Topic 7- Stress and mood disorders
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
the stres responce
• Some aspects of the response to many “stress-full” conditions are shared
• Being attacked
• Attacking somebody
• Hunger
• Cold
• Overheating
• ….
• Has effects throughout the body
Stress Stimulates the Sympathetic and Inhibits the Parasympathetic Nervous System
in voleved in the stress response –constrics blood vessels
symathetic involvend
paarsymthatics- supresses
less slivia made
increases hart rates
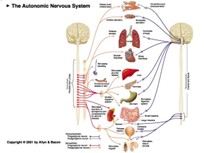
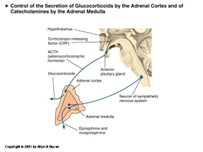
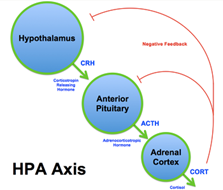
Systems Stimulated during Stress: Adrenal Hormones
ealicing neroadrilin onto our organs
two hormones that taher reliced into the blood stremes wicth are reliced by the adrenal gland- ontop of the kindey
it two separate glands
adrenal medulla(outside) and adreinal cortex ( outside)
adrenal madula- adrenalin and noraldarenialin
making postganglionic neorns into the relices of hormones
the adril;a madullia was triggared by the pituatry glan form the symathetic nervous system- nero stymliation
adrenal cortex- cortaisal (in humans) in response to acth witch comes in the blood stream stimulated and relaced
adrial cortex is stimualted by ACTH is in the blood stream nd binds to the receptors
act comes form the hpa axis
actch comes for the anteria pirtutary gland wicth is stimulated by the be crf/crh (same molucle ) witch comes form the hypothalumas
PVN part of the hypothalumas
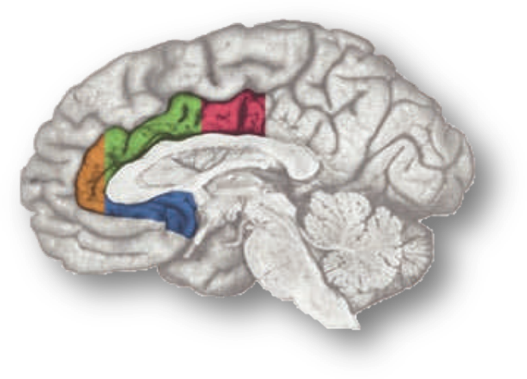
Activation of the Stress Response
amygdala
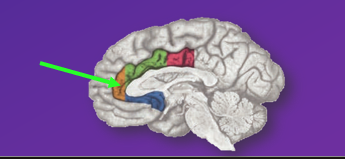
Subgenual Anterior Cingulate Cortex (sgACC -Telencephalon):
activations of the stress responce- Amygdala (Telencephalon):
Respnds to different challenges still make sthe same outcome
– Central Nucleus of the Amygdala
• In response to homeostatic challenges
– Medial Nucleus of the Amygdala
• In response to psychogenic challenges
– Amygdala activates the sympathetic nervous system (via lateral hypothalamus) and the HPA axis (via disinhibition)
2) Subgenual Anterior Cingulate Cortex (sgACC - Telencephalon):
– Indirect activation
Large area all he coulors the subegnual (blue) when is active activate sthe stress response
Activation of either brain area:
– activates the sympathetic nervous system
– activates the HPA axis
Regulation of the HPA axis
Body s not effectient during stress reponec
The body is constantly crearing hormones the concentration gose down nnee the body to keep cleaning and stop producing more
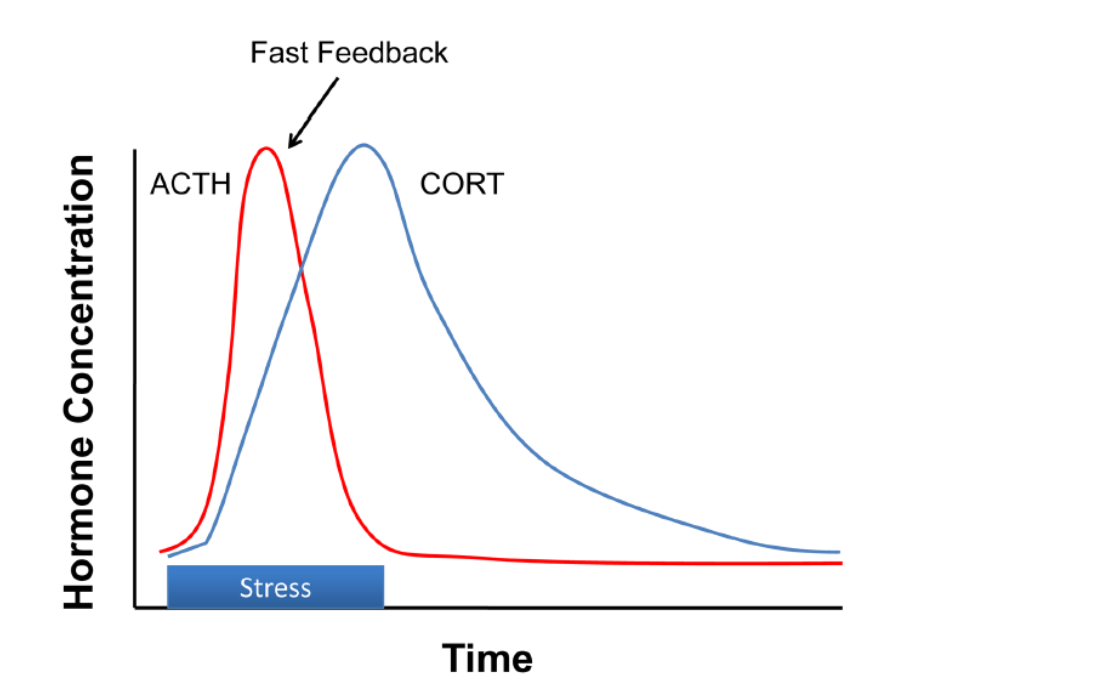
HPA axis: negative feedback
Direct negative feedback of Cortisol on the PVN via glucocorticoid receptors (GR)
to stop the cortisal (anterior) Hippocampus (Telencephalon)- get down after a stress responec
– Indirect inhibition
– Contains many MR and GR
– Intermediate-term feedback: returns psychogenic stress response back to baseline
Dorsal Anterior Cingulate Cortex (Telencephalon):
– Indirect inhibition
– GR receptors
– Early and intermediate-term feedback
Orage one-
Shoterning of the response and decraseing of the response
Major (Unipolar) Depression
• Some Symptoms:
• depressed mood • change in appetite
• sleeping problems • lethargy
• fatigue • feelings of worthlessness
• This has to be persistent and debilitating, and not easily explained by outside factors
• Twice as common in women as in men
Depression and the HPA axis
• Dysregulated HPA axis is common in affective disorders
• Both pathological increases and decreases in cortisol (due to other causes) can lead to depressive symptoms
Chronic Stress: Positive Feedback
• Amygdala stimulates the HPA axis
• Always a negaticve thing
• Can develop and cause dep
• Glucocorticoids activate the Locus Coeruleus
• Locus Coeruleus has noradrenergic projections which activate (among other brain areas) the Amygdala
oversystem of the stress responce witch makes constativly activataed
Chronic Stress: Reduced Negative Feedback
• Repeated stimulation by glucocorticoids reduces the sensitivity of receptors in the hippocampus
• Chronically high glucocorticoids also damage hippocampal neurons, leading to a further reduction of negative feedback (in the long term)
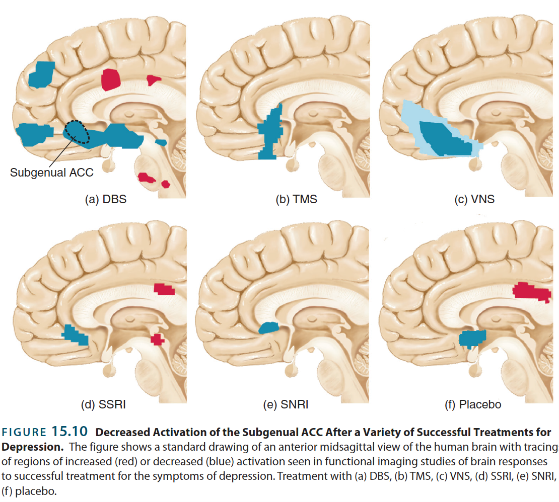
Reduction of the stress response is a common theme among effective treatments
Stress sresponce is an important aspet of depoersion
Reduction in activation of stressresponce- more effective trments
subjenial antiral cortex - reduce activity in
Decrese in activation of stress responce
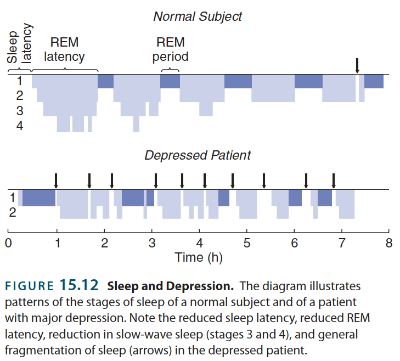
Major Depressive Disorder and Sleep
Sleep pattarns are desturbed
Tome of night and stage of sleep
Go to rem sleep to soon more intupted sleep poor slow wave sleep
fall aslep faster
distoerbed sleep
low levels of slow wave sleep
• REM sleep is entered too early
• REM sleep deprivation has long-term effects
• Many anti-depressants (but not all) suppress REM sleep
Monoamine Effects of Chronic Stress
• Depletion of noradrenaline from Locus Coeruleus
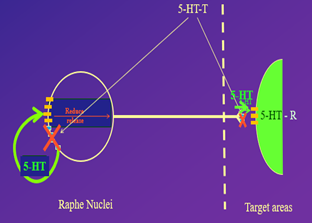
• Depletion of serotonin from Raphe Nuclei
• Depletion of dopamine from Ventral Tegmental Area to n. Accumbens and prefrontal Cortex
keeping seritionin and nerodreenilin higher
cronic activation of alternes mena sthat they use up all the seitonin and neodrenlim
Major Depressive Disorder: Pharmacological Treatments
• Targeting mono-amines
• Ketamine
Role of Mono-amines in depression
• Reserpine (Mono-Amine antagonist) can induces depression menaing taht monoaminics ddont work/less effective
• Lower levels of 5-Hydroxyindoleacetic Acid (5-HIAA) in Cerebrospinal Fluid- breack down produtcs of seritionin, deprestedn patoiants have lower seritionin
• Tryptophan (part of making seritonin comes form our diat) depletion experiments –depressed paiciret repond well to ssri’s then depleat trptophan then relay high amino acids- so have relay low trptophan they fall back inro a deprssed episode
Targeting Monoamines: SSRIs
• Usually ingested (pills)
• All very lipophilic
• Different pharmacokinetics for different drugs:
– Fluoxetine (Prozac): slow uptake, half-life 1-4 days
– Fluvoxamine (Faverin): bit faster, half-life 8-28 h
– Citalopram (Cipramil): bit faster, half-life ~36 h
BUT:
• SSRIs only work after several weeks- beacuse
– First two weeks: adaptation of auto-receptors
adaptation of auto recepteors
when taking ssris it blocks the uptake chanles mening thet tahe seritioning isnt getting recycled
the auutoreceptors will see the high level of seritoning and prevent seritonin from getting releced
so the sma eamout of seritionin is in the gap
it takes two weeks for auto recepters to adapat and suggest that that is the normal level of seritonin becomes less sesntive
• Initially, SSRIs increase 5HT levels in the synapse (by blocking reuptake channels)
• Autoreceptors respond to this and reduce 5HT release through negative feedback
• This leads to no change in 5HT levels at the target cells (lower release, but stays in synapse for longer, cancelling each other out)
• It takes about 2 weeks for the autoreceptors to adapt (tolerance) to the higher levels of 5HT
• This adaptation dials down the negative feedback, leading to a gradual increase in release of 5HT
• Since 5HT reuptake is still blocked, now levels of 5HT at the synapse do go up above original levels, leading to more 5HT binding to post-synaptic receptors
SSRI’s
BUT:
• SSRIs only work after several weeks
– First two weeks: adaptation of auto-receptors
– Further weeks:
• Could they have the opposite effect?
• Could be normalization of HPA axis feedback?
Maybe the effect is a healing process?
Adult hippocampal neurogenesis
• In animal models of depression, adult hippocampal neurogenesis is suppressed
• Anti-depressants increase neurogenesis
• Time course of increase = time course of effectiveness
• Destroying adult neurogenesis prevents anti-depressant effects
• Exercise increases adult neurogenesis and improves depression symptoms
Ketamine
• Dissociative anaesthetic and analgesic
• Taken through different routes:
– Snorted as a powder
– In pills
– Injected IV (including clinical use)
• Initial biological half-life 10-15 minutes (overall on average about 45 minutes)
Short term effects
• Low doses:
– Lightness & euphoria
– Disconnection of thoughts and from the world
– Strange perceptions
• Higher doses
– Mind-body disconnect
– K-holing (unresponsive to the world, hallucinations)
Ketamine physiological action
• NMDA-R Antagonist
• Responsible for
– Anaesthesia
– Dissociation & Hallucinations
– Amnesia
– Analgesia (in the spinal cord)
Ketamine as an antidepressant
• Origianly used as an anstetic
• Sub-anaesthetic dose can have a profound effect within hours of injection
• Typically a course of several doses per week for a few weeks
• Does not last more than a few months
• Seems to work through new synapse formation in anterior cingulate cortex
Ketamine long-term effects
• Memory/cognitive problems (possibly reversible)
• Bladder and kidney damage (irreversible)
• Abdominal cramps (k-cramps)
Ketamine addictiveness
• Physical addictiveness:
– tolerance does build up
– withdrawal symptoms include psychotic features
• Psychological addictiveness:
– Less known about it
– NMDA-R antagonists can influence dopamine release in nAcc
Anxiety disorders
• A range of disorders, characterized by extreme worry, fear, and chronic stress
• Often comorbid with depression and other disorders
• To be a disorder, it has to last more than 6 months, be inappropriate to the situation, and be debilitating
• Twice as common in women than in men
Treatments for anxiety
• Talking therapies (e.g. CBT)
• Exposure therapies
• Drug treatments
– SSRIs
– Beta-blockers
– Benzodiazepines
Benzodiazepines: Sedatives and Anxiolytics
• Usually ingested (pills)
– Valium, Xanax, Librium, Klonopin, Rohypnol,…
• Reach max. blood concentration in about 60 minutes (different drugs, different kinetics)
• Lipid solubility varies from drug to drug
• Depending on the exact chemical, half-life can be 90 min - 6 days (including active metabolites)
Benzodiazepines Short Term effects
• Effects:
– Sleepiness (sedative)
– Reduction of anxiety
– Anterograde amnesia
– Muscle relaxation
– Mental confusion
• Clinical use:
– Sleeping pills (against insomnia)
– Anxiolytic (against anxiety and panic disorders)
– Recovery from alcohol withdrawal
– Anticonvulsant (in combination with other drugs)Benzodiazepines: Physiological Action
Benzodiazepines: Physiological Action
• Facilitation of GABA-A receptors (increases inhibitory processes) -increase gabab effect
• GABA-A receptors exist throughout the brain:
– Cerebral cortex (amnesia & confusion)
– Hippocampus (amnesia and anti-epileptic)
– Spinal cord, brain stem (muscle relaxant)
– Cerebellum (muscle relaxant, anti-epileptic)
– Amygdala, orbitofrontal cortex, insula (anxiolytic)
– Tuberomammillary nucleus, etc. (hypnotic)
Benzodiazepine Long-term effects
• Mental confusion
• Induction or extension of dementia
• Learning problems
• Can improve after cessation of the medication
Benzodiazepine Addictiveness
• Physical dependence
– Will develop even with therapeutic doses
– Withdrawal symptoms include:
• Anxiety (possibly higher than before)
• Insomnia
• Restlessness
• Agitation
• Irritability
benzo • Psychological dependence:
– Alcoholics can be sensitive to benzodiazepine addiction as well
– There are GABA-A receptors in the Ventral Tegmental area and the N. Accumbens as well