Structure and Motion of the Hip PT 706
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
what populations have disease and injury in hip joint?
old and young
where does pelvis transmit weight?
standing: down the legs
sitting: ischial tuberosity
pubic symphysis
cartilaginous joint at which two pubic bones fuse together
sacroiliac joint
synovial in childhood, but changes to synarthrosis as we age (little movement)
sacroiliac joint surface
As you age, your sacrum becomes more rigid and less smooth, used to give the age of a specimen at death
angle of inclination
angle in frontal plane formed between the longitudinal axis of the femoral head/neck and the longitudinal axis of the femoral shaft
angle of inclination adult norms
125 degrees
angle of inclination child norm
150 degrees
coxa varus
angle of inclination is less than 125 degrees
coza valgus
angle of inclination is more than 150 degrees
femoral torsion
Transverse plane, rotation between the bones shaft and neck
Head and neck are rotated anteriorly (normal)
normal femoral torsion in adults
10-20 degrees
normal femoral torsion in children
40 degrees
excessive anteversion
more than 20 degrees of femoral torsion
excessive retroversion
less than 10 degrees of femoral torsion
Forces from HAT (head, arm and trunk) and GRF (ground reaction force) contribute to what?
tensile forces on superior femoral neck and compressive forces on inferior femoral neck
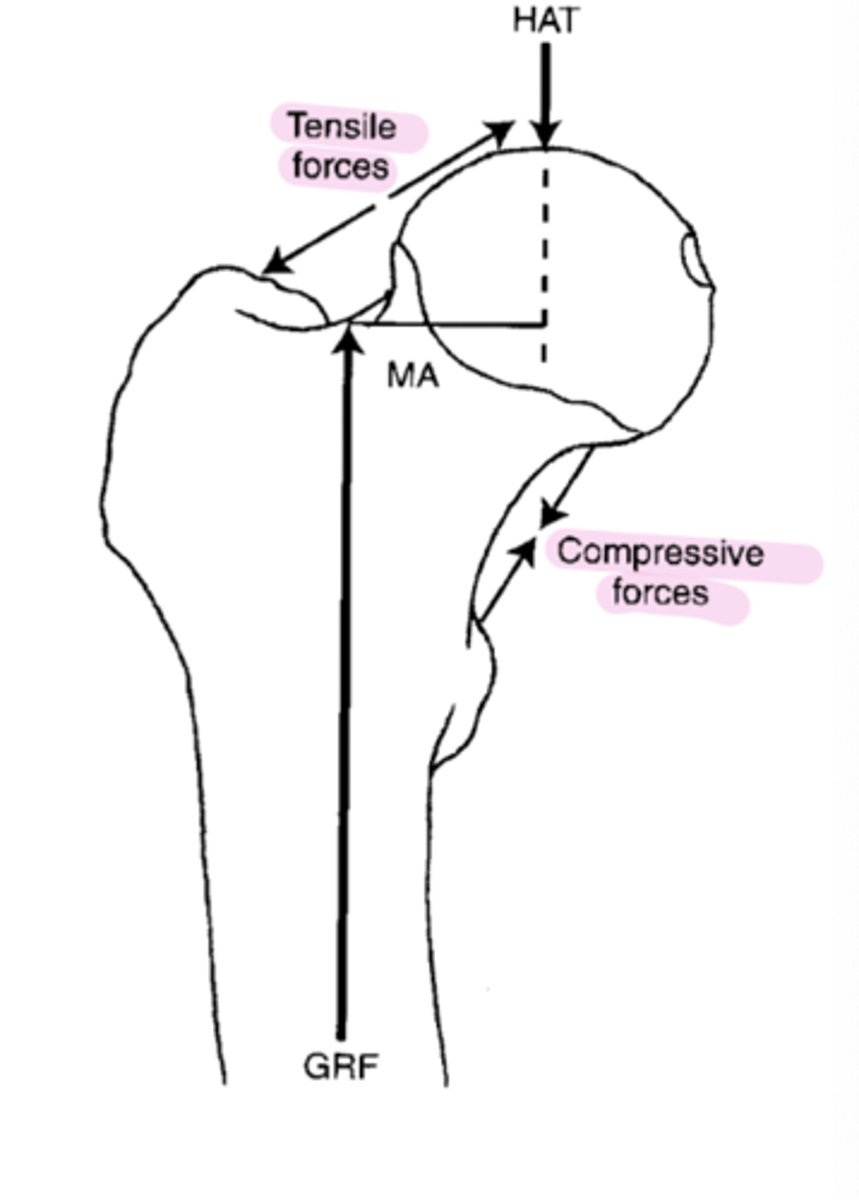
What resists the tensile and compressive forces from HAT and GRF?
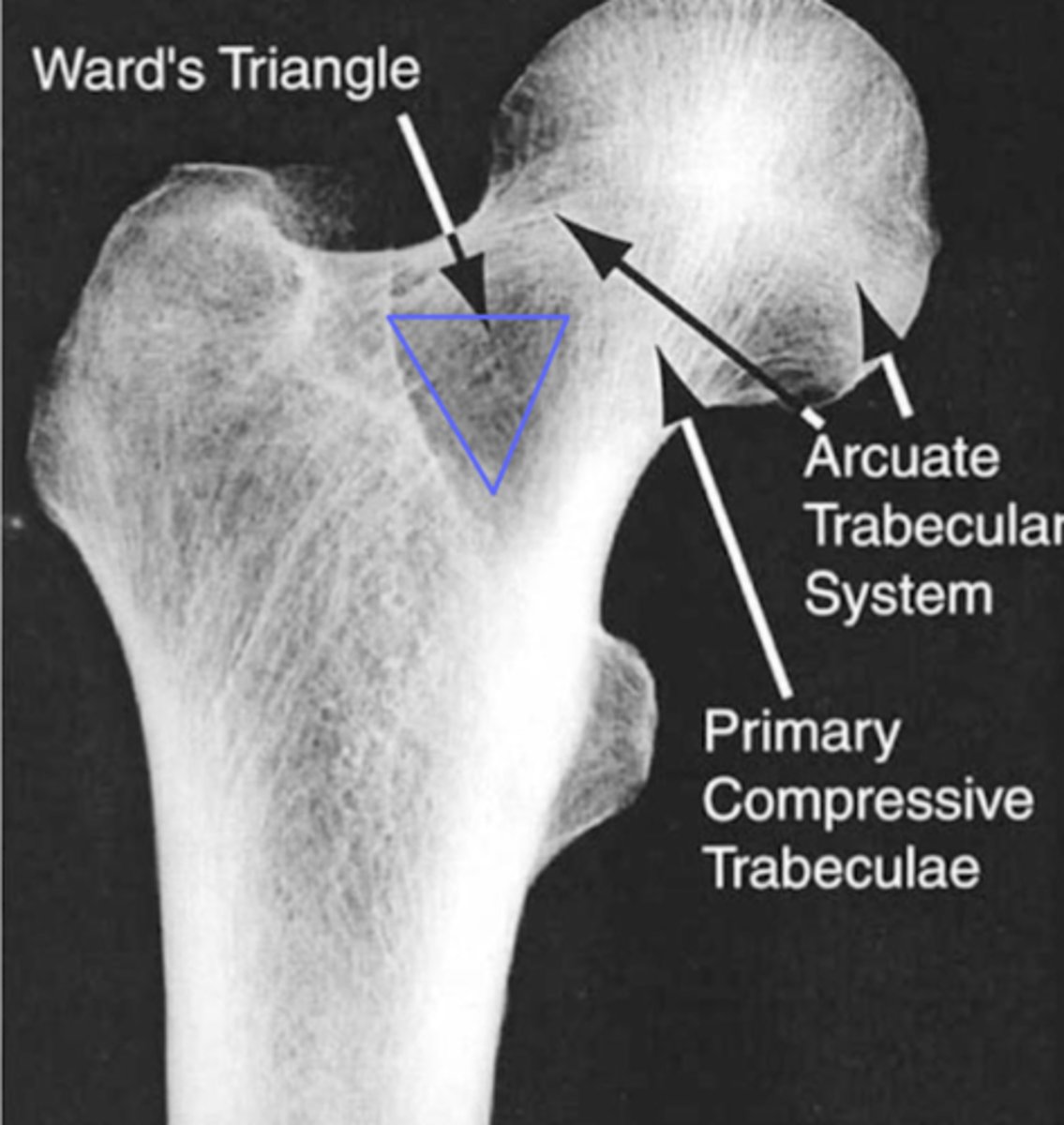
trabecular systems of bone
trabeculae
calcified plates of tissue within the cancellous bone
Adapt to stress requirements
what dictates formation of trabeculae?
mechanical stresses and structural adaptation to forces through the hip (bone forms based on the loads you apply, different parts of bone will look different depending on forces)
Wards Triangle
zone of weakness in femoral neck, no crossing of trabeculae, more potential for failure, fractures and osteoporosis
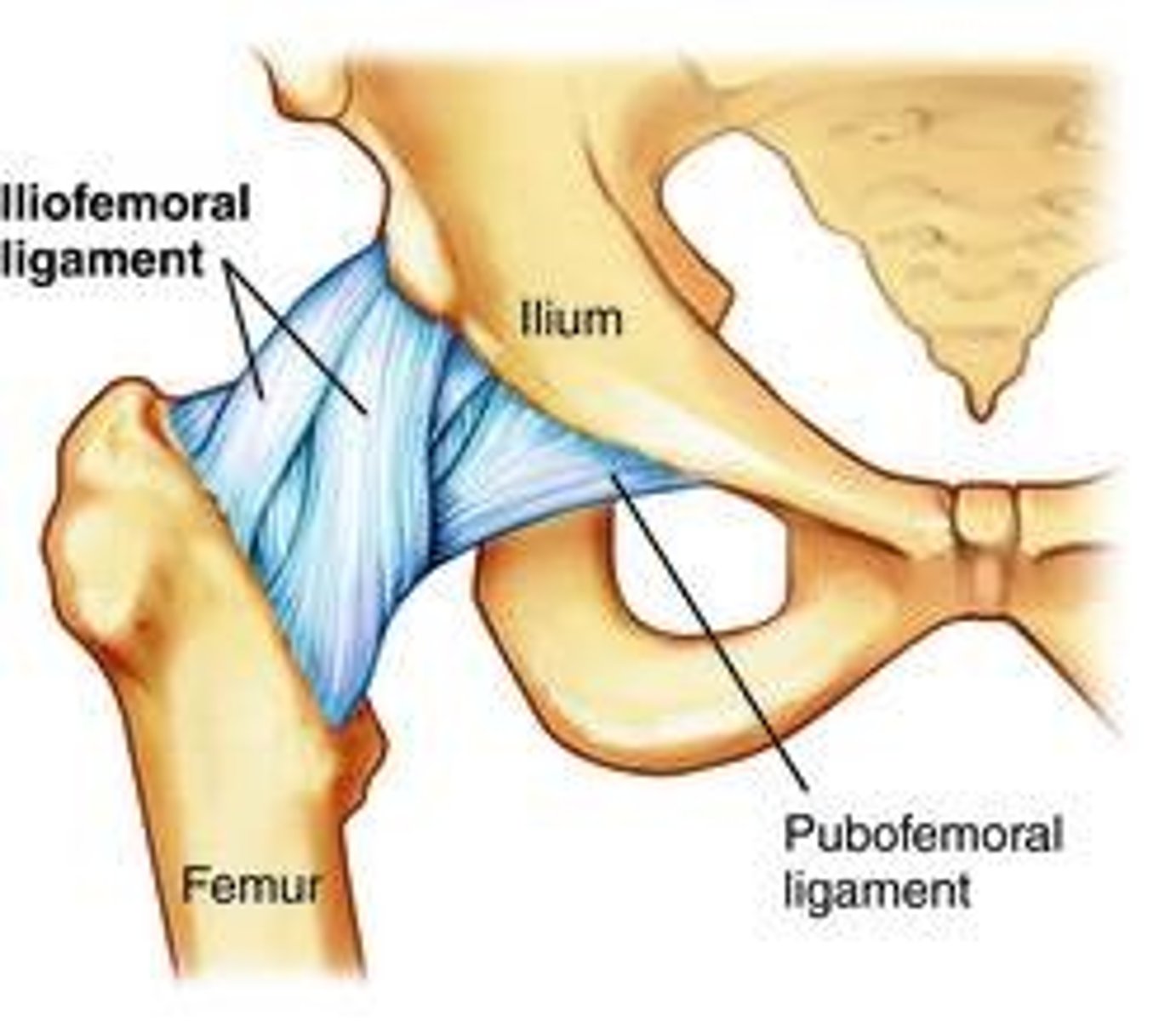
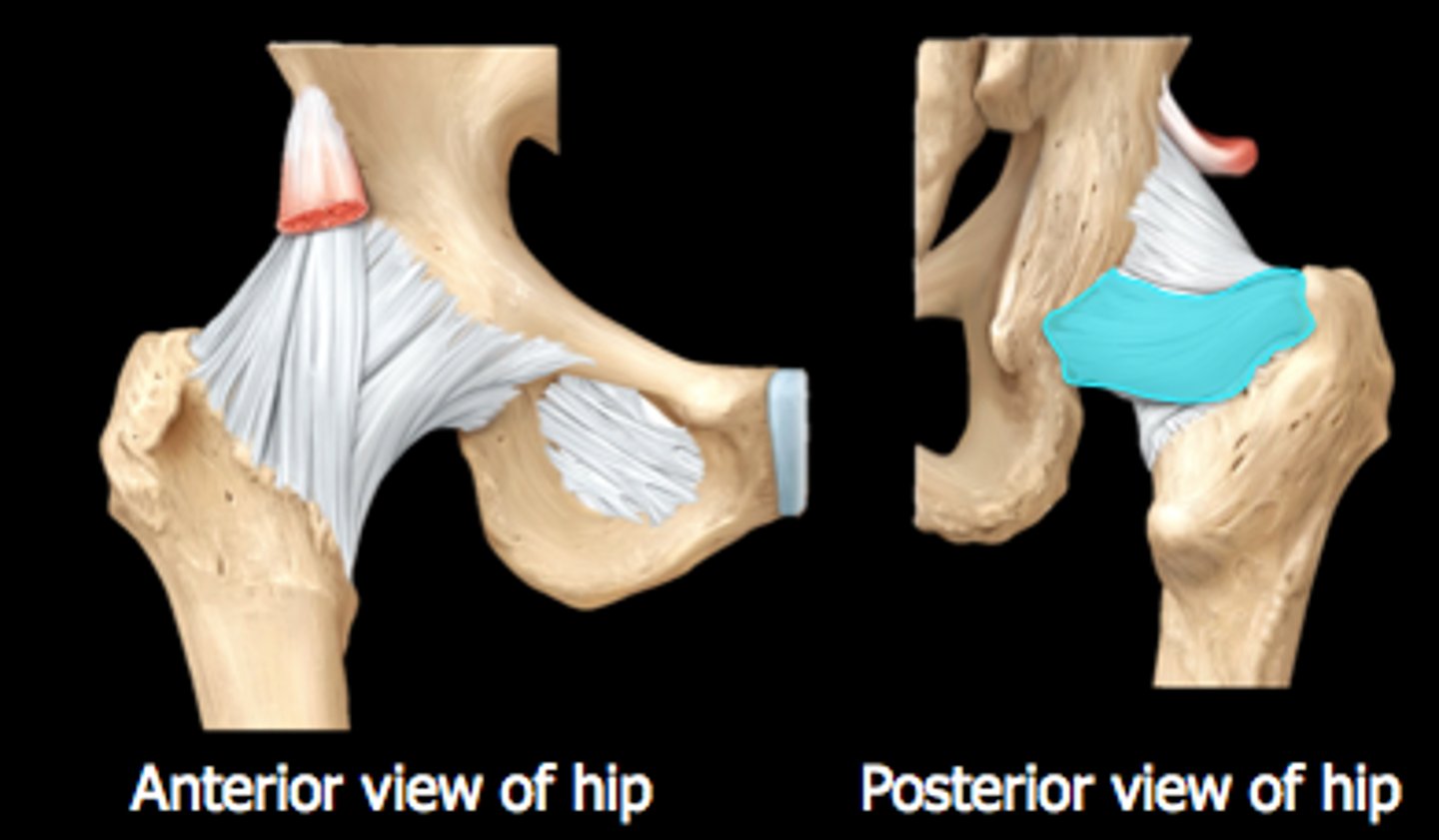
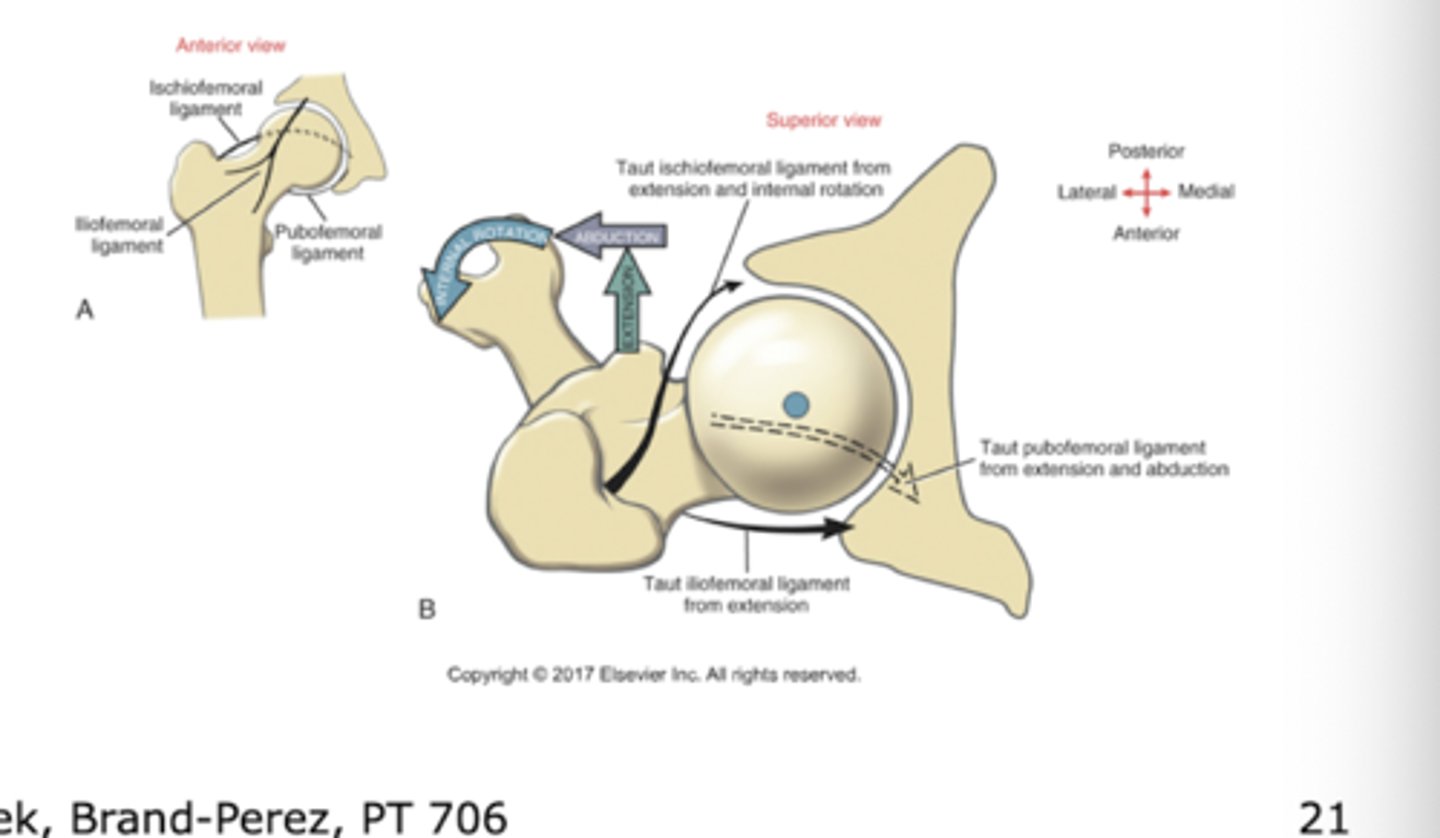
iliofemoral ligament
anterior hip ligament (y shaped)
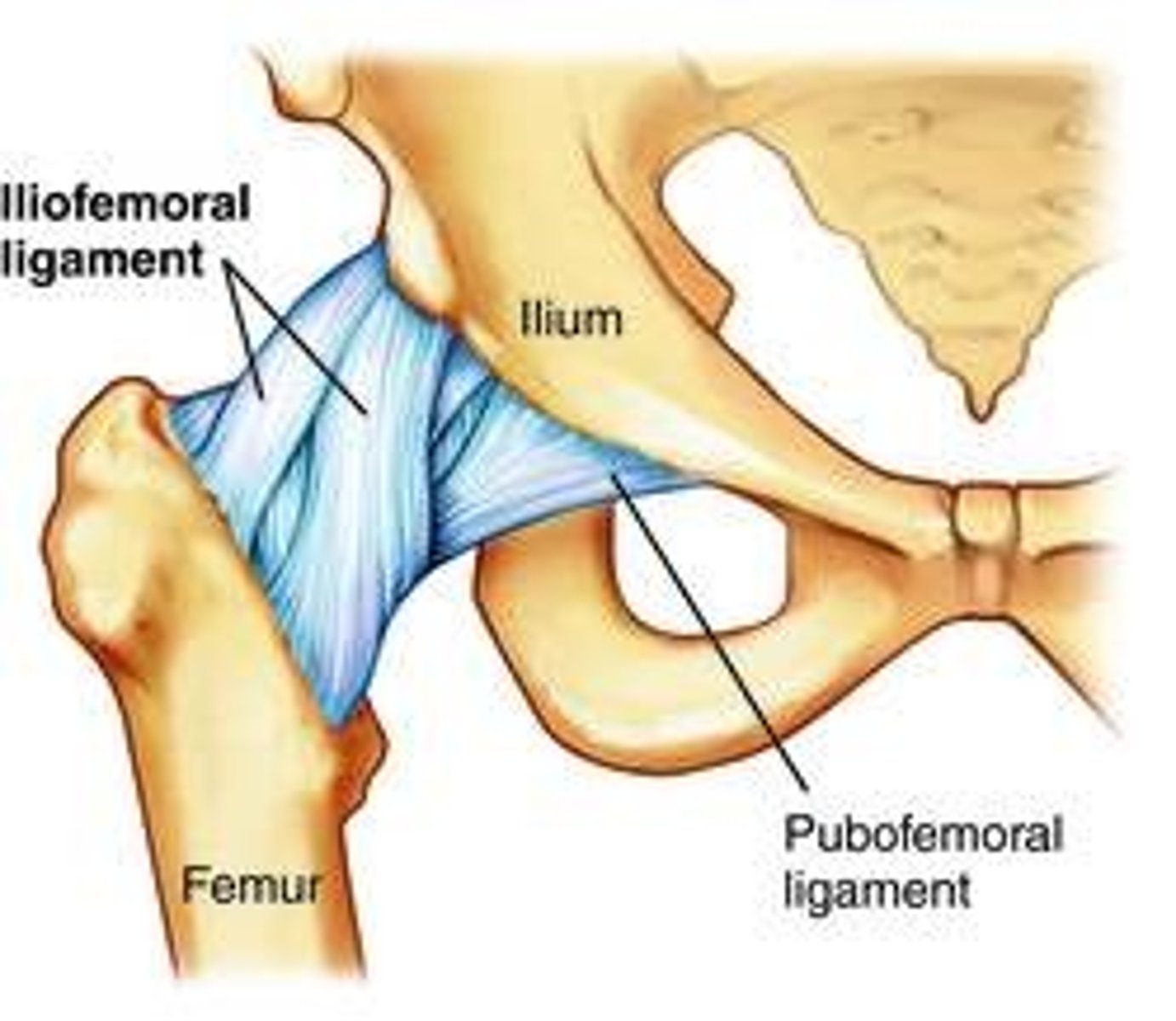
pubofemoral ligament
inferior hip ligament
ischiofemoral ligament
posterior hip ligament
ligamentum teres
intra-articular, extrasynovial
Not a significant stabilizer, acts as conduit for secondary blood supply to head of femur
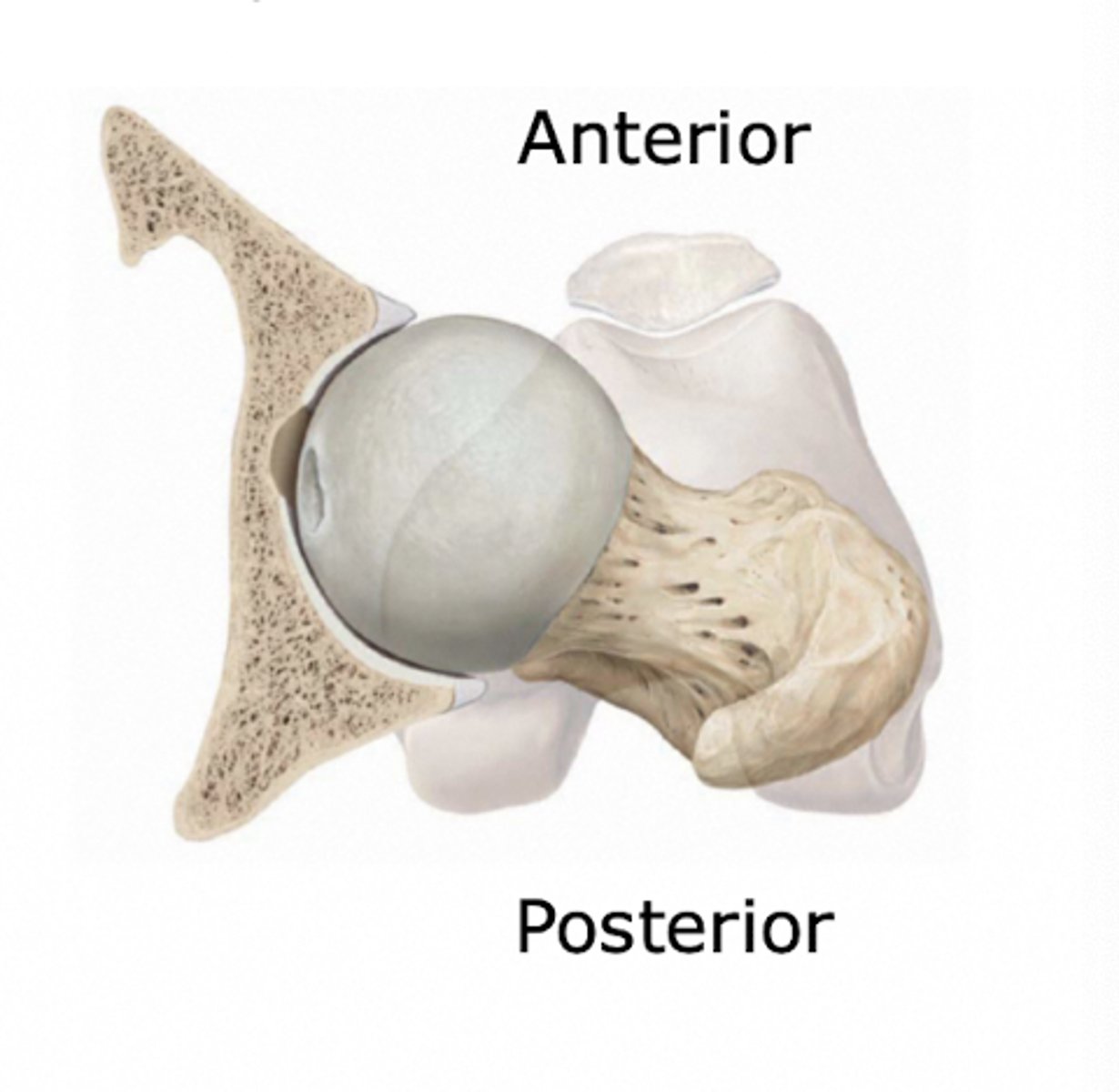
congruency during normal standing
femoral head is exposed anteriorly and slightly superiorly during normal standing
most bony congruency of hip
quadruped, femoral flexion, abduction and slight external rotation

ligamentous close packed position of hip
internal rotation with extension, some abduction
* different than the most bony congruent position of the hip
open packed (resting) position of hip
30 degrees of fexion, 20 dgerees of abduction and external rotation
(lying with pillow under knees)
hip flexion normal ROM
120 degrees
hip extension normal ROM
20 degrees
hip abduction normal ROM
40 degrees
hip adduction normal ROM
20 degrees
hip IR normal ROM
45 degrees
hip ER normal ROM
45 degrees
open chain arthrokinematics
hip flexion
Roll: anterior/superior
Glide: posterior/inferior
open chain arthrokinematics
hip extension
Roll: posterior
glide: anterior
open chain arthrokinematics
hip abduction
roll: superior
glide: inferior
open chain arthrokinematics
hip adduction
roll: inferior
glide: superior
open chain arthrokinematics
hip IR
roll: anterior
glide: posterior
open chain arthrokinematics
hip ER
roll: posterior
glide: anterior
closed chain arthrokinematics
hip flexion
roll: anterior
glide: anterior
closed chain arthrokinematics
hip extension
roll: posterior
glide: posterior
closed chain arthrokinematics
hip abduction
roll: superior
glide: superior
closed chain arthrokinematics
hip adduction
roll: inferior
glide: inferior
closed chain arthrokinematics
hip IR
roll: anterior
glide: anterior
closed chain arthrokinematics
hip ER
roll: posterior
glide: posterior
closed kinematic chain
anterior tilt of pelvis closed kinematic chain leads to what hip movement
flexion
closed kinematic chain
posterior tilt of pelvis closed kinematic chain leads to what hip movement
extension
closed kinematic chain
pelvic drop on non weight bearing side will cause
adduction of weight bearing hip
closed kinematic chain
pelvis hike on non weight bearing side will cause
abduction of weight bearing side
closed kinematic chain
forward rotation of pelvis on non weight bearing side causes
IR of hip of stance side
closed kinematic chain
backward rotation of pelvis on NWB side causes
ER of hip on stance side
primary flexors of hip
iliopsoas, sartorius, TFL, rectus femoris, adductor longus, pectineus
muscle force couple
two or more muscles simultaneously produce forces in different linear directions, although the resulting torques act in the same rotary direction
what muscle force couple produces anterior tilt of the pelvis
hip flexors and erector spinae work together in a rotary motion in the same direction
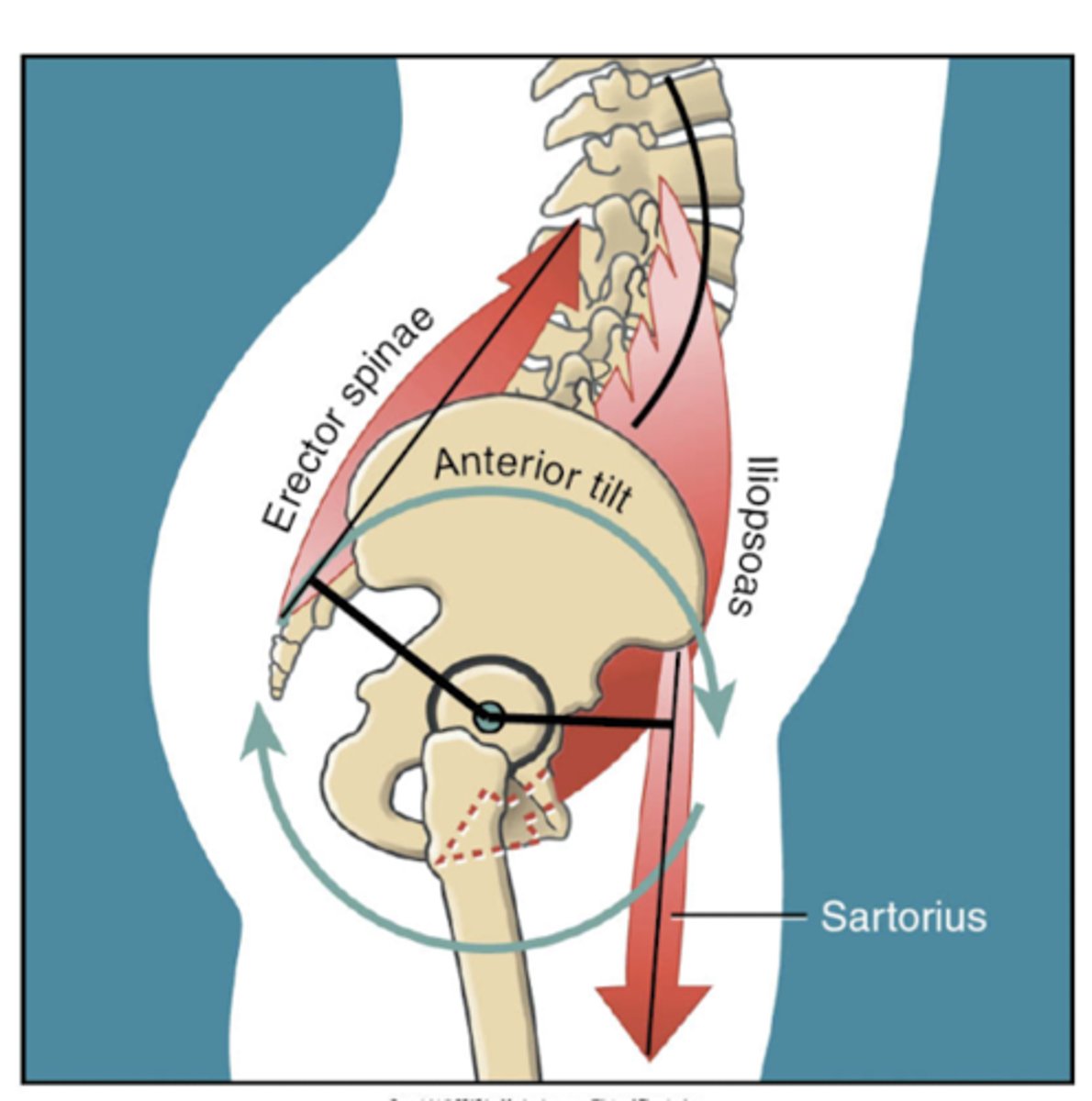
what must contract to keep the pelvis stable, and not tilt anteriorly due to hip flexor tendency
lower abs
primary hip extensors
gluteus maximus, hamstrings, adductor magnus
primary adductors
pectineus, adductor longus, adductor brevis, adductor magnus
what plane do adductors move in
frontal AND sagittal plane
near full flexion, adductors produce what (sagittal plane)
hip extension
near full extension, adductors produce what
hip flexion
primary hip abductors
gluteus medius, TFL, gluteus minimus
What plane do abductors control the pelvis in
frontal plane, preventing contralateral hip drop

what muscle group accounts for most of the compressive forces of the femoral head into the acetabulum
abductors
primary/secondary hip IR at neutral stance
NO PRIMARY HIP IR AT NEUTRAL
Secondary IR: adductors, glute min/med (anterior fibers)
With hip flexion to 90 degrees or more internal rotation torque increases due to changing muscle pull direction.
Some external rotators can even become internal rotators when hip is flexed.
active insufficiency
when a multi joint muscle is not at an optimal length to further shorten and develop maximal force
A muscles force is limited due to its short length (length tension curve)
passive insufficiency
when a multi joint muscle is lengthened beyond its optimal optimal length, thereby passively resisting full motion
a muscle will limit range of motion at a joint because it is over stretched over two joints