15. In Utero & Pubertal Development
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
What is fertilization?
Fertilization, or conception, occurs when a single sperm enters a single egg to produce a zygote
Prior to fertilization, sperm must undergo two processes:
Capacitation
Acrosome reaction (Ovum: zona pellucida)
What are the two key processes sperm must undergo before fertilization, and what do they do?
1. Capacitation:
Occurs in the reproductive tract before sperm can fertilize an egg.
Removes masking proteins from sperm surface → activates enzymes.
Once capacitated, sperm can only live for a few hours.
Prepares sperm to respond to chemical attractants (scent) from the egg.
Enables sperm to swim toward and recognize the egg.
2. Acrosome reaction:
Happens when sperm reaches zona pellucida (egg’s protective layer) → acrosome fuses with zona pellucida
Sperm acrosome membrane releases digestive enzymes.
Enzymes break down zona pellucida, allowing sperm to enter the egg.
Purpose: Both steps are essential for fertilization; capacitation readies the sperm, acrosome reaction allows entry.
How does the conceptus implant in the uterine wall?
2-celled conceptus: Fertilized ovum (sperm + egg)
4-or 8- cell stage: Conceptus’ genes are activated; early cell divisions occur (mechanisms not fully known).
16-cell stage: Conceptus becomes a compact mass of cells called a morula; cells can be counted by technicians.
4 days post-fertilization: Conceptus is swept from the oviducts to the uterus by cilia lining the oviducts. In IVF, conceptus transferred to uterus if environment and hormones are suitable.
32-cell stage: Blastocyst; Develops a fluid-filled cavity and implants itself in the wall of the uterus
6 days: Conceptus secretes the hormone hCG
Significance: Cell stage terminology helps track development and implantation timing in IVF.
During embryonic life, when do the body plan and organ systems develop?
By 2 weeks
ectoderm (outside → nervous system, skin), mesoderm (middle → cardiovascular and musculoskeletal system), and endoderm (inside → gut, lungs)
The embryonic phase of development is complete by 6 weeks postconception at which point the embryo is referred to as a fetus
Subsequent fetal development involves an increase in size and functional maturation of body systems
How is genetic sex determined at fertilization?
Our understanding of sex differentiation is based upon studies by the French embryologist Alfred Jost
Male development depends upon a gene or genes that trigger the development of testes required to masculinize the rest of the body
Female development (with the exception of ovaries) proceeds in the absence of specific genetic instructions
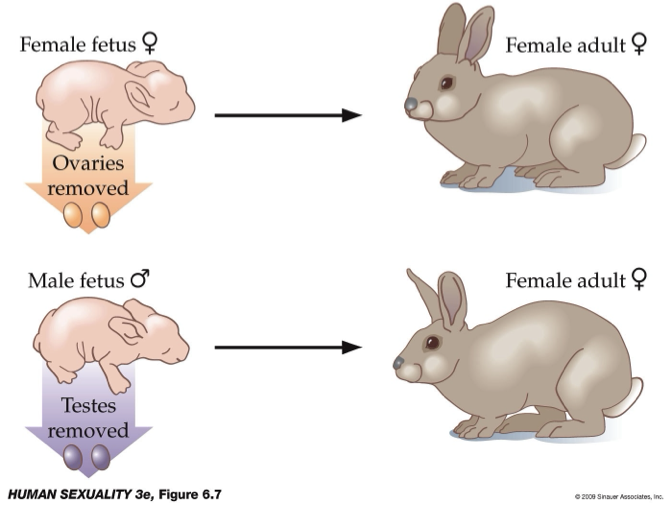
What do animal studies show about the role of hormones in masculinization and sexual behavior?
Method: Removal of ovaries (females) or testes (males) in animal models.
Observation:
Both groups show similar, non-male sexual behavior.
Males without testes do not exhibit mounting behavior.
Conclusion:
Sexual behavior is influenced by hormones (especially testosterone), not just genetics.
Masculinization requires hormonal exposure, not simply male anatomy.
What do all embryos that develop as males and females possess?
All embryos that possess at least one Y chromosome develop as males
The presence of SRY or sex-determining region of the Y chromosome causes the fetus to develop testes
A key gene in ovary development is DAX-1
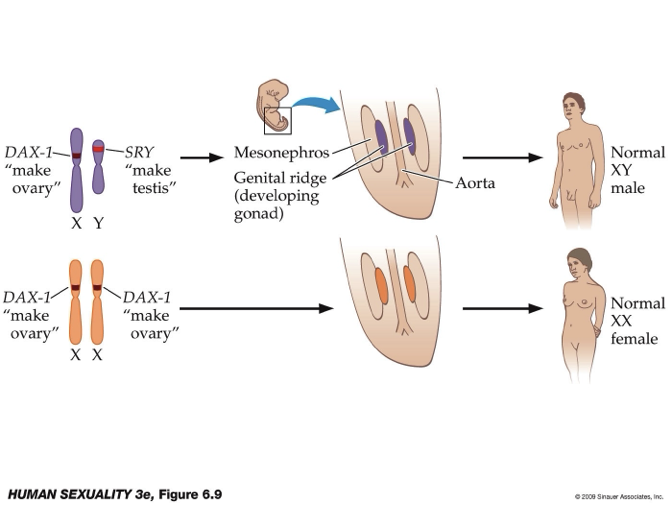
What are the molecular genetics of gonad development?
Chromosomes:
XY (male): Presence of SRY gene (Y chromosome) → dominant → testes develop.
XX (female): No SRY; DAX-1 (X chromosome) promotes ovary development.
Common origin:
Both testes and ovaries develop from the genital ridge (with tissue contribution from mesonephros).
Cell differentiation:
With SRY: → Sertoli cells form → gonads develop into testes.
Without SRY: → Granulosa cells form → gonads develop into ovaries.
Key idea:
Gonadal development depends on SRY presence vs absence; hormones and cell signaling then drive male vs female pathways.
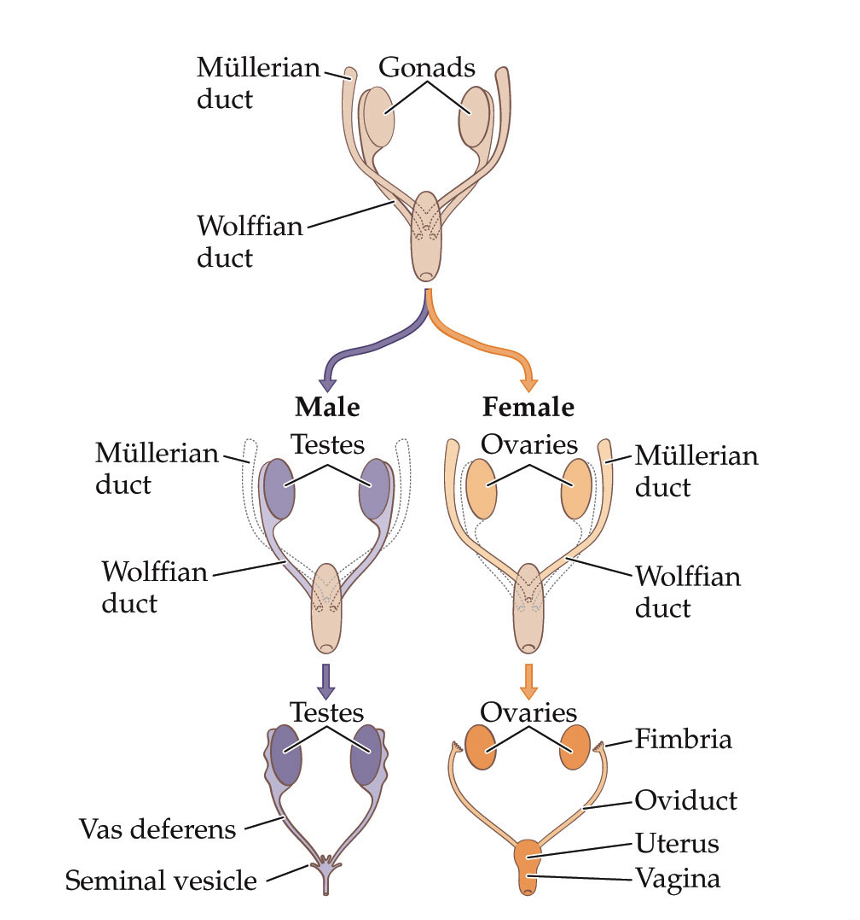
How does sexual development involve the growth and breakdown of precursor structures?
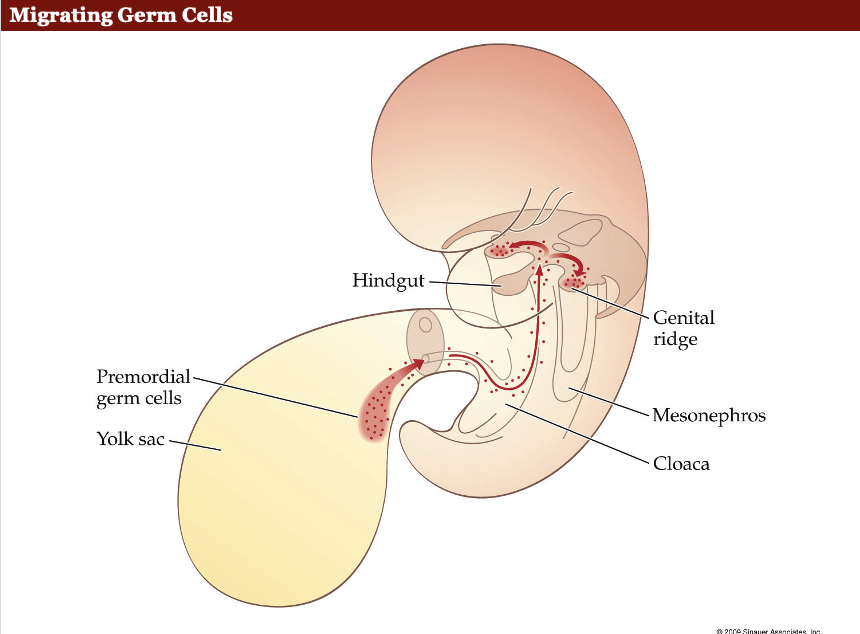
Sperm and ova originate from a group of cells called the yolk sac
At 6 weeks postconception, two sets of ducts run from each gonad to the future site of the external genitalia
Wolffian ducts
Müllerain ducts
Male embryos must regress their Müllerian ducts and development of their Wolffian duct structure must proceed
Female embryos must regress their Wolffian duct structures and development of their Müllerian ducts must proceed
How do primordial germ cells reach the developing gonads during embryonic development?
Primordial germ cells (PGCs): Migrate toward the genital ridge (future gonads).
Mechanism: Guided by chemical signaling/attractants released by the genital ridge.
Evidence: Animal studies show that relocating the genital ridge changes PGC migration direction.
So males and females have identical primordial gonads?
Initially, both males and females have identical primordial gonads
4-6 weeks post conception
Sex-determining region of the Y chromosome (SRY)
Testis-determining factor
Differentiation of Internal organs
First three months: Wolffian + Müllerian system
Presence of testes: Testosterone + anti- Müllerian hormone

How do hormones drive male vs female reproductive development in the embryo?
Male pathway (with SRY/testes-determining factor):
Testes develop → release testosterone + anti-Müllerian hormone (AMH).
Testosterone: supports Wolffian duct → male reproductive structures.
AMH: causes Müllerian duct regression.
Female pathway (no SRY):
No testosterone or AMH → default development.
Müllerian duct persists → female reproductive system develops.
Key idea:
Male = active hormonal process;
Female = default pathway in absence of these hormones.

How do male and female genitalia develop?
Male and female external genitalia develop from the same precursors
In male fetuses, testosterone must be converted to 5α-dihydrotestosterone (DHT) for masculinization of the external genitalia to occur
**Whether it's the genital ridge that activates SRY or SRY that activates the genital ridge is up for debate.
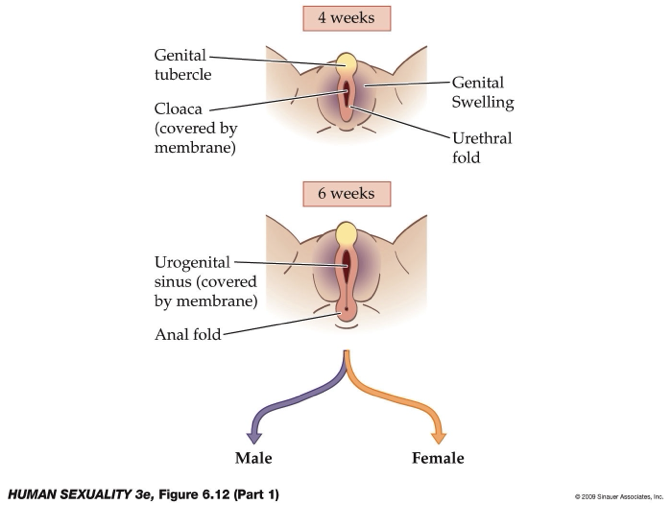
How do hormones and early embryonic structures (4–6 weeks) drive differentiation of male vs female external genitalia?
Hormonal control (critical window ~4–6 weeks):
Requires testosterone, DHT, and anti-Müllerian hormone (AMH) for male development.
If absent/low or receptor defects → development shifts toward female-like (default) phenotype (not fully female).
DHT is key for external male genitalia (acts via DHT receptors).
Common early structures (both sexes):
Cloaca: primitive opening, covered by membrane.
Urethral folds (→ labia minora / penile shaft).
Genital swelling (→ labia majora / scrotum).
Genital tubercle (→ clitoris / glans penis).
Urogenital sinus: essential for external genitalia development.
Male differentiation (with DHT receptors):
Urethral folds → penile shaft
Genital swelling → scrotum
Genital tubercle → glans penis
Female differentiation (default):
Genital swelling → labia majora
Urethral folds → labia minora
Genital tubercle → glans of clitoris
Key concepts:
Differentiation depends on hormone presence + receptor function.
Disruptions (hormones, receptors, endocrine factors) → ambiguous/intersex development.
Many variations are due to hormonal mediation, not just genetics.
How do the gonads descend during development?
Site of origin: Upper lumbar region
10 weeks post-conception: At rim of pelvis
Males (6-7 months post-conception): Descend into pelvis, enter scrotum
Males
Gubernacula: Fibrous band (part of this band facilitates development of spermatic cord)
Attachment between testis and abdominal wall
As testes enter the scrotum, they bring along various structures that contribute to spermatic cord
How can early hormonal exposure influence later sexual behaviour?
Experiments in rodents reveal both organizational (in utero to organize organs and brain) and activational actions of hormones (sexual maturity)
Primates exhibit multiple sensitive periods during which hormonal effects can impact subsequent behaviour
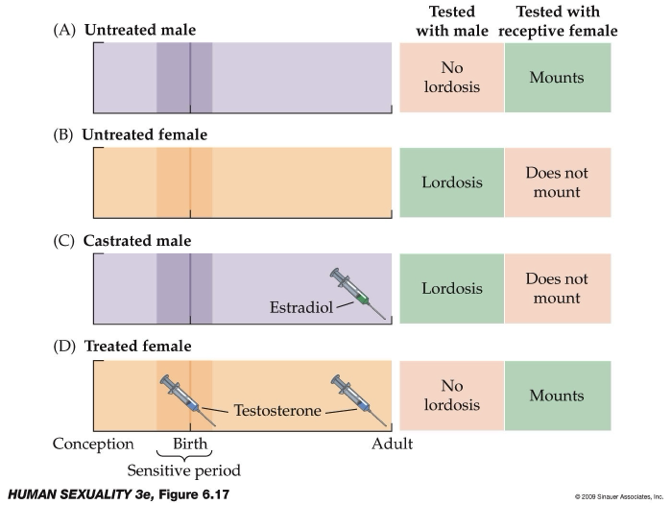
What do animal studies reveal about hormonal control of sexual behavior (mounting vs lordosis)?
Behaviors:
Mounting = male-typical behavior.
Lordosis = female-typical posture (facilitates sperm transfer).
Normal patterns:
Untreated males → mounting.
Untreated females → lordosis.
Experimental findings:
Castrated males + estradiol (in adulthood) → show lordosis (female behavior).
Females + testosterone (at birth + adulthood) → show mounting (male behavior).
Key concepts:
Sensitive period: Hormones organize brain (early life; birth in rodents, prenatal in humans).
Hormones (testosterone/estradiol) shape brain circuits, not just reproductive organs.
The brain, specifically the hypothalamus, is central in controlling sexual behaviour.
Hormones can override genetic sex in determining behavior.
How does puberty mark sexual maturation?
Puberty is the biological transition to sexual maturity
Pubertal growth spurts occur earlier in girls than in boys
In girls, breast development proceeds through many stages and the onset of menstruation, or menarche, is a dramatic event in female pubertal development
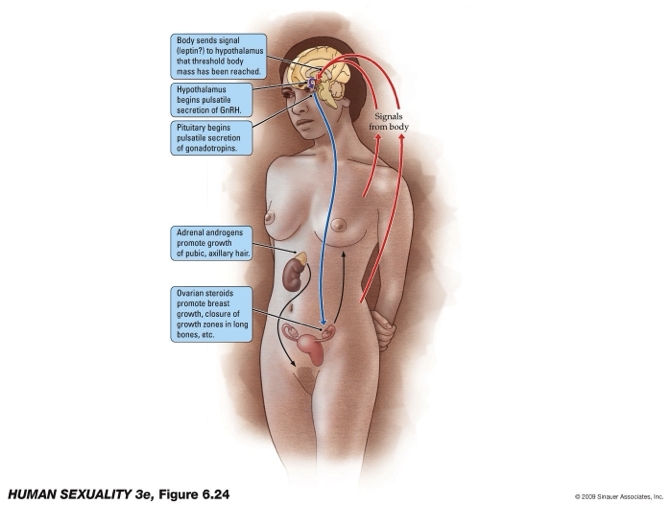
What is one proposed mechanism that initiates puberty, and how does it activate the reproductive system
Key trigger (theory): Increase in body fat → leptin release.
Leptin role: Signals hypothalamus that energy stores are sufficient for reproduction (pregnancy).
Hormonal cascade:
Hypothalamus → pulsatile GnRH release
Pituitary → gonadotropins (LH, FSH)
Gonads/adrenals → sex hormones (estrogen, progesterone, androgens)
Effects:
Development of secondary sexual characteristics (e.g., breasts, body changes).
Estradiol → important for growth plate closure (height regulation).
Key idea: Puberty is initiated by metabolic signals (fat/leptin) activating the HPG axis.