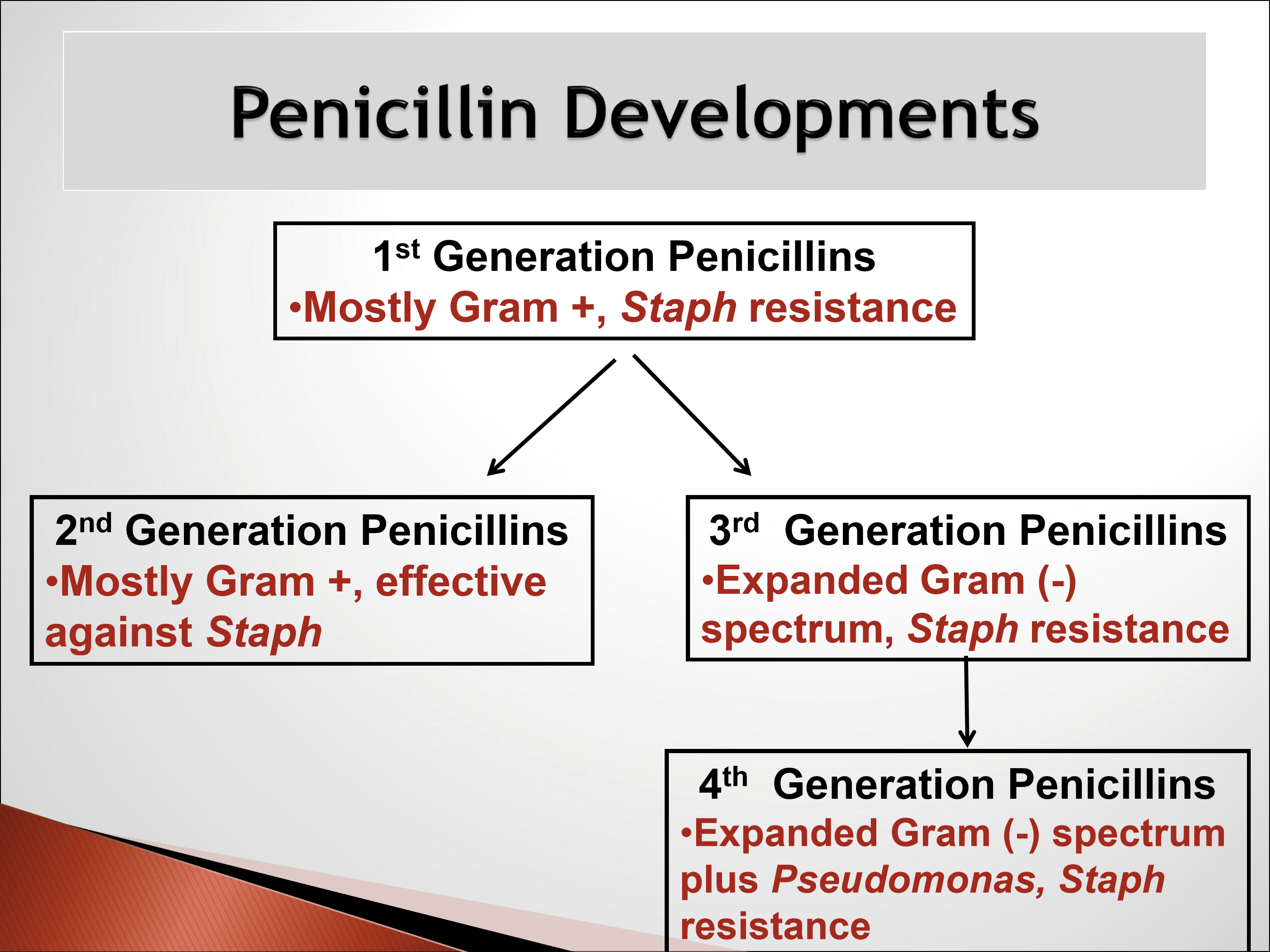
What are the general characteristics of the different penicillin drug class generations?
1st gen: effective against gram +
2nd gen: protected against Beta lactamase
3rd gen: Extended spectrum to include gram -
4th gen: Now with antipseudomonal activity
What is the specturm of activity for 1st gen penicillins?
Originally good for gram +, including treponema pallidum. Now 90% of staph are resistant.
What is 1st gen penicillin still used for?
DOC for ocular manifestations of systemic syphilis infection
What is the spectrum of activity for 2nd gen penicillins?
Good gram + and scant gram -. Maintain effectivity against staph aureus bc protected against beta-lactamase.
What are some examples of 2nd gen penicillins?
Methicillin
Oxacillin
Nafcillin
Dicloxacillin *preferred bc has best absorption and penetration
All are oral and generics
What is the ocular indication for 2nd gen penicillins?
Hordeola, but is not the DOC/first prescribed.

What is the spectrum of activity of 3rd gen penicillins?
Gram -, including haemophilus influenzae; not good gram + d/t staph resistance. Not protected against beta-lactamase.
What are examples of 3rd gen penicillins?
Ampicillin
Amoxicillin
Augmentin: amoxicillin and clavulanate (clavulanic acid)
DOC for infectious lid disease
Also available in generic formulations
Why would clavulanate be added to amoxicillin?
Clavulanic acid is an enzyme that inhibits beta-lactamase.
What is the typical dosing of Augmentin for an adult?
500-875 mg PO BIDx 10 days
What are the ocular indications of Augmentin?
It is the DOC for:
Hordeola
Preseptal cellulitis
Dacryocystitis: an infection or inflammation of the lacrimal (tear) sac
Useful for both adults and peds patients due to coverage against Staph and H. Flu
What is the pediatric dosing of Augmentin?
Age >3 months: 25mg/kg/day in 2 divided doses
What is the specturm of activity for 4th gen penicillins?
AKA penicillins with antipseudomonal activity
Gram - including:
Haemophilus influenzae
Pseudomonas aeruginosa
Proteus
Little gram + coverage d/t staph resistance
Resistance from beta-lactamase
What are some examples of 4th gen penicillins?
Ticarcillin: only available in combo with clavulanate
Pepercillin
Both are IV only
What are the ocular indications for 4th gen penicillins?
Can be used topically for pseudomonas corneal ulcers that fail to respond to initial treatment, however, must be specifically formulated into ophthalmic solution by pharmacy since IV only.
What is the general characteristics of cephalosporin drugs?
All 5 gen are systemic meds. No topical ocular formulations.
What is the MOA for cephalosporin?
Inhibit transpeptidation of peptidoglycans, a crucial component in bacterial cell wall.
Why are cephalosporin still effective against Staph?
Big and bulky molecule, so naturally protected from beta-lactamase.
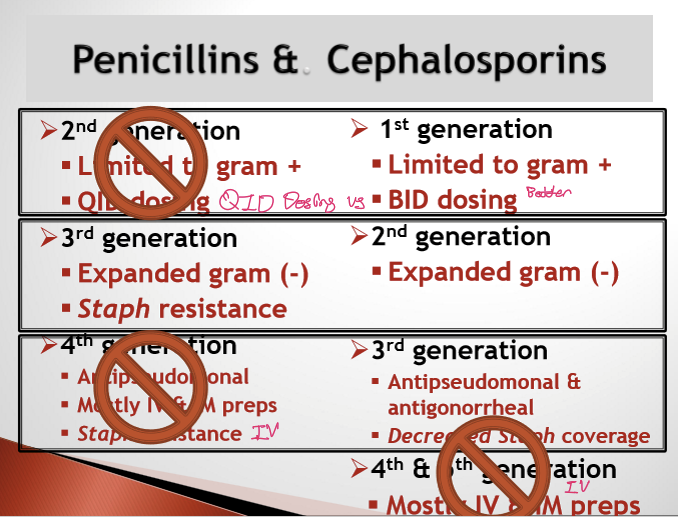
What is the general trend for the spectrum of activityfor cephalosporins as generation increases?
Increase gram negative coverage
Decrease gram positive coverage
What is the spectrum of activity for 1st gen cephalosporin?
Mostly limited to Gram+, maintains effectiveness against Staph Aureus.
What is the spectrum of activity for 2nd gen cephalosporin?
Has broader Gram- coverage, including H. Flu.
What is the spectrum of activity for 3rd gen cephalosporin?
Little gram +, great gram -, including H. flu, Pseudomonas, & Neisseria
What is the spectrum of activity for 4th and 5th gen cephalosporin?
Some activity against MRSA, mostly IV, and IM routes.
What penicillins and cephalosporins are used by optometrists?
1st gen cephalosporin: cephalexin (Keflex) 500mg BIDx 10d
2nd gen cephalosporin: cefprozil 500mg BIDx 10d
3rd gen cephalosporin: cefdinir 300mg BIDx 10d
3rd gen penicillins: Amoxicillin w/clavulanate (Augmentin): 875mg BIDx 10d OR 500mg TIDx 10d
What are the signs of an internal hordeolum?
Redness
Pain
Warm to touch
Painful to touch
Soft in texture: filled w/ puss
Isolated

What is the difference between Chalazion vs Internal Hordeolum?
Chalazions have no active infection, no pain, less acute, firm in texture, not warm/hot to the touch
What drugs can be used to treat an Internal Hordeolum?
Cephalexin 500mg BIDx 10d (1st gen Ceph)
Cefprozil 500mg BIDx 10d (2nd gen Ceph)
Augmentin 875mg BIDx 10d OR 500mg TIDx 10d (3rd gen PNC)
Why are 3rd gen Ceph not used?
Not particularly good aginst staph.
What is Preseptal Cellulitis? What are its signs?
Active infection of diffuse tissue in-front of orbital septum
Signs:
Warm
Tender
Painful to touch

What are the possible etiologies for preseptal cellulitis?
Trauma/laceration to skin of eyelid
Spread of localized lid infection
Spread of ethmoid sinus infections
What are the likely offending organisms for preseptal cellulitis?
Staph aureus
Staph epidermidis
Strep
H. Flu

What drugs are used to Tx Preseptal Cellulitis?
Cefprozil 500mg BID (2nd gen ceph)
Augmentin 875mg BIDx 10d OR 500mg TIDx 10d (3rd gen PNC)
Why is 1st gen and 3rd gen ceph not used for preseptal cellulitis?
1st gen: The infection is not self contained, so it has a greater risk of spreading, so need greater gram - coverage.
3rd gen: No coverage for Staph
What are the signs of orbital cellulitis?
Fever
Feels ill
Proptosis/globe displacement

What is Dacryocystitis? What are its signs?
Acute infection of lacrimal sac
Signs:
Painful
Redness
Tenderness over lacrimal sac
Purulent reflux
Epiphora

What is the treatment for Dacryocystitis?
Cefprozil 500mg BIDx 10d
Augmentin 875mg BIDx 10d OR 500mg TIDx 10d
Is Bacitracin prescribed by itself?
No, it is only availabe in combination with other antibiotics.
What is the Vancomycin MOA?
Inhibits peptidoglycan syntehsis by binding dialanine, preventing cell wall cross-linking.
What is the spectrum of activity of Vancomycin?
Excellent Gram + coverage, including MRSA and C.Diff
Much less risk of resistance than PCN and Ceph to Staph and Strep species
IV formulation
What are the SE of Vancomycin?
High risk of ototoxicity and nephrotoxicity
What are the contraindications for Vancomycin?
Known Hypersensitivity
What are the indications for Vancomycin?
Systemic Indications:
DOC for pseudomembranous colitis from clostridium difficile (Gram+)
DOC for systemic MRSA infections
Ocular indications:
IV meds is specially formulated for intravitreal injection to cover gram + bugs in case of bacterial endophthalmitis
What is the mechanism of action of bacitracin?
Inhibits bactoprenol, a lipid carrier that transports peptidoglycan subunits → blocks bacterial cell wall synthesis.
What is the antimicrobial spectrum and clinical use of bacitracin?
Gram‑positive organisms only.
Used topically (dermatologic and ophthalmic) due to nephrotoxicity.
What are the formulations and adverse effects of bacitracin?
Dermatologic: OTC, ointment only
Ophthalmic: Ointment only, Rx, usually combined with other antibiotics ± steroid
Adverse effect: Rare contact dermatitis
What are the effects of Cell membrane inhibitors on bacteria?
All are bactericidal
What is the MOA for cell membrane inhibitors?
Disrupts the osmotic integrity of the cell membrane, resulting the cell lysis.
What are some cell membrane inhibitor drugs?
Gramicidin
Polymyxin B
What are the key characteristics and formulations of gramicidin?
Topical only
Same general role as bacitracin, but is a solution (not ointment)
Not available as a stand‑alone drug
Used only in combination with other antibiotics ± steroids
What is the spectrum of activity for Polymyxin B?
Gram - including H. flu and Pseudomonas
What are the formulations for Polymyxin B?
Systemic formulations:
IV and IM only. No orals
Topical formulations:
Ophthalmic solution or ointment
What are the systemic SE of Polymyxin B?
Neurotoxic
Nephrotoxic
Used only in cases of meningitis
What are the contraindications for Polymyxin B?
Known hypersensitivity
What are the ocular indicationss for Polymyxin B?
Prophylaxis in the presence of corneal abrasion/large epi defect, especially in CL wearer
QHS dosing for bacterial corneal ulcer to supplement daytime treatment with a topical fluoroquinolone
Bacterial conjunctivits QID (rarely used)
Anterior blepharitis BID-QID (rarely used)

What is the first‑line treatment for anterior blepharitis?
Lid hygiene with soap‑based eyelid cleansers
What is the difference between OcuSoft original lid scrubs/foam cleanser and OcuSoft PLUS Lid scrubs/foam cleanser?
Plus contains soaps and disinfectants.
What are the
What is the second‑line treatment for anterior blepharitis?
Hypochlorous acid (HOCl)–containing products
Used when soap‑based lid scrubs are insufficient
Why are hypochlorous acid containing products effective in anterior blepharitis?
High antimicrobial kill rate
Effective against Staph aureus, Staph epidermidis, MRSA, and some Demodex
Why do Medicinal-based lid hygiene products not contain additives or preservatives?
To limit side effects.
What is Demodex blepharitis?
Lid margin inflammation caused by parasitic Demodex mites
Common in chronic or treatment‑resistant blepharitis
What are the two Demodex species involved in blepharitis, and where do they live?
Demodex folliculorum: inhabits hair/lash follicles
Demodex brevis: inhabits sebaceous and meibomian glands
How is Demodex blepharitis diagnosed?
Lash manipulation at the slit lamp to visualize mites
Epilate lashes and examine under light microscopy
When should Demodex blepharitis be suspected?
Chronic, recurrent blepharitis
Poor response to standard lid hygiene
Often associated with cylindrical dandruff at lash base

What is used to treat demodeex blepharitis and what is its MOA?
Xdemvy (0.25% lotilaner ophthalmic solution)
MOA: GABA chloride channel blocker causing paralysis to demodex mites. Is specific to invertebrates, so no harm to mammalian cells

How is Xdemvy dosed and how is it ordered?
1 gt BID OUx 6wks
10 ml Bottle thru BlinkRx Mail-order pharmacy

What are the SE of Xdemvy? Are there any contraindications?
10% sting on instillation. No contraindications.

What was previously used to treat demodex?
OTC commercial products with Tea Tree Oil

What are the indications for in‑office lid and lash exfoliation?
Chronic or severe blepharitis
Meibomian gland dysfunction (MGD)
Lid margin debridement
Demodex blepharitis
What devices are commonly used for in‑office lid and lash exfoliation?
BlephEx
ABMax
What device is used for at‑home lid and lash exfoliation?
NuLids
