Nutrition I+II
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
nutrients
chemicals used by the body for cellular purposes and energy
micronutrients→ vitamins, minerals
macronutrients→ carbs, proteins, fats
energy is measured in calories(c/kcal)→ energy needed to raise 1 kg of kg by 1 degree Celsius(varies by age)
energy sources→ proteins + carbs=4 cal/g, fats=9 cal/g
if energy is not used it is stored as fat
failure to thrive
inadequate nutrition to support growth and development
organic cause→ cachexia(kuh·kek·see·uh) due to pathology→ e.g. cardiac, GI disease, cancer
cachexia: wasting syndrome associated with chronic illness→ accelerated BMR, high cytokines affecting normal hunger triggers=low appetite
non-organic causes: poverty and neglect(child abuse)
neglect→ most predominant type of child abuse in North America
tx: treat the cause, increase calories per mL, hydrate, vitamins and minerals
marasmus
deficient in calories and proteins
person needs adequate protein, fats, and carbohydrates
subcutaneous fat is not preserved
ribs become very prominent, severe muscle wasting
no fatty liver or edema
voracious feeder→ very hungry
common in infants under 1 year
kwashiorkor(kwaa·shee·or·kor)
develops in children ages 6 months to 3 years whose diets are deficient of protein
patient requires adequate amounts of proteins
subcutaneous fat is preserved
ribs are not prominent, mild or absent muscle wasting
enlarged fatty liver
edema is present(protuberant belly)
poor appetite→ because the child is eating but does not have enough protein
common in children weaned off of breastmilk who lack protein→ low albumin(plasma protein) leads to fluid shift
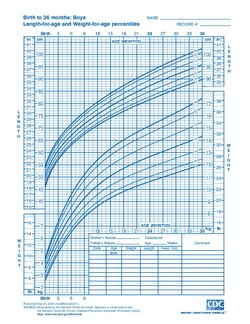
testing and treatment for growth & development
growth charts→ pediatric patients(measure head circumference too)
weight
BMI-adults
serum albumin for protein intake assessment
tx: increase or limit caloric intake
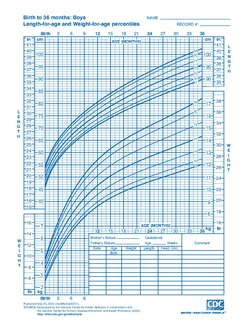
growth charts
trend=general direction of change
it is expected to be a little below or above
*know how to plot
enteral nutrition
use for patients who need to increase calories or who cannot eat regular food
PO→ GI feeding tubes e.g. NG, NJ, nasoduodenal(ND) G-tubes
preparations:
polymeric(proteins, lipids, carbs)= intact nutrients, high calorie e.g. pediasure, ensure
oligomeric(easily digestible components e.g. amino acids, peptides)→ hydrolyzed nutrients
specialized→ if organ disease is present
timing of enteral nutrition
bolus: mimics normal meals, 3x per day
intermittent→ similar to bolus but at a slower infusion e.g. 30-60 min
continuous→ ideal for recovery, avoids dumping syndrome= osmotic shift
total parenteral nutrition
is patient specific delivered via central IV line
goal→ increase nutritional intake
s/e: fluid overload, infection, electrolyte imbalances, hyperglycemia, GI dysfunction
osteoporosis
fragile bones due to increased bone resorption
most common cause=menopause→ decreasing estrogen at middle age for females
bone cells have intracellular estrogen receptors which stimulate osteoblast bone building
other causes→ thyroid hormone deficiency, genetics, very high ETOH and caffeine intake
monitoring→ bone scan
tx:
vitamin D and calcium
bisphosphonates: suppress osteoblast activity, “-nate”
alendronate, risedronate
vitamin D and calcium
Calcitriol(1.25-dihydroxyvitamin)→ active vitamin D3, given for vit D deficiency if at risk risk due to GI/liver/renal dysfunction
calcium→ gluconate, acetate, citrate
vitamin D3 can be overdosed because it is lipid soluble
→ S&S: fatigue, N&V, GI pain
breastmilk
breastfeeding recommended exclusive 6 months up to 2 yrs of age
56% milk fat
70 calories per 100 mL
contains:
fatty acids essential to brain development
amino acids
carbohydrates→ lactose
essential minerals, vitamins, trace elements
free water
immunity components: IgA, EGF, leukocytes
Iron→ bioavailability up to 100%
is low in vitamin D, so this must be supplemented
breastfeeding physiology
female lactation hormones stimulation:
prolactin(from anterior pituitary gland)→ milk synthesis
oxytocin(posterior pituitary)→ milk excretion
quantity and quality of breastmilk is hormone dependent and stimulated by infant’s suckling
contraindications for breastfeeding: HIV infection, drug abuse, lactose intolerance
breastmilk
colostrum→ 1-3 days post delivery, highly immunologic(IgA, EGF), low in lactose
transitional milk→ 3-14 days post delivery, contains: lactose, protein, fat
mature milk→ > 14 days post delivery:
◦foremilk→ higher in free water
◦ hindmilk→ higher calorie and fat
lactose intolerance
inability to breakdown(hydrolyze) milk sugar lactose due to lack of enzyme lactase
lactase enzyme deficiency(brush border duodenum)
lactose is broken down into glucpse and galactose
high incidence, increasing with advancing age
common in Asia, Africa, South America
types:
congenital→ autosomal recessive trait
primary→ decreasing levels of lactase with age(common after 2 yrs old)
secondary→ associated with other illness→ crohn’s disease flare-up
S&S of lactose intolerance
unabsorbed lactose causes an osmotic shift
fluid shifts into intestine creating watery stool + the fermentation of lactose by colony bacteria
leads to diarrhea, gas, bloating/cramping and flatulence
galactosemia
inability to metabolize galactose with the enzyme GALT
arginine supplementation does not help
treatment for lactose intolerance
stop + avoid milk intake(human or dairy)
lactose free formula is available for babies
drug: lactaid→ lactase enzyme supplement, not for infants