OMFPR 28 - Differential Diagnosis (Dr. Campos)
1/98
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
What are the six parts of the radiographic description to help decide on category and formulate differential diagnosis (radiographic interpretation)?
- Location (Localized/ generalized, Position/ epicenter, single/ multifocal)
- Extent , Size , Shape , Number
- Periphery, Shape (well defined, ill defined, circular, scalloped, irregular)
- Internal Architecture (radiopaque, radiolucent, mixed, septae, calcifications, etc)
- Effect on adjacent structures (teeth, lamina dura, PDL space, cortical bone, antrum, IAN, surrounding bone density)
What are the three types of benign structures?
- Cyst
- Vascular
- Neoplasia/tumor

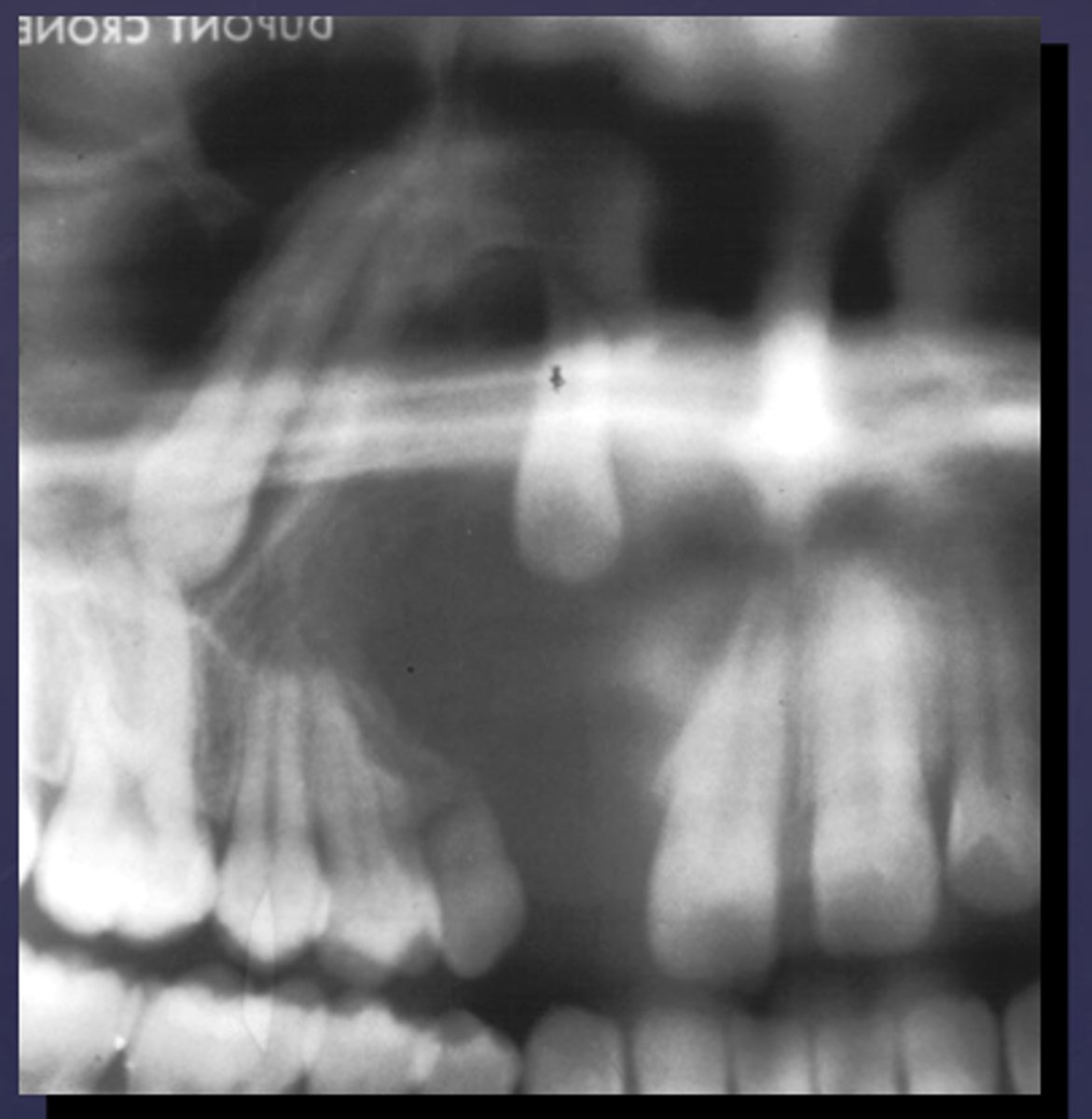
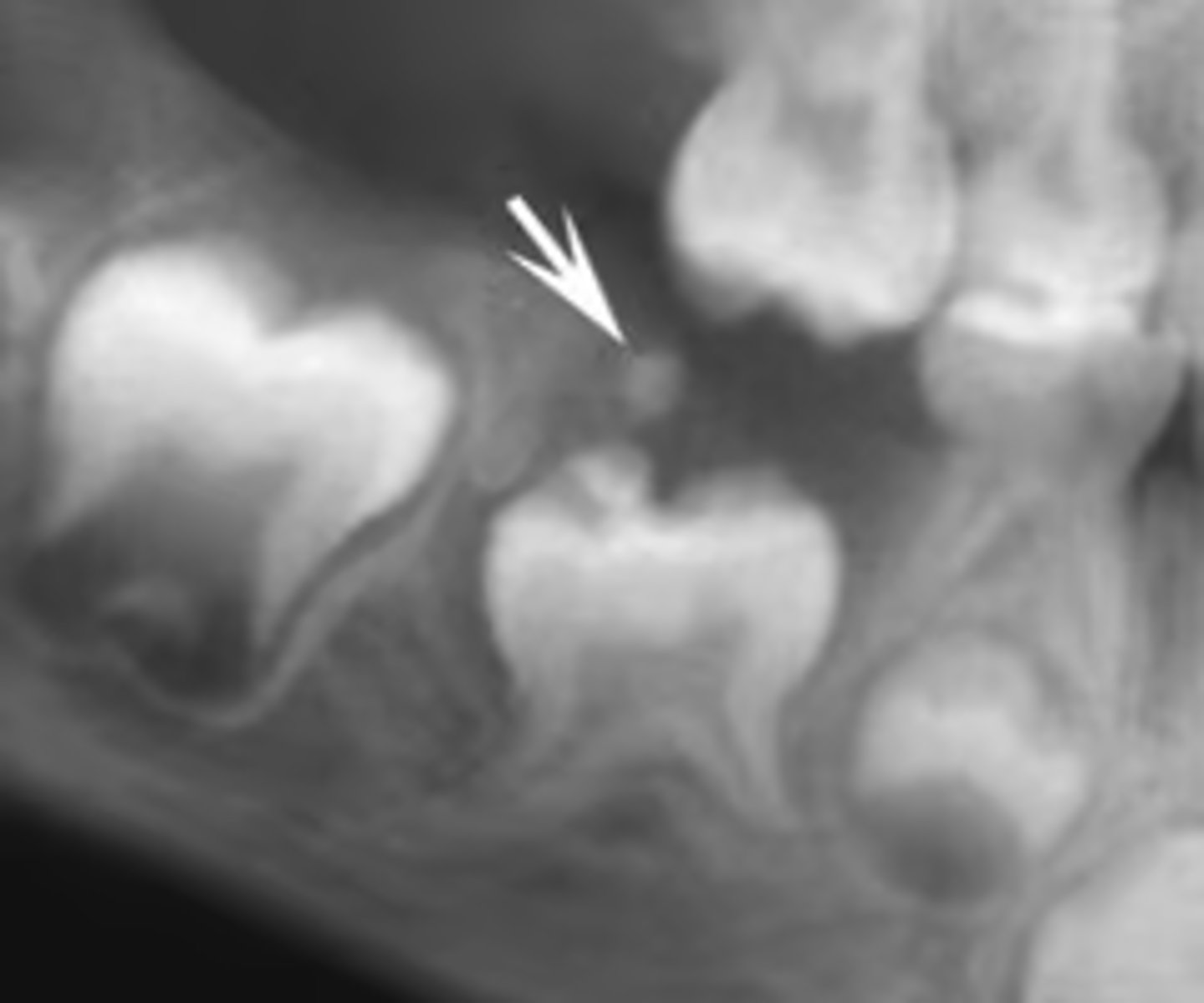
how would you describe this lesion? (not the giant cavity btw)
A. defined, corticated, periapical radiolucency causing loss of lamina dura and PDL space on #6-7
B. defined, non-corticated, periapical radiolucency causing loss of lamina dura and PDL space on #6-7
C. ill-defined, circular radiolucency located above tooth #7
D. well-defined, corticated, radiopacity
B. Defined, non-corticated, periapical radiolucency causing loss of lamina dura and PDL space on #6-7
- Also note epicenter located above apex # 7 which has large dental caries.

What category would this lesion be part of?
Inflammation/benign

all of the following could be a differential diagnosis for the following lesion EXCEPT?
A. radicular cyst
B. Periapical granuloma
C. apical rarefying osteitis
D. renal osteodystrophy
D. renal osteodystrophy

what category would this lesion be classified into?
inflammatory/benign cystic
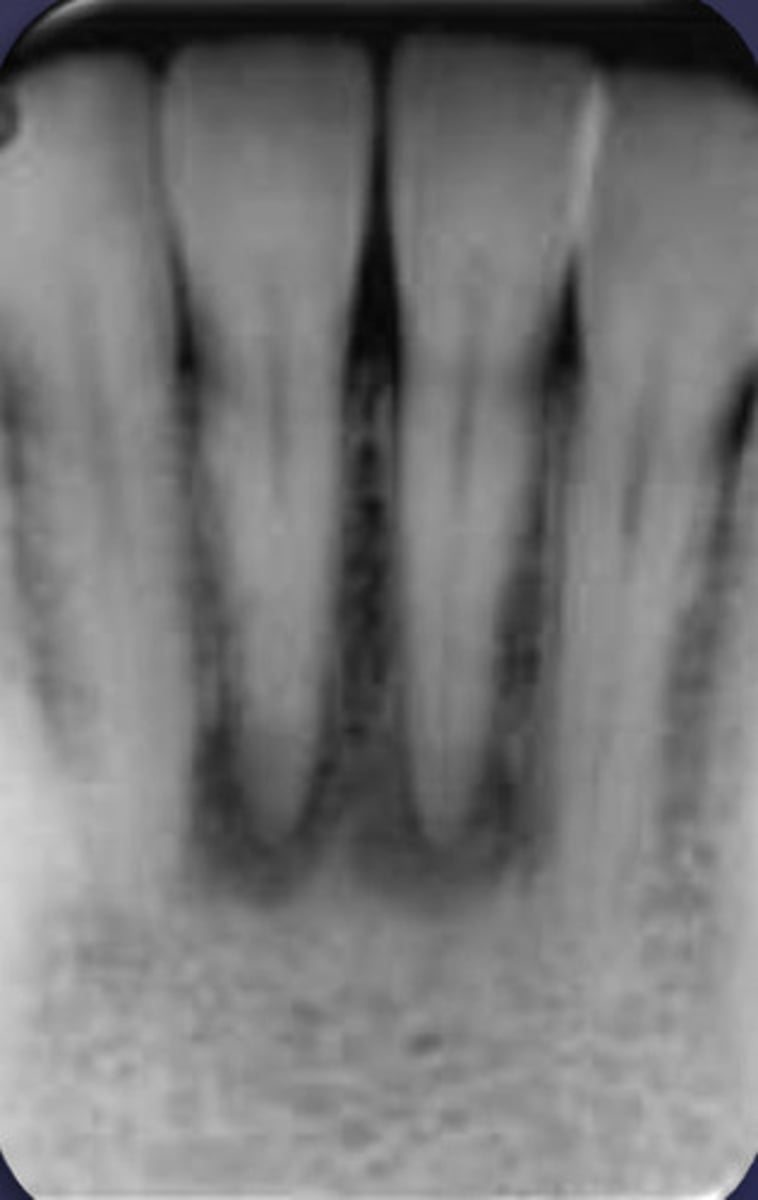
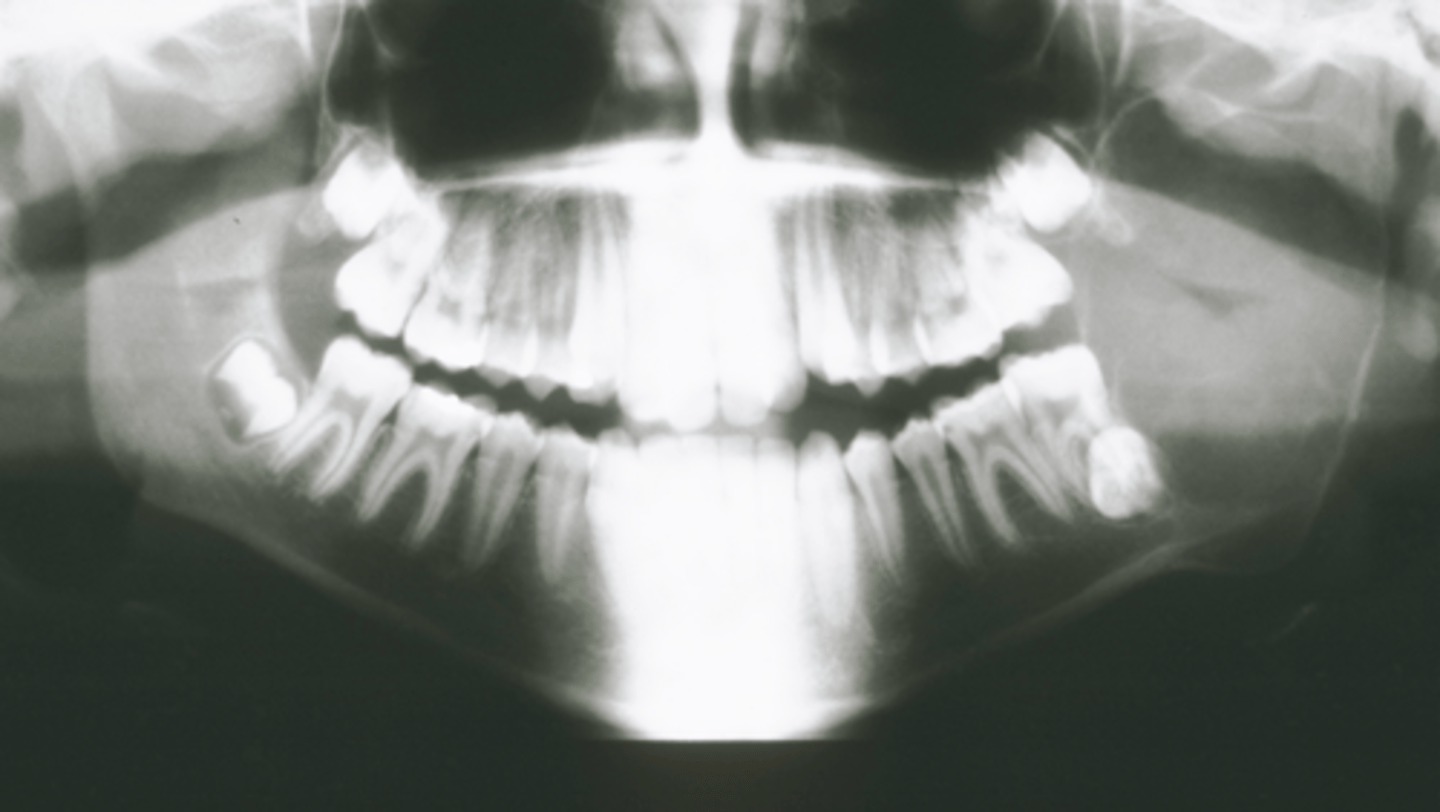
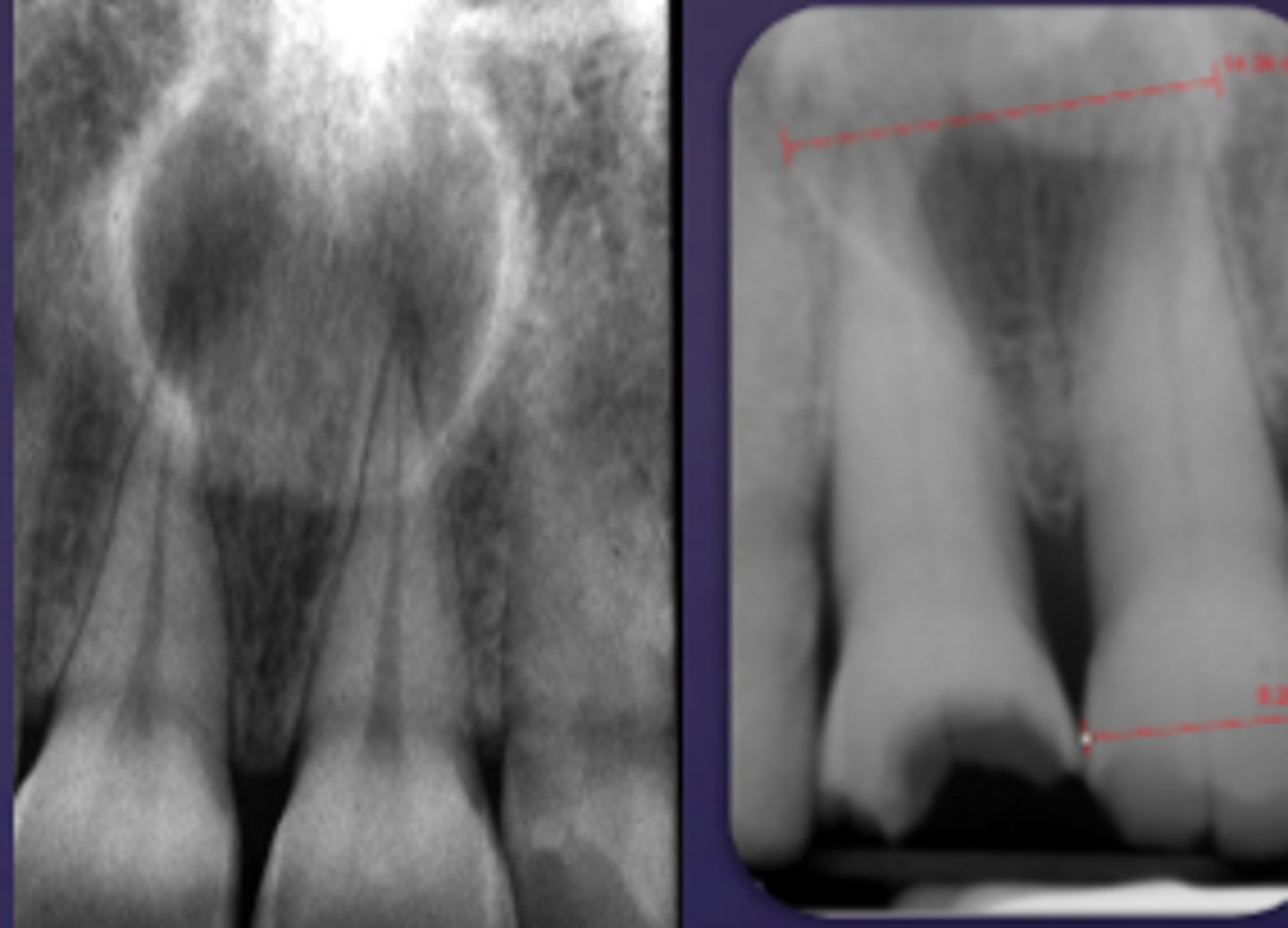
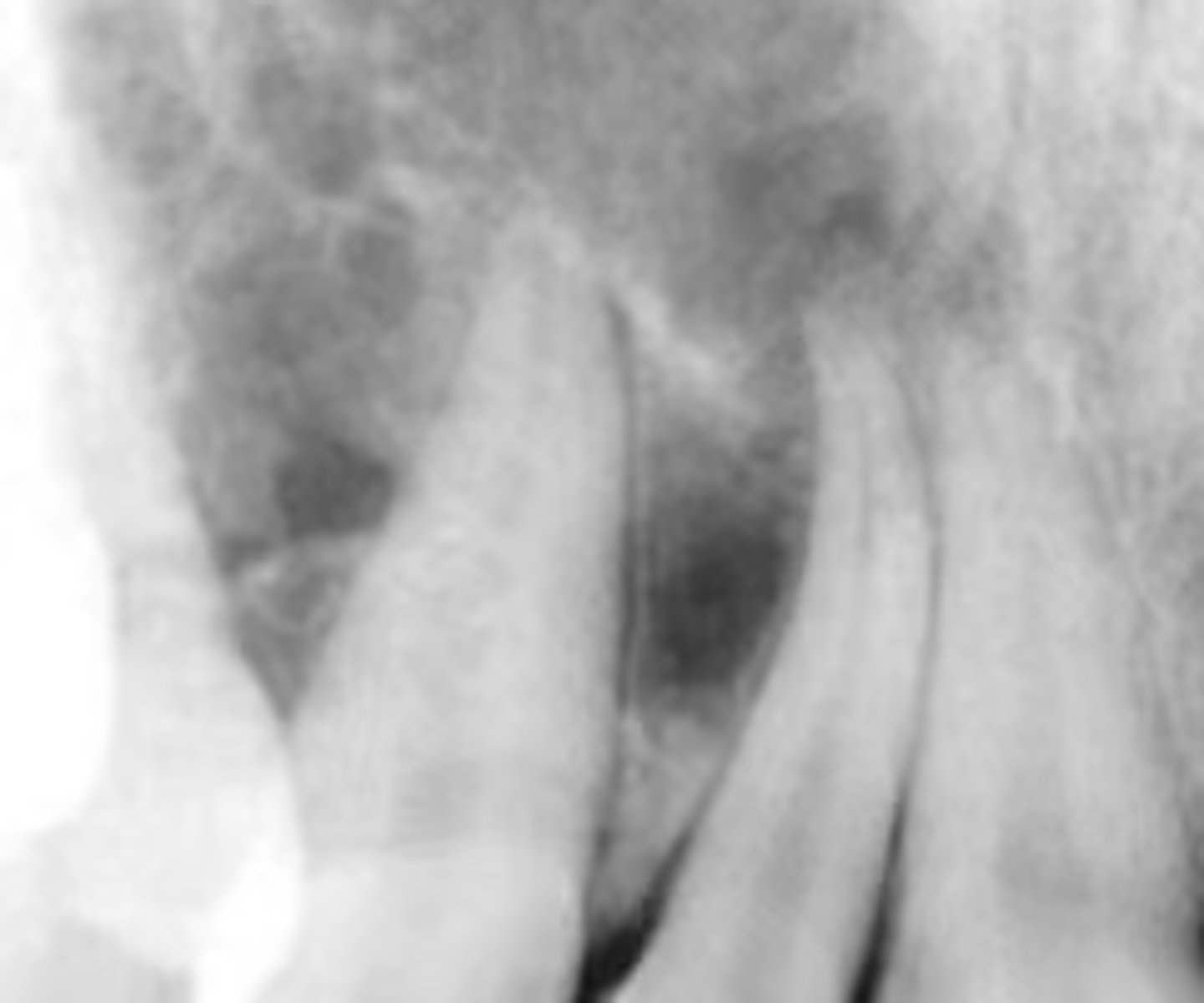
how would you describe this lesion?
A. well-defined, periapical radiolucent lesion associated with #24 and 25
B. ill-defined, periapical radiolucent lesion associated with #24 and 25
C. well- defined, multilocular periapical lesion associated with tooth number 24 and 25
D. mixed density, periapical lesion associated with teeth number 24 and 25
A. well-defined, periapical radiolucent lesion associated with #24 and 25
- Also note loss of apical lamina dura of 24, 25
What category would this lesion be part of?
Dysplasia

What would be a differential diagnosis for this lesion?
PCOD (stage 1)

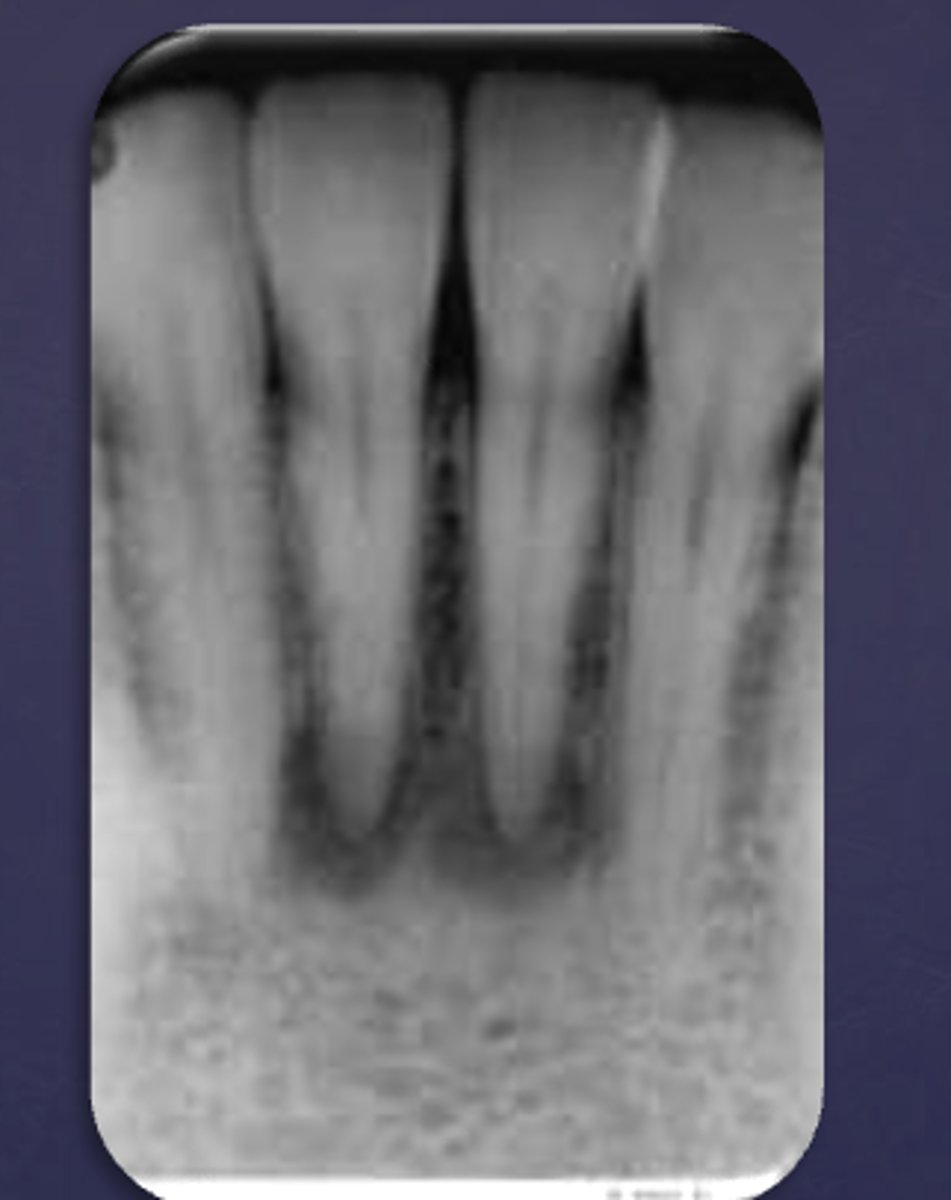
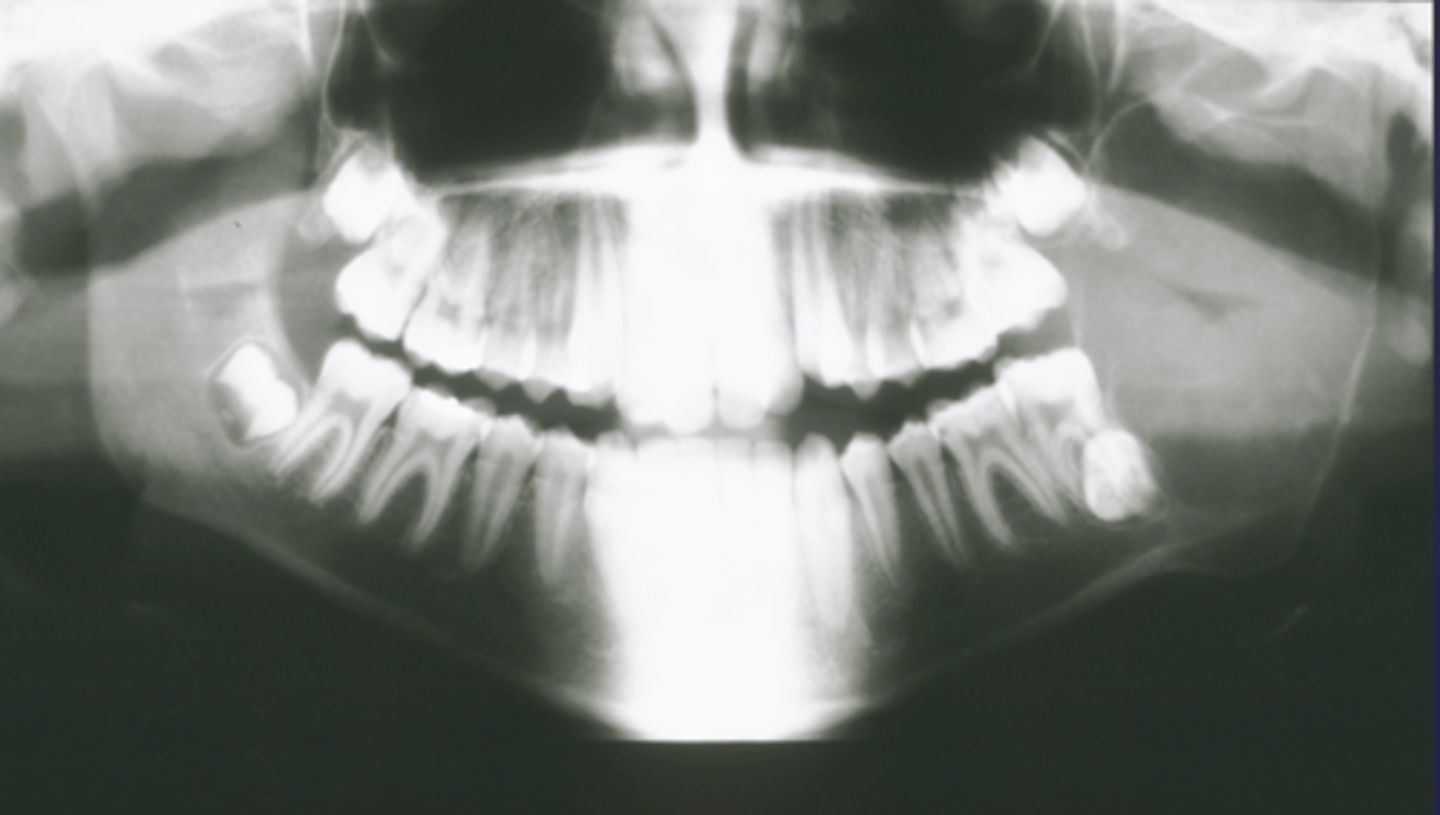
How would you describe the following lesion?
Multiple mixed density periapical target-like entities
The teeth are vital. What category would you put this lesion into?
dysplasia (PCOD)
what could be a differential diagnosis for this lesion?
A. radicular cyst
B. periapical granuloma
C. PCOD (stages 2/3)
D. apical rarefying osteitis
C. PCOD (stages 2/3)

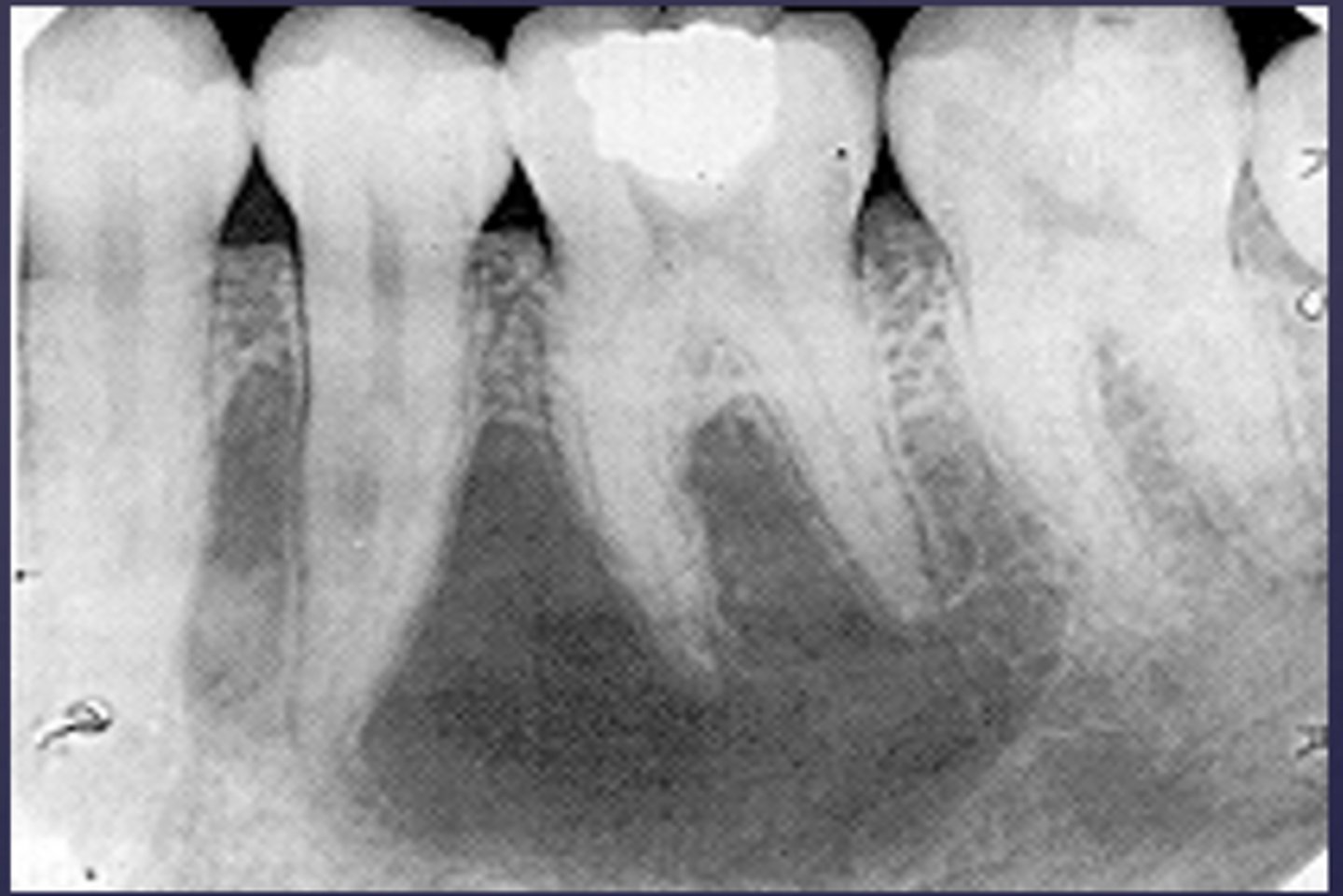
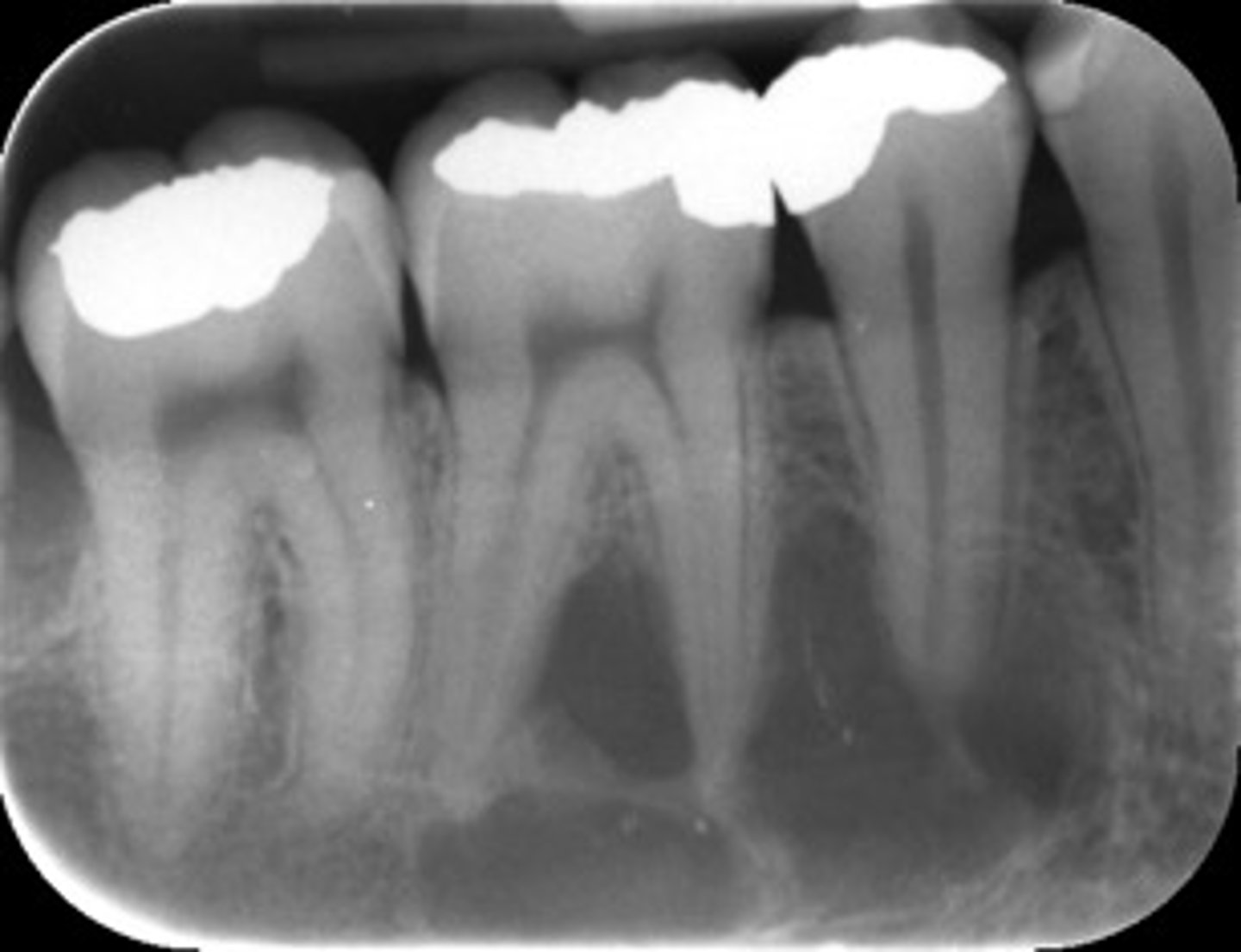
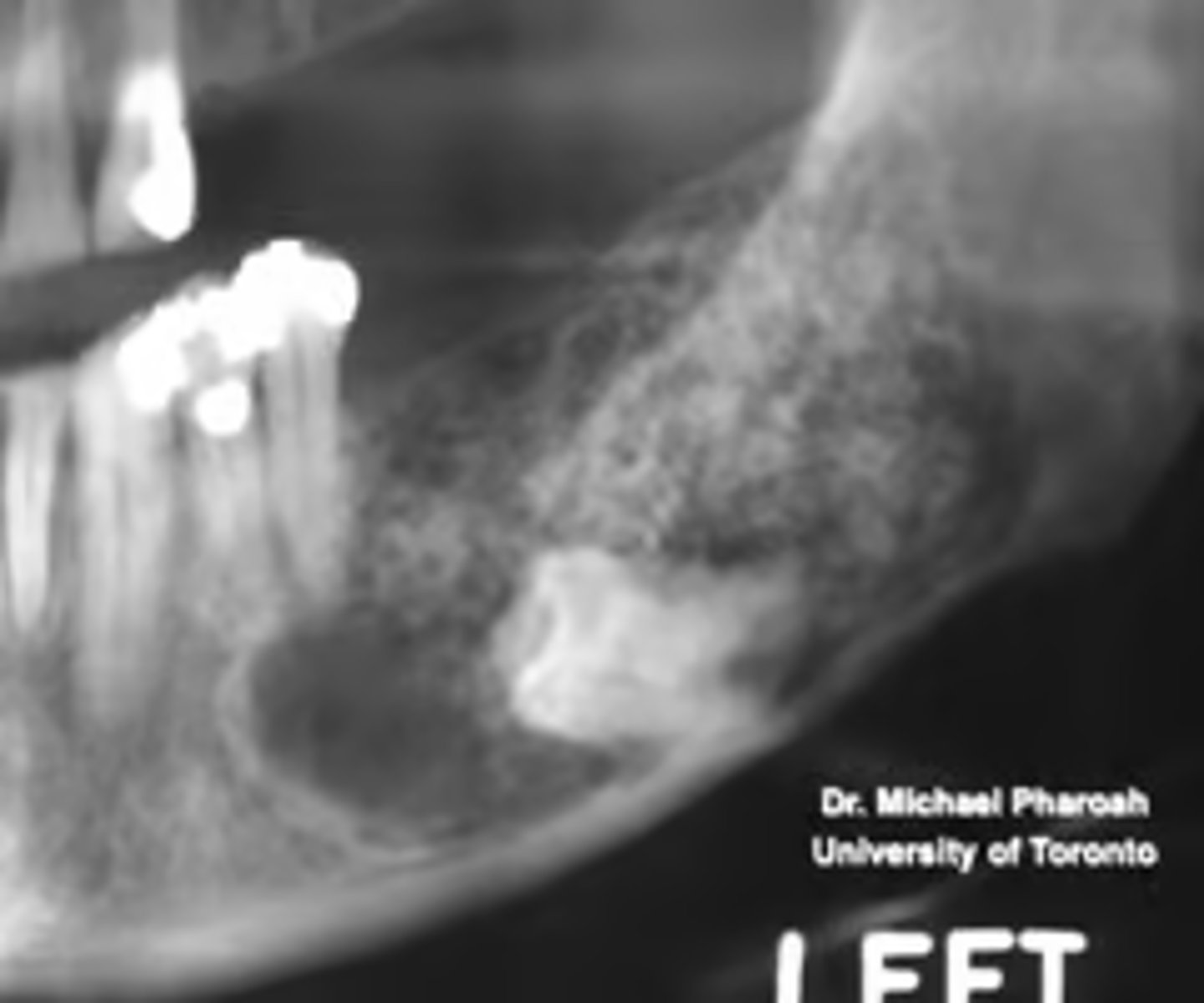
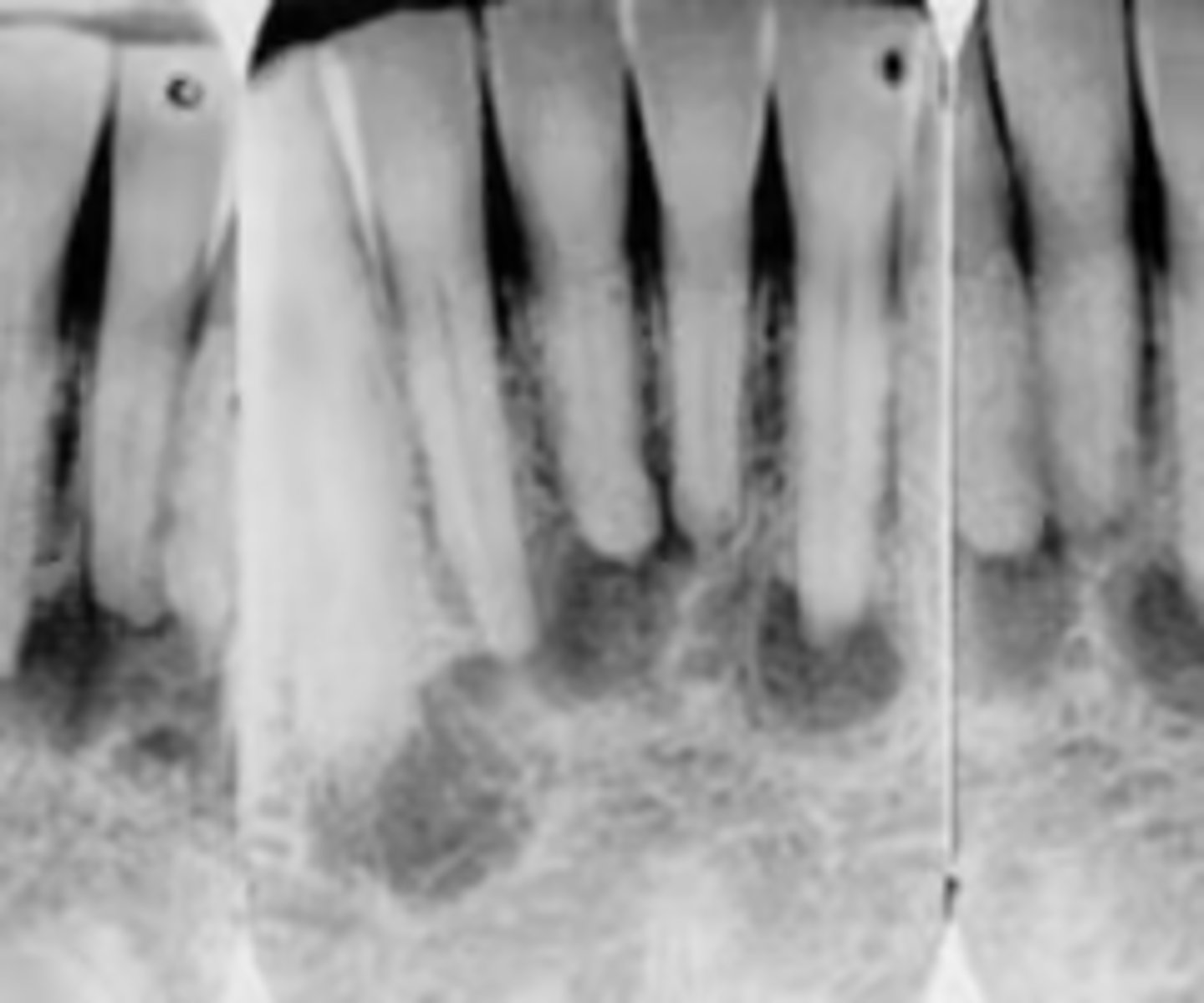
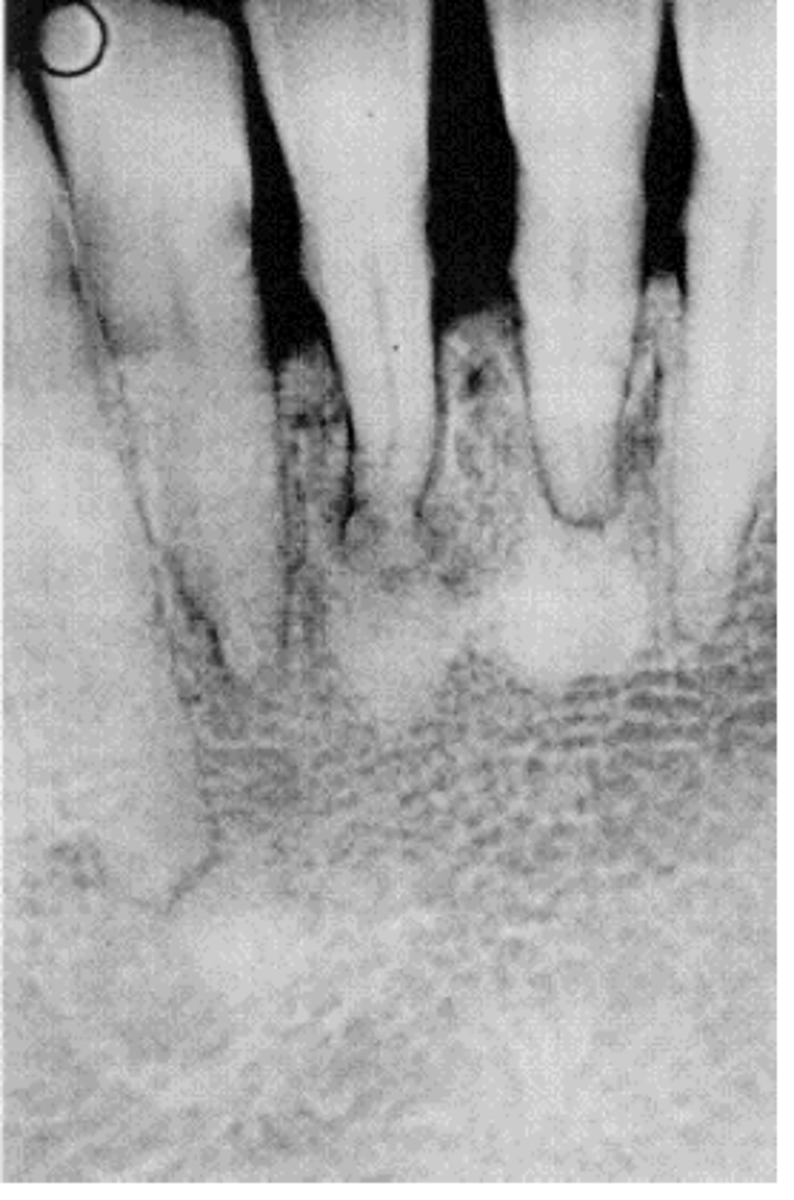
How would you describe the lesion?
- Periapical radiolucency associated with #30
- Has a band of sclerotic change extending from the apical radiolucency to the inferior alveolar canal and beyond
- Furcation involvement
(Furcation involvement as well as a band of sclerotic change extending from the apical radiolucency to the inferior alveolar canal and beyond)

What category would you put this lesion into?
Inflammation

what could be a differential diagnosis for this lesion? (select all that apply)
A. PCOD
B. multiple myeloma
C. apical rarefying osteitis
D. chronic sclerosing osteomyelitis
C. apical rarefying osteitis
D. chronic sclerosing osteomyelitis
Also note apical rarefying osteitis #14 ( remnant root fragments, no crown due to caries)

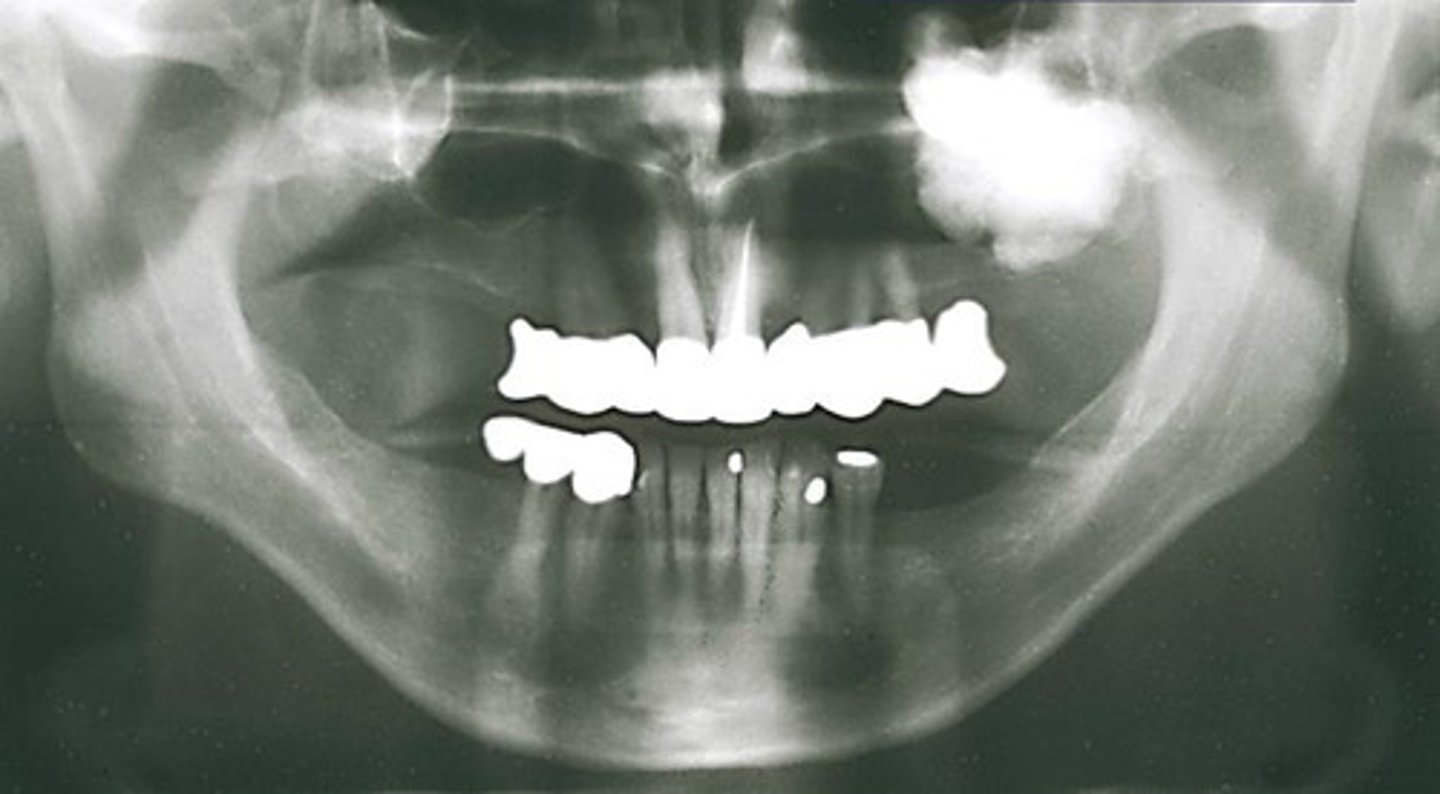
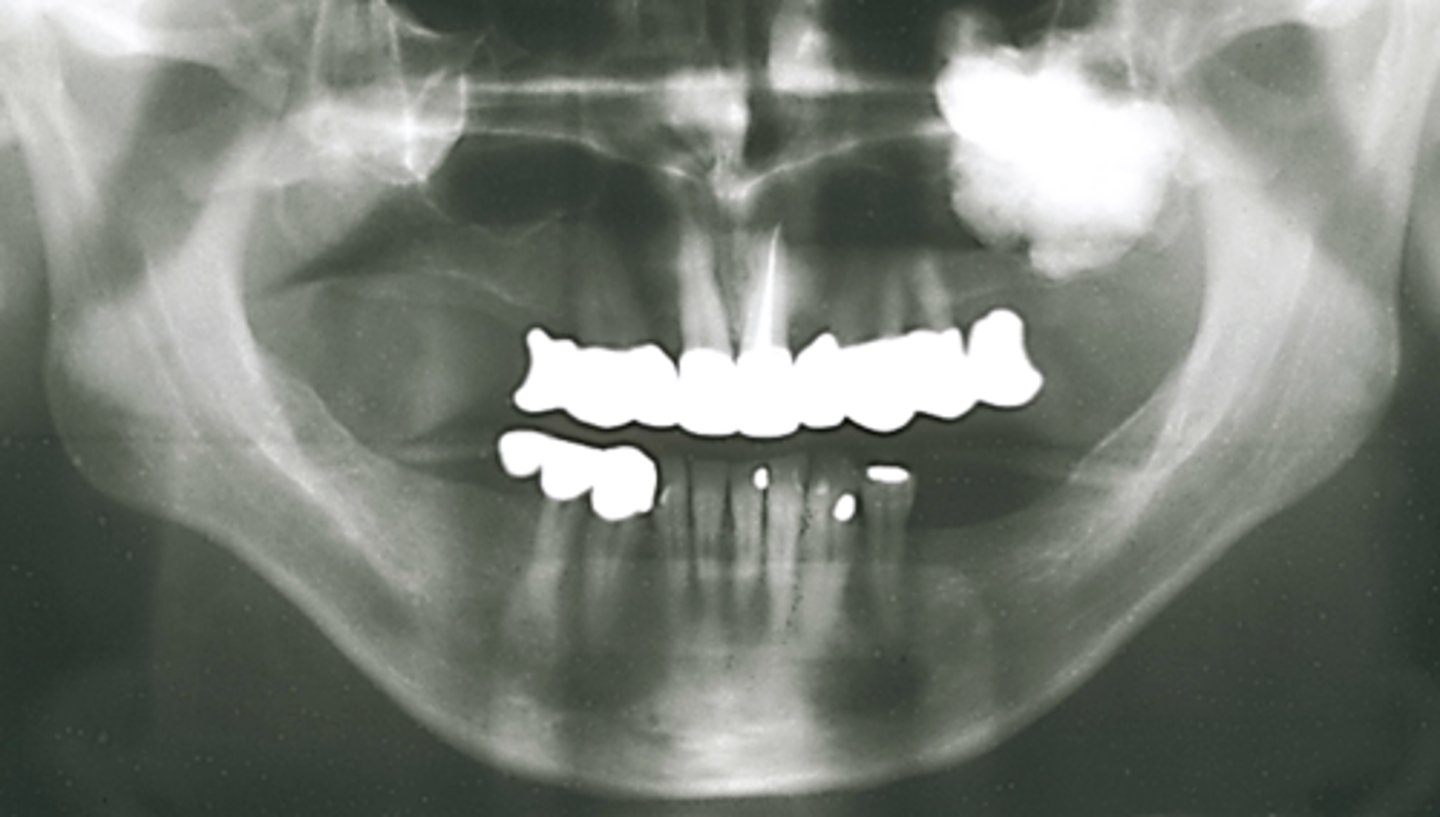
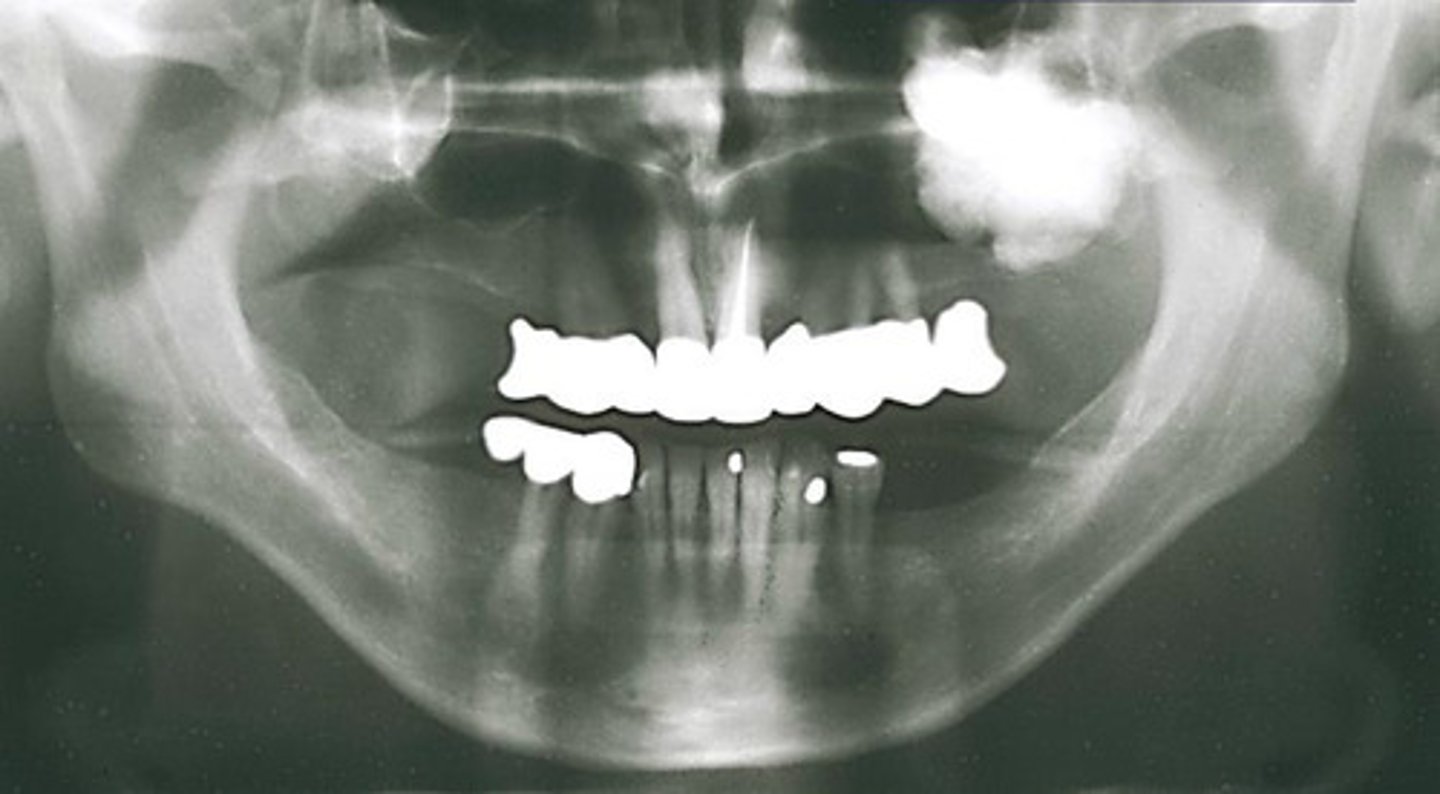
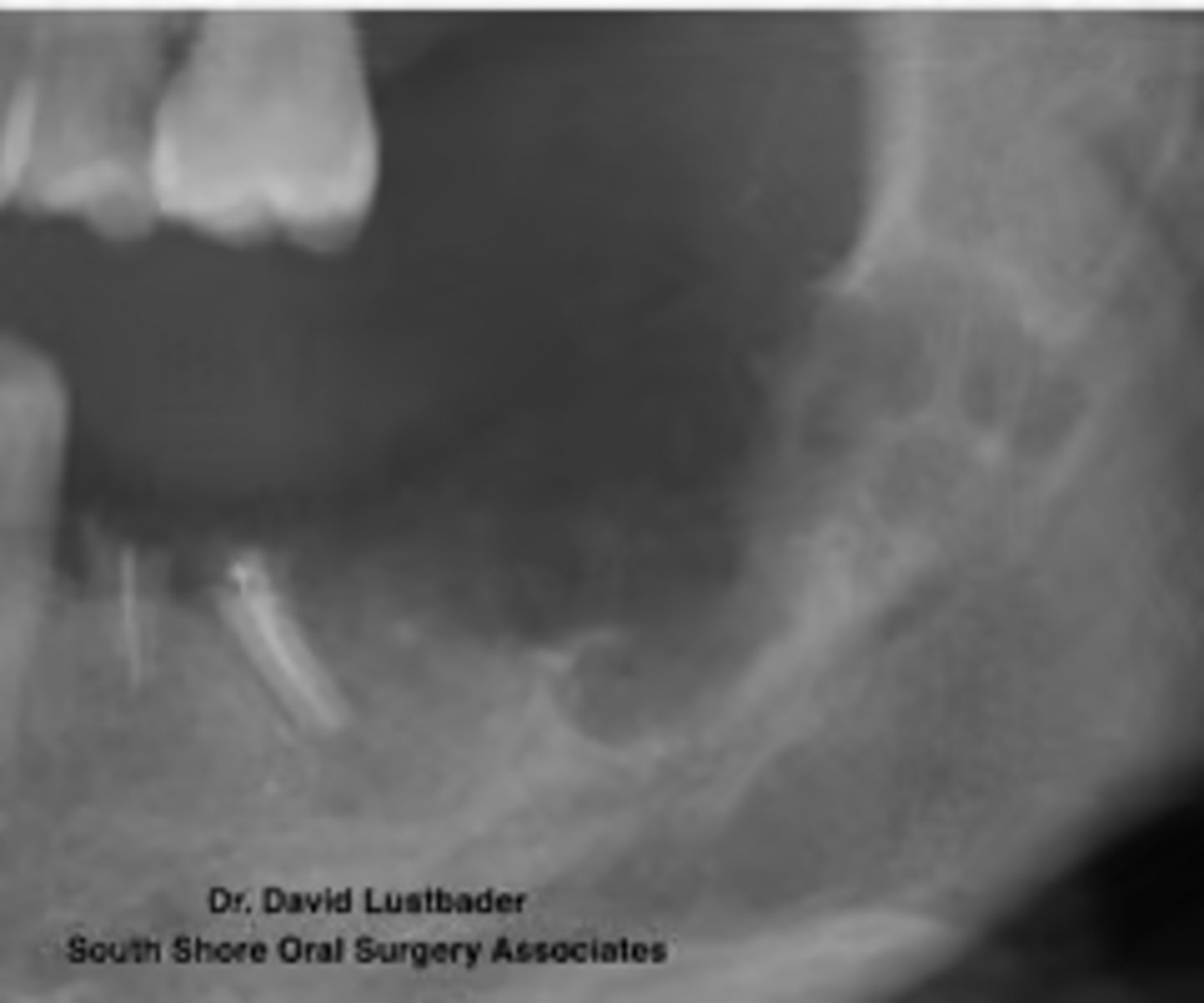
How would you describe the lesion?
- Ill-defined, moth eaten area in the posterior mandible
- How would you describe the lesion?

What category would you put this lesion into?
malignant

all of the following could be a differential diagnosis for this lesion except?
A. squamous cell carcinoma
B. multiple myeloma
C. osteogenic sarcoma
B. multiple myeloma

How would you describe the lesion?
- Ill-defined moth eaten area in the posterior mandible
- Radiopacities extending beyond the mandibular borders.

what category would you put this lesion into?
malignant

What would be a differential diagnosis for this lesion?
- Osteogenic sarcoma
- Squamous cell CA

how would you describe the lesion?
A. well-defined, corticated, pericoronal radiolucency associated with tooth number 7
B. well-defined, non coritcated periapical lesion associated with tooth number 6
C. ill-defined, corticated periapical lesion associated with tooth number 6
D. ill-defined, corticated periapical lesion associated with tooth number 5
A. well-defined, corticated, pericoronal radiolucency associated with tooth number 7
(root resorption also seen)

What category would you put this lesion into?
Benign odontogenic tumor/cyst
What would be a differential diagnosis for this lesion?
- AOT
- Calcifying Epithelial Odontogenic Tumor (Pindborg tumor)
- Calcifying Epithelial Odontogenic Cyst( Gorlins cyst)

how would you describe the lesion?
A. well-defined, non corticated, periapical radiolucency associated with tooth number 14
B. ill-defined, non corticated, periapical radiolucency associated with tooth number 14
C. well-defined, corticated, pericoronal lesion with radiopaque flecks associated with an impacted tooth
D. well-defined, corticated, pericoronal radiopacity associated with an impacted tooth
C. well-defined, corticated, pericoronal lesion with radiopaque flecks associated with an impacted tooth

What category would you put this lesion into?
Benign odontogenic tumor/cyst

all of the following could be a differential diagnosis for this lesion except?
A. AOT
B. calcifying epithelial odontogenic tumor (pindborg tumor)
C. Calcifying Epithelial odontogenic cyst (gorlin cyst)
D. osteosarcoma
D. osteosarcoma
How would you describe the lesion?
- Defined corticated pericoronal radiolucency associated with #32, that is unerupted
- The borders are continuous with the distal follicular space.
what category would you put this lesion into?
Benign odontogenic cyst
What would be a differential diagnosis for this lesion?
- Dentigerous cyst
- OKC
- Ameloblastoma

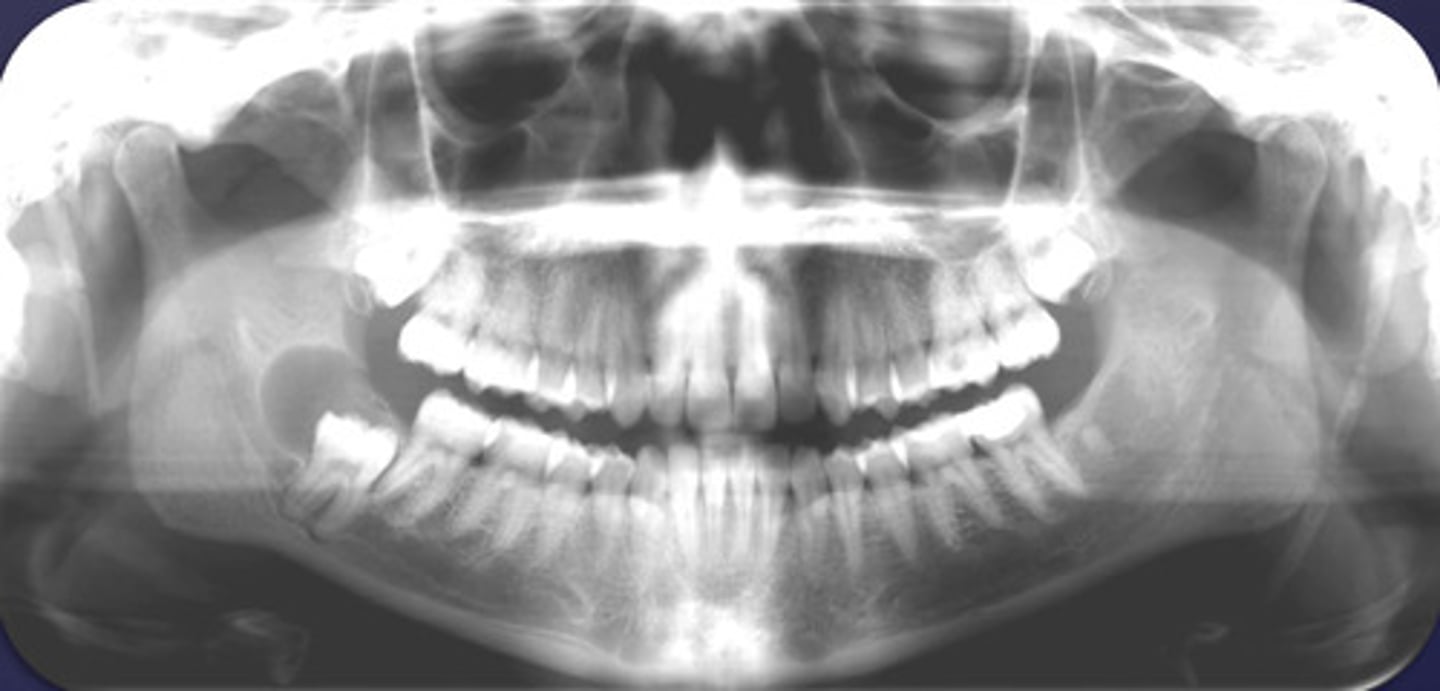
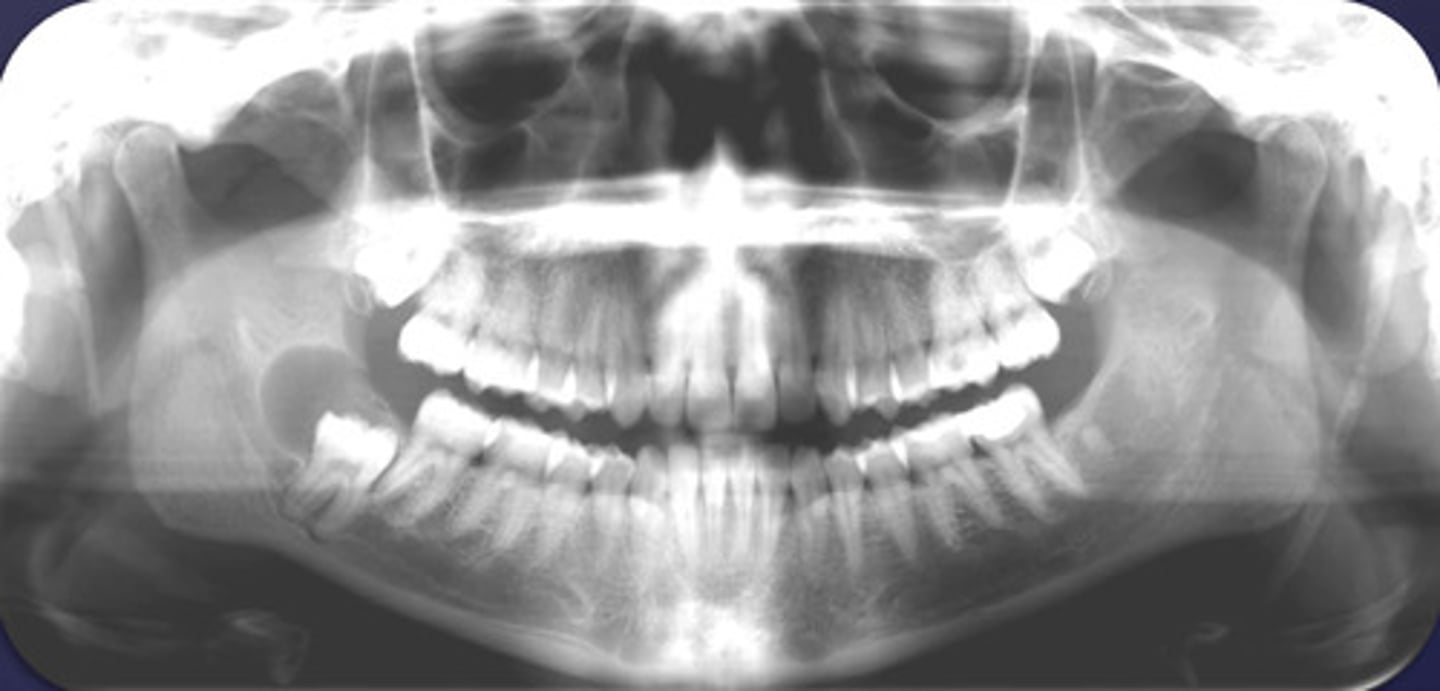
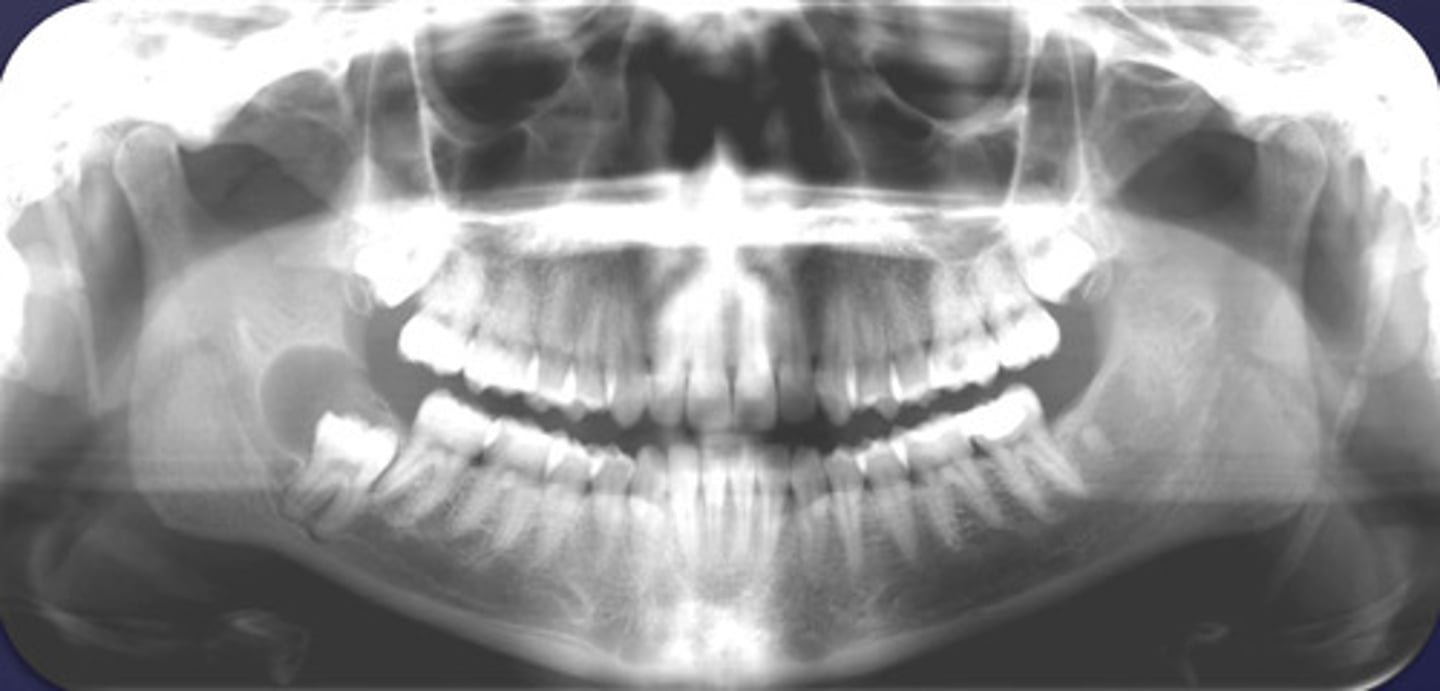
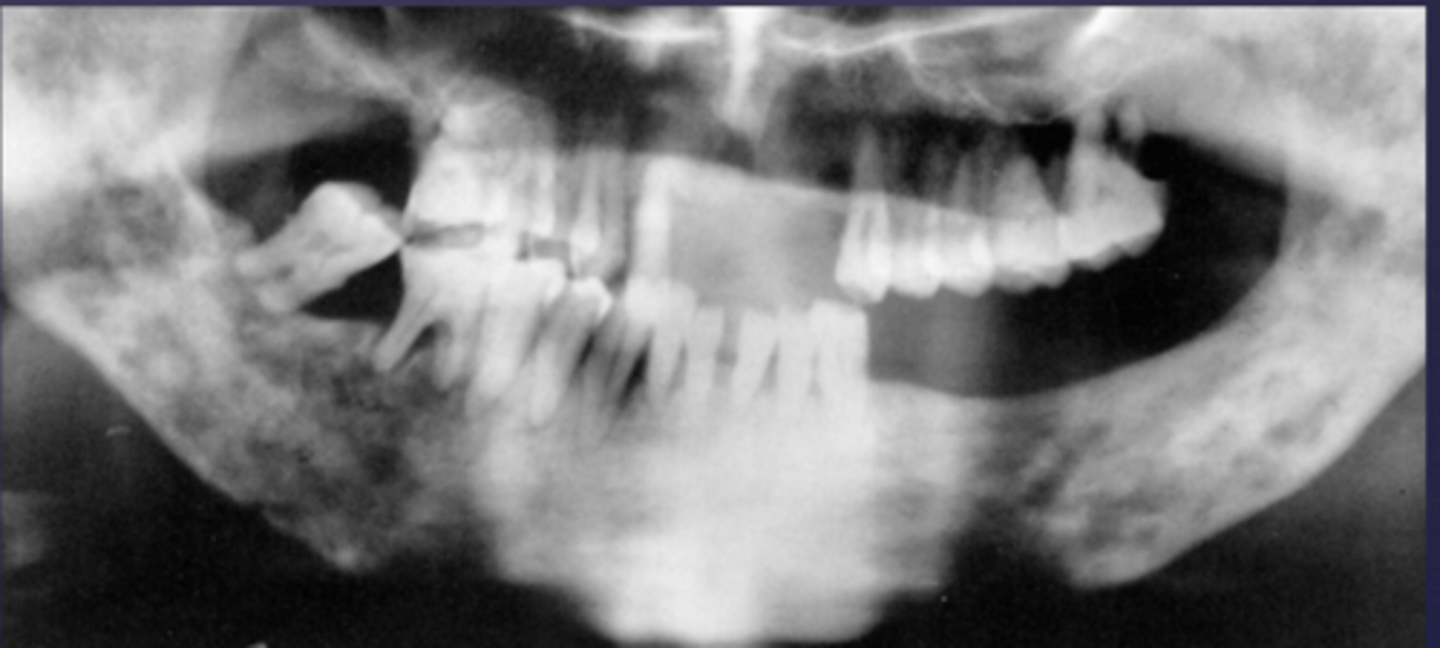
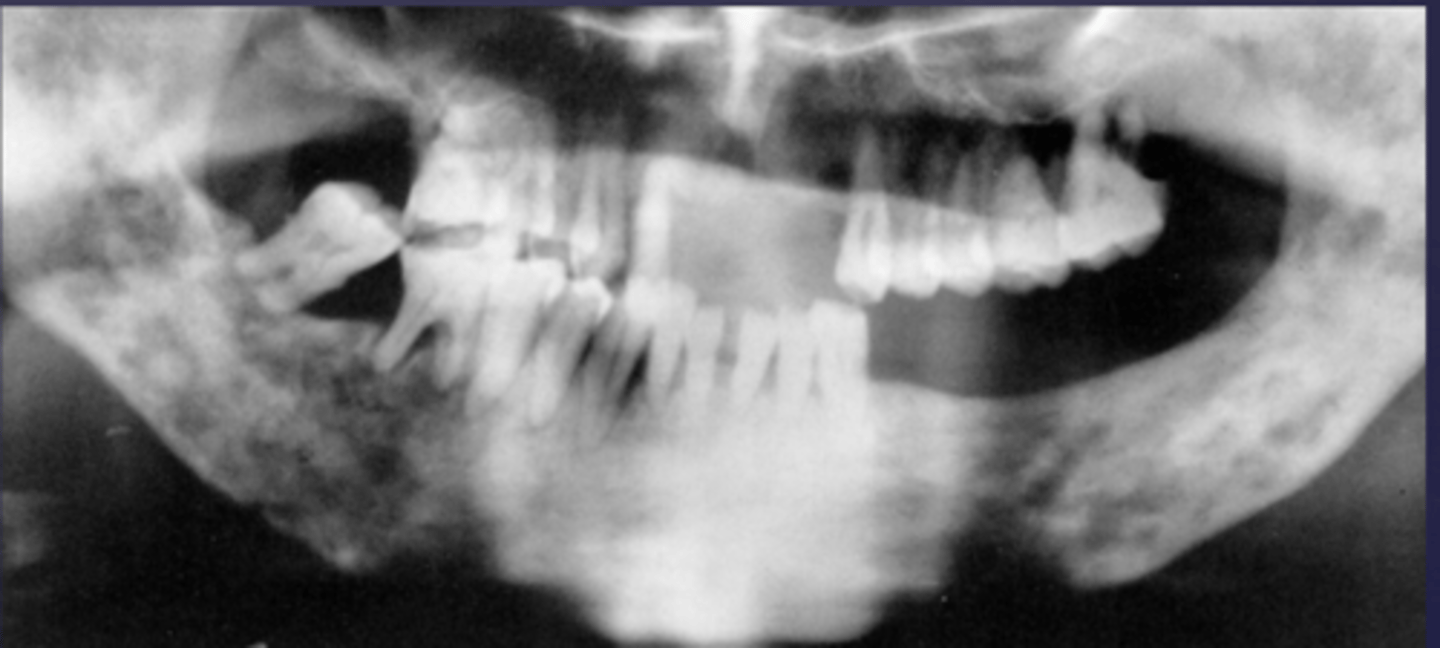
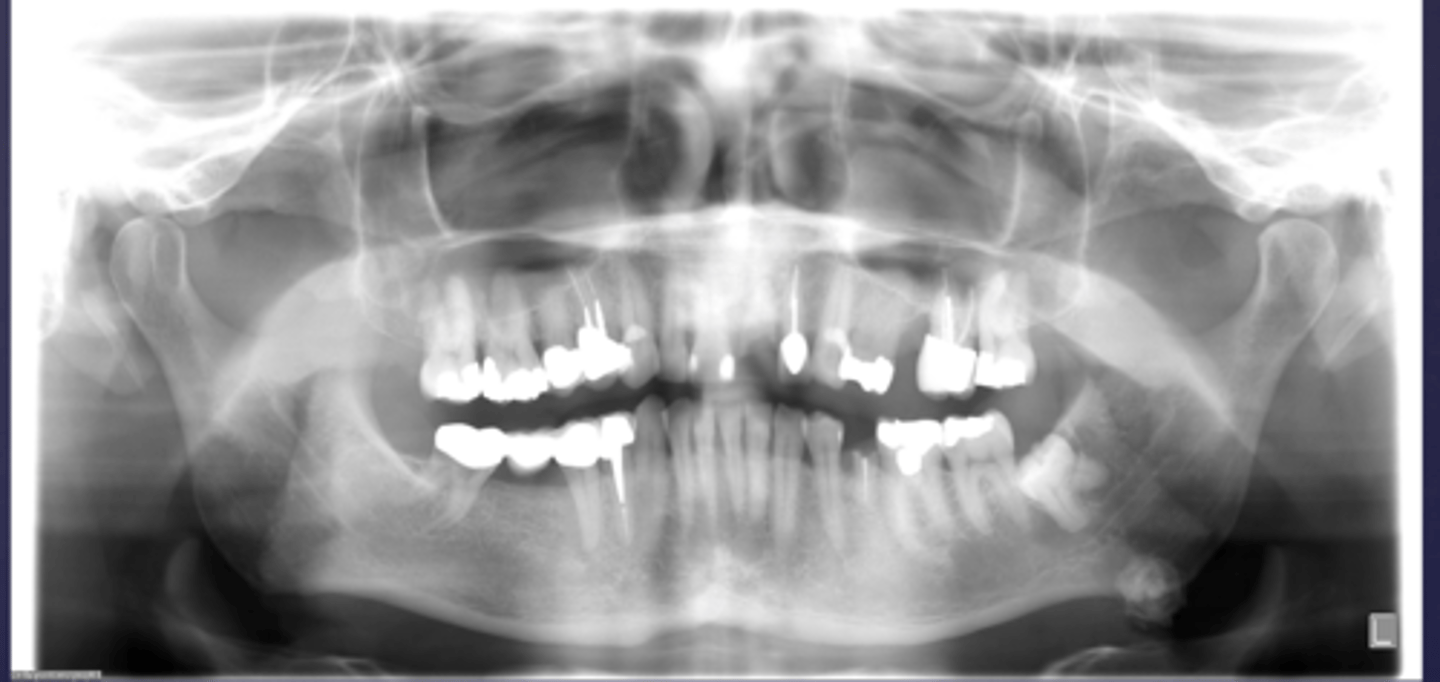
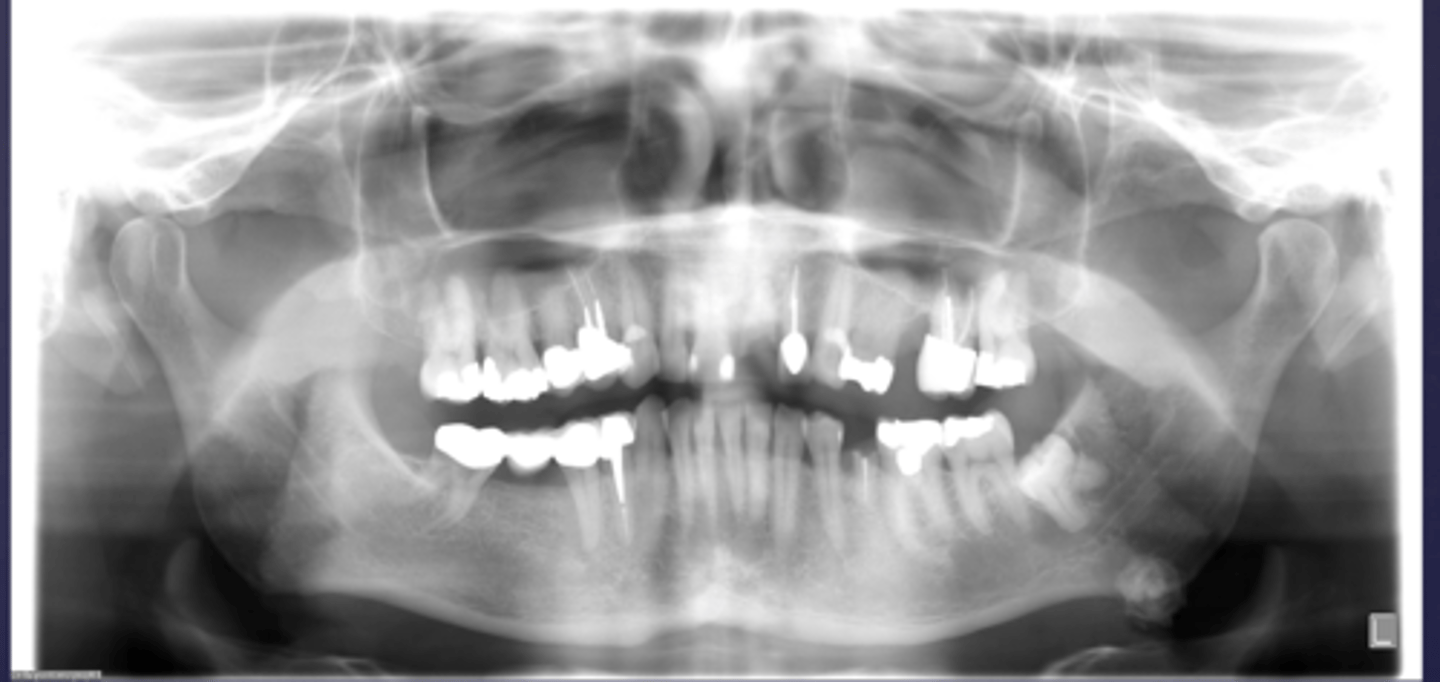
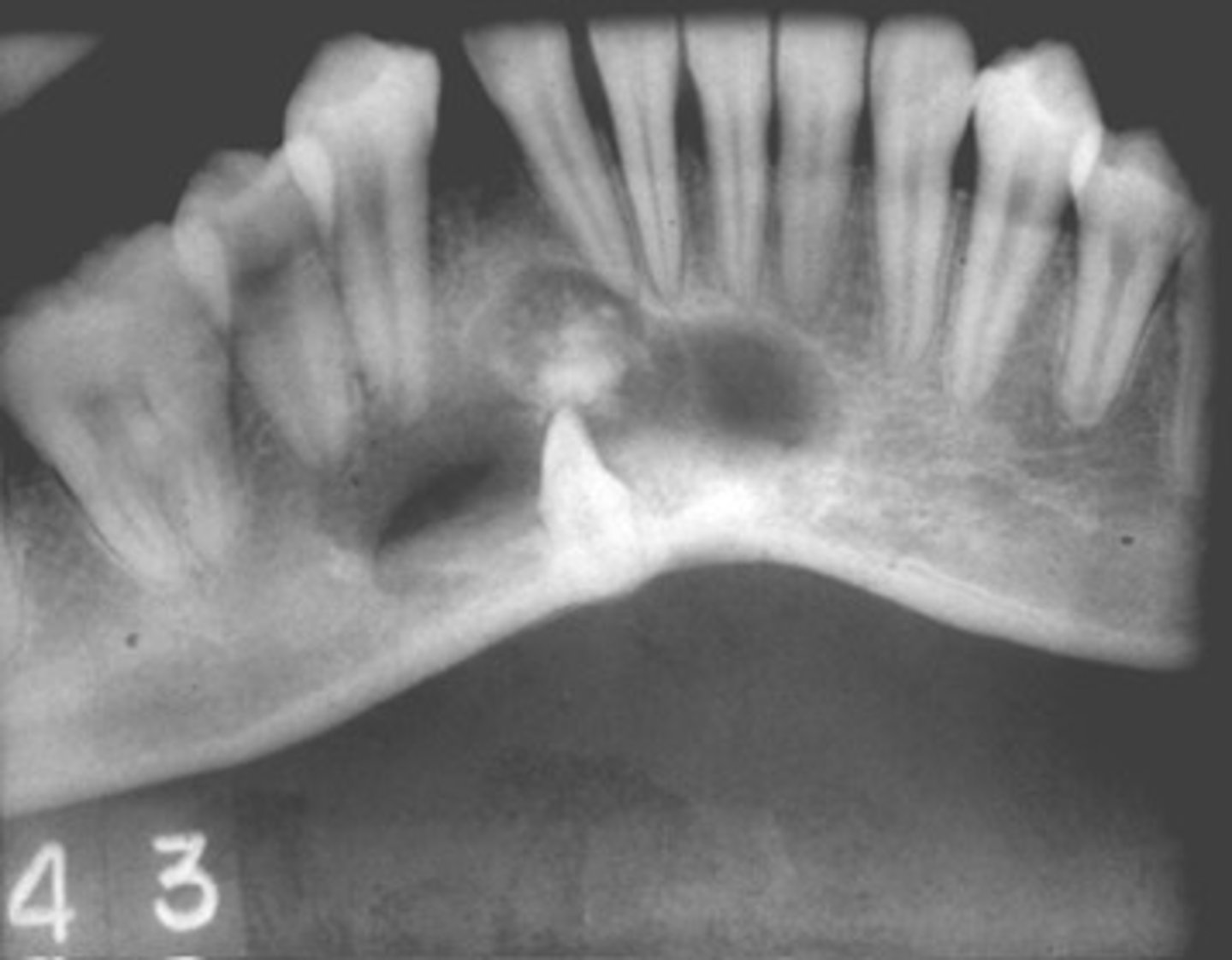
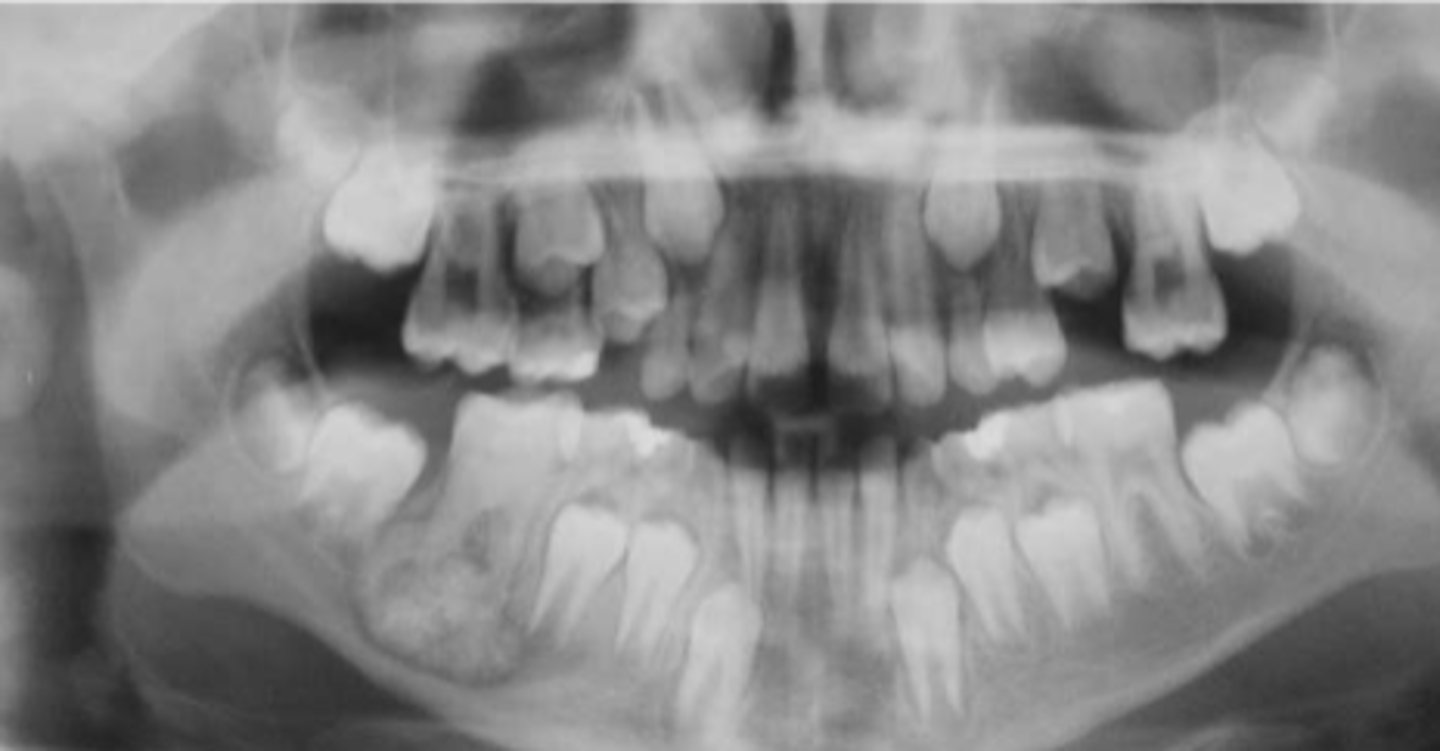
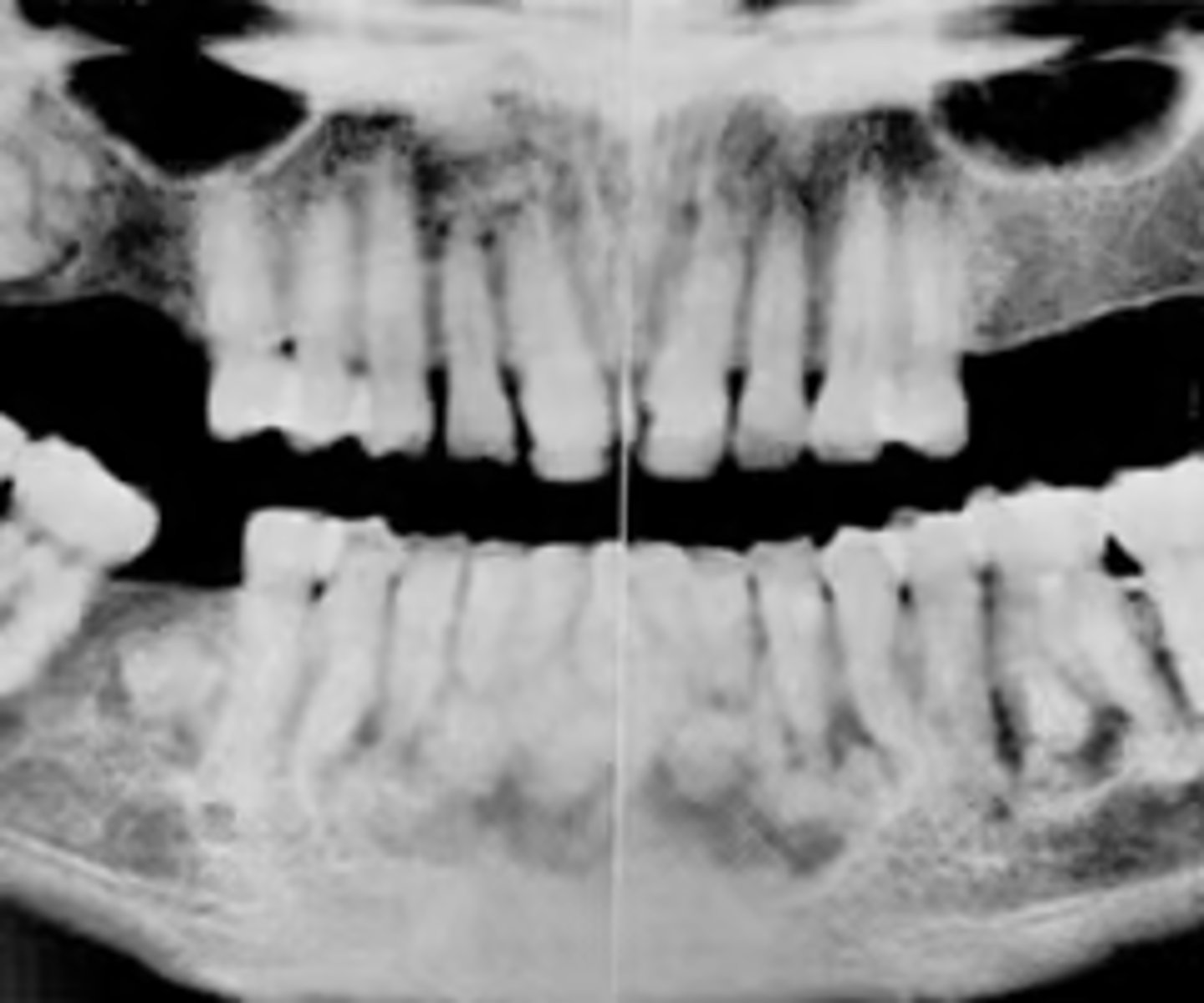
How would you describe the lesion?
- Generalized reduced trabecular bone density in maxilla and mandible
- The teeth appear to be more prominent with the lacking osseous support. Lamina dura not very distinct in multiple locations.
- There are two large defined radiolucencies located in the posterior mandible
- The right side radiolucency is causing thinning of the inferior mandibular cortex and displacement of inferior alveolar canal
- There is wispy septae noted within
- The left mandibular lesion appears to be defined but scooped out along the alveolar crest

What category would this lesion be part of?
Systemic

What would be a differential diagnosis for this lesion?
Hyperparathyroidism (brown tumor)

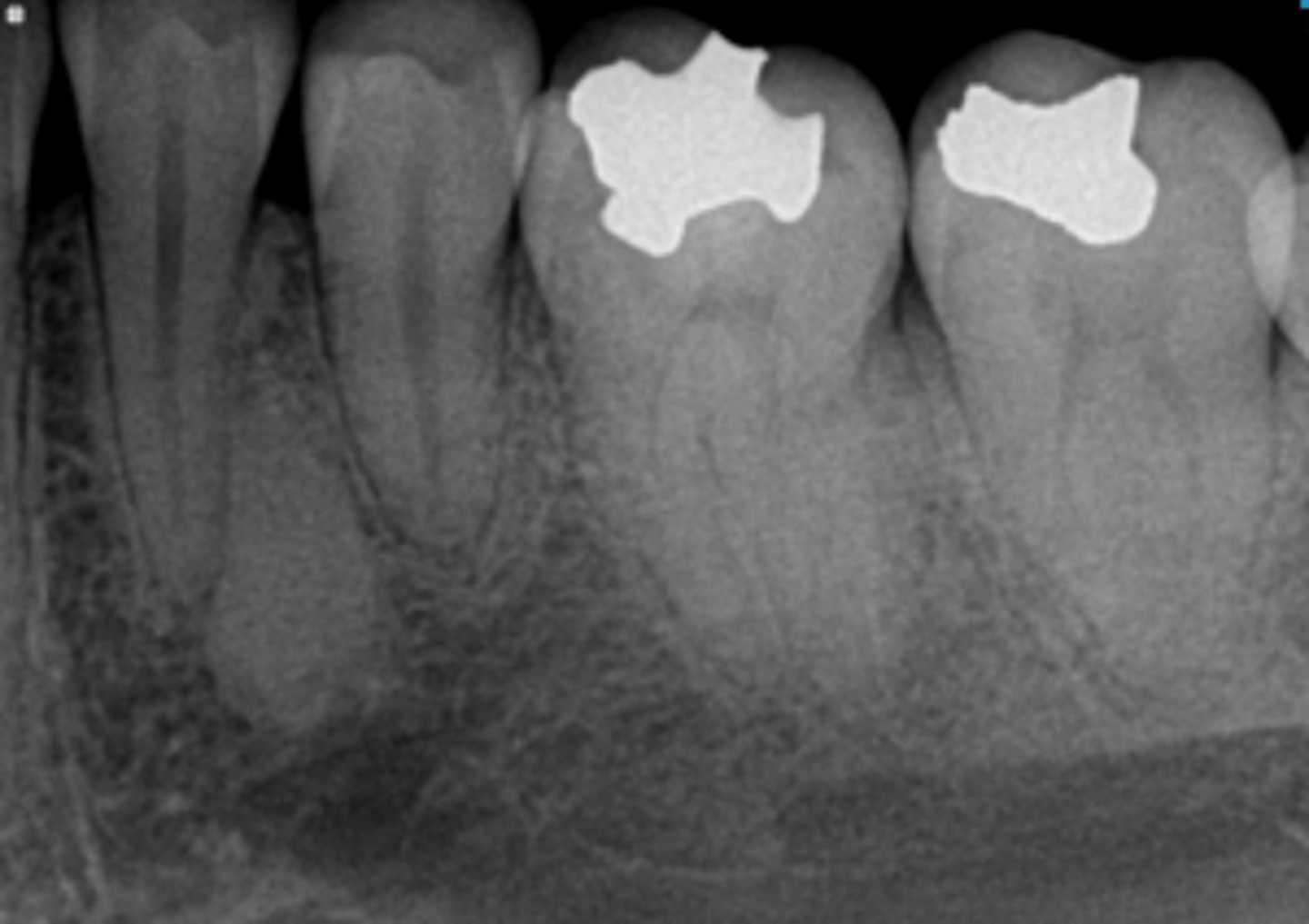
How would you describe the lesion?
- Well defined
- Corticated radiolucent lesion around the roots of #19-20
- Lamina dura of teeth are intact, some thinning noted
- The lesion scallops superiorly between roots
- No effect on teeth noted
What category would this lesion be part of?
Developmental/benign

What would be a differential diagnosis for this lesion?
- Simple bone cyst
- Traumatic bone cyst (scalloping)
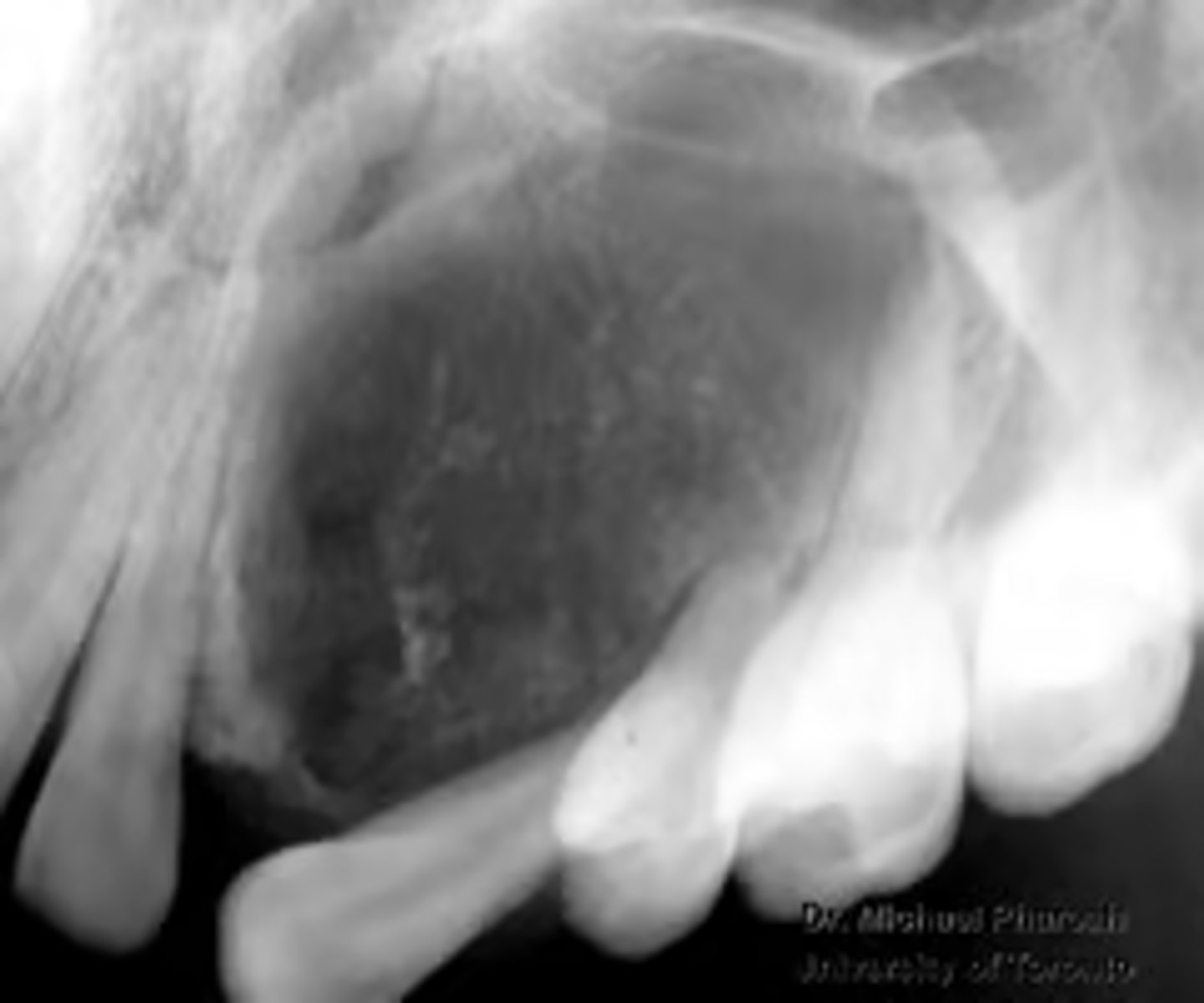
How would you describe the lesion?
- Well-defined
- Dense homogeneous radiopacity, within the left maxillary sinus and the edentulous left posterior maxillary alveolus
- The floor of the left sinus can be visualized just inferior to the entity
- No inferior expansion into oral cavity noted
What category would this lesion be part of?
Benign
What would be included in your D/D?
Osteoma in the left maxillary sinus. Complex odontoma very low on the DD as the entity is within sinus.
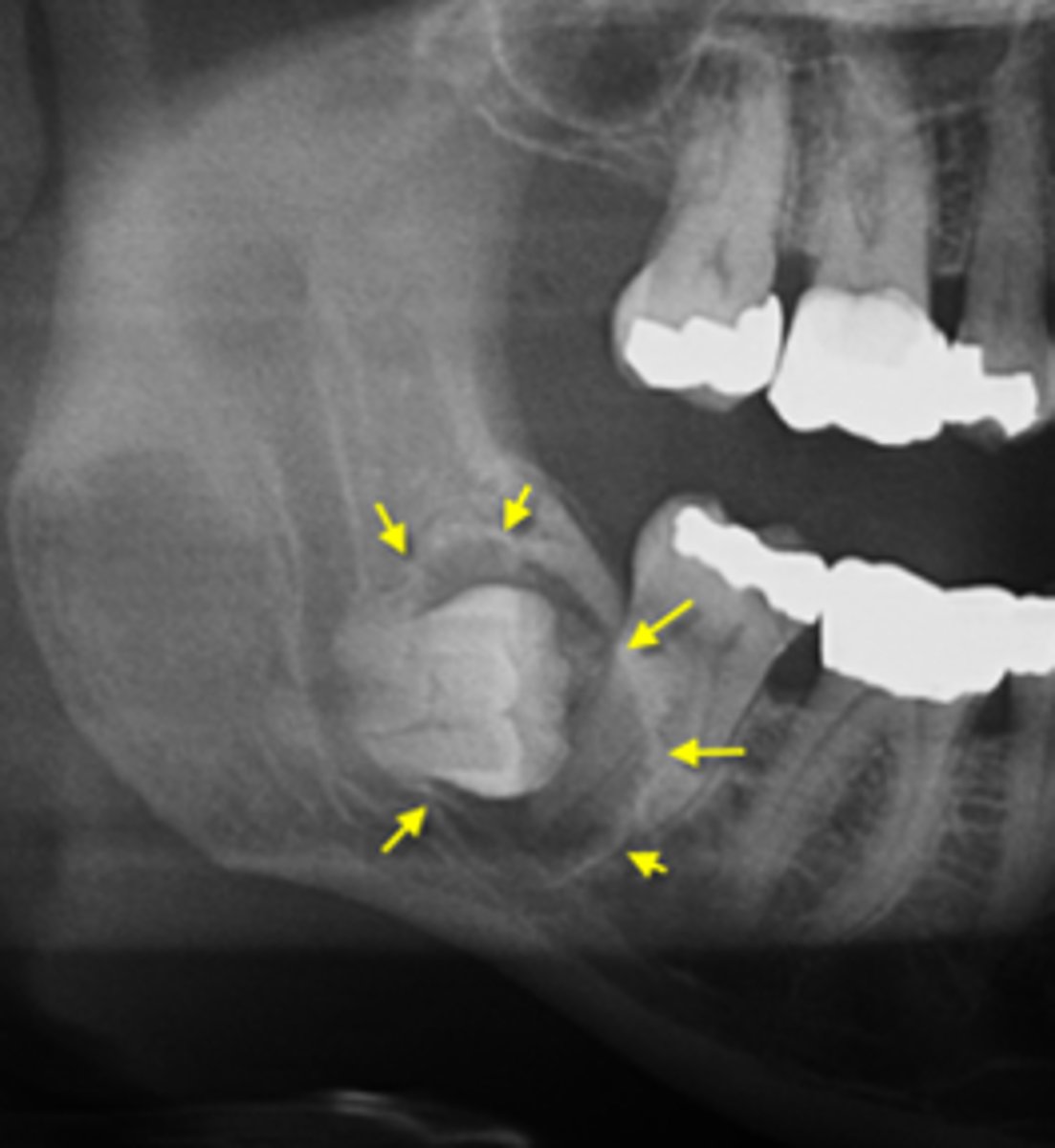
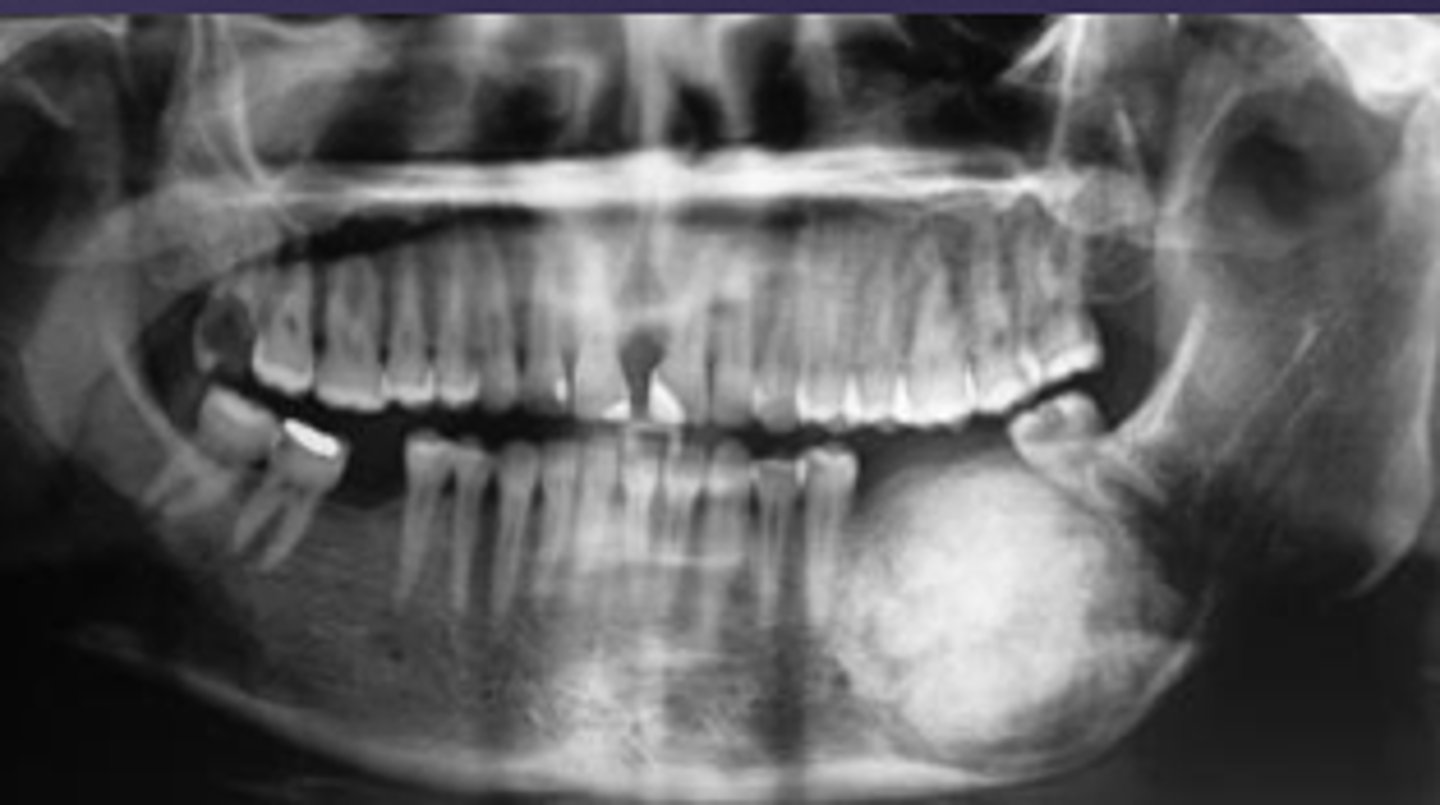
How would you describe the lesion?
- Well-defined corticated unilocular radiolucency in the left ramus causing expansion and thinning of
anterior and posterior walls of ramus, inferiorly below the inferior mandibular cortex and the coronoid process
- Dispalcement of the developing third molar.
What category would this lesion be part of?
Benign
What would be included in your D/D?
- OKC
- Unicystic ameloblastoma
- Dentigerous cyst

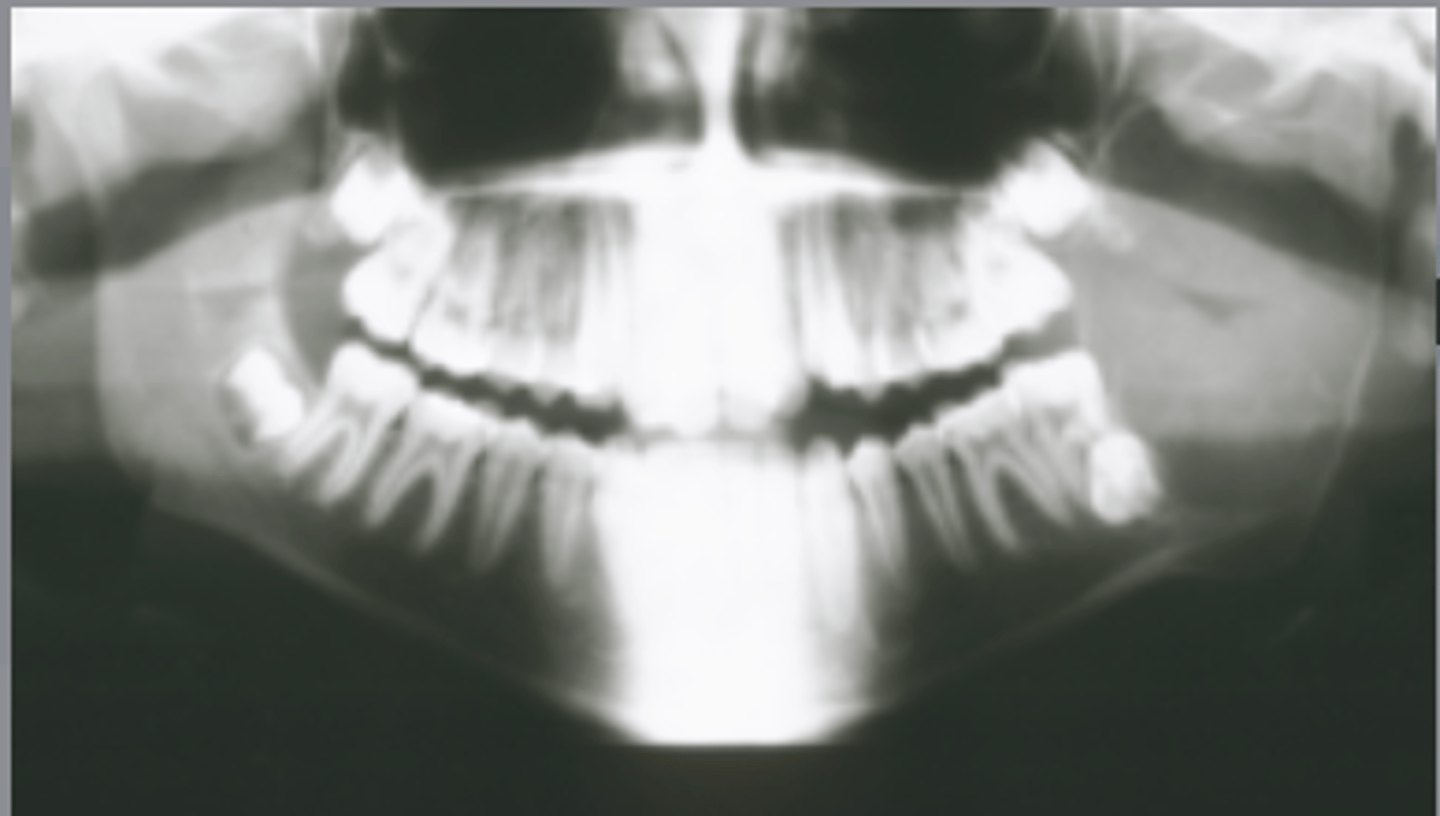
How would you describe the lesion?
Multiple multi-focal coalescing target-like radiopacities in multiple quadrants

What category would this lesion be part of?
Dysplasia

What would be a differential diagnosis for this lesion?
Florid cemento-osseous dysplasia
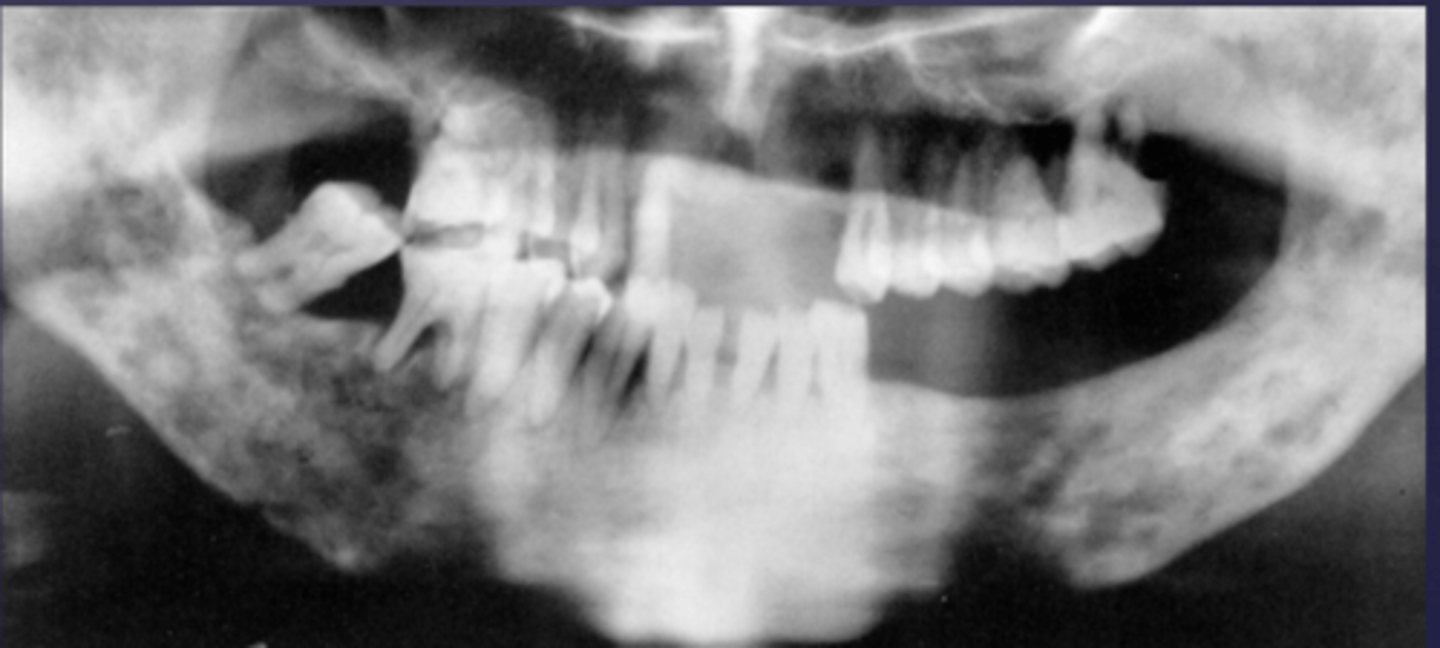
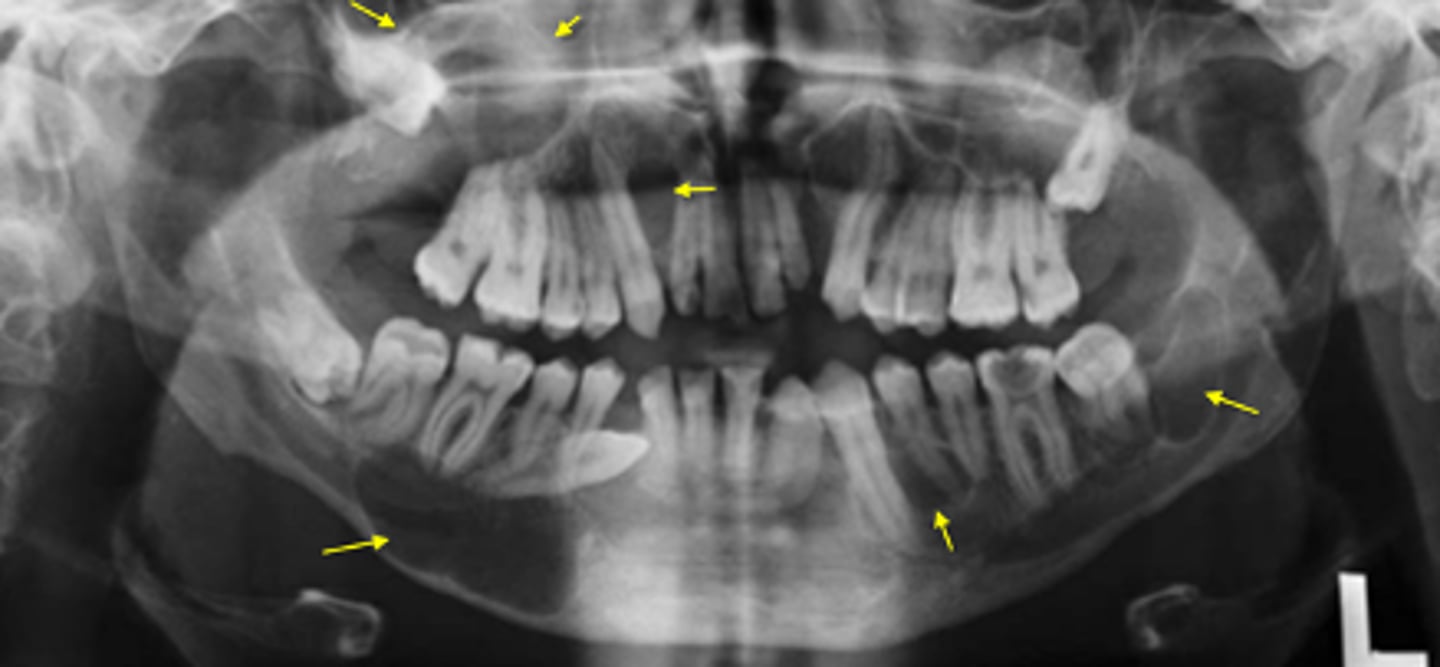
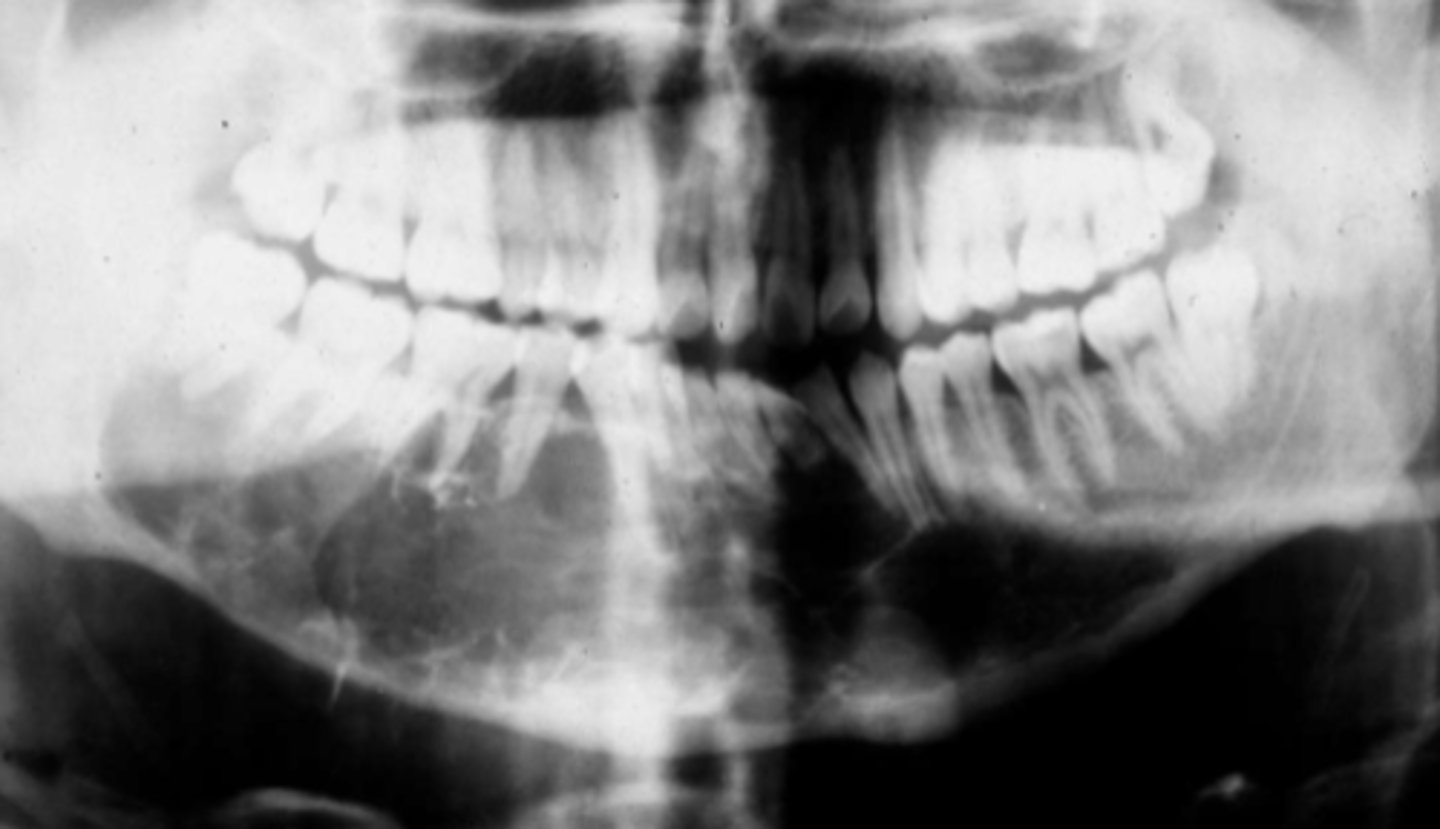
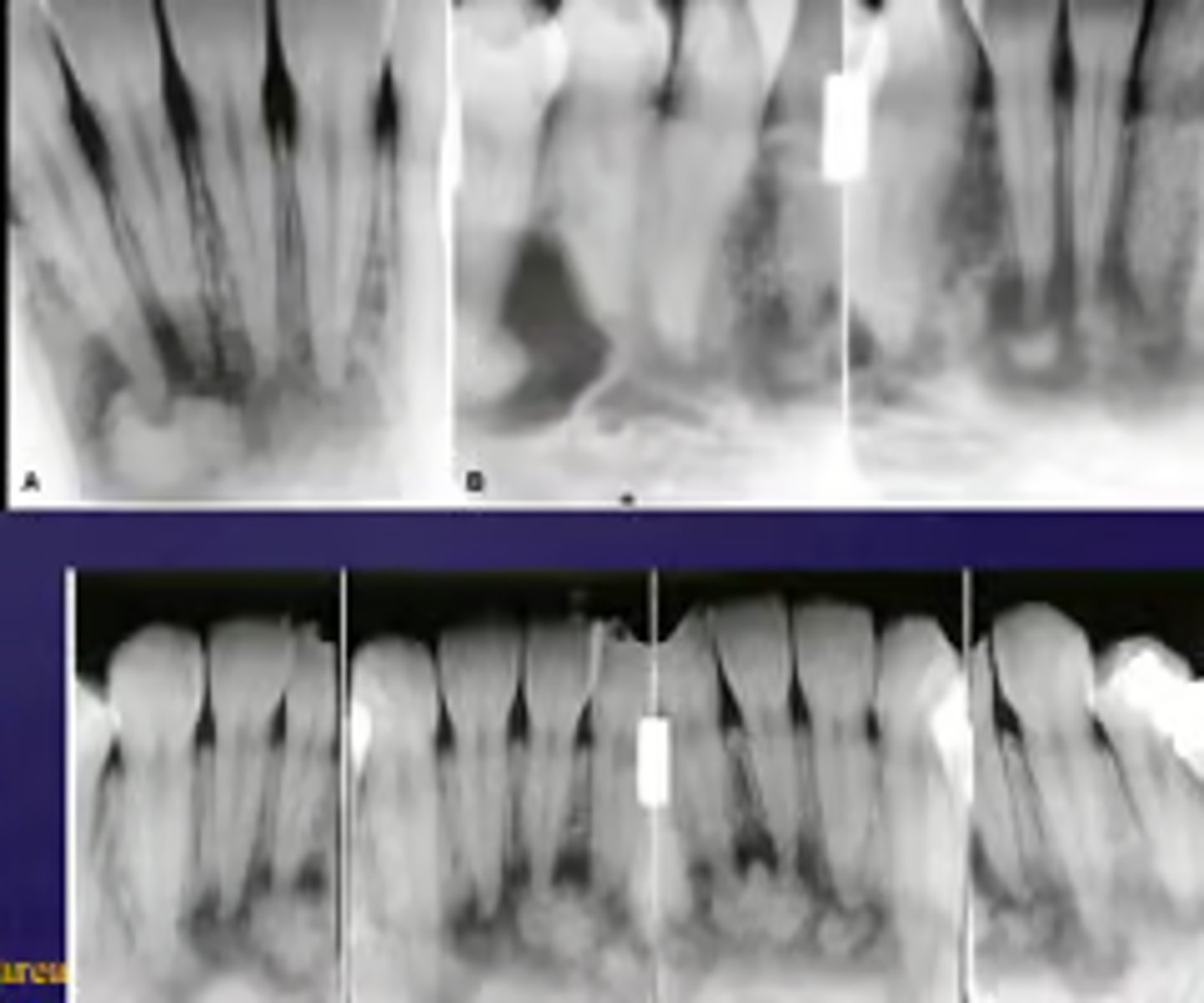
How would you describe the lesion?
- Ill defined, moth-eaten trabecular pattern in the entire mandible
- There is chronic periodontal bone loss associated with most mandibular teeth with furcation involvement and apical radiolucencies
- There is thinning of the inferior mandibular cortex.
- Can also be described as ill-defined areas of mixed radiolucent and radiopacities throughout the
mandible
What category would this lesion be part of?
Inflammation/Malignant
What would be a differential diagnosis for this lesion?
Chronic osteomyelitis
(DD: osteomyelitis, multiple myeloma)

How would you describe the lesion?
- Well-defined corticated multilocular radiolucency in the right ramus
- Mandibular body causing root resorption
- Expansion and thinning of anterior wall of ramus, coronoid process, inferior border of mandible
- Displacement of the inferior alveolar canal

What category would this lesion be part of?
Benign

What would be a differential diagnosis for this lesion?
- Ameloblastoma
- OKC
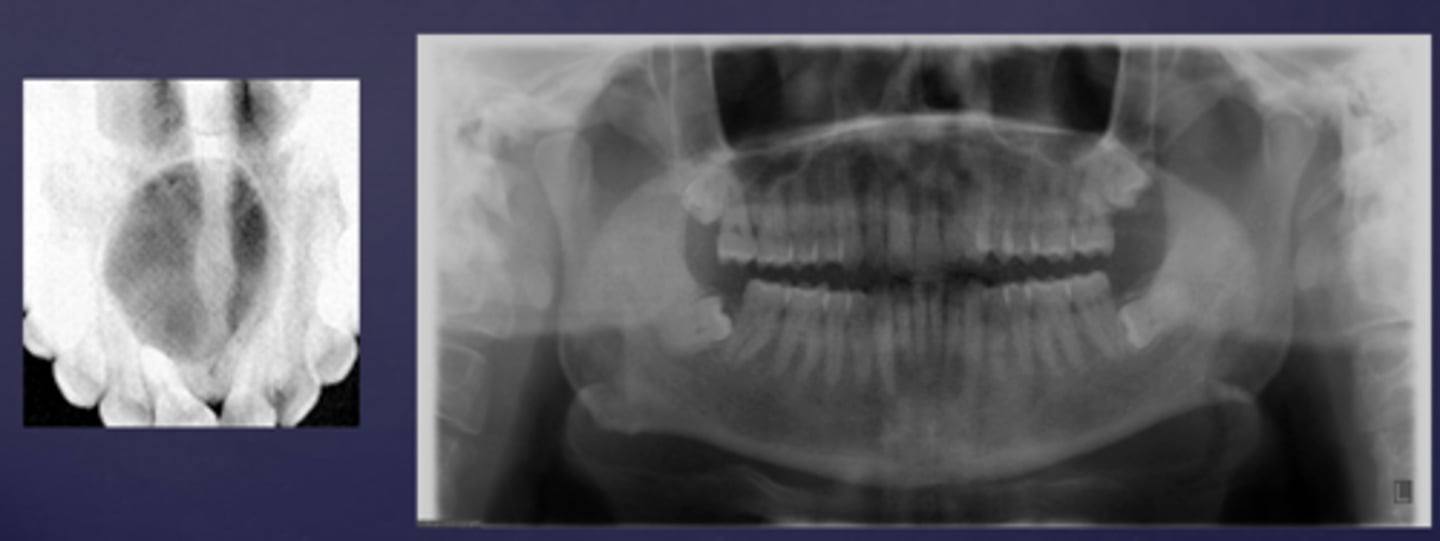
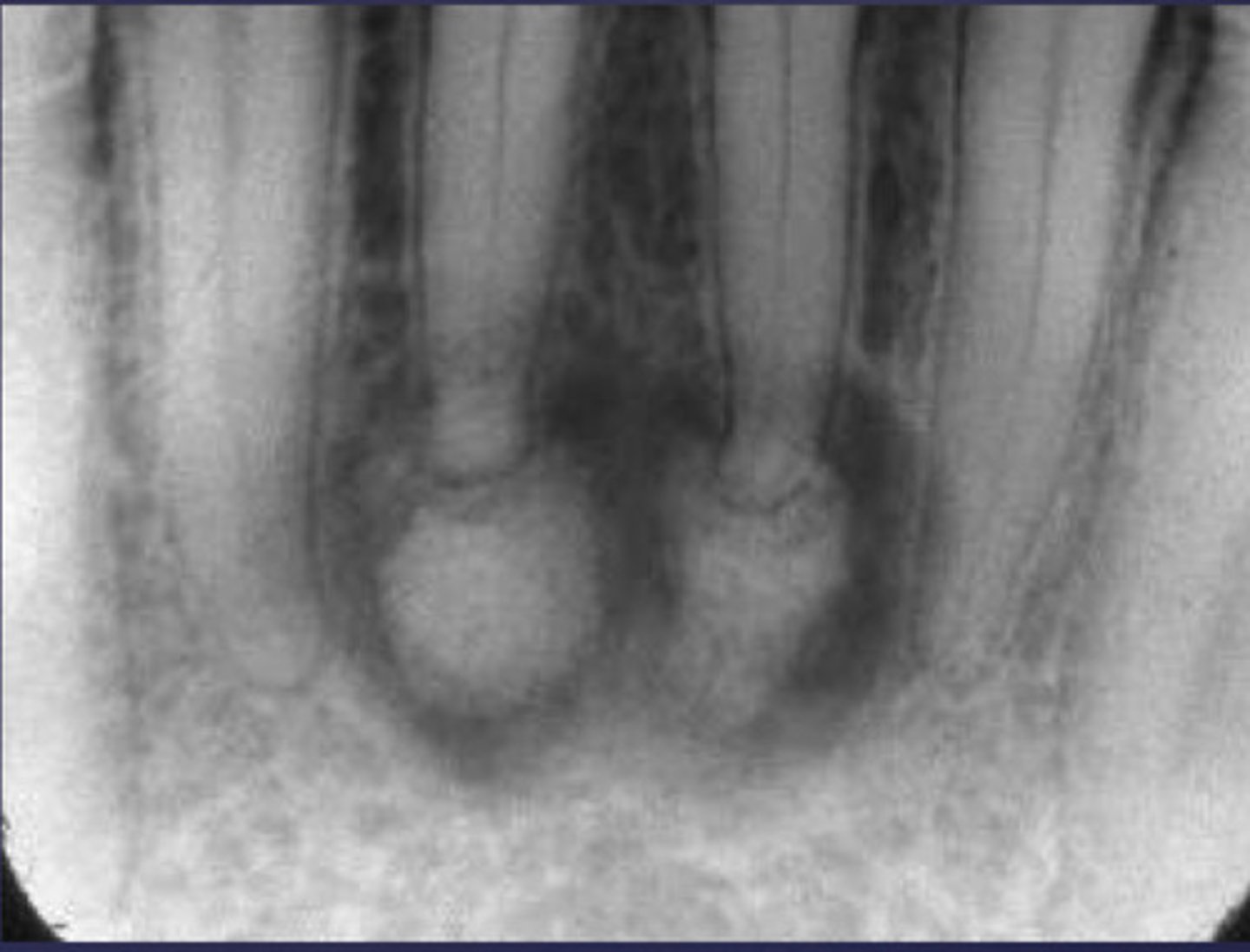
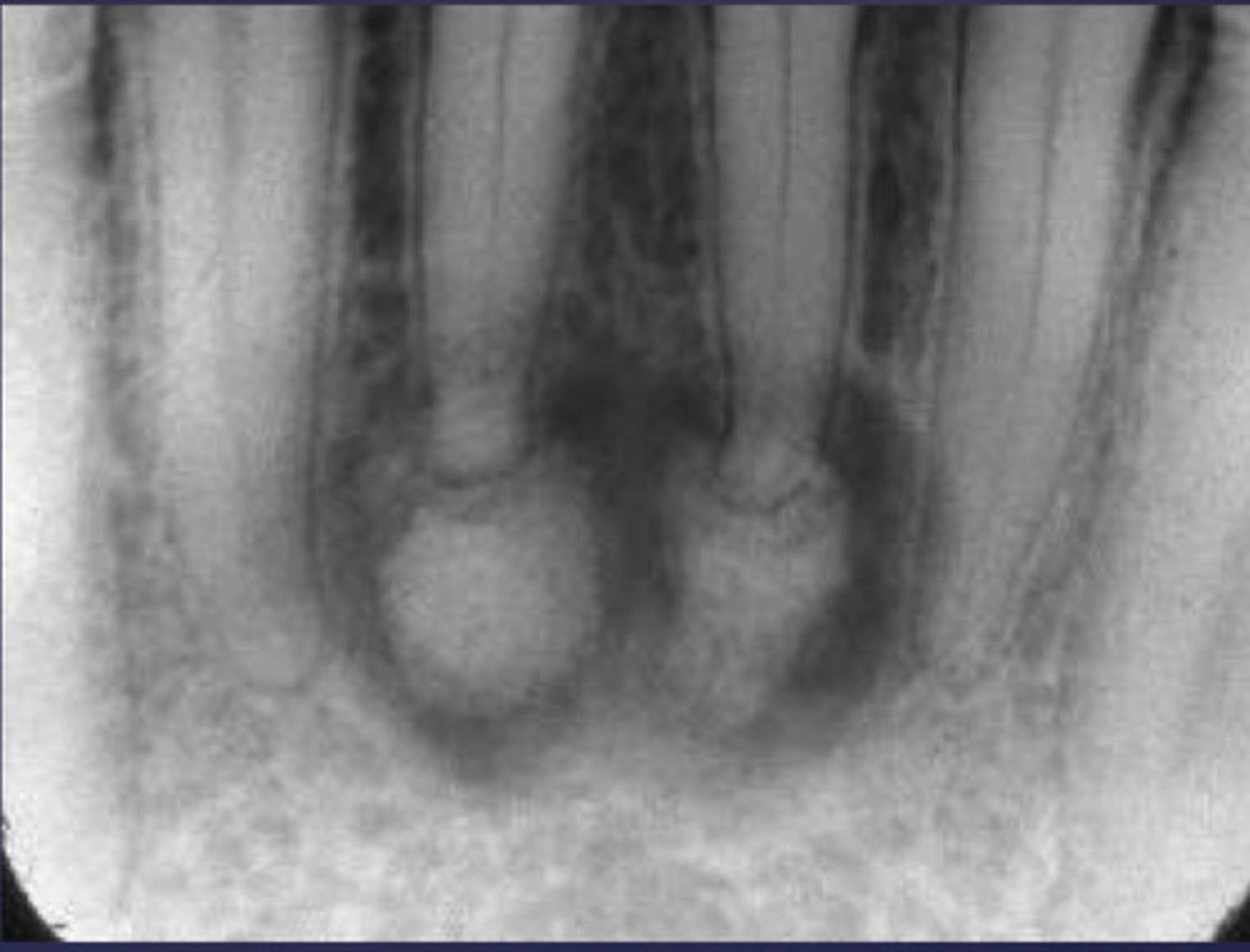
How would you describe these lesions?
- Defined, corticated midline maxillary radiolucency
- Causing tooth displacement in the occlusal image
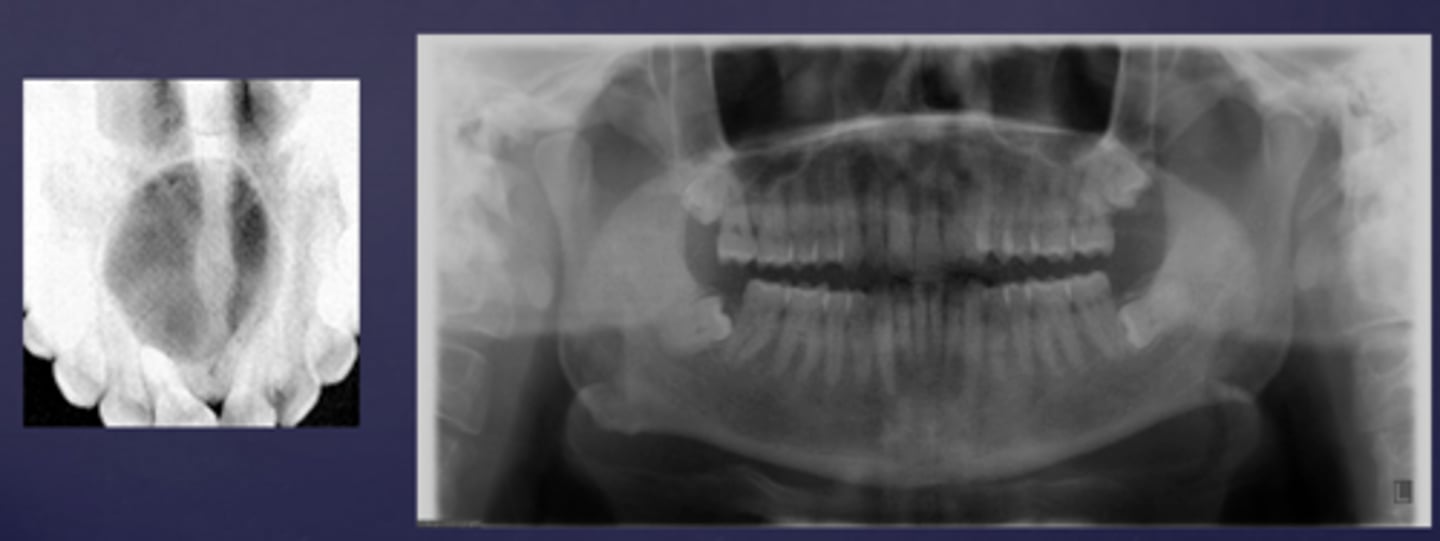
What category would these lesions be part of?
Benign
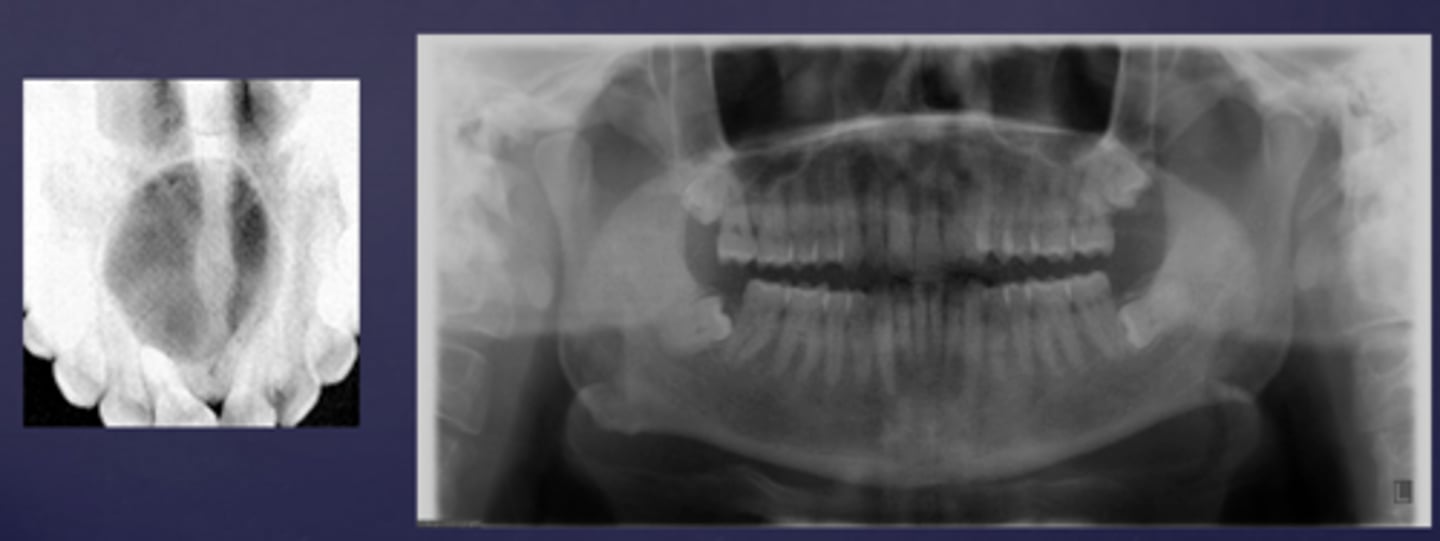
What would be a differential diagnosis for these lesions?
Incisive/nasopalatine duct cyst
(Pan and occlusal are not from the same case but they share the diagnosis)
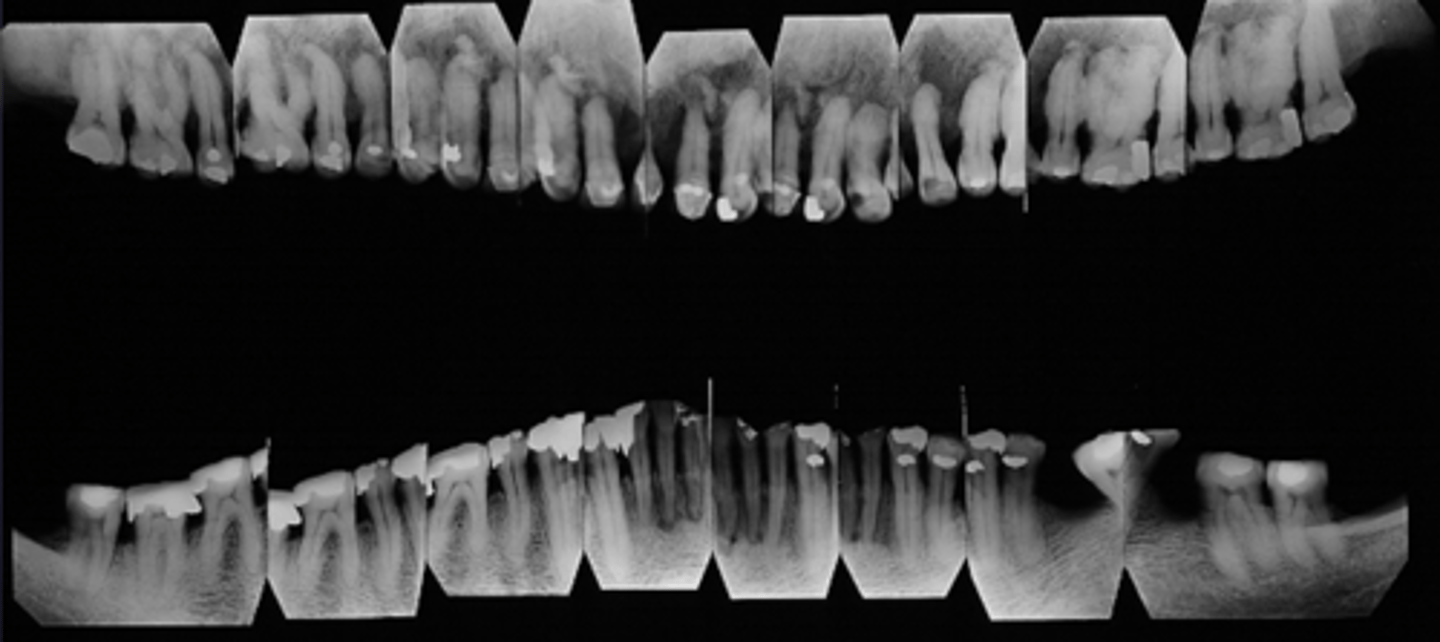
How would you describe the lesion?
Generalized alteration in the alveolar trabecular pattern with exuberant hypercementosis on multiple teeth
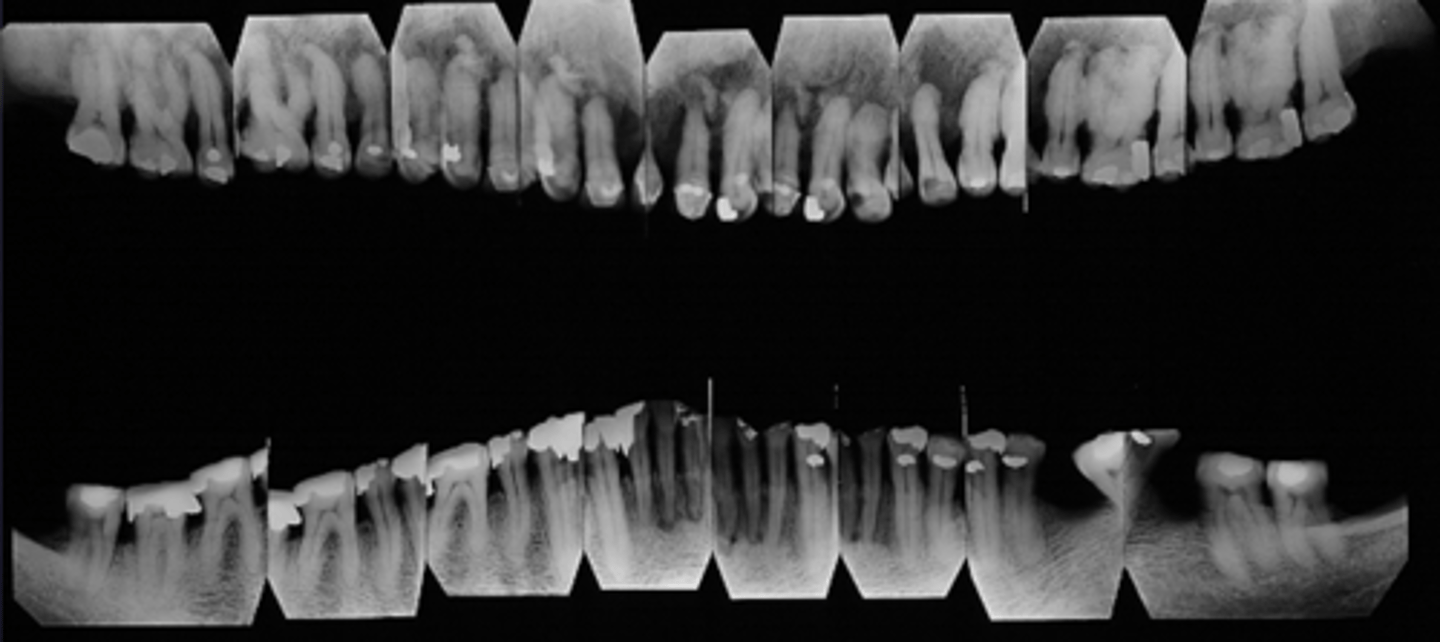
What category would this lesion be part of?
Systemic/metabolic
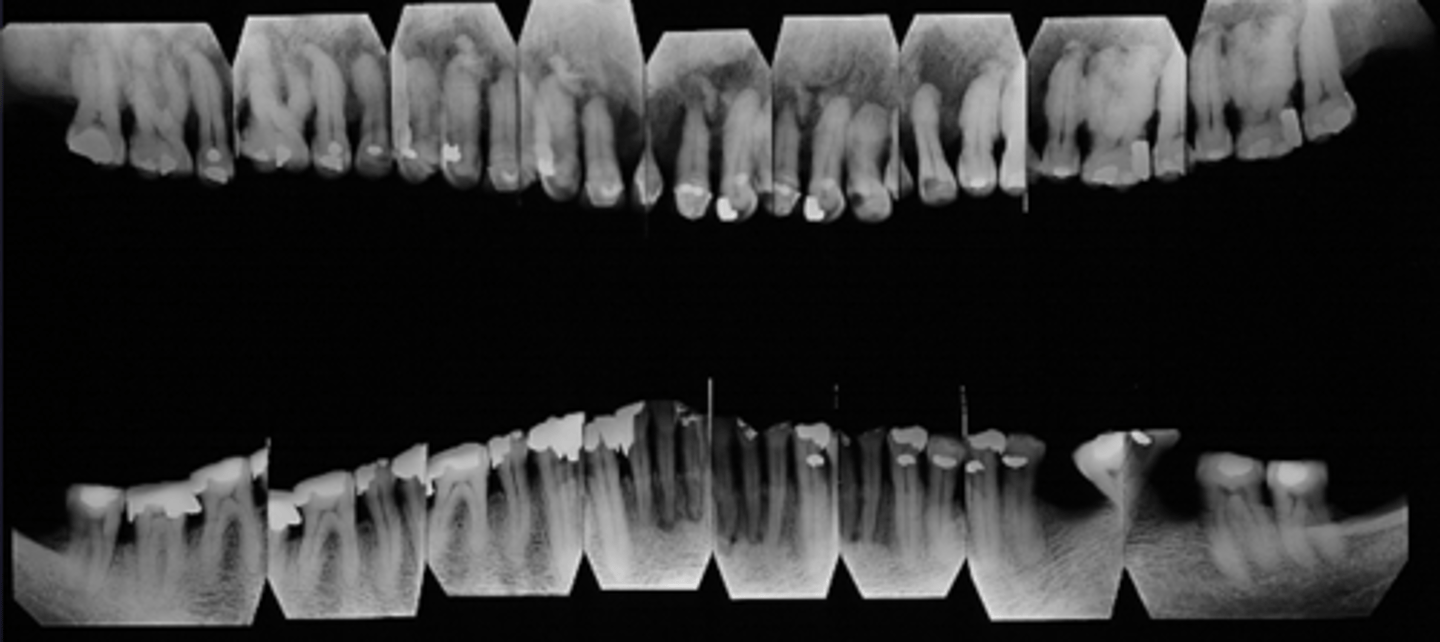
What would be a differential diagnosis for this lesion?
Pagets disease of bone

How would you describe the lesion?
- Defined multilocular( honey comb/soap bubble)
- Interradicular radiolucency causing loss of lamina dura on the mid-root level of the canine and premolar

What category would this lesion be part of?
Benign

What would be a differential diagnosis for this lesion?
- OKC
- Ameloblastoma
- Lateral periodontal cyst

How would you describe the lesion?
- Defined corticated radiolucency associated with an impacted, displaced tooth
- Root resorption and teeth displacement also present along with thinning of the inferior mandibular cortex
- large calcifications noted just coronal to the impacted tooth

What category would this lesion be part of?
Benign

What would be a differential diagnosis for this lesion?
- Gorlins cyst
- Pindborg tumor

What would be a differential diagnosis for this lesion?
Calcified carotid atheromatous plaque
How would you describe the lesion?
- Lamellar or concentric pattern
- Located below the IAN and in the area of submandibular salivary gland
What would be a differential diagnosis for this lesion?
Left submandibular sialolith

What would be a differential diagnosis for this lesion?
Calcified carotid atheromatous plaque and mucous retention pseudocyst in the right maxillary sinus

ID the cyst:
- Well defined corticated periphery
- Radiolucent
- Involves nasopalatine canal and incisive foramen
- Lesion is palatal to the teeth
- Maybe 'heart-shaped' due to superimposition of anterior nasal spine
nasopalatine duct cyst

what is your diagnosis?
- Unilocular radiolucency
- Scalloping between roots of vital teeth
- No root resorption
- Empty cavity
simple bone cyst

what is your diagnosis?
- Located between inferior alveolar nerve canal and inferior border of mandible
- Oval/round/elliptical shape
- Well-circumscribed radiolucency
- Dense sclerotic corticated (radiopaque border) usually on the superior aspect
stafne bone cyst

Patient's radiograph shows the following. What is the diagnosis?
- Garrington sign (widened PDL space)
- Ragged, ill-defined radiolucent/paque mixed area
- 'sun ray' periosteal reaction
- spiked root resorption pattern
osteosarcoma

ID the cyst:
- Radiolucent lesion
- Well defined corticated periphery
- Round/oval
- Located between cervical margin & apex of adjacent vital teeth
- Typically in contact with root surface
lateral periodontal cyst

ID the cyst:
- Radiolucent lesion
- Well defined, corticated borders
- Hydraulic/round
- Periapical in location (apex of a non vital tooth)
radicular cyst
what is your diagnosis?
- Well defined and corticated lesion
- Radiolucent
- Pericoronal (associated with crown of unerupted tooth)
- Usually unilocular
- Osseous expansion- of outer cortical boundary of the involved jaw
dentigerous cyst

ID the cyst:
- Well defined corticated periphery
- Radiolucent interior
- Undulating/scalloped borders
- Multilocularity (internal septae) is typically noted, but may be unilocular
Keratocystic Odontogenic Tumor (KOT)/Odontogenic Keratocyst (OKC)
ID the condition:
- Multiple OKCs/ KOTs in multiple locations of both jaws
- Other findings:
- - Basal cell carcinoma
- - Skeletal anomalies- bifid ribs
- - Calcification of falx cerebri
Gorlin Goltz Syndrome/Nevoid Basal Cell Carcinoma Syndrome
ID the cyst:
- Well defined corticated periphery, maybe ill defined
- Internal aspect- Radiolucent or mixed radiolucent-radiopaque
- Maybe associated with unerupted tooth (impeding eruption)
- May cause displacement, resorption of roots, cortical perforation
Calcifying Epithelial Odontogenic Cyst (CEOC/Gorlin Cyst )Calcifying Cystic Odontogenic Tumor (CCOT)
ID the cyst:
- Lesion is superimposed over the apices of maxillary central incisors
- No changes in apical structures of these teeth (lamina dura, PDL)
- Vital teeth
- May displace these teeth
nasopalatine duct cyst
ID the cyst:
- Radiolucent lesion
- Moderately to well-defined borders
- Unilocular or multilocular
- May create scalloping between roots of involved teeth
- Does not resorb or displace tooth roots
simple bone cyst/ traumatic bone cyst

What is the diagnosis?
- Not a true cyst
- Obstruction or dilatation of the duct of sero-mucous glands in sinus resulting in submucosal accumulation of secretions
- Radiographic feature :
- Relative radiopacity on the floor of sinus
- Well-defined, not corticated
- Dome-shaped
mucus retention pseudocyst
Patient presents with an expansion on the posterior mandible. Radiograph shows a multi-locular, "soap bubble" radiolucency with wispy trabecular resembling cobwebs that are more angular in shape and cause root resorption and displacement.
What is the diagnosis?
odontogenic myxoma
What is the diagnosis?
- Tumor with features of ameloblastic fibroma plus enamel and dentin
- Average age = 10
- Seen most often in posterior, especially mandible
- Asymptomatic
- Often associated with an unerupted tooth
ameloblastic fibro-odontoma
"Soap bubble" or "honeycomb" appearance on a radiograph is associated with what pathologies?
- Ameloblastoma
- Odontogenic myxoma
ID pathology based on radiographic features:
- Usually multilocular
- “Soap bubble” or “honeycomb”appearance
- Buccal and/or lingual cortical expansion
ameloblastoma
What is the diagnosis?
19 y/o female patient presents with a large mass growing on the anterior maxilla. Patient is asymptomatic. Radiograph shows well-circumscribed unilocular radiolucency with fine "snowflake" calcifications surrounding impacted incisor. Radiograph shows tubular/ duct-like structures and scattered calcifications.
adenomatoid odontogenic tumor (AOT)
What is the diagnosis?
Patient presents with an expansion on the posterior mandible. Radiograph shows a multilocular radiolucency containing calcifications within lesion and impacting the 3rd molar. Histopathology shows epithelial islands with calcifications that form concentric Liesegang rings.
Calcifying Epithelial Odontogenic Tumor/Pindborg
Patient presents with pain and swelling. Radiograph shows a radiopaque mass fused to root of tooth surrounded by thin radiolucent rim, and some root resorption.
cementoblastoma

14 year old patient presents with all teeth erupted except for the 1st molar. Radiograph shows a collection of tooth-like structures surrounded by radiolucent zone. What is the pathology?
compound odontoma
ID the benign tumor:
- Radiolucent lesion, variable size, unilocular
- Radiopaque foci, radiolucent halo
- Ground glass, cotton-wool appearance
- Well-defined, "cystlike" growth-thinning of cortices
- Tooth displacement, root resorption
cemento-ossifying fibroma

What is the diagnosis?
Patient presents with a radiograph that shows a well defined, uniformly radiopaque exophytic mass (the same density as cortical bone), located on the posterior inferior mandible.
osteoma

What is the diagnosis?
Patient presents with a dense, radiopaque shadow in the midline of the hard palate area that has a well defined periphery and is superimposed over the roots of the maxillary teeth. Patient opens their mouth and the etiology is visible.
torus palatinus
What is the diagnosis?
Patient presents with a radiograph that has a well defined radiopaque lesion that seems to blend with trabeculae of surrounding bone. It has no affect on the adjacent teeth. This condition is contraindicated for ortho and implants due to decreased vascular supply in that region.
Enostosis (dense bone island/ idiopathic osteosclerosis)

ID the pathology:
- Reactive lesion
- CF: Common lesion, appro. 20 years of age, painless swelling and asymmetry
- RF: anterior mandible, secondary-anterior maxilla, can cross midline
- Well defined corticated or non-corticated borders
- Uni-or multilocular, completely radiolucent or wispy straight septae
central giant cell granuloma (CGCG)
What is the diagnosis?
30 y/o Black female presents asymptomatic to your office. Radiograph shows multiple apical radiolucencies that are < 1cm and are round and well-defined in the anterior mandible. The lamina dura is discontinued by the lesion. Tooth is still vital.
Periapical Cemento-Osseous Dysplasia (PCOD) stage 1: Osteolytic
ID the lesion:radiopacity in center of radiolucent area
Periapical Cemento-Osseous Dysplasia (PCOD) stage 2: Cementoblastic
30 y/o Black female presents asymptomatic to your office. Radiograph shows multiple apical crescent-shaped, central radiopaque masses surrounded by radiolucent halo in the anterior mandible. Tooth is still vital. What is the diagnosis?
Periapical Cemento-Osseous Dysplasia (PCOD) stage 3: Mature
ID the pathology based on radiographic features:
- Multiple mixed density/radiopaque masses
- More than 1 quadrant of tooth-bearing areas
- Varying amounts of radiolucent areas
- Cotton-wool appearance
- Concurrent traumatic bone cysts
florid cemento-osseous dysplasia

What is the diagnosis?
16 y/o patient presents with facial asymmetry from swelling. Patient denies pain. Radiograph shows a slow growing diffuse/ ill-defined dense sclerotic pattern that is orange-peel/fingerprint/ground glass/cotton wool-like in appearance in the posterior maxilla. There is expansion of the maxilla, tooth displacement and loss of lamina dura of adjacent roots. Opacification of the maxillary sinus is also noted.
fibrous dysplasia
What is the diagnosis?
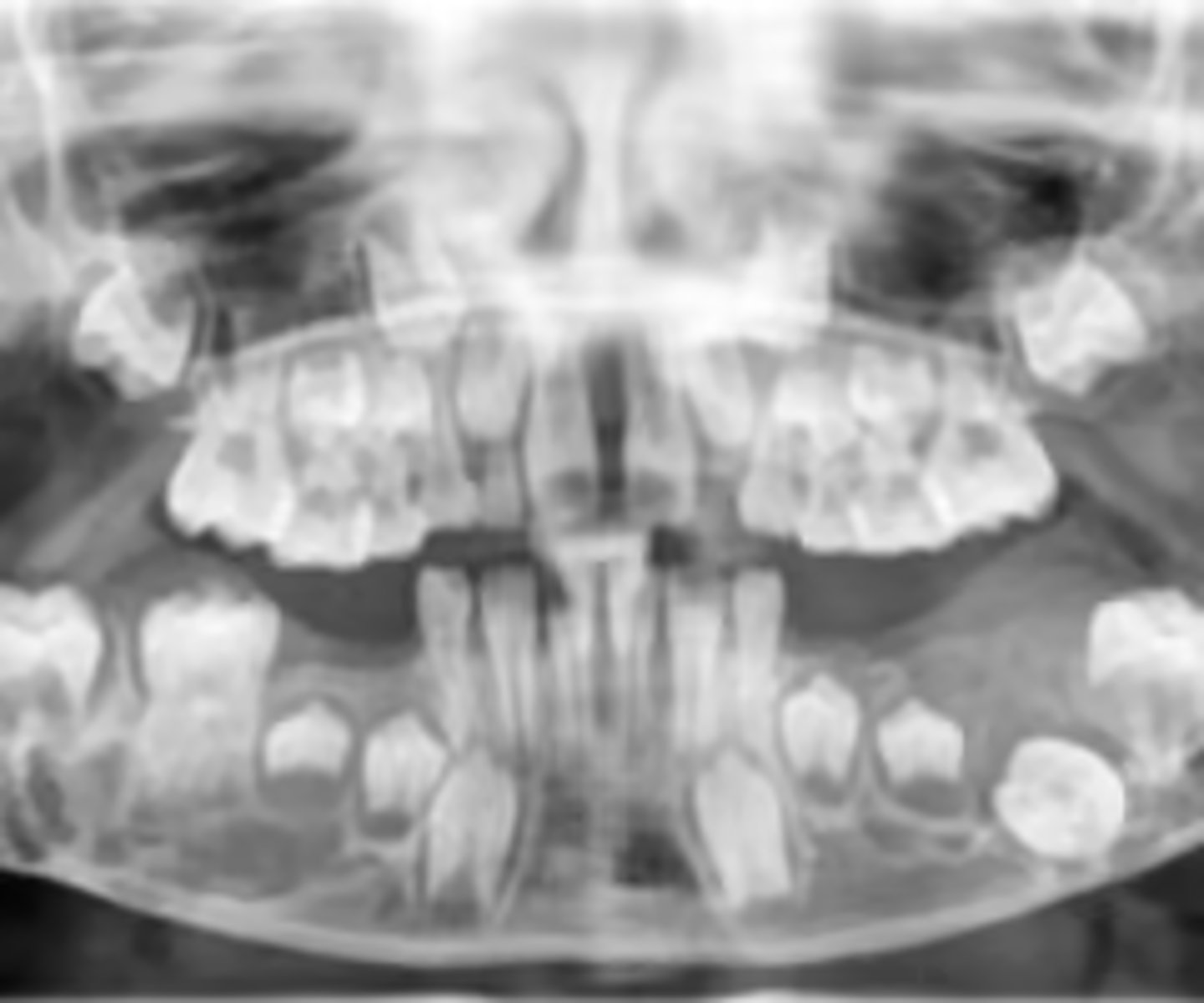
6 y/o patient presents to your office with a bilateral chubby face that is firm on palpation. Patient denies pain. Clinically, the mucosa looks normal. Radiograph shows bilateral, multilocular radiolucencies that are multicystic in appearance, in the posterior mandible (some maxilla). There is expansion/thinning of cortices, tooth displacement and resorption of adjacent roots.
cherubsim