Right Ventricle (AE exam)
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
What is the right ventricle function?
Ejects deoxygenated blood into the pulmonary artery.
What is the RV Location?
Anterior to the left ventricle. To the left of the sternum
What is the RV Shape? With what base? when viewed from the side its what shape? when viewed in Cross section it’s what shaped?
It’s crescent shaped with a triangular base. When viewed from the side…It’s triangular in shape. When viewed in cross section it’s crescent shaped.
what determines the RV shape?
The Interventricular septum determines the RV shape
What are the RV 3 sections
Inlet
Trabecular (Apical)
Outlet
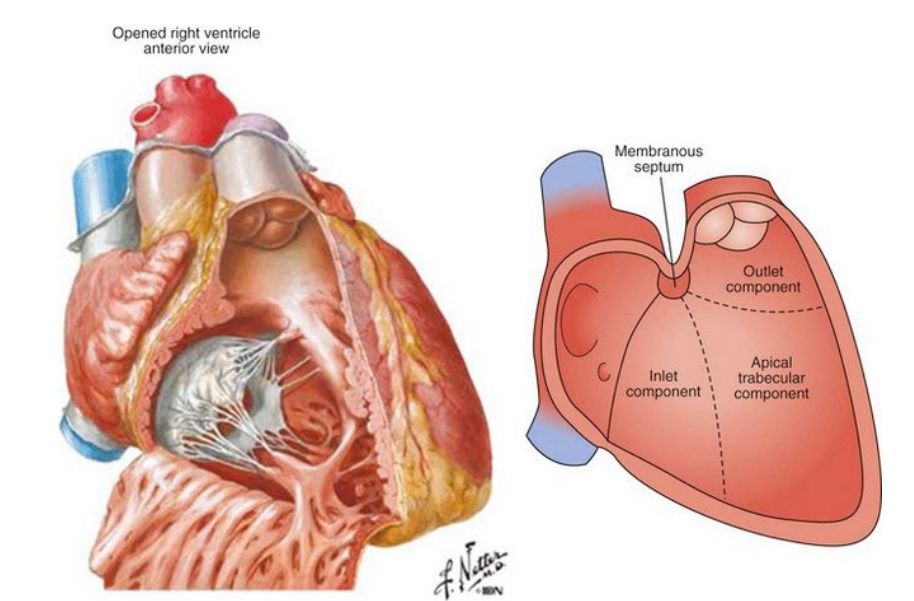
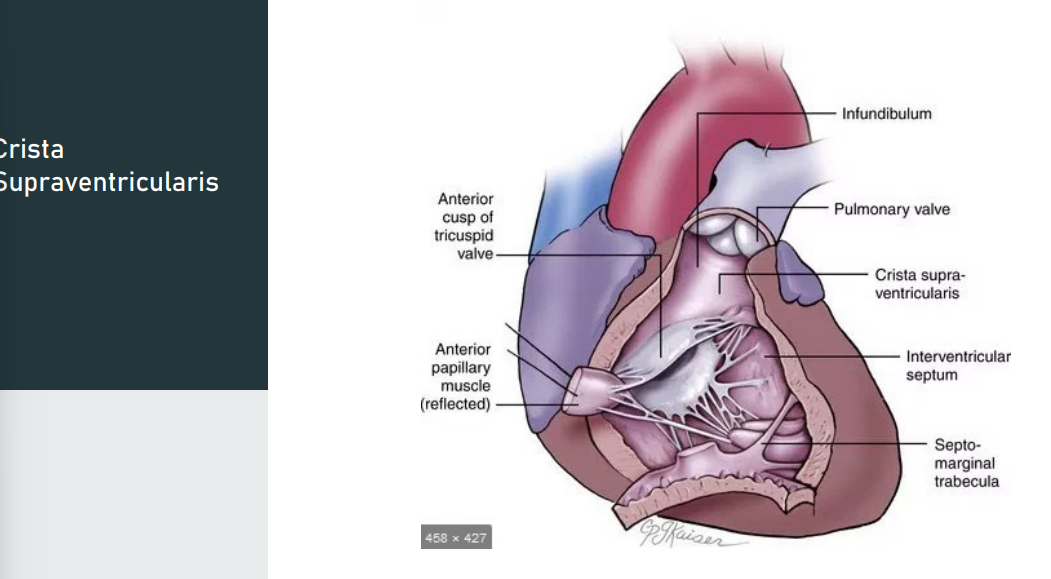
The Crista Supraventricularis, what does it separates?
Separates: the inlet (TV) portion from the outlet (PV) portion
what is the Crista Supraventricularis description and its shape, what are also found in the RV?
Description: prominent muscular ridge formed by the parietal muscle band and the infundibular septum
Shape: arch shaped
*2 other muscle bands are found in the RV
parietal" refers to the part of this muscular ridge that extends along the parietal wall (free wall) of the right ventricle, specifically between the tricuspid and pulmonary valves
What are the muscular bands of the RV
Three Muscular Bands:
Moderator band
Parietal band
Septal band
Moderator Band: what is the description? what is the location? where does it extends? what is the function?
Description: thick intracardiac muscle
Location: the central portion of the RV
Extends: The interventricular septum to the anterior papillary muscle
Function: carries part of the conduction system of the heart to the anterior papillary muscle.
Due to the shape, we must use do what to interrogate the walls and sections of the right ventricle.
Due to the shape, we must use multiple views to interrogate the walls and sections of the right ventricle.
Name the RV walls
Anterior wall
Lateral wall
Inferior wall
What is the primary blood supply for the right ventricle?
The right coronary artery is the primary blood supply for the right ventricle.
Coronary blood flow to the RV occurs during what cardiac cycle?
Coronary blood flow to the RV occurs during both diastole and systole
The conus artery from the RCA supplies blood flow to what?
The conus artery from the RCA supplies blood flow to the infundibulum
The RV is more tolerant of what due to what?
The RV is more tolerant of ischemia due to a redundant blood supply and lower metabolic demand
Three Papillary muscles that contract during when to do what?
Three Papillary muscles that contract during systole to close the inflow valve
Three Papillary muscles that contract during systole to close the inflow valve, what are the three papillary muscles?
Anterior papillary muscle
Posterior papillary muscle
Septal (medial) papillary muscle
What is the Anterior papillary muscle – located
Anterior papillary muscle – located on the anterior wall
Posterior papillary muscle – located
Posterior papillary muscle – located on the RV free wall
Septal (medial) papillary muscle attach to what
Septal (medial) papillary muscle – attached to the interventricular septum
Infundibular Septum, define
Its a intracardiac structure that separates what? beneath where?
And its the what wall of the what?
Intracardiac structure that separates the two ventricular outflow tracts beneath the right and left cusps of both semilunar valves.
Smooth walled outflow tract
The RV is susceptible to various conditions: what are they name 7
•Pulmonary hypertension
•Regional wall motion abnormalities from Right coronary artery disease •
pericardial diseases
•acute pulmonary embolism
•rhythm disturbances
•Congenital heart disease
•heart failure
What can The RV experience?
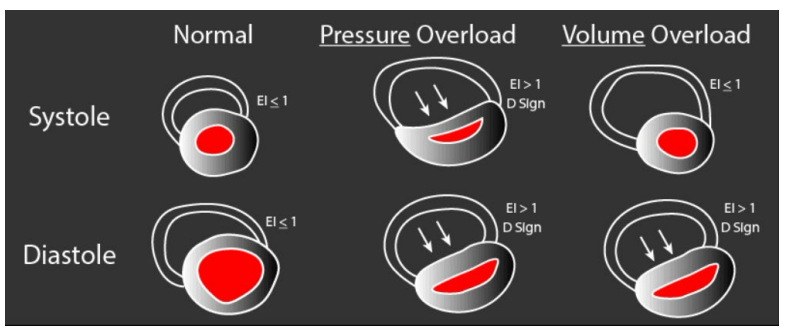
The RV can experience volume overload and pressure overload and experience enlargement and hypertrophy
-Volume overloading of the RV causes the septum to be what and and this is during what phase of the cardiac cycle?
Volume overloading of the RV causes the septum flattens during the diastolic phase of the cardiac cycle
-Pressure overload of the RV from an what causes the what septum to become what during which phase of the cardiac cycle?
-Pressure overload of the RV from an elevated afterload or resistance causes the interventricular septum to flattens during systole
When pressures in the RV increase (in diastole or systole or both), the LV assumes a what shaped configuration with what happening to the septum?
When pressures in the RV increase (in diastole or systole or both), the LV assumes a ‘D’ shaped configuration, with flattening of the septum
The position and configuration of the interventricular septum depends on what?
The position and configuration of the interventricular septum depends on the pressure gradient between the LV and RV during the cardiac cycle.
analysis of septal motion for ventricular interdependence requires absence of what?
analysis of septal motion for ventricular interdependence requires absence of paradoxical septal motion from other causes (e.g. LBBB, RV pacing, etc.)
an abnormal, anterior (outward) movement of the heart's septum toward the right ventricle during systole, rather than the normal inward movement toward the left ventricle. Commonly known as "septal bounce" or "abnormal septal motion", it frequently indicates RV overload, conduction issues,
D-shaped left ventricle evidenced during what cardaic cycle and suggest what RV pressure overload?
D-shaped left ventricle evidenced during systole (particularly endsystole) suggests RV pressure overload
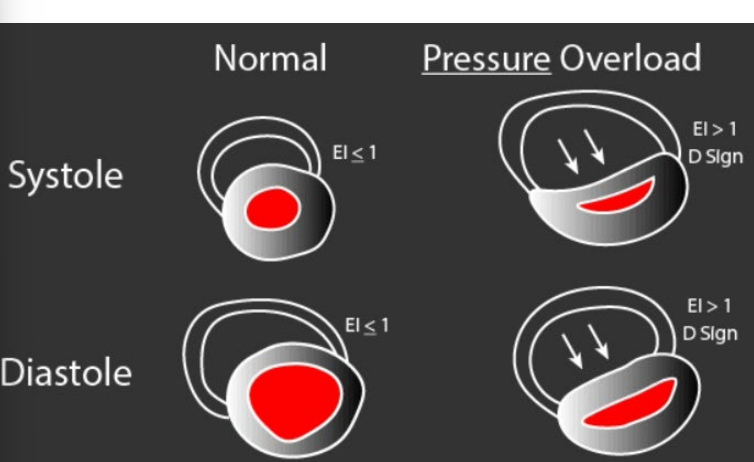
A D-shaped ventricle in what cardiac cycle suggests RV volume overload?
a D-shaped ventricle in diastole suggests RV volume overload
Right Ventricle Size Measurements:
The essential views for measurement of the RV are what name 4
Left parasternal long-axis view (PLAX)
Left parasternal short-axis view (PSAX)
Apical 4-chamber view
Subcostal views
How do measure the RV in PLAX and whats the abnormal number?
Diameter measured at end diastole.
Inner edge of RV to the septal aortic junction.
Abnormal is >3.0 cm
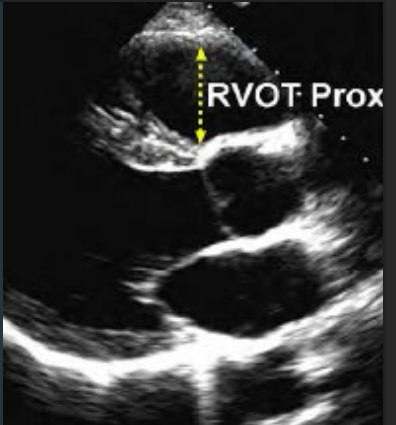
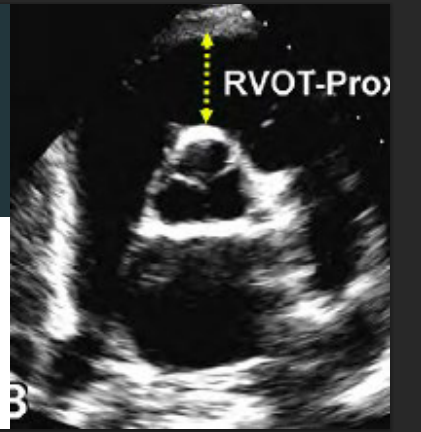
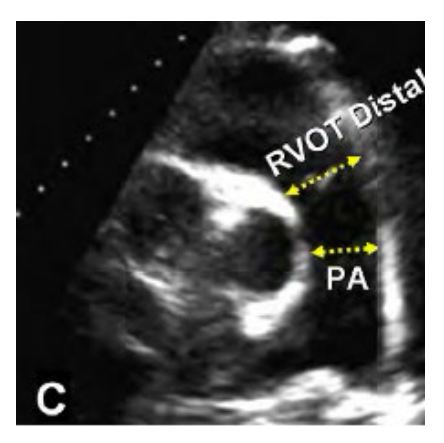
How do you measure the RV diameter in PSAX at the great vessel view prox?
Whats the abnormal number?
Diameter measured at end diastole.
Inner edge of RV to the aortic root
Abnormal is >3.5 cm
ow do you measure the RV diameter in PSAX at the great vessel view Distal, whats the abnormal diameter number?
RVOT distal diameter measured at end diastole. Inner edge to inner edge just proximal to the pulmonic valve
Abnormal is a Diameter > 2.5 cm
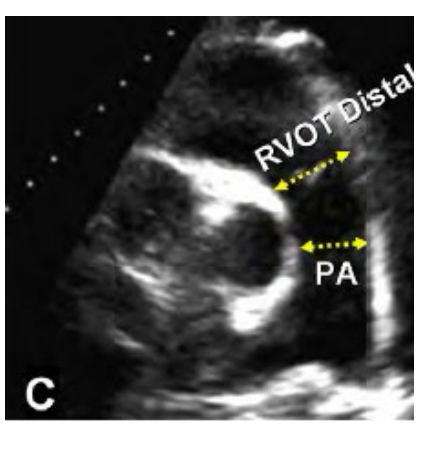
How is the main Pulmonary artery measured and what is the abnormal number?
Main Pulmonary artery is measured inner edge to inner edge at end diastole at the mid point.
Abnormal is > 2.0 cm
Quantification—LV eccentricity index:
Ratio between what and on what view?
Normal LV/RV relative?
Eccentricity index = ?
Eccentricity index should be evaluated over what?
Quantification—LV eccentricity index:
Ratio between LV anteroposterior diameter and LV septal-lateral dimension (on PSAX view)
Normal LV/RV relative pressures → LV appears round → index = 1
Eccentricity index >1 (antero-posterior diameter larger than septal–lateral diameter) → RV overload
Eccentricity index should be evaluated over the cardiac cycle
What is the LV Eccentricity Index?
👉 It’s a measurement that tells you if the RV is pushing on the LV
📏 The Formula (what you measure)
In PSAX view, you measure:
Anteroposterior diameter (front → back)
Septal-lateral diameter (septum → free wall)
👉 Then:
Eccentricity Index=Anteroposterior diameterSeptal-lateral diameter\text{Eccentricity Index} = \frac{\text{Anteroposterior diameter}}{\text{Septal-lateral diameter}}Eccentricity Index=Septal-lateral diameterAnteroposterior diameter
🔵 What does NORMAL look like?
LV = round
Both diameters are equal
👉 Index = 1
✅ Means:
Normal RV pressure
No septal flattening
🔴 What happens when RV pressure/volume increases?
👉 The RV pushes the septum toward the LV
LV becomes D-shaped
Septal-lateral diameter ↓
Anteroposterior diameter ↑ (relatively)
👉 So:
Index > 1
🚨 KEY INTERPRETATION 👉 Eccentricity Index > 1 = RV overload
This could be:
Pressure overload (pulmonary hypertension)
Volume overload (TR, ASD)
⏱ WHY “evaluate over the cardiac cycle”?
This is where people get confused — but it’s HUGE for exams:
🟢 If abnormal mainly in diastole:
→ Volume overload
🔴 If abnormal in systole AND diastole (worse in systole):
→ Pressure overload
🔥 Super Simple Way to Think About It
👉 LV shape tells you what the RV is doing
Round LV → normal
D-shaped LV → RV problem
When it happens tells you WHAT kind of problem
🧠 Exam Quick Hits (memorize these)
Normal index = 1
Index > 1 = RV overload
Measure in PSAX
Look at timing (systole vs diastole)
RV volume overload: Examples: chronic severe TR, large ASD, severe PI
septal shift noted mainly at what cardiac cycle?
Eccentricity index = ?
RV volume overload:
Examples: chronic severe TR, large ASD, severe PI
Septal shift noted mainly at end diastole
Eccentricity index = 1 at end systole, increased at end diastole
RV pressure overload: Examples: pulmonary hypertension, pulmonic stenosis
septal shift is seen during what cardiac cycle and when is most pronounced?
Eccentricity index = ?
RV pressure overload: Examples: pulmonary hypertension, pulmonic stenosis
Septal shift seen both at end systole and end diastole (most pronounced at end systole)
Eccentricity index >1 at end diastole and end systole
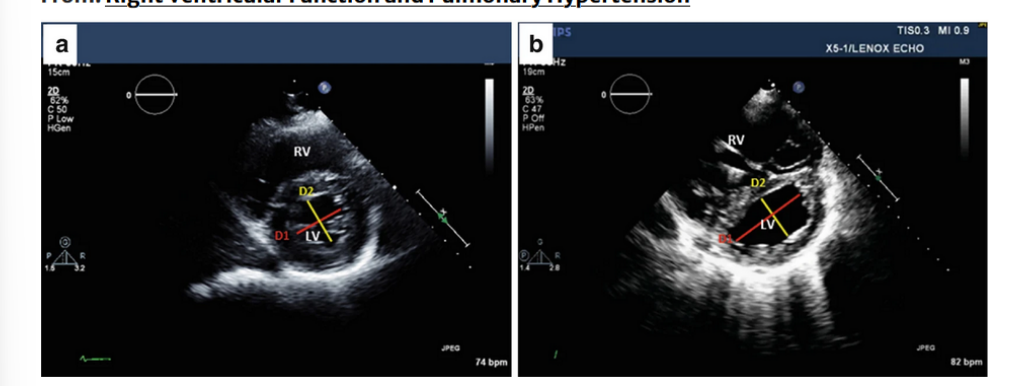
RV/LV interdependence-Eccentricity index. (a) Normal right and left ventricular morphology:
the left ventricle has a what shape configuration; the ratio of the what (D1) to the what (D2) is clost to what number?
Right ventricular overload, the LV takes a what shape, and then what flattens? and what dimension of the what is greater then the what?
RV/LV interdependence-Eccentricity index.
(a) Normal right and left ventricular morphology: the left ventricle has a round configuration; the ratio of the antero-posterior dimension (D1) to the septal-lateral dimension (D2) is close to
1. (b) Right ventricular overload, the LV takes a crescentshape, the interventricular septum flattens, and antero-posterior dimension of the left ventricle is greaterthan the septal-lateral
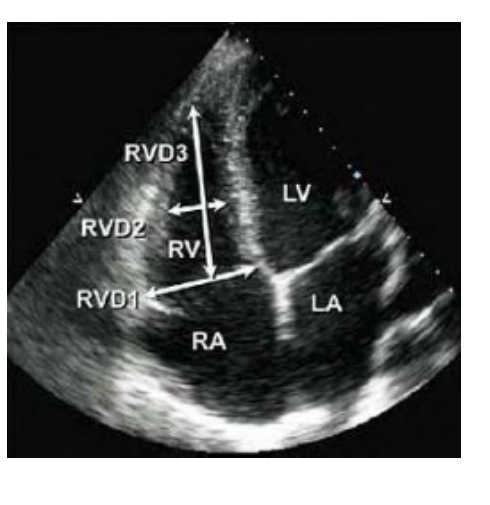
Right Ventricle Measurements Obtained from what view, at what cardiac cycle,
base diameter is made in where and tell me the way you would measure this?
The mid cavity diameter is made where and tell me how you would measure this?
abnormal Diameter is what number at the base and what number at the mid level what does this abnormal numbers indicated?
what is the abnormal longitudinal dimension?
Obtained from an Apical 4 chamber view at end diastole.
Base diameter is made in the RV near the TV insertion inner edge to inner edge
Mid cavity diameter is made at the level of papillary muscles inner edge to inner edge
Abnormal Diameter is > 4.1 cm at the base and
> 3.5 cm at the mid level
(indicates RV dilatation)
Abnormal longitudinal dimension is > 8.3 cm
Fractional Area of Change, trace what border ? you want to start from where to the where and back to you started.
make measuremnet during what cardiac cycle ?
Trace the endocardial tissue border from the tricuspid annulus to apex back to the tricuspid annulus. Make measurement at both end diastole and end systole.
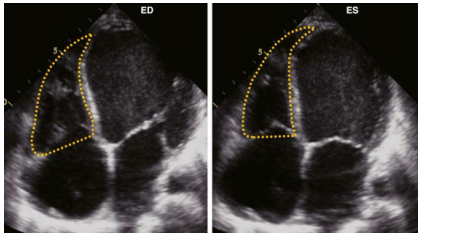
FAC reflects what?
what is the normal and abnormal %
FAC reflects both longitudinal and radial components of RV systolic contraction
Normal >35%
Abnormal < 35%
. Longitudinal contraction
Movement from base → apex
Think: tricuspid annulus moving downward
This is the MAIN way the RV contracts
🔴 2. Radial contraction
Movement of the free wall inward
Think: RV walls squeezing toward the center
💡 Why this matters
Some measurements only look at ONE type of motion:
TAPSE → only longitudinal
S’ (TDI) → only longitudinal
👉 But FAC = BOTH longitudinal + radial
🔥 Why FAC is useful
👉 It gives a more complete picture of RV function
Because:
RV contraction is complex (not just one direction)
FAC includes global function
🧠 Easy way to remember
👉 FAC = “Full RV squeeze”
Longitudinal ↓
Radial inward
BOTH included ✅
🚨 Exam tip
If you see:
👉 “Which measurement reflects both longitudinal and radial RV function?”
✅ Answer: FAC
what is the FAC equation?
(RV ED Area- ES Area) / ED Area = FAC
RA severity scale this valves will = to what?
RA area
RA length
RA diameter
RA area > 18 cm2 - i think now 19
RA length > 53 mm
RA diameter > 44 mm
= Right Atrial Enlargement (RAE)
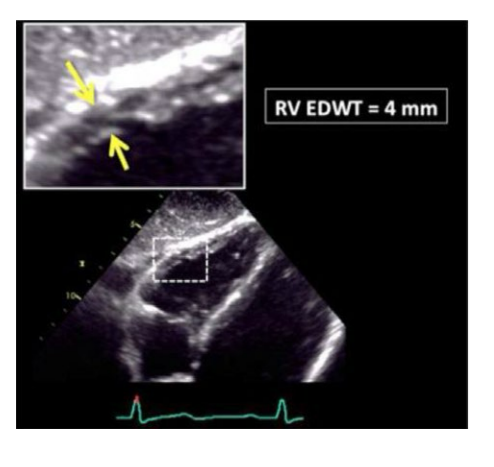
Wall thickness is obtained from what view during which cardiac cycle and what do you want to zoom on?
A thickness of what number is abnormal
what is normal
Wall thickness is obtained from the Subcostal view at end diastole.
Zoom on mid RV wall
A thickness of >5mm is abnormal
<5mmis normal
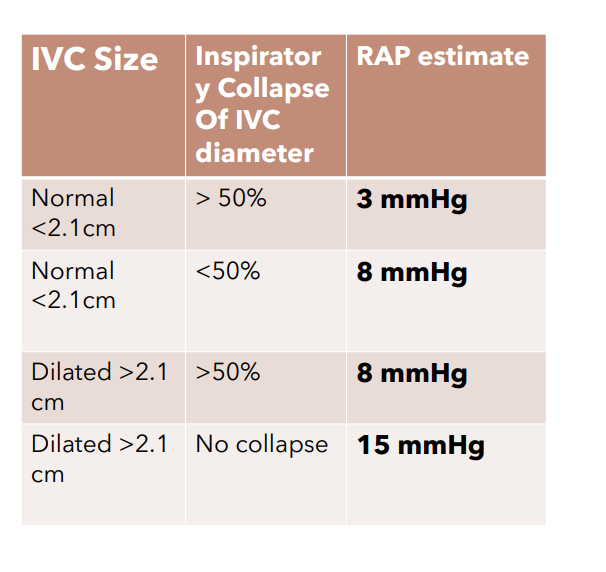
Estimation of RA Pressure from IVC
tell me the chart?
IVC size, Inspiratory collapse of IVC diameter
RAP estimate
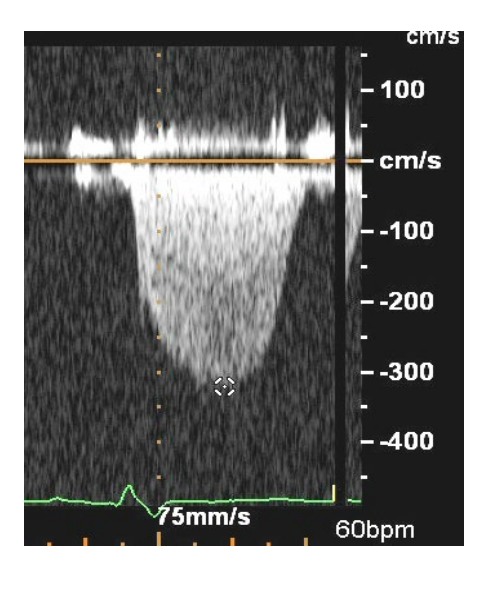
what does this image show?
PIG of Tricuspid Regurgitation
RIGHT VENTRICLE : HEMODYNAMICS
Normal RA pressure =
Normal oxygen saturation =
Normal RA pressure = 2 - 8mmHg
Normal oxygen saturation = 75%
RIGHT VENTRICLE : HEMODYNAMICS
Normal RV pressure, systole and diastole
Systole = 15 – (25)30mmHg (RVSP)
• Diastole = 2 - 8mmHg (RVDP)
RVSP mmHg =
4( TR peak jet velocity 2) + RAP
Normal pulmonary artery pressure systole and diastole
PASP = RVSP when?
Normal pulmonary artery pressure
Systole = 15 - 30mmHg (PASP)
Diastole = 2 - 8mmHg (PADP)
*PASP = RVSP in the absence of RVOT obstruction
Normal mean pulmonary pressure =
MPAP mmHg =
Normal mean pulmonary pressure • 9 – 18mmHg
MPAP mmHg = • 4 x (PI peak velocity2)
Pulmonary artery end diastolic pressure (PAEDP) Normal = ?
whats the equation?
Pulmonary artery end diastolic pressure (PAEDP)
Normal = 4 to 12mmHg
PAEDP = 4 x (PI End Diastolic velocity2) + RAP
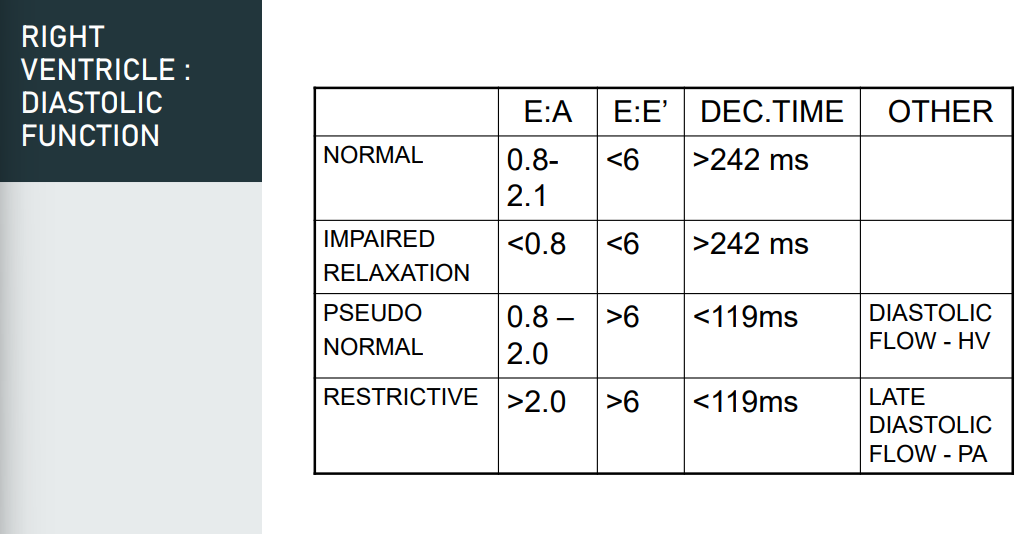
RIGHT VENTRICLE: DIASTOLIC FUNCTION
what are the imaging guidelines name 4
Imaging guidelines
1. Pulse wave Doppler TV
2. Tissue Doppler TV lateral annulus
3. Pulse wave Doppler hepatic veins
4. IVC size & collapsibility *end expiration