Class 24: Therapies
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
50 Terms
Trephination
Evidence in Neolithic man, with spherical holes cut in ancient skulls, that healed
in Ancient Greece (Hippocrates) to release “humors” or bodily fluids related to head injury. Later epilepsy. By 15th century, for melancholy
Thomas Willis (famed 16th century neuroanatomist who coined the term “neurology” and named the striatum) advocated trephination for melancholy
Early “Therapies“ for Psychological Disorders
In 1897, general paresis was discovered to be a consequence of syphilis
General paresis caused by syphilis accounted for about 25% of psychiatric inpatients at the time
Syphilis discovery provided proof that psychological disorders could have medical causes paved the way for a biomedical approach to psychological disorders
Sigmund Freud’s “talking cure” around the same time because the first formal therapy for psychological disorders that drew attention to environmental and social factors in mental illness
Classical Psychoanalysis
Freud believed that emotionally charged memories and conflicts were repressed (pushed out of consciousness) i.e. “motivated forgetting”
Emotions around repressed memories were expressed in symptoms like aggression, anxiety, depression and in physical symptoms like “psychogenic pain”
The goal of psychoanalysis was to bring unconscious conflicts and emotions into consciousness where they could be dealt with rationally
Free association
A method in which the patient says anything that comes to mind, no matter how apparently trivial, embarrassing, or disagreeable
Resistance
A patient’s self-censorship or avoidance of certain topics
Transference
Interpreting how the patient acted toward the therapist, considered to be a re-enactment of significant relationships (Emotional re-education)
Slips of the tongue
Mis-speaking provided insight into true beliefs
Interpretation of dreams
Considered the content of dreams to be an expression of the unconscious that could be interpreted thru interpreting symbols which he thought of as the language of dreams
Psychodynamic approaches
Contemporary psychodynamic therapies have been modified from psychoanalysis
less frequent than Freud’s (daily) sessions and lasts months to a year, not years
Meet face-to-face, rather than our of sight while the patient reclined on a couch
Conscious thoughts receive as much consideration as unconscious conflicts
Includes focus on improving current responses to stressors to improve functioning and relieve symptoms
Psychodynamic approaches: interpersonal therapy (IPT)
Assumption is that mood is tied to relationship quality and life events
targets problems like life transitions, complicated grief, interpersonal disputes, and interpersonal deficits
Time limited (usually 12 - 16 weeks)
First weeks are spent collecting information, creating an “interpersonal inventory” of relationships, and choosing a focus for therapy
Subsequent sessions consider actions that could improve the situation
Identifying conflict in relationships
Role-playing difficult conversations
Identifying challenges related to life transitions and building social support networks to help
Patient works on solutions between sessions
Humanistic approaches
Focus on self-actualization, growth he present and the future
Assume shall humans are oriented toward growth, the search for meaning and self-actualization
Therapy focuses on the present and the future
Helps patients see themselves as agents in their lives, and take productive action and responsibility
regards psychoanalysis as too concerned with basic urged like sex and aggression, and too focused on the past
Motivational interviewing
A brief, client-centered therapy designed to address specific problematic behaviors such as alcohol or drug use
draws out the client’s goals, reduce ambivalence, and clarify gaps between how client says they want to live and how they are living
Used in Serious Mental Illness (e.g. schizophrenia), before beginning an intervention to help the person identify with the purpose and goals and autonomously choose to participate
Client-centered therapy (person -centered therapy)
The therapist’s genuineness, unconditional positive regard, and empathic understanding are crucial to therapeutic success (“Rogerian therapy”)
seeks to help clients accept themselves as they are without pretense or self-imposed limits
Behavioral Approaches
Exposure techniques
systematic desensitization
In vivo exposure
Exposure and response prevention
Exposure techniques
Remove the anxiety connected to a feared stimulus through repeated approach toward the feared stimulus
Systematic desensitization
Gradually increasing encounters with the feared stimulus with periods of relaxation between
In vivo exposure
Patient is exposed to the phobic stimulus in the real world or through interactive computer programs (VR)
Exposure and Response Prevention
Behavioral treatment of OCD where the patient delays performing the compulsion to relive anxiety
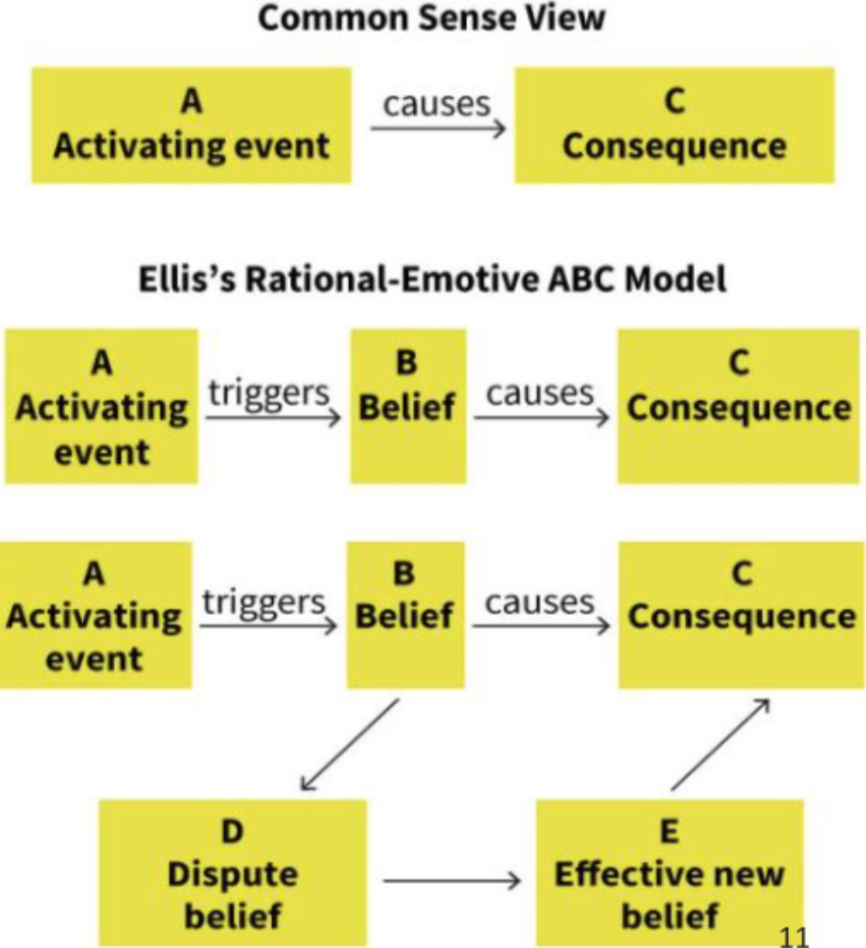
Rational Emotive Therapy (cognitive approach)
Therapist challenges the patient’s irrational beliefs
pioneered by Albert Ellis
Assumes that beliefs (B) link activating events (A) and consequences (C)
If a client’s beliefs are irrational, they will lead to negative consequences
The therapist disputes the irrational beliefs and offers more effective substitutes
Cognitive Therapy
An approach that aims to change patient’s habitual modes of dysfunctional thinking about themselves, their situation, and their future
developed by Aaron Beck
Negative cognitive triad
Three types of dysfunctional beliefs related to oneself, their situation world, and the future
unhelpful assumptions (core beliefs): “I am inferior”, “My worth depends on what others think of me”
Critical incident later in life: relationship breakup
Negative automatic thoughts or cognitive distortions: “It’s all my fault”, “I’ll be alone forever”, “I’m stupid”, “something is wrong with me”
Cognitive restructuring
A set of cognitive therapy techniques for changing a person’s maladaptive beliefs or interpretations through persuasion and confrontation
Cognitive-Behavioral Therapy (CBT)
A hybrid approach focused on changing the patient’s habitual interpretations of the world and behaviors by combining cognitive and behavioral approaches to therapy
General principles of CBT
Present-focused
Concerned with identifying and solving problems that clients wish to address
Sessions are highly structured, with assigned homework
Goals are transparent, set collaboratively, and progress is openly discussed
Acceptance and commitment therapy
Aims to help clients achieve greater awareness and acceptance of thoughts and feelings; de-fuse from thoughts; emphasizes pursuing valued goals despite unwanted thoughts and feelings
Mindfulness-based stress reduction
Draws from southeast Asian meditative traditions to teach clients to be fully present by observing their thoughts, feelings and sensations non-judgmentally. Practices controlled breathing
What is eclecticism?
Approach to treatment that weaves together multiple types of therapy
Dialectical behavior therapy
Now a single therapy, but brought together different approaches to treat Borderline Personality Disorder
“dialectic” — a dialogue about two different points of view to arrive at truth through reasoned argument
The relationship between things defines things (no single cause/effect, no blame, ficus on acceptance and adaptation)
Holding two opposite ideas simultaneously is the foundation of change (e.g. accepting the present and working toward chnage
moves away from all-or-nothing, either/or thinking (“I am angry AND I love you” “I accept who I am AND I want to change”
Also has a group component to allow people to practice interpersonal skills like communication in a safe space, develop community and reduce shame
Cognitive-Behavioral
Clarifying link among thoughts, feelings, and behaviors, and identifying and changing unhelpful thought patterns
Psychodynamic
Interprets transference and resistance, and considers the influence of the past on current relationships
Humanistic
Focus on validation, self-acceptance and personal growth
Matched-Treatment Eclecticism
The clinician selects the treatment approach based on the person’s complaints. Different approaches for different patients and more than one approach for a single patient
Exposure and response prevention for OCD and CBT for maladaptive cognitions
CBT and medication for depression
CBT and Mindfulness-Based Stress Reduction for Generalized Anxiety Disorder
Challenging for clinician to stay up to date and expert in the practice of multiple treatment interventions
Group therapy
A form of therapy in which two or more patients meet with one or more therapists at time
Advantages over one-on-one therapy:
More clients can be accommodated by a limited number of therapists
Allows therapists to observe and treat problems that emerge in group settings (interpersonal relations)
Patients can see problems more objectively in other people
A sense of group belonging, support, and encouragement
Self-help and Support Groups
Individuals with a particular type of problem gather to share information, advice, support
e.g. Alcoholics Anonymous
Therapeutic Efficacy and Common Factors
Different forms of therapy each inspire in clients new ways of thinking about difficulties they are having, provide strategies to overcome difficulties, and support on the journey their role in repetitive interpersonal conflicts
conflicting goals and see a path towards reconciling them
What triggers their anxiety and how to develop confidence to interact normally
The powerful role of automatic thoughts
That psychological disorders, like medical disorders, are treatable and not shameful problems
Therapeutic alliance
The relationship between therapist and patient that helps ,any patients feel hopeful and supported
most important predictor of therapy efficacy, even in med response
psychopharmacology: Typical Antipsychotics
antipsychotic medications that blocks the transmission of dopamine, by binding to the D2 dopamine receptor
reduce the positive symptoms of schizophrenia like thought disorder and hallucinations
Less effective at treating negative symptoms of schizophrenia, like flat affect and the inability to feel pleasure
Side effects:
common: fatigue, weight gain, restlessness, sexual dysfunction, amenorrhea, dry mouth, hyperprolactinemia (can disrupt menstruation, cause milk discharge from nipples, cause males to grow breasts), falls From sudden drops in blood pressure, heart arrhythmias
Long-term: Tardive dyskinesia (involuntary movements of face and younger)
Clozapine: the Original Atypical
Antipsychotic medication that blocks the transmission of dopamine, but unbinds quickly, and also binds to alpha-adrenergic receptors and serotonergic receptors
reduce the positive symptoms of schizophrenia-like thought disorder and hallucinations
Better than typical antipsychotics at treating negative symptoms, like flat affect and the inability to feel pleasure
Reduces suicidality
Side effects:
Greater than typicals: weight gain, hyper-salivation, fatigue, diabetes,, agranulocytosis (requires blood monitoring)
Does not cause hyperprolactinemia and its complications
Similar to typicals in restlessness, sexual dysfunction, falls from sudden drops in blood pressure, heart arrhythmias
Long-term: (less than typicals but present) Tardive dyskinesia
Antidepressants
Early antidepressants fell into two major classes:
monoamine oxidase (MAO) inhibitors and Tricyclics
Both increased synaptic levels of norepinephrine
Both had potentially fatal side effect profiles
Selective serotonin reuptake inhibitor (SSRI)
Increases synaptic serotonin levels (e.g. Prozac, Zoloft, Celexa)
fewer side effects than earlier treatments
Side effects: headache, nausea, insomnia, bad dreams, sexual dysfunction
Must be slowly down-titrated to discontinue
Selective serotonin reuptake inhibitor (SNRI)
Increases synaptic serotonin and norepinephrine levels (e.g. Effexor)
Less used because more dry mouth, sweating and can increase anxiety
Limitations of antidepressants
one month to take effect
Uncertainty about how much benefit can be attributed to placebo effects
Placebo effects: the influence of a patient’s beliefs and expectations In bringing about a cure
Necessary trial and error period of prescription to determine benefits and side-effects of different drugs for individuals
Potential for reduced benefit after prolonged use slide effects: weight gain, insomnia, loss of sexual desire
Mood stabilizer
A medication that treats manic, mixed, or depressive states . Use to treat bipolar disorder
Lithium carbonate (the first mood stabilizer and still used today)
more effective at reducing manic than depressive symptoms
Works for 60-70% of people with bipolar disorder
Side effects: weight gain, sedation, dry mouth, tremors
Toxic at higher doses
Carbamazepine
Anti-seize med also used as a mood stabilizer
Anti anxiety Medications (Anxiolytic)
Benzodiazepines and Beta blockers
Benzodiazepines
Enhance the effect of GABA binding, hyperpolarizing the cell (prevents from firing) (e.g. Xanax, Ativan, Valium)
other agents that bind to GABA sites: barbiturates (sedative sand anti-seizure) and an aesthetics like propofol (both potentially fatal) and alcohol
Beta blockers
Blocks beta-adrenergic receptors (involved in fight or flight) so decrease physical symptoms of anxiety and prevents negative spiral. Used especially for situational anxiety (performance anxiety, social anxiety, flying phobia) ((e.g. propranolol (Inderal), atenolol). Also used in PTSD
Antianxiety Medications: Considerations
Benzodiazepines:
Can be useful short-term. Not recommended for long-term use due to
High addictive potential
Dangerous interactions with alcohol
Risk to fetal development if patient is pregnant
Rebound effects
Does not address the cause of anxiety
Beta-blockers:
can cause drowsiness, cold hands and feet, low blood pressure
Medication Treatment for ADHD
Stimulants: Methylphenidate, D-amphetamine
Bind to the presynaptic dopamine transporter (DAT) and norepinephrine transporter (NET) to block reuptake of DA and NE into the presynaptic neuron
This increases synaptic levels of dopamine and norepinephrine transporter
Effects: improves ADHD symptoms in 70-80% children, 70& of adults
Discontinuation rates: high in transition from childhood to late adolescence. In adults, discontinuation rates range from 52-87%
Reasons for discontinuation: mood changes, increased anxiety, irritability, personality changes, and perceived ineffectiveness
Costs and Benefits of Using Psychotropic
Psychotropic medications have provided profound benefits for many people
Lifted people out of misery and allowed for more normal lives
Allowed people to remain in communities and avoid being hospitalized
Guesswork regarding dose and right medication
Statistically effective medications still do not work in many people
Adaptive response may not be learned so problem persists when meds stop
Side effects can mean people want to discontinue, and then may relapse
Some drugs cause rebound symptoms when discontinued, making them difficult to discontinue