Etiology and Pathogenesis- Local Factors, Occlusion, Epidemiology
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
local factors
-factors that influence periodontal health status at a particular site (or sites) with no known systemic effects
-not themselves etiologic factors
-anatomic contributing factors, restorative contributing factors, orthodontic factors
anatomic contributing factors
-proximal contact relation- loose contacts, uneven marginal ridges promote food trapping and create difficulty with hygiene
-cervical enamel projections and enamel pearls
-intermediate bifurcation ridge- convex ridge of cementum that runs from mesial to distal roots of mandibular molar
-root anatomy

-cervical enamel projections
-won’t have attachment of CT with enamel
-projects into furcation area

-enamel pearl
-tends to involve furcation defects
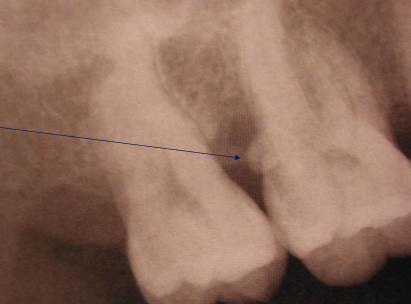
root anatomy
-palatogingival groove
-root trunk length
-root proximity
-root groove

root trunk length
-distance from CEJ to opening of furcation
-shorter means less distance to travel = get to furcation entrance sooner
-difficult to treat area
restorative contributing factors
-overhanging restorations
-margin location
-crown contours
-pontic form
-restorative materials
-overhanging restorations
-plaque retentive
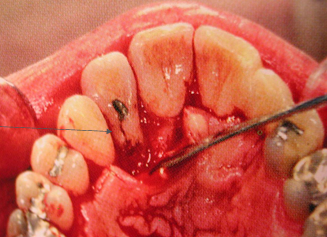
margin location
-inflammation and/or uncontrolled bone loss if restorations impinge on biologic width
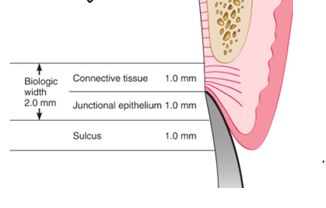
periodontal health is best achieved by placement of restorative margins ___
-supragingivally or at the gingival margin
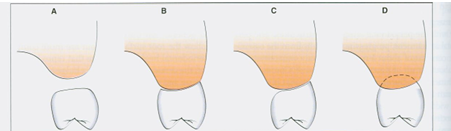
pontic form
A) sanitary pontic- places the convex ridge-facing surface of pontic 3mm or more away from the tissue surface
B) ridge-lap pontic- concave intaglio surface straddling the ridge, difficult to clean adequately with floss
C) modified ridge lap- slightly concave intaglio surface on the facial aspect, but the lingual aspect is convex, allowing better access for plaque removal than ridge-lap
D) ovate- completely convex intaglio surface that extends into a prepared region of the soft tissue, dental floss able to pass in all dimensions, most often used in esthetic regions of the mouth
orthodontic contributing factors
-crowding
-malalignment
-brackets/bands
occlusal trauma
-injury or adaptive change in the periodontal attachment apparatus due to excessive occlusal force
primary v. secondary occlusal trauma
-primary: injury resulting in tissue changes from excessive occlusal forces applied to a tooth or teeth with normal support
-secondary: injury resulting in tissue changes from normal or excessive occlusal forces applied to a tooth or teeth with reduced support
signs of occlusal trauma
-mobility
-widened PDL
-fremitus (palpable or visible movement of a tooth when subjected to occlusal forces)
-occlusal wear

-widening of the PDL
-could happen if restoration is too high on occlusal
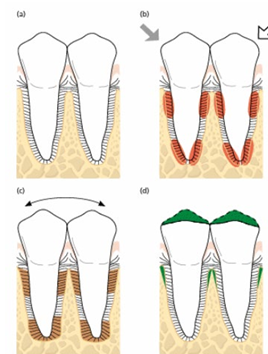
jiggling force study- normal periodontal tissues
-jiggling forces mimic human occlusal forces
-PDL adapts and widens
-once occlusal trauma force is removed, will go back to normal
-there is no bone loss
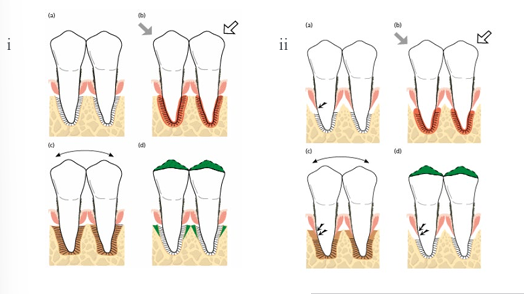
jiggling forces- suprabony and infrabony pockets
-suprabony: jiggling forces did not result in loss of CT attachment, occlusal adjustment reduces the width of the PDL and less mobile teeth
-infrabony: enhanced loss of CT attachment and further downgrowth of the epithelium, occlusal adjustment did not improve attachment levels
key facts related to occlusion
-excessive occlusal forces cannot induce pathologic alterations in supra-alveolar CTs and does not initiate loss of periodontal attachment
-in the presence of inflammation, occlusal trauma MAY accelerate periodontal breakdown
types and purposes of epidemiology
-descriptive: levels of disease, allocation of resources
-analytical: identification of risk factors
-interventional: modulation of risk factors, public health policy
prevalence v. incidence
-prevalence: occurrence (%) of the condition in the population at a given time point
-incidence: occurrence (%) of new cases over a time period
periodontitis- extent and severity
-extent: proportion of the dentition (% of sites) affected by the disease
-severity: magnitude of attachment loss or bone loss, expressed in mm or % of the root length
Scherp 1964
-periodontal disease is a major public health problem affecting 100% of the individuals after the age of 40 (likely an overestimation)
-the disease starts as gingivitis in young age and, if not treated, turns to destructive periodontal disease (last part not true)
-90% of the variance in the prevalence of the disease can be explained through oral hygiene and age (more factors than just these two)
Lindhe 1983
-looked at what happens if you don’t treat periodontal disease, looking at site level
-progression of periodontal disease in adult subjects (Sweden) in the absence of periodontal therapy
-6 year follow-up of 64 untreated patients with periodontal disease
-baseline to 3 years, only 4% showed an attachment loss of more than 2mm
-baseline to 6 years, 11% showed attachment loss of more than 2mm
-showed that not all sites progressed (as previously thought)
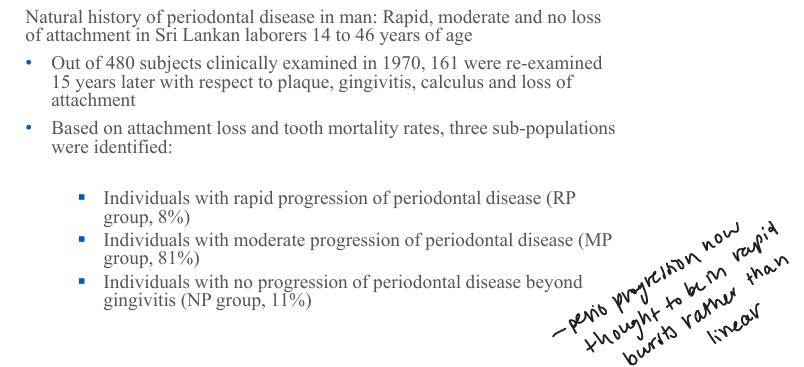
Loe 1986
Hugoson 2006
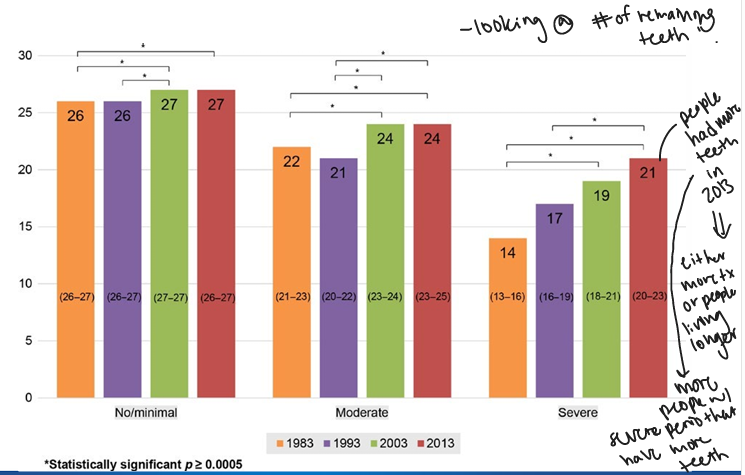
Wahlin 2018
epidemiology of severe periodontitis- current concepts
-1.1 billion cases of severe periodontitis globally
-higher prevalence among “developing” countries/regions
-an 8.5% increase in prevalence rate of severe periodontitis from 1990 to 2019
-global population growth primarily accounts for the increase