Lymphatic and Immune System- A&P 2
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
Pathogens
Microscopic organisms that cause disease
Viruses
Bacteria
Fungi
Parasites
The lymphatic system includes…
…Cells, tissues, and organs responsible for defending the body against:
Environmental pathogens
Toxins
Abnormal body cells, such as cancers
Immunity
Ability to resist a pathogen and mount a defense, infectious response, or counter a pathogen
Nonspecific defenses (Innate defenses)
1st line of defense: Phagocytes, granulocytes, lysozymes, opsins, etc
Block or attack any potential infectious organism
Does not distinguish one invader from another
Specific defenses (Adaptive defenses)
Lymphocytes, T-Cells and B-Cells
Identify, attack, and develop immunity to a specific pathogen
Extended or lifelong memory for specific pathogen
Lymph
A fluid similar to plasma but much fewer proteins, contains more lipid metabolites
Originates as interstitial fluid from excess extracellular fluid
Lymphatic vessels (Lymphatics)
Carry lymph from peripheral tissues to the venous system (via the thoracic duct)
Lymphoid tissues
High concentration of lymphocytes, macrophages
Lymphoid organs
High concentration of lymphocytes, macrophages, and NK cells enclosed in fibrous capsule
Lymph Nodes
Are the body’s Police Checkpoints
Quarantine off pathogens or cancer to a point
Concentrated at points of vulnerability
Lymph nodes survey lymph fluid and components in the lymph fluid
Lymphatic System function
To aid in production of lymphocytes
T-Cells mature in lymphatic tissues and organs
Drain Excess Interstitial fluid and return to the blood
Maintain blood volume
Ensure similar composition of interstitial fluid throughout the body
Immunity
Lymph passes through lymph nodes
Immune cells activate immune response if needed
Fat Absorption
Lacteals
Chyle
Lacteals
In the small intestine absorb dietary fats and fat-soluble vitamins and transport them to the blood as chyle
Chyle
Is a collection of fat particles: Chlyomicrons, Trig, Vit ADEK
Lymphatic capillaries
Differ from blood capillaries in 4 ways:
Start as pockets rather than tubes
Have larger diameters
Have thinner walls
Irregular outline in sectional view
Overlap
Loosely binds together endothelial cells
Overlap acts as a one-way valve
Allows fluids, solutes, lipids, viruses, parasites, and bacteria to enter
Prevents return into interstitial fluid/intercellular space
Lymphangiogenesis
Lymphatic vessels
Lymphatic capillaries flow to lymphatic vessels
Contain one-way valves
Travel through body with veins as they head towards trunk by LMCs
Superficial lymphatics
Located in skin, mucous membranes, serous membranes lining body cavities
Deep lymphatics
Larger vessels that accompany deep arteries and veins in the:
Neck
Limbs
Trunk
Lymphatic trunks
The joining of superficial and deep lymphatics together
Empty into two major collecting vessels: Thoracic duct and right lymphatic duct
Right lymphatic duct
Collects lymph from the right side of the body, superior to the diaphragm
Empties into right subclavial vein
Thoracic duct
The base expands into cisterna chyli which receives lymph from the abdomen, pelvis, and lower limbs.
Collects lymph from the left arm, left side of head, neck, and chest
Empties into left subclavial vein
Lymphedema
Blockage of lymphatic drainage from a limb
Causes buildup of interstitial fluid, swelling
Risk of severe infection in the area because it is essentially cut off from the rest of the lymphatic system
Most commonly a result of removal of damage to lymph nodes during cancer treatment
Elephantiasis
Lymphatic filariasis (worms)
Mosquito-borne parasitic disease
Blocked lymph vessels
Swelling, skin-thickening, stiffening of limbs
Tx: Ivermectin + Albendazole + Diethylcarbamazine
Lymphocytes
Make up 20-30% of circulating leukocytes
Most lymphocytes are not circulating
Types: T Cells, B cells, NK cells
T Cells
Thymus-dependent
Make up 80% of circulating lymphocytes (Defectives)
Cytotoxic T Cells (Specific Killers)
CD8 Cells
Attack foreign cells or cells infected by viruses
Helper T Cells (Generals)
CD4 Cells
Stimulate function of T cells and B cells
Antigen presentation by Macrophages and Dendritic cells
Pathogens must be processed before cytotoxic and helper T-Cells can recognize an invader
Antigen Presentation; APCs: Dendritic cells, langerhans cells, macrophages, B-Cells
• Engulf pathogen (exogenous)
• Extract antigens and package different pieces (epitopes) for presentation
• Display on cell surface on MHC I and MHC II
• APC “presents” the antigen to Helper T-Cell
• Activated Helper T-Cell to authorize APC to engage CD8 (NO auth, no go)
Stimulates B-Cells to make antibodies
Help activate cytotoxic T-Cells by releasing cytokines
Trigger destruction of pathogens engulfed by Macrophages
Antigen Presentation; Co-stimulation of Cells
Cells display MHC I proteins on cell surface of all nucleated cells
When antigen on MHC is normal, no response stimulated
When antigen on MHC is abnormal (virus infected/cancer cells):
Cytotoxic T-Cells specific for that antigen are activated
Apoptosis of target cell (and damage to viral DNA)
Induce Caspase enzymes path
Proliferation of T-Cells specific for that antigen
Memory T Cells
Formed in response to foreign substance when T-cells are activated
Remain in body to give “immunity” to that substance
Suppressor T Cells (Regulatory T Cells / Tregs)
Limit the immune response - dose dependent expression
Important in preventing autoimmune diseases
Express inhibitory cytokines
B Cells
Make up 10-15% of circulating lymphocytes
Do not directly attack invaders, but responsible for antibody mediated immunity called humoral immunity
T-Cell-Dependent Activated B-Cells differentiate into:
Plasma cells: Produce and secrete antibodies (immunoglobulin proteins) – IgG, IgE, IgA, IgM, IgD (require 14-21 days)
Memory B Cells: Remain in lymph nodes after primary infection. Lead to production of antibodies quickly if secondary infection occurs (within 2-3 days)
T Cell- Independent B-Cell Activation
• These B-Cell reside in the Marginal Zone of the Lymph Nodes
• Rapid Response to Non- Protein Antigens
• Bacterial Polysaccharides & Lipopolysaccharides (LPS)
• E-Coli, Salmonella, Staph, Strep, Hib, N. Menin
• Gram- LPS endotoxins & Gram + polysaccharides are Highly repetitive on bacterial membrane
• Cross-link Multiple TLRs
• Antigens bind to several surface IgD’s on B-Cell
• High-intensity surface signaling to trigger low affinity IgM & some Memory B cells
Antigens
• Molecule that triggers an immune response
• Epitope binds to antibodies and CD8 cells
• VERY specific recognition-dependent binding
• Strong affinity at the Antigen Binding Site variable region to the pathogen
• Fc Region recognized by immune cells
• Ex: COVID Spike Proteins
Immunoglobulins (Antibodies)
• Soluble proteins that bind to antigens
• Pathogen is tagged for destruction
• IgG most abundant, affinity, pass placenta
• IgA (mucosal), IgE (allergies), IgM (1st)
Antibody function
Neutralize: Blocking immunogenic regions of antigen
• IgGs bind to Viral capsule proteins
• Tagged for destruction by the other B-cells
Complement fixation
• Antibody binds to antigen
• Complement proteins bind to antibody
• Inflammation, improved phagocytosis, cytolysis
Agglutination (IgG, IgM)
• Antibody binds to multiple antigen molecules
• Clumping prevents spread
• Immobilized Pathogens
Natural Killer (NK) Cells
• Make up 5–10% of circulating lymphocytes
• Apart of the Innate Immune System
• Normal cell express MHC class I
NK Tolerance with normally expressed receptors
• 1st line defense for virus-infected cells and cancerous cells
• Bind to target cell expressing Stress Signals or No MHC class I receptor
• Cancer cells mutate & STOP expressing MHC class I receptors to evade CD4 surveillance
• NK cells Release perforins and cytokines to perforate plasma membrane on target
• Cytolysis – granzymes B
Lymphopoiesis
Process of producing T cell, B cell, and NK cells
Stem cell differentiation in progenitor cells then differentiate into effector cells
Lymphopoiesis maturation and activation sites
• Bone marrow – B cells maturation
• Thymus – T cells mature in the Thymus after leaving the bone marrow
• Peripheral lymphoid tissues
• Lymphoid follicles have B cells that rapidly proliferate in Germinal Centers when activated
• T-cell Zones (paracortex) of the lymph nodes
Hemocytoblasts
In bone marrow, divide into two types of lymphoid system cells
Group 1: Remains in bone marrow, produces B cells and NK cells
Group 2: Migrates to thymus, produces T cells into environment isolated by blood-thymus barrier
T Cells and B Cells location
• Are located throughout the periphery, especially in lymphoid tissue
• Retaining their ability to divide is essential to immune system function
• B cells differentiate with exposure to a type of hormone called a cytokine (interleukin: IL-4, IL-6, IL-21, BAFF)
• T cells differentiate with exposure to several thymic hormones (thymosin) as well as interleukin (IL-2, IL-7, IL-12, IL-15, IL-18)
Lymphoid tissues
• Connective tissues dominated by lymphocytes
• Do not have a fibrous capsule surrounding them
Lymphoid Nodules
• Areolar tissue with densely packed lymphocytes
• MALT, tonsils, Peyer’s Patch
• Germinal center contains dividing lymphocytes
• Transient in most tissues
Diffuse Lymphoid Tissue
Constant in lymph nodes, tonsils, appendix, along GI, urinary, and reproductive tracts
Mucosa-Associated Lymphoid Tissue (MALT)
Collection of lymphoid tissues that protect the epithelia of the Mucus Membranes of the respiratory (BALT), digestive (GALT), urinary, and reproductive tracts for 1st line of defense protection.
• Aggregated Lymphoid Nodules “Peyer’s patches”
Organized GALT clusters of nodules deep to Small Intestines epithelial lining
• Appendix (Vermiform Appendix)
A mass of fused lymphoid nodules where the small and large intestines meet
• Tonsils
Large nodules in the walls of the pharynx
Tonsilitis
• Most common reasons for pediatric medical visit
• Inflammation of the tonsils
• Usually caused by Viruses (flu, EBV mono) or Group A Strep infection
• Treatment: Fluids, ibuprofen, acetaminophen, Amoxicillin, tonsillectomy
Lymphoid Organs
• Are separated from surrounding tissues by a fibrous connective tissue capsule
Lymph fluid pass through
• Lymph nodes
• Thymus
• Spleen
Lymph Nodes
Small lymphoid organs concentrated in the neck, armpit, and groin for 1st line of defense
Trabeculae
• Bundles of collagen fibers
• Extend from capsule into interior of lymph node
Hilum
A shallow indentation where vessels and nerves reach the lymph node
Afferent lymphatics
Carry lymph from peripheral tissues to lymph node
Vessels on opposite side from the hilum
Efferent lymphatics
Carry lymph from the node to venous circulation
Leave lymph node at hilum
Lymph Flow
Flows through lymph node in a network of sinuses
Subscapular space (contains macrophages and dendritic cells cDC & FDC) → Outer cortex (contains B Cells within germinal centers) → Deep cortex (dominated by T Cells) → Through the core (medulla)(contains B Cells and plasma cells) → Hilum and efferent lymphatics
Lymph Node Function
• A filter that purifies lymph before returning it to venous circulation
• Removes: Debris, pathogens, 99% of antigens
• Site of B-Cell and T-Cell activation
• Stop pathogens before they reach vital organs of trunk
• Carries dietary fats and utilizes these lipids for energy, structural integrity, and signaling.
• LEC use fatty acid beta-oxidation (FAO) as a primary energy source for growth
• Proliferating T and B cells within lymph nodes utilized significant FAO
• LMC utilize FAO as a critical component of their mitochondrial bioenergetics
Lymphadentitis
Inflammation of a lymph node
When a node is fighting an antigen, pathogen, or cancer it may swell
Increase in the number and size of germinal centers within cortex
PMN infiltration can lead to abscess formation and swollen node that are often painful
Can be palpated on PE
Lymphoma
Cancer of a lymph node
• Cancerous cells destroy the normal structure and
breach the capsule
• Lymphatic capillaries are highly permeable
• Lymph nodes are common sites of metastasis
• Lymph Node are critical in determining Dx and Tx
Thymus
• Located in mediastinum
• Academy of the Immune System – central tolerance
• Thymus is divided into 2 lobes (Bilobed)
Each lobe is divided into many lobes by trabeculae
• Large in infants/children, atrophies after puberty
• Diminishing effectiveness of immune system making elderly more susceptible to disease
• Pivotal in immune cell education of self
• Heavily implicated in the development of various autoimmune disease
• T1 DM, SLE, MG
Thymic Lobule
Contains a dense outer cortex and a pale central medulla
T-Cells in Thymus
• Divide, differentiate in the cortex
• Migrate into medulla where they are tested
• Mature T cells leave thymus by medullary blood vessels
Thymus: Secrete thymic hormones (thymosin)
WBC recruitment (chemotaxis), directs movement, and proliferation
T Cell differentiation
Enhances NK and DC activity
Thymus: Reticular Epithelial Cells
Framework for lymphocytes in thymus
Cortex
Surrounded T-Cells and vessels to create blood-thymus barrier
Promiscuous gene expression — Molecular mirror of 20,000+ proteins
Thymus: Medulla
• No blood–thymus barrier
• T cells can enter or leave bloodstream
Spleen
Spleen is the largest lymphatic organ, blood rich, lies between lateral border of stomach and diaphragm
Functions of Spleen
• Removal of aged and abnormal blood cells, platelets, and other blood components by phagocytosis (macrophages)
Initiation of immune responses by B cells and T cells
Macrophages and Lymphocytes monitor the blood for antigens
Activate T-Cells and B-Cells when antigen present, esp. IgM
Pathogen Clearance esp. encapsulated bac.
• Maintain blood volume
Stores red blood cells and platelets
Mobilizes in case of hemorrhage & hypoxia
Iron recycling to bone via transferrin
Histology of the Spleen: Red Pulp
Contains many red blood cells
Removal of old blood cells by macrophages
Destroy antibody coated cells and virus or bacterial infected cells
Histology of Spleen: White pulp
Resembles lymphoid nodules
T-Cell activation
Immune surveillance
Initiation of immune responses
Splenectomy
• Spleen is very fragile and capsule ruptures easily
• If capsule ruptures, massive internal bleeding is possible, leading to circulatory shock
• Spleen cannot usually be repaired because structure is so delicate
• Treatment is to remove the spleen (splenectomy)
• Increased risk of infection post splenectomy
• Risk of Overwhelming Post-Splenectomy Infection (OPSI)
• Decreased immunity against encapsulated pathogens; Strep Pneumonia, HiB, N. Meningitis
• Prophylactic and acute antibiotic treatment: Pen V, Vanc, Ceftriaxone, or Levofloxacin
Innate (Nonspecific) defenses
• Present at birth
• Always work the same way against any type of invading agent
• Nonspecific resistance
Adaptive (Specific) defenses
• Protect against specific pathogens
• Depend on activities of lymphocytes
• Specific resistance (immunity) develops after exposure to pathogen/antigen (accidental or intentional)
• APC-mediated and antigen-receptor binding responses
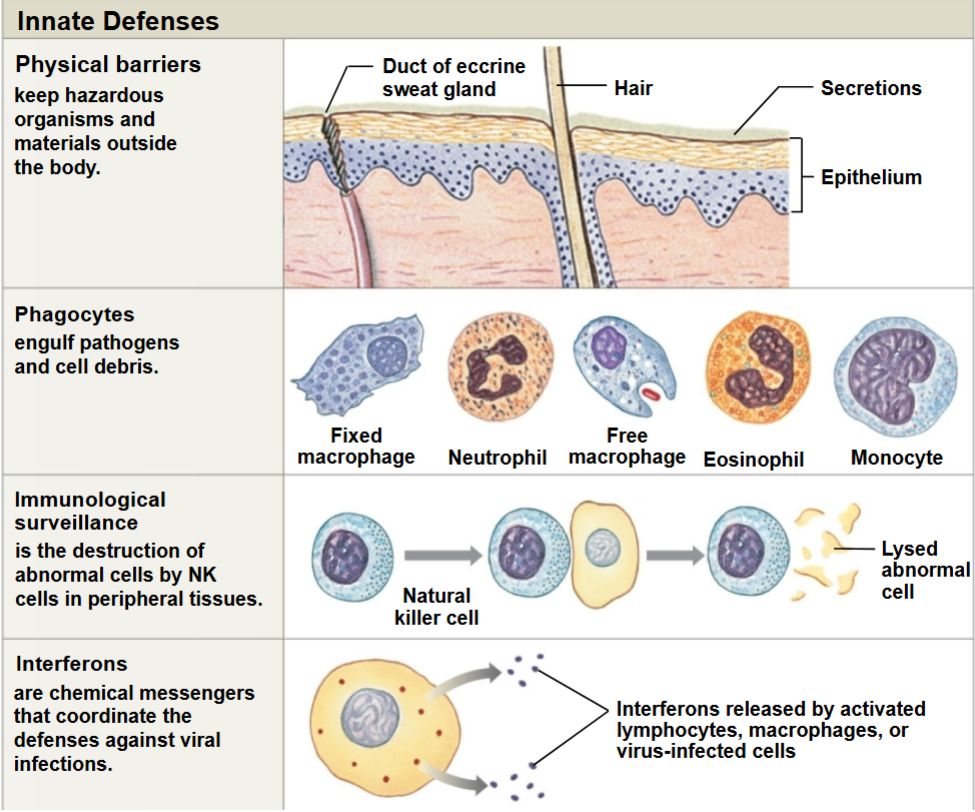
Physical Barriers
Keep pathogens outside of the body
Epidermis (Vit C aka Ascorbic Acid) is needed for skin and gums
Scurvy- Severe Vit C deficiency
Mucous membranes
Hair/cilia
Secretions that flush away materials (Perspiration, lacrimal apparatus, mucus, urine, vaginal secretions, defecation/vomiting)
Secretions that kill or inhibit microorganisms (saliva, sweat, sebum, and stomach acid)
Phagocytes (Leukocytes)
Engulf and degrade cellular debris, foreign compounds, pathogens
Basophil (Non phagocytic leukocyte)
• Aid in mobility and action of other WBC
• Leukotrienes: attract WBC to the area
• Histamine: Dilates blood vessels bring WBC into tissue quickly
• Heparin: Prevents blood clots that may impede entry of WBC
• Allergic Responses, parasitic defenses
• Immune Regulation
Microphages
• Neutrophils and eosinophils
• Circulate in the blood
• Enter peripheral tissues that are injured or infected
• Once activated and phagocytize pathogens they usually die within hours to days.
• Leave behind Pus that is composed of active and dead leukocytes, mainly leukocytes
Macrophages
Large phagocytic cells derived from monocytes
Phagocyte Functional Characteristics
• Move through capillary walls (emigration)
• Are attracted or repelled by chemicals in surrounding fluids (chemotaxis)
• Phagocytosis:
Begins when phagocyte attaches to target (adhesion)
Then surrounds it with a vesicle (Endocytosis)
Finally digests target
Immunological Surveillance
Constant monitoring of normal tissues searching for abnormal cells
• Is carried out by natural killer (NK) cells & CD8 T-cells, esp. seeking out tumors
• But NK cells respond more quickly than T-cells or B-cells
• Can attack bacteria, cancer cells, and cells infected with viruses
• NK Cells kill abnormal cells by releasing vesicles containing perforins and granzymes.
Perforins are proteins that create pores in the abnormal cell’s plasma membrane
Granzymes enter cell and induce apoptosis
Interferons (IFNs)
Proteins released by activated lymphocytes and form virus infected cells
Chemical messengers that trigger production of antiviral proteins in healthy cells
Antiviral protiens: Do NOT kill viruses or block entry, they DO block viral replication in cell
Slow the spread of viral infections and stimulate activity of macrophages and NK cells
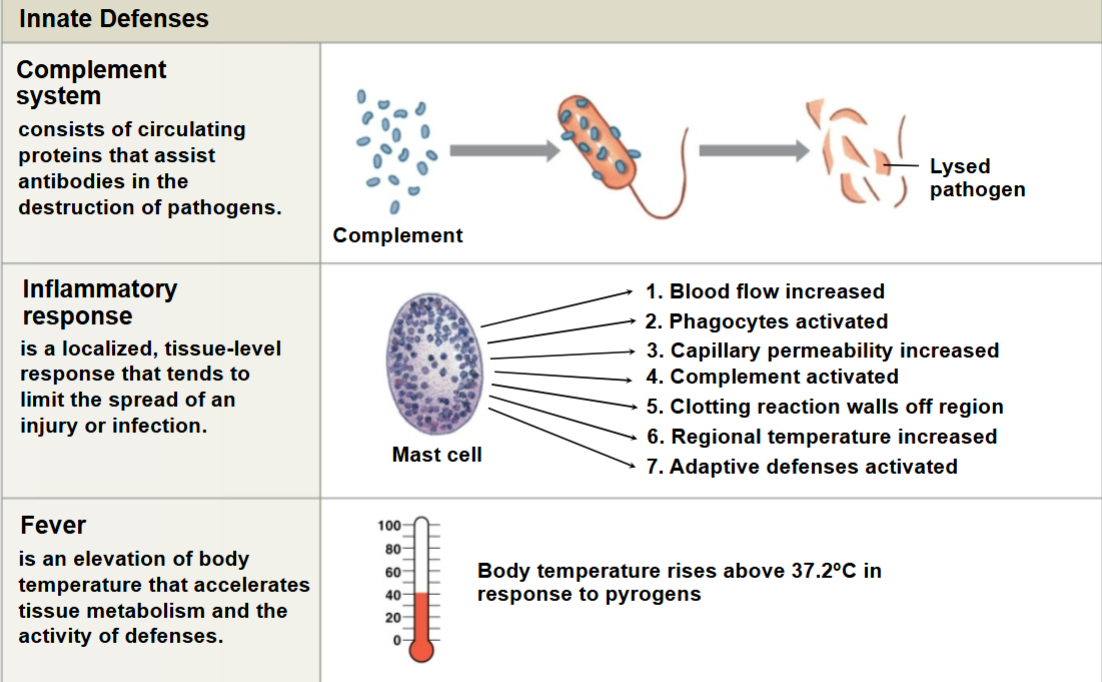
Nonspecific Defenses: Complement
• Plasma contains 11 complement (C) proteins that form the complement system
• Made in Liver
• Assists antibodies in destruction of pathogens (“complement” antibody action)
• Complement activation
• Complement proteins work together in cascades
Three pathways activate the complement system
Classical pathway →
Alternative pathway → Membrane Attack Complex
Lectin pathway →
All pathways end with the splitting of C3 to the active C3a and C3b
Effects of Complement Activation
• Pore formation to destroy target’s plasma membrane
• Complement proteins form membrane attack complex, MAC
• Enhancement of phagocytosis by opsonization
• Histamine release
• Increases the degree of local inflammation and blood flow
• Increased Vascular Permeability
Inflammation “inflammatory response”
• A local tissue response to injury
• Triggered by any stimulus that kills cells or injures tissue
• Tends to limit the spread of injury or infection
• Cardinal Signs and Symptoms of Infection
Swelling
Redness
Heat
Pain
Fever
An abnormal elevation of body temp (>100.4 degrees F)
Increases body metabolism
Intensifies effects of interferons
Inhibits some viruses and bacteria
• Pyrogen raises the hypothalamic set point
• Hypothalamus releases prostaglandin
• Body thinks it is too cold and initiates mechanisms to raise body temperature
Shivering
Constriction of cutaneous vessels
• Body temp rises, fever is now present
• Aspirin, ibuprofen, and naproxen inhibit the COX-2 enzyme to prevent prostaglandin synthesis
Pyrogens
• Any material that causes the hypothalamus to raise body temperature
• Exogenous pyrogens: From foreign pathogens (glycolipids from bacteria, viruses)
• Endogenous pyrogens: Released by active macrophages and neutrophils
• Interleukin Initiated by IL-1 氰 & IL-1 氠 (most potent), IL-6 (maintain fever), TNF 氠 (stimulate release of IL-1s)
• Induce the COX-2 and microsomal Prostaglandin E Synthase 1 (mPGES-1)
HIV: Human Immunodeficiency Virus
• Spread through infected bodily fluids (blood, semen, vaginal secretions, breast milk, exposed cuts, direct contact with immune cells)
• Binds to, Invades, and Replicates in Helper T-Cells (CD4), Dendritic Cells, Macrophages
• Destroys CD4 T-Helper Cells, inhibits immune system function
• Initial symptoms are flu-like but worsen as CD4 count drops
AIDS: Acquired Immunodeficiency Syndrome
• CD4 count < 200 cells/microliter
• Patient succumbs to opportunistic infections and cancer (Kaposi Sarcoma)
• Experience Oral Thrust (Candidiasis), PCP Pneumonia, TB, CMV, HSV, HPV, PML
Lupus
• Chronic, widespread, autoimmune disease
• Immune system forms Autoantibodies against healthy, self, cells
• Antibody-antigen complexes accumulate and lead to widespread inflammation
• Symptoms can be present in skin, joints, kidneys (lupus nephritis), hair loss, deep breathing chest pain (pleurisy), and other organs
• Malar “Butterfly” rash
• Photosensitivity & Joint Pain
• Organ failure
• Not contagious (Genetic, 90% Women, Epstein Barr Virus)
• Positive Antinuclear Antibody test
• No cure