Looks like no one added any tags here yet for you.
definition of a depressive disorder
psychiatric disorder characterized by disturbances of mood and/or emotion
DSM-5 criteria for MDD
(a) 5 (or more) of the following present during the same 2-week period; at least one of the symptoms is either 1 or 2
depressed mood
lost of interest or pleasure
weight loss/gain
insomnia or hypersomnia
psychomotor agitation or retardation
fatigue, loss of energy
feelings of worthlessness or guilt
diminished ability to think or concentrate, indecisiveness
recurrent thoughts of death, suicidal ideation without a plan, or a suicide attempt/specific plan
(b) symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
(c) episode not attributable to physiological effects of a substance or other medical condition
(e) there has never been a manic or hypomanic episode
how MDD is assessed and diagnosed
clinical interview
DSM-5 criteria
assessment tools
Beck Depression 21 Item Inventory
MDD: demographic info
liftime risk: 10-20%
~ 1 in 3 women, ~ 1 in 5 men
by age 65
women 2x higher diagnosis rate
3x higher in LGBTQ+ community
affects all age groups & ethnicities
veterans 5X higher rates
most individuals do not seek treatment
~20% of those with untreated MDD attempt suicide
~60% of those who attempt suicide have MDD
heterogeneous disorder
depression: historical info
first written accounts in 2nd millennium BC in Mesopotamia
similar writings in many cultures, including ancient Greeks, Romans, Babylonians, Chinese, Egyptians
Hippocrates (Greek physician) said melancholia caused by excess of black bile in spleen
recommended treatments like bloodletting, baths, exercise, dietary changes
historically viewed as a spiritual condition caused by demonic possession
treated by both physicians and priests
trepanation
1917: Freud theorized depression as a response to real or symbolic loss, leading to unconscious anger & malaise, manifested as depression
psychoanalysis (talk therapy) to resolve unconscious feelings
late 19th, early 20th centuries: depression still thought to be bio based, physiological treatments ensued
frontal lobotomies
go in thru eye socket to remove part of frontal lobe
ECT
1950s: beginning of frequent medication use
stimulants, like Ritalin
still used off-label to augment SSRIs
not FDA-approved
effective at reducing self harm, suicide attempts
trepanation
drilling hole in skull to release evil spirits
did not penetrate brain
used throughout history by Aztecs, Incas, and others
also used during US civil war to remove bullets, fragments, etc.
variation still used today: CRANIOTOMY
relieve pressure in brain due to build up of fluid, blood, pus
also used to relieve build up of blood under toenail
etiologic theories of MDD
monoamine theory
familial/genetic
structural & functional brain differences
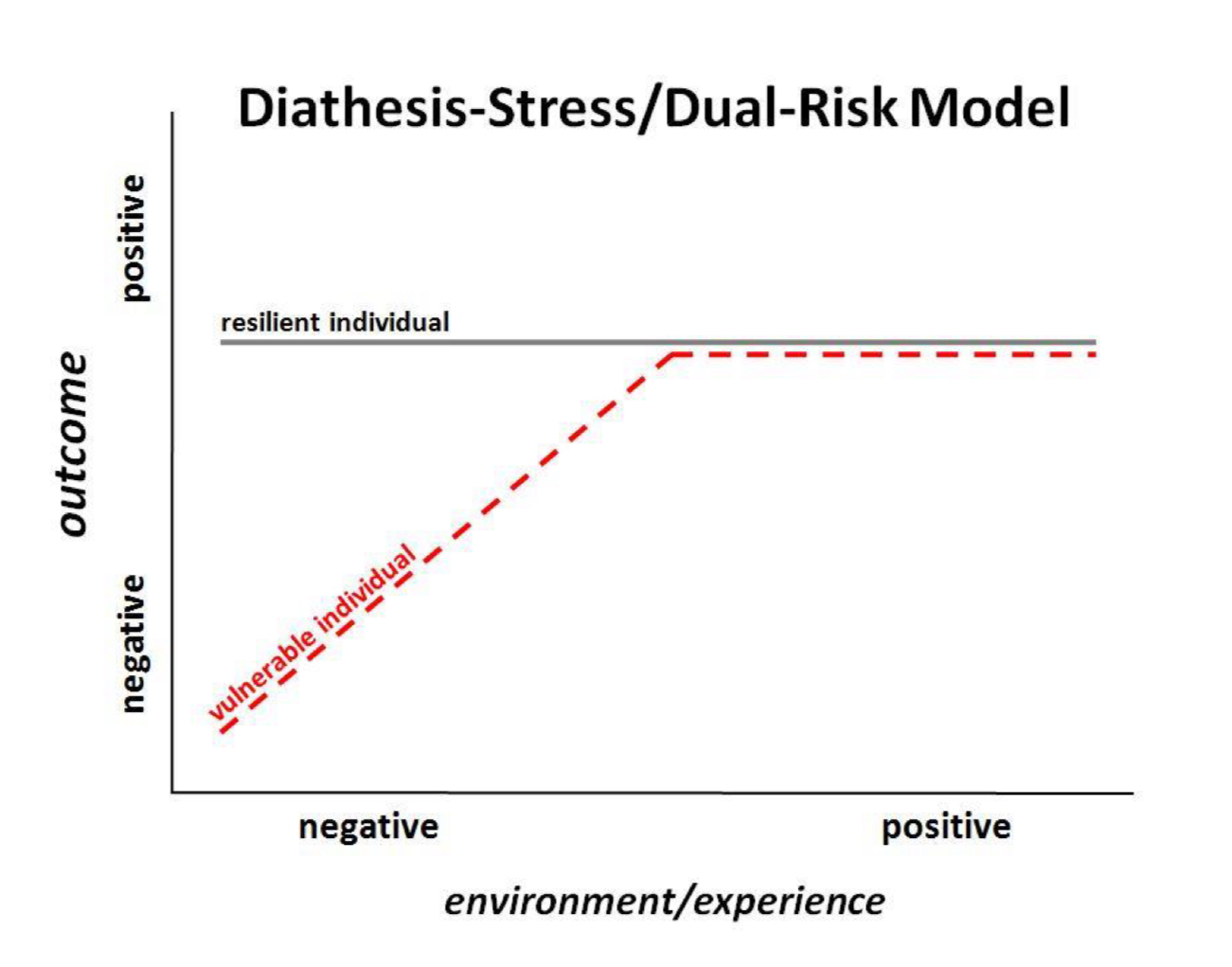
diathesis-stress
MDD: monoamine theory
depression is due to reduced or “imbalanced” levels of monoamines (serotonin, DA, NE) in the brain, particularly serotonin
early 1960s: Reserpine found to produce depressive-like effects in animals and humans treated for hypertension (high BP)
inhibits the vesicular monoamine transporter, depleting monoamine levels
theory was advanced
WRONG
antidepressants alter NTs but many people don’t improve
monoamine depletion in healthy participants DOES NOT produce depressive symptoms
but associated with severity of symptoms
monoamines may play a modulatory role
tryptophan depletion did not rapidly worsen symptoms in patients with MDD
85-90% of the public believes this theory
MDD: familial/genetic
offspring of depressed parents are 3-4x more likely to develop a depressive disorder
MDD does tend to run in families
no gene has been identified as causing MDD
likely result of combined risk factors that may interact with multiple genes
serotonin transpoter gene, COMT gene, TPH, 5-HT, NT receptor genes
MDD: structural findings
wide variety of differences found in those with MDD compared to control
none are unique to MDD
differences in structure of hypothalamus and cerebellum
large volume reductions in the frontal regions
moderate volume reductions in hippocampus, putamen, caudate nucleus
alterations in brain regions presiding over emotional recognition and evaluation
amygdala, hippocampus, insula, prefrontal cortex
MDD: diathesis-stress/dual risk model
treatment of MDD
medication
antidepressants (SSRIs) & augmentation
Prozac, Paxil, Zoloft, etc.
not more effective than older antidepressants (tricyclics), but fewer side effects
SNRIs (e.g., Effexor) can also be effective
cognitive behavioral therapy (CBT)
family therapy
mindfulness interventions
exercise
deep brain stimulation (DBS)
for severe / treatment resistant MDD
CBT
core principles
our thoughts & feelings affect our behavior
our behavior affects our thoughts & feelings
therapy
identify & alter the negative, irrational, distorted thoughts
induce behavior change
more effective over time than meds
changing thought + behavior patterns
ketamine
NMDA (glutamate) receptor antagonist
blocks glutamate postsynaptic receptors (NMDA) and pre synaptic dopamine transporters
unclear if these or other downstream (e.g., increase BDNF) result in the improvement of symptoms
nasal spray (esketamine) FDA approved March 2019 for treatment resistant depression
risk of sedation, dissociation, abuse and misuse, suicidal thoughts and behaviors
pharmacogenetics
genetic testing to identify whether an individual is a poor, ultra/rapid, intermediate, or essential metabolizer of an antidepressant or antipsychotic med before prescription
antidepressant response could be from 42-50% genetically determined
variants of ABCB1 gene associated with concentration levels of various meds in the brain
DSM-5 criteria for Bipolar I Disorder
current or recent Major Depressive Episode
previous Manic Episode or Mixed Episode (at least one)
mood episodes not due to Schizoaffictive Disorder or part of other disorders
DSM-5 criteria for Bipolar II Disorder
current or history of major depressive episodes (one or more)
current or history of hypomanic episode (at least one)
elevated moods that do NOT meet the threshold for mania
no history of manic episode or mixed episode
mood symptoms not due to other disorders
mood swings, but less intense than BP I
symptoms cause significant distress & impairment in social, occupational, or other important areas of functioning
the current episode meets appropriate criteria for hypomania or depression
mania
distinct period of abnormally & persistently elevated, expansive, or irritable mood and goal-directed behavior or energy, lasting at least 1 week and present most of the day, nearly every day
bipolar: demographic info
~ 2.5% of adult population
both BP I and II are more common in females than males
women more likely to experience rapid cycling
manifestation similar across racial/ethnic groups
average age of onset: 25
2/3 have a family member or relative with the disorder
high suicide rate (1 in 5)
bipolar: genetic studies
consistent concordance rate
identical: ~ 0.8
fraternal: ~ 0.2
higher incidence of BP in children with BP parents
no specific gene currently identified as “causing” BP
SEE TEXTBOOK for areas of focus
AKAP11 gene
provides instructions for proteins that may interact with lithium
CACNA1C gene
Ca2+ channel regulation
COMT gene
deactivates monoamines
BDNF gene
associated with increased susceptibility of BP in children & adolescents
BP: structural findings
highly variable findings, not unique to BP
structural differences predominantly observed in
prefrontal & temporal cortex
cingulate gyrus
subcortical regions
greater ventricle enlargement
greater subcortical decline over time
decreased grey matter
mania
cortical thickness remains stable or increases during periods of mania compared to control
limitations of BP research
longitudinal studies needed
confounding variables
comorbidity, medication + substance use
larger sample sizes needed
BP: functional findings
inconsistencies across studies
hypoactivity (decreased activity) of the ventral prefrontal cortex in the right (sometimes left) hemisphere
hyperactivity of the amygdala, basal ganglia, & anterior cingulate cortex in the left (sometimes right) hemisphere
during manic episodes, decreased neural activity response throughout ventrolateral & prefrontal regions during tasks designed to elicit emotional response
treatment approaches for BP
medication
mood stabilizers (lithium)
antipsychotics (Abilify)
anticonvulsants (Tegretol)
2/3 don’t response favorably to first med
CBT
more for depressive symptoms
family therapy
mindfulness interventions
suicide: demographic info
WHO: ~ 700,000 people die by suicide each year
in USA, ~ 45,000 each year
suicide rates in USA have increased by 30% in past 20 years
compared to pre-pandemic, more suicides during COVID-19 in preteens 5-12, young adults 18-24, across all ethnicities
compared to white peers, black youth in USA 2x more likely to attempt without telling anyone
suicide: research with biomarkers
to date, biomarkers do NOT have the sensitivity + specificity needed for clinical utility
examples
cortisol levels
blood protein levels
inflammation C-reactive protein
fMRI scans
resting state activation, functional connectivity, grey matter volumes, etc.
which are neurodevelopment disorders?
ADHD
motor disorders (Tourette’s, tic disorder)
ASD
disorders of learning
tic disorders
Tourette’s
persistent motor OR vocal tic disorder
specify “motor/vocal tics only”
provisional tic disorder
motor AND/OR vocal
tics < 1 year
other
specified: criteria not met (ex: onset after 18)
unspecified: chooses not to specify, insufficient info
what is a tic?
sudden, rapid, recurrent, non-rhythmic stereotyped motor movement or vocalization
common motor tics seen in Tourette’s
simple
eye blinking
shoulder shrugging
eye darting
mouth movements
complex
touching/smelling objects
repeating observed movements
stepping in a certain pattern
obscene gesturing
bending or twisting
hopping
common vocal tics seen in Tourette’s
simple
grunting
throat clearing
complex
palilalia: repeating one’s own words or phrases
echolalia: repeating others’ words or phrases
coprolalia: using vulgar, obscene, or swear words
DSM-5 criteria for Tourette’s Disorder
both multiple motor + at least one vocal tic present
not necessarily concurrently
motor tics usually appear first
tics occur many times a day, nearly every day or intermittently thru a 1 year period
never a tic-free period of more than 3 consecutive months
onset before 18
disturbance not due to direct physiological effects of a substance or condition
Tourette’s: demographic info
1% worldwide prevalence in children 5-18 yrs
onset: common but typically transient in childhood
tics usually emerge in early childhood (4-6), wax + wane
but similar in expression across lifespan
peak severity: 10-12
gradual decline in most cases
small % worsen & continue into adulthood
boys:girls :: 2:1-4:1
occurs in all cultures
2x less common in african-americans and hispanic-americans
symptom characteristics similar across gender, race, ethnicity, and culture
developmental progression of Tourette’s
motor tics usually appear first
EF deficits correlated with symptom severity
stress, anxiety, and fatigue worsen symptoms
comorbid disorders
ADHD
OCD
anxiety
depression
suicide risk
4x greater risk of both committing and attempting suicide
persistence of tics beyond young adulthood and previous attempt are strongest predictors of death by suicide
Tourette’s: genetic findings
no conclusive genetic findings
identical: 50%, fraternal 8%
rates are 3x higher if one or both parents have Tourette’s
focus on DA genes
motor symptoms
worsening of tics with stimulants
improvement with antipsychotics
block DA postsynaptic receptors
80% improve with DA antagonists
brain stimulation in globus pallidus (rich in DA) often improves symptoms
Tourette’s: structural findings
no anatomical pattern for all patients with Tourette’s
several structures + regions smaller in some studies
basal ganglia
anterior cingulate
corpus callosum
occipital
some studies found enlargement of cerebral ventricles
white matter increases in frontal and parietal regions
lower white matter volume bilaterally in prefrontal cortex
greater gray volume in thalamus, hypothalamus, midbrain, insula and sensorimotor cortex
Tourette’s: treatment
antipsychotic medications
clozapine
educational
combo of meds
nicotine patch
THC
DBS
botulism toxin
surgery
lesioning of anterior cingulate
psychotherapy/counseling
biofeedback, relaxation
family therapy
assessment of OCD
similar to psychological evaluations conducted for other disorders
background info & present symptoms (DSM-5)
interviews, observations, assessment tools (rating scales)
Obsessive-Compulsive Inventory (OCI)
DSM-5 criteria for OCD
presence of obsessions, compulsions, or both
the behaviors are aimed at preventing or reducing anxiety/distress
excessive, unrealistic
OC symptoms are not caused by substance or other condition
disturbance not better explained by symptoms of another disorder
OCD: demographic info
~ 1-2% of global population
can occur during childhood, adolescence, or adulthood
typically gradual onset with fluctuations over time
average age of onset varies among studies
before 25
slightly earlier for men than women
extremely limited info regarding minorities
symptoms differ across cultures and genders
childhood: more common in males
adulthood: more common in females
comorbid with anxiety, depression, PTSD, Tourette’s, anorexia
most common obsessions
contamination
harming others
symmetry
sexual
superstitions
most common compulsions
cleaning
checking
ordering
OCD: genetic & NT findings
primarily focused on serotonin, DA, glutamate systems
SSRIs can improve symptoms, serotonin antagonists worsen
dopamine antagonists can improve symptoms, dopamine agonists (stimulants) can worsen symptoms
SAPAP3 gene knock out mice (altered glutamate system) induce or worsen OCD-like behaviors
improvement with glutamate antagonists
heritability component, but values differ among studies
concordance rate for identical twins: 60-80%
OCD: brain function
pathways from basal ganglia to prefrontal cortex are most often implicated in OCD
heightened activation in caudate nucleus, putamen, thalamus, frontal cortex at rest + during provocation
these patterns look similar to controls following ~ 12 weeks of CBT and/or antidepressant therapy
OCD: treatment approaches
CBT
desensitization, exposure therapy
antidepressants
SSRIs and tricyclics
40-60% effective
augmentation with antipsychotic/seizure/anxiety med or CBT improves response rate
severe cases
surgery
cingulotomy: lesioning anterior cingulate
capsulotomy: lesioning part of internal capsule pathways
DBS
TMS
What is ADHD?
A neurodevelopmental disorder characterized by inappropriate levels of inattention, impulsivity, and hyperactivity
Diagnostic criteria for ADHD
Individual presents 1 or both of the following patterns:
(a) For 6 months or more, individual frequently displays at least 6 of the following symptoms of inattention, to a degree that is maladaptive and beyond that shown by most similarly aged persons
Unable to properly attend to details, or frequently makes careless errors
Finds it hard to maintain attention
Fails to listen when spoken to by others
Fails to carry out instructions and finish work
Disorganized
Dislikes or avoids mentally effortful work
Loses items that are needed for successful work
Easily distracted by irrelevant stimuli
Forgets to do many everyday activities
(b) For 6 months or more, individual frequently displays at least 6 of the following symptoms of hyperactivity and impulsivity, to a degree that is maladaptive and beyond that shown by most similarly aged persons
Fidgets, taps hands/feet, or squirms
inappropriately wanders from seat
inappropriately runs or climbs
unable to play quietly
in constant motion
talks excessively
interrupts questioners during discussions
unable to wait for turn
barges in on others convos and activities
Individual displayed some of the symptoms before 12 years of age
Individual shows symptoms in more than 1 setting
individual experiences impaired functioning
3 Subtypes of ADHD
predominantly inattentive
more common in females
hyperactive-impulsive
more common in males
combined
more common in males
ADHD: demographic info
~5-7% US school age population, 3.5% worldwide prevalence
~2.5% of the adult population
Male to female ratio 2:1 in children, adults 1.6:1
Symptoms continued into adulthood, although may attenuate
Commonly co-occurs with depression, conduct disorder, learning disorder, oppositional defiant disorder (behavioral)
MDD: functional findings
inconsistent results across studies
hypoconnectivity in frontal and parietal regions
hyperconnectivity in regions implicated in decision-making and self-referential thinking
reduced global blood flow in prefrontal regions
Tourette’s: functional findings
increase in prefrontal D2 receptors, dopamine transporters, concentration of dopamine and NE metabolites in prefrontal and striatum regions
overactive dopamine transporter system, particularly in basal ganglia
increased presynaptic dopamine activity in caudate and putamen
ADHD: structural findings
widespread volumetric reductions
overall cerebral volume
overall cortical thickness
frontal regions
cerebellum
corpus callosum
amygdala, caudate, hippocampus
reduced white matter density (frontal-stratal tracts)
in normal brain, prefrontal white matter associated with improved inhibition, cognitive skills, reading performance, executive function
not unique to ADHD
ADHD: functional findings
largely fMRI studies, some PET and SPECT scans
frontostriatal pathways have been primary focus
less activation during inhibition tasks
poor task performance
stimulate medication associated with more activation
reduced rCBF and glucose metabolism in frontal regions
stimulants increases rCBF and reduces behavioral symptoms
inconsistent findings with respect to
density of DAT
density of postsynaptic DA receptors
ADHD: genetic findings
biological relatives 5-10x more likely than adoptive
concordance rate higher in identical twins (0.78) than fraternal (0.45)
heritability estimate 70-80%
primary focus is DA related genes
presynaptic DAT gene
postsynaptic DA receptor genes
inconsistent findings
serotonin and other genes also investigated
no definitive answers
prenatal factors associated with increased risk of ADHD
cigarette smoking
drugs/alcohol
inadequate nutrition
pesticide exposure
prematurity
ADHD: treatment approaches
medication
FDA approved
stimulant medications (Adderall, methylphenidate)
non-stimulants (Strattera)
pro-stimulants (Vynanse)
off-label
antidepressants
trigeminal nerve stimulation
behavioral support programs
CBT
child and family education
exercise, meditation, yoga, etc.
gender dysphoria: demographic info
Includes but is not limited to:
• Gender dysphoria typically emerges in childhood & persistence rates into adolescence or adulthood range from 2% to 50% (APA, 2013).
• Most individuals report experiencing gender dysphoria for the first time between ages 3 and 7 years (Zaliznyak, 2021).
• APA reports 2 to 6 times as many males transition to female than females transition to male.
gender dysphoria: treatment options
• Talk Therapy
• Gender Affirming Surgeries
• Hormonal Treatments
• Gender-Affirming Care