Lungs Part 1 (E1)
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
43 Terms
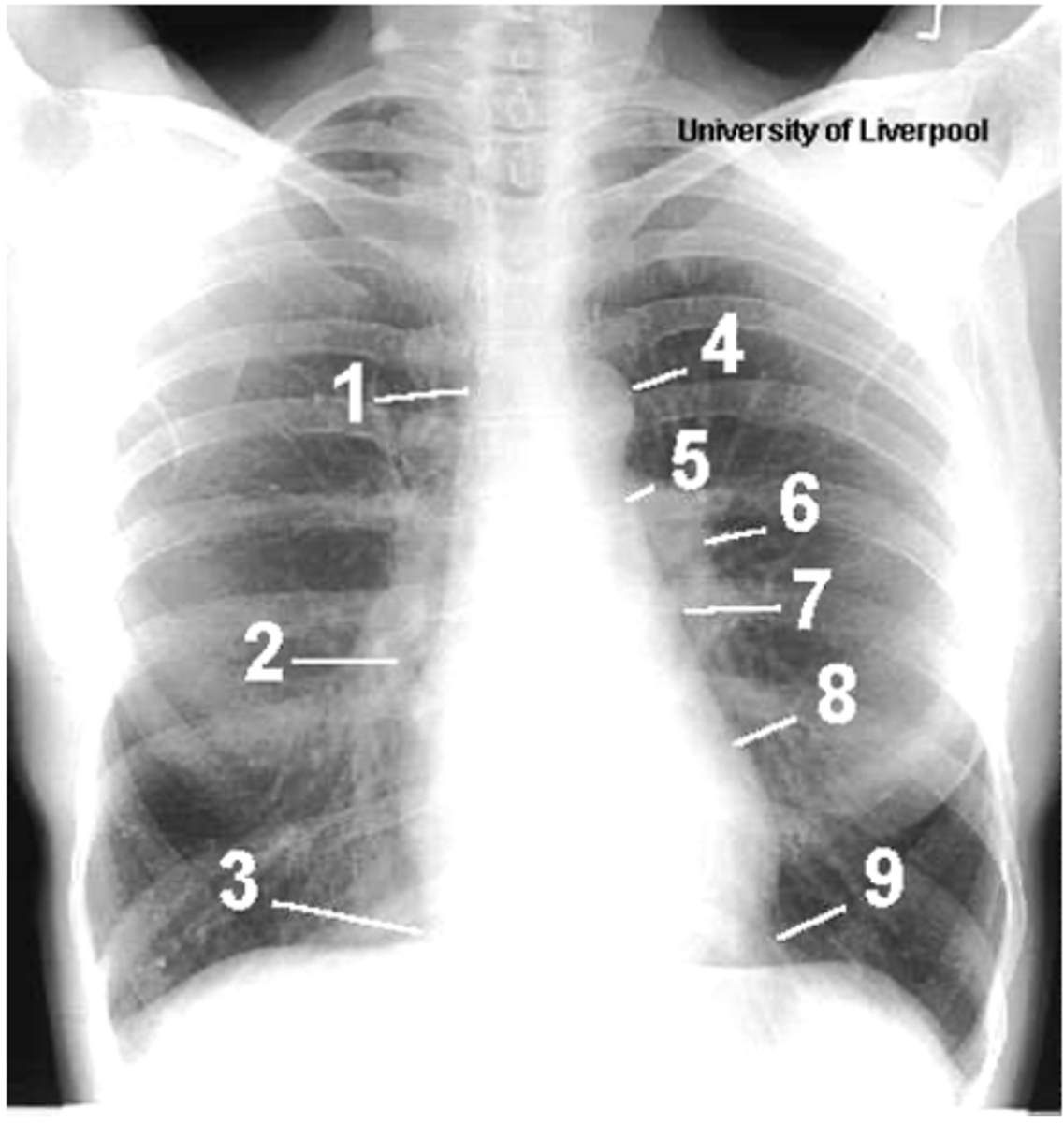
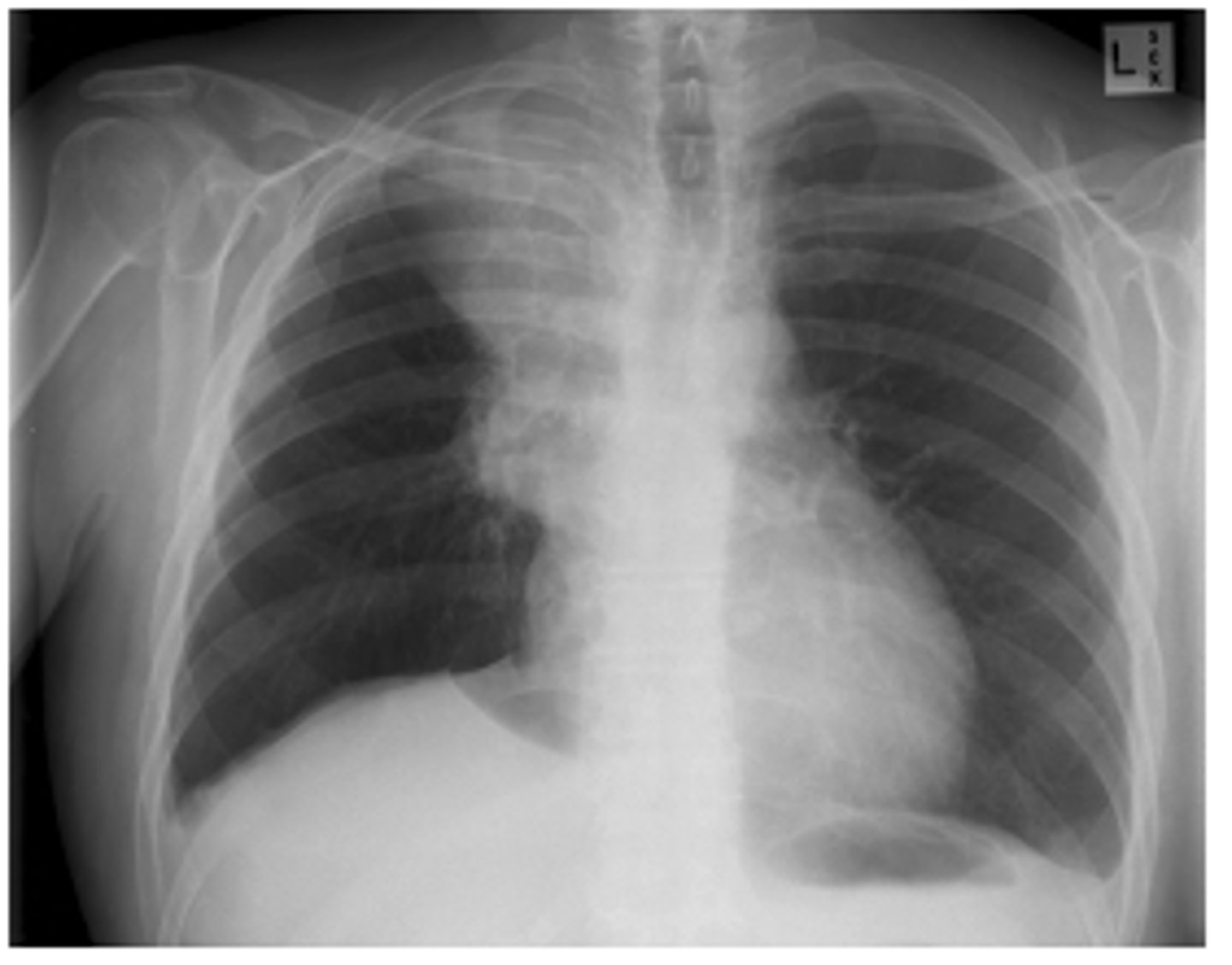
ID structures
1- superior vena cava
2- right atrium
3- inferior vena cava
4- aortic arch or knob
5- left pulmonary trunk
6- left pulmonary artery
7- left atrium
8- left ventricle
9- left cardiophrenic angle
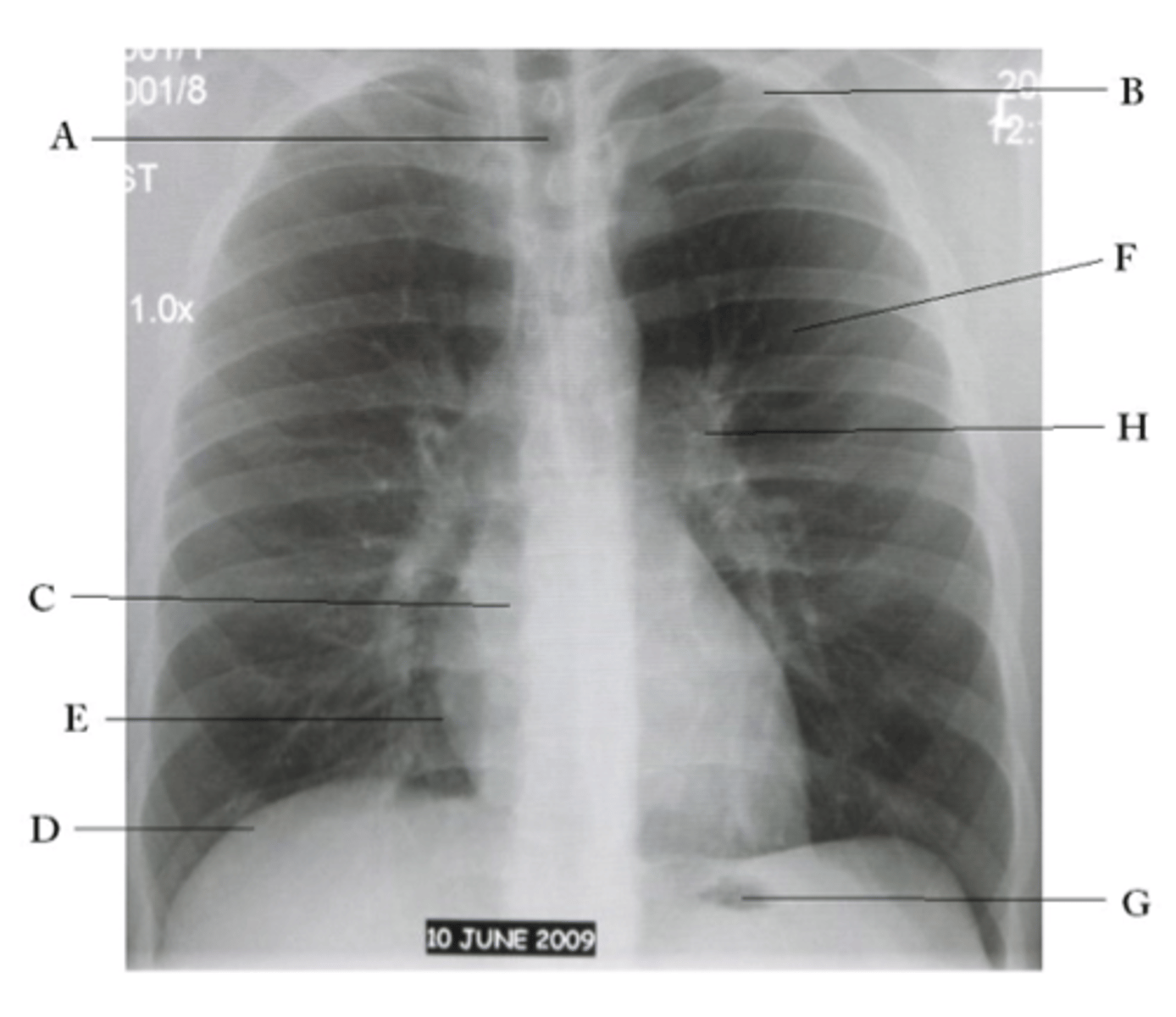
ID structures
oA - Trachea
oB - Clavicle
oC - Right Atrium
oD - Diaphragm
oE - Cardiophrenic angle (Costocardio)
oF - Left upper lobe
oG - Gastric Bubble
oH - Left Hilum
Define interstitial
tissue outside of the alveoli are affected. (diffuse)
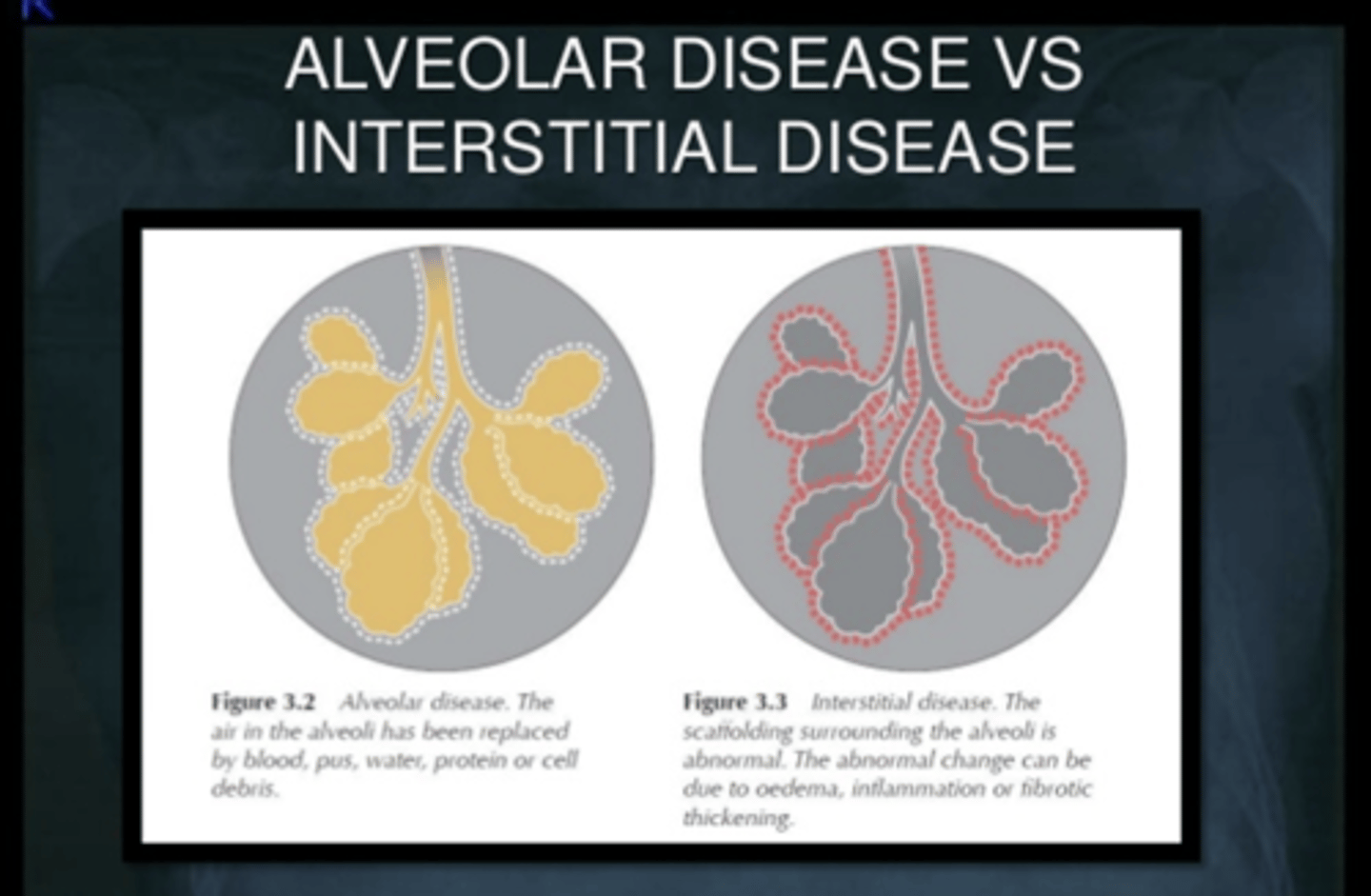
Define alveolar
o alveolar spaces are filled with some material such as blood, pus, fluid or cells (tends to be localized)
In a normal lung, what will bronchogram show?
Both the bronchi and the surrounding alveoli are filled with air, making the bronchi invisible on an X-ray.
What pathological processes can cause infiltrates?
- non specific....but CHF, pulmonary fibrosis, collagen vascular diseases, etc.
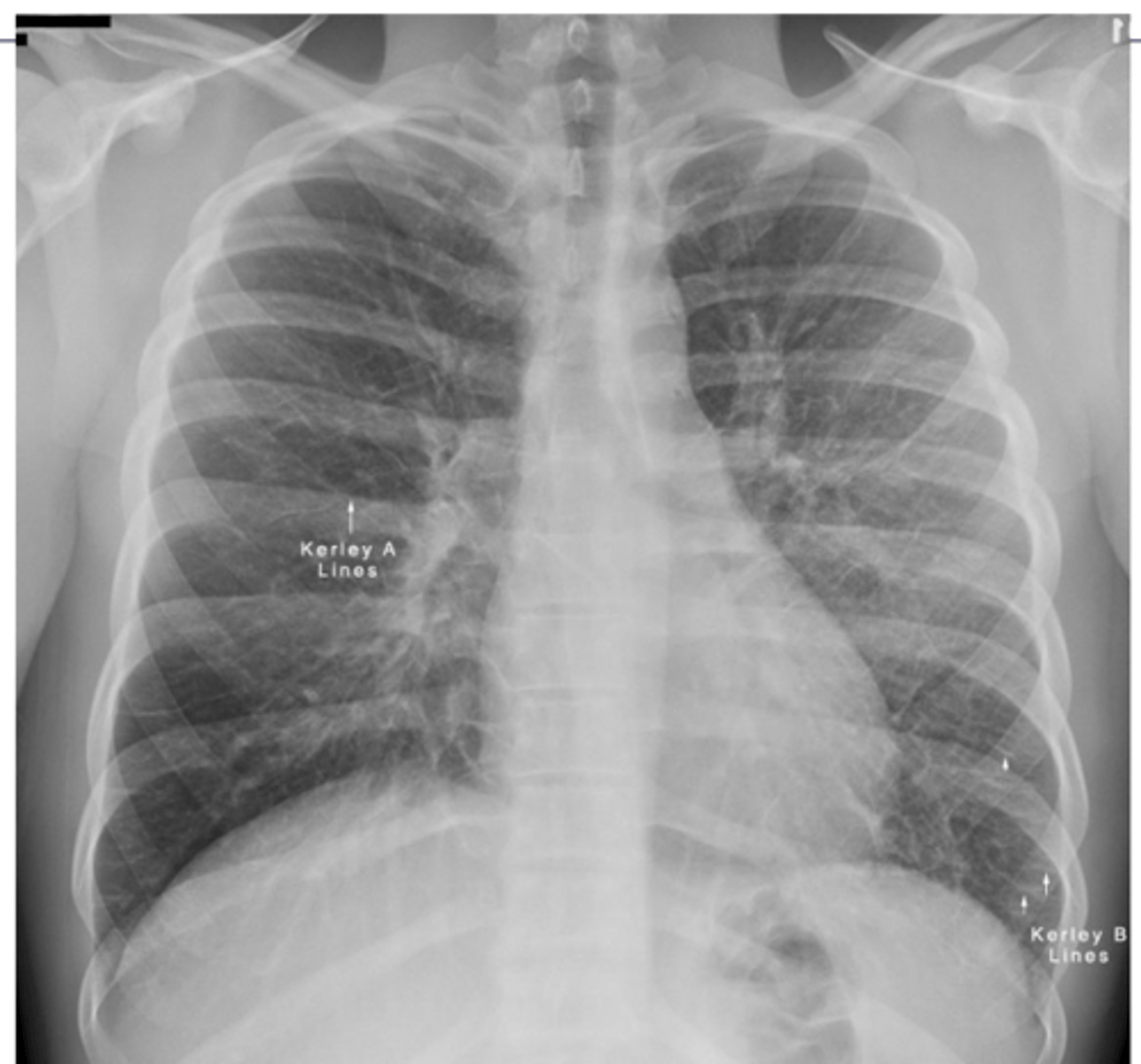
What are kerley A and B lines?
•Kerley A lines are linear opacities extending from the periphery to the hila caused by distention between peripheral and central lymphatics
•Kerley B lines are small, horizontal, peripheral straight lines demonstrated at the lung bases that represent thickened interlobular septa on CXR.
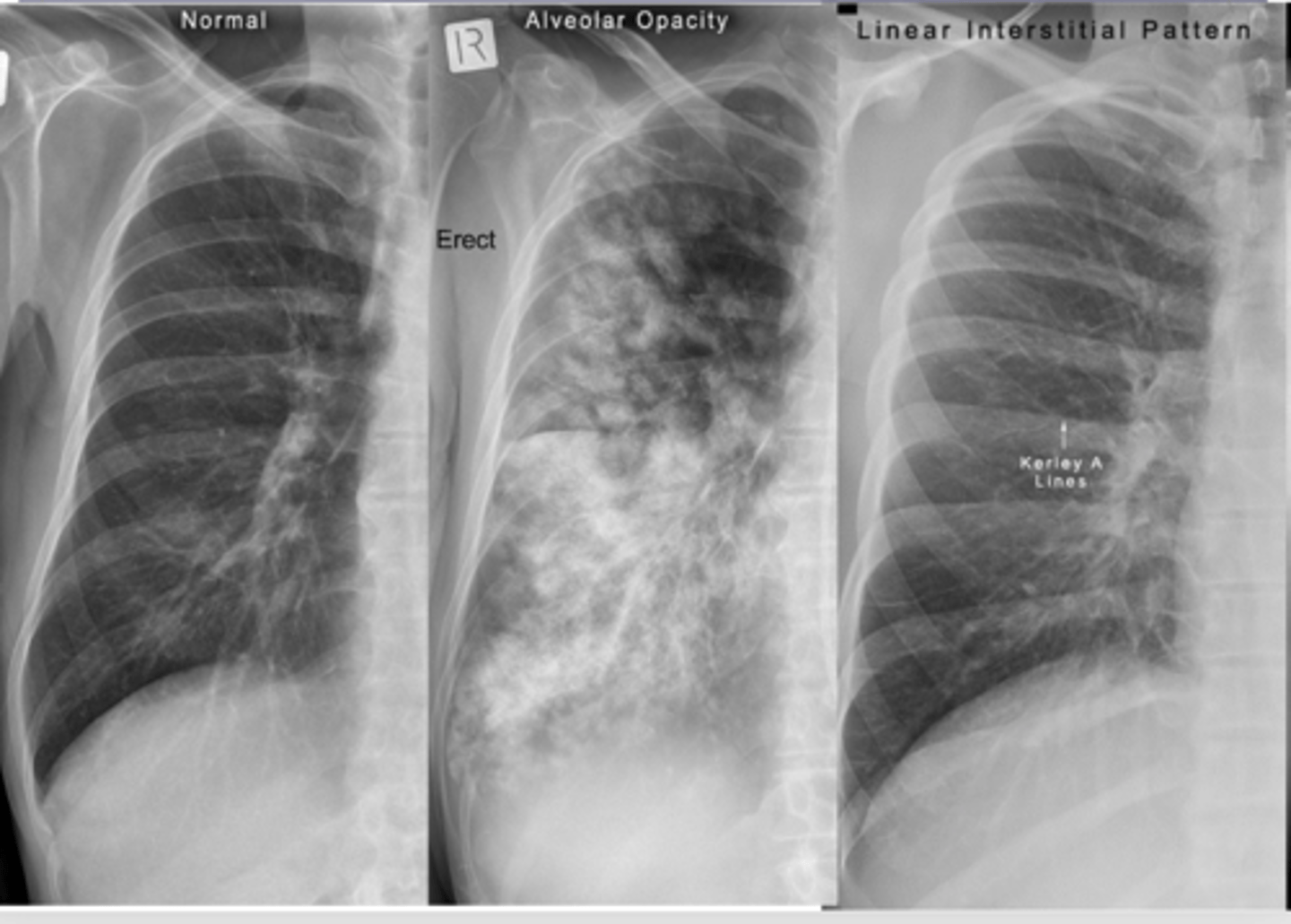
What does alveolar infiltrate look like?
alveolar infiltrate - looks "fluffy
Dx middle
lung fibrosis
What does an air bronchogram sign look like? What causes the abnormal appearance?
Alveoli are white but bronchi remain dark creating a visible pattern
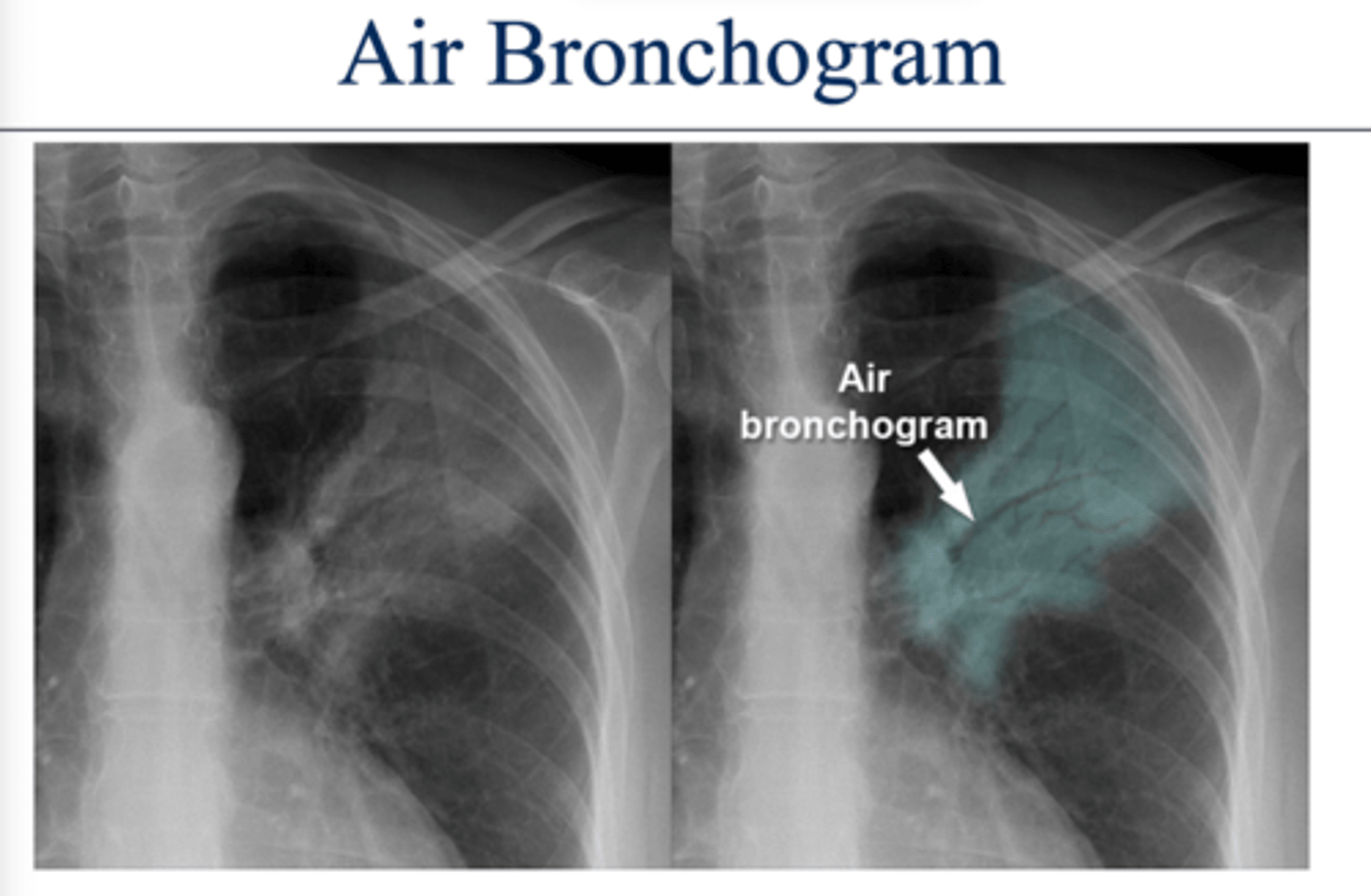
What dz would have an air bronchogram sign?
Pneumonia.
The infection causes the alveoli to fill with fluid.
What do interstitial infiltrates look like and what are some causes? IS this sign specific or non specific?
caused by acute and chronic disease processes that affect the tissue outside of the alveoli.
Interstitial processes are usually diffuse & are seen as thin white lines. May appear honeycombed (reticular)
Interstitial infiltrates are nonspecific as they can be caused by many processes such as CHF, pulmonary fibrosis, collagen vascular diseases, etc.
What are linear interstitial infiltrates also called? What is this sign commonly associated with?
Kerley lines --> interstitial pulm edema
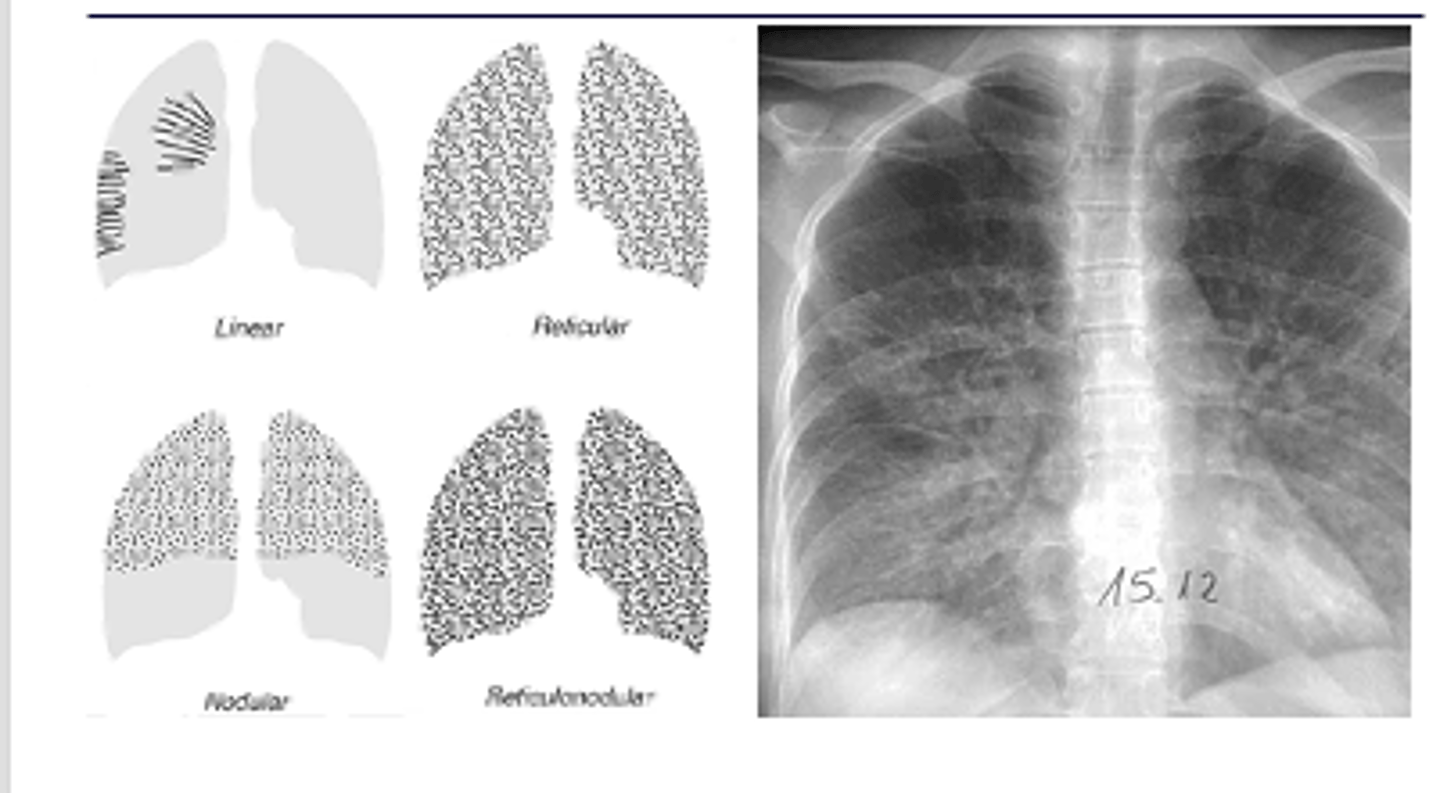
What is reticular opacity? What is this difference between fine and coarse?
Coarse - greatest width of opacity (fine on L and coarse on R)
Describe nodular pattern interstitial infiltrate
Nodular
A nodular pattern consists of multiple round opacities, generally ranging in diameter from 1 mm to 1 cm
What 2 patterns can community acquired pneumonia appear as? Typical patterns of bacterial, viral, mycoplasma and conolidation
Alveolar or interstitial
oBacterial – usually alveolar and focal
oViral and mycoplasma– usually interstitial and diffuse
oA consolidation = severe alveolar infiltrate
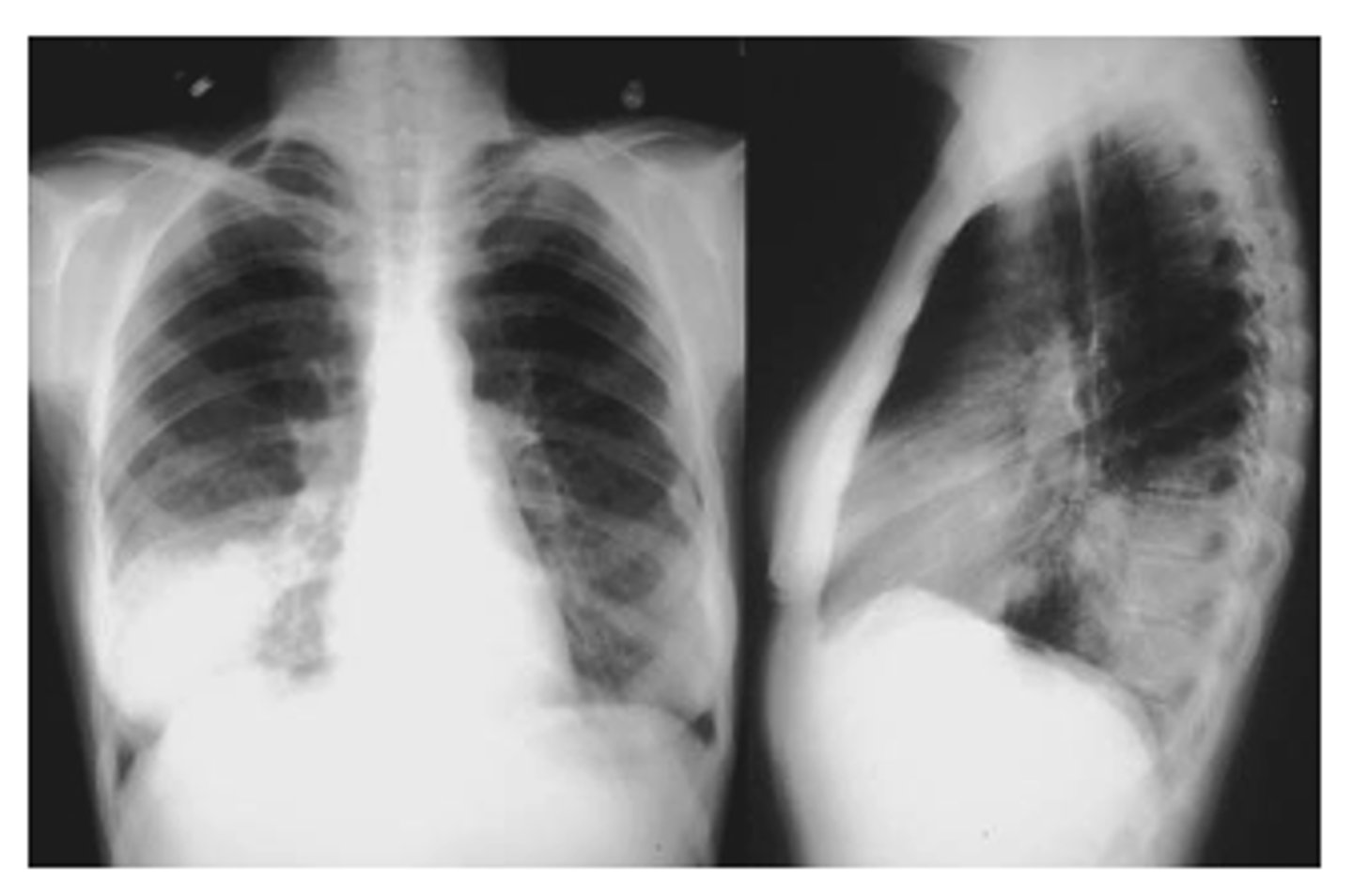
ID picture on back
LLL pneumonia
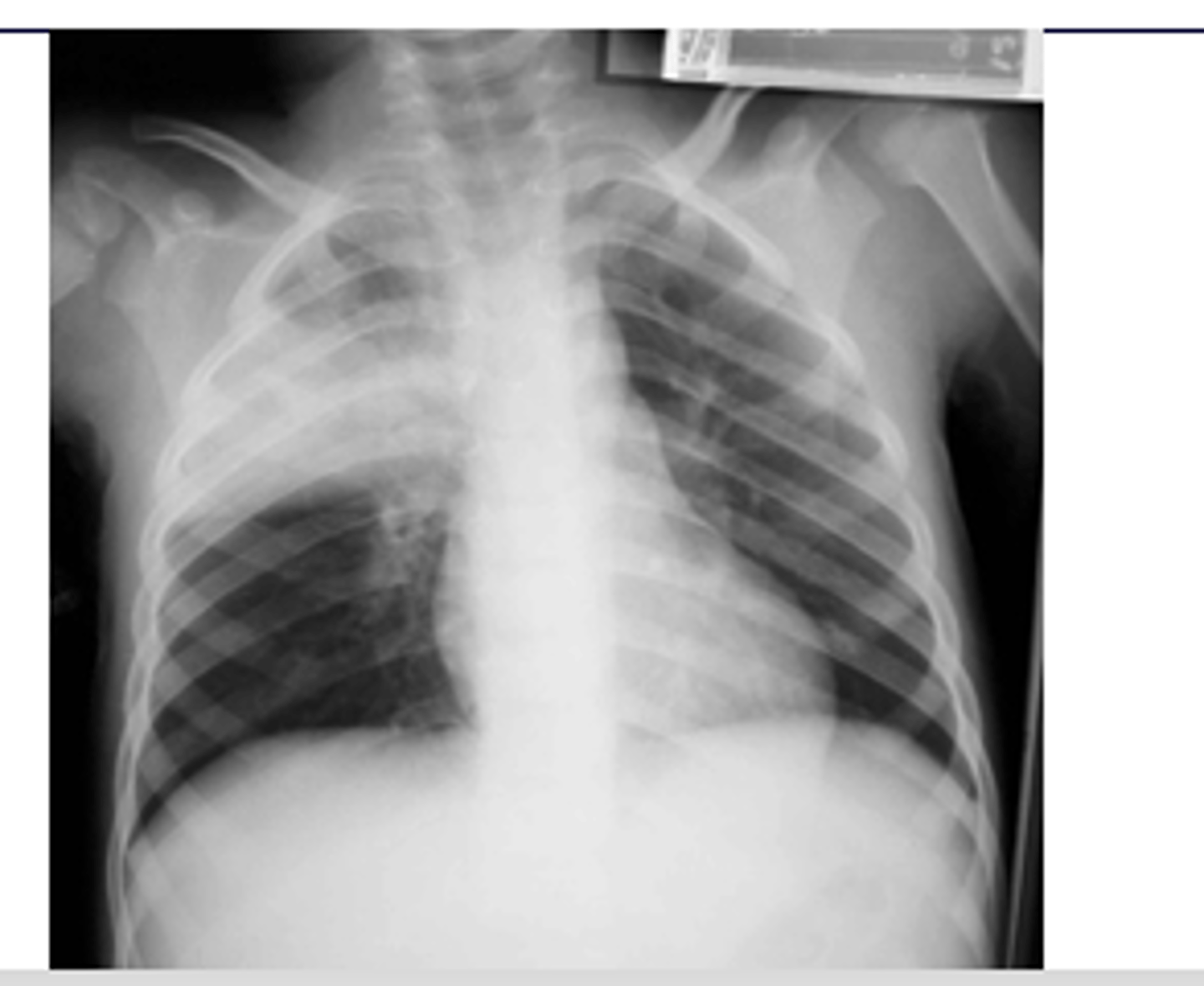
ID picture on back
RUL pneumonia with air bronchogram sign
What is the silhouette sign? What does it help determine?
oHelps determine the location of an abnormality in comparison to normal anatomy.
oLoss of a normal border and contour occurs if there is an abnormality contiguous with that structure (next to)
EX: if the R cardiac border is obscured, then the infiltrate must be in the medial segment of the R middle lobe.
(pic also has spine sign)
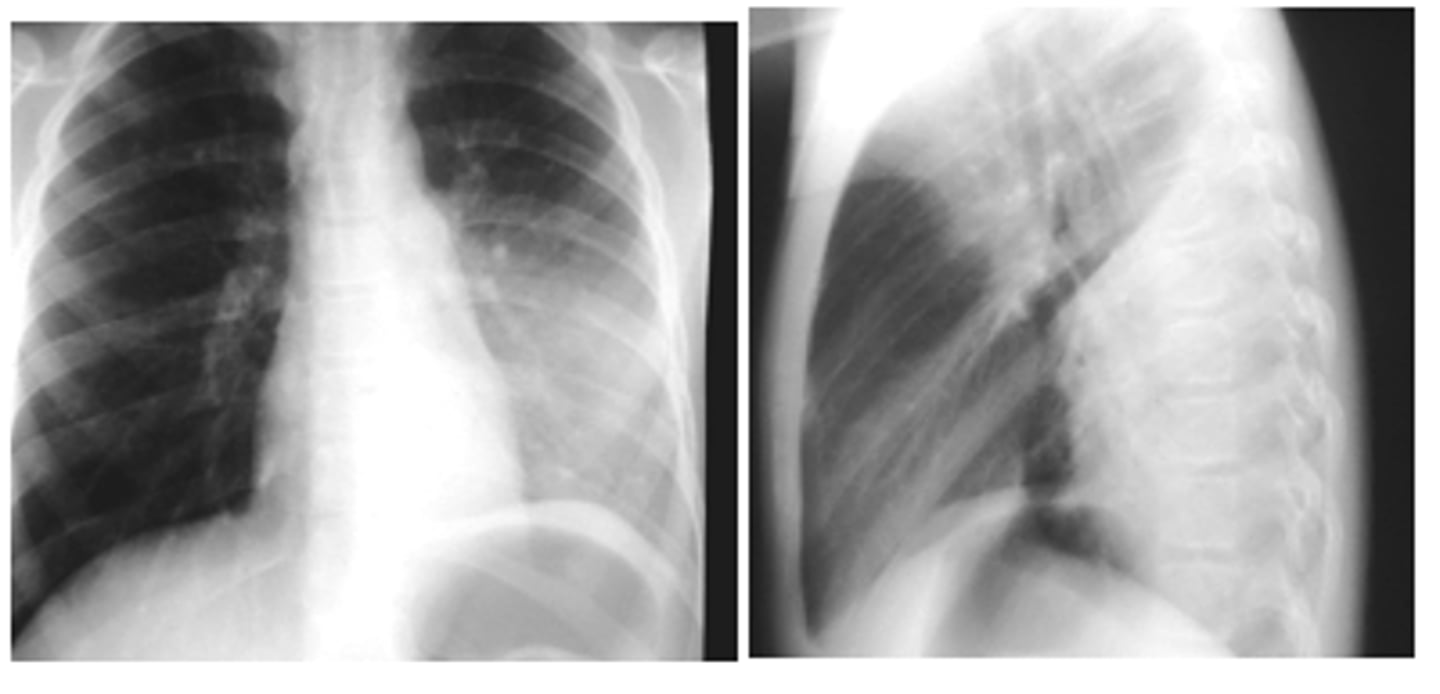
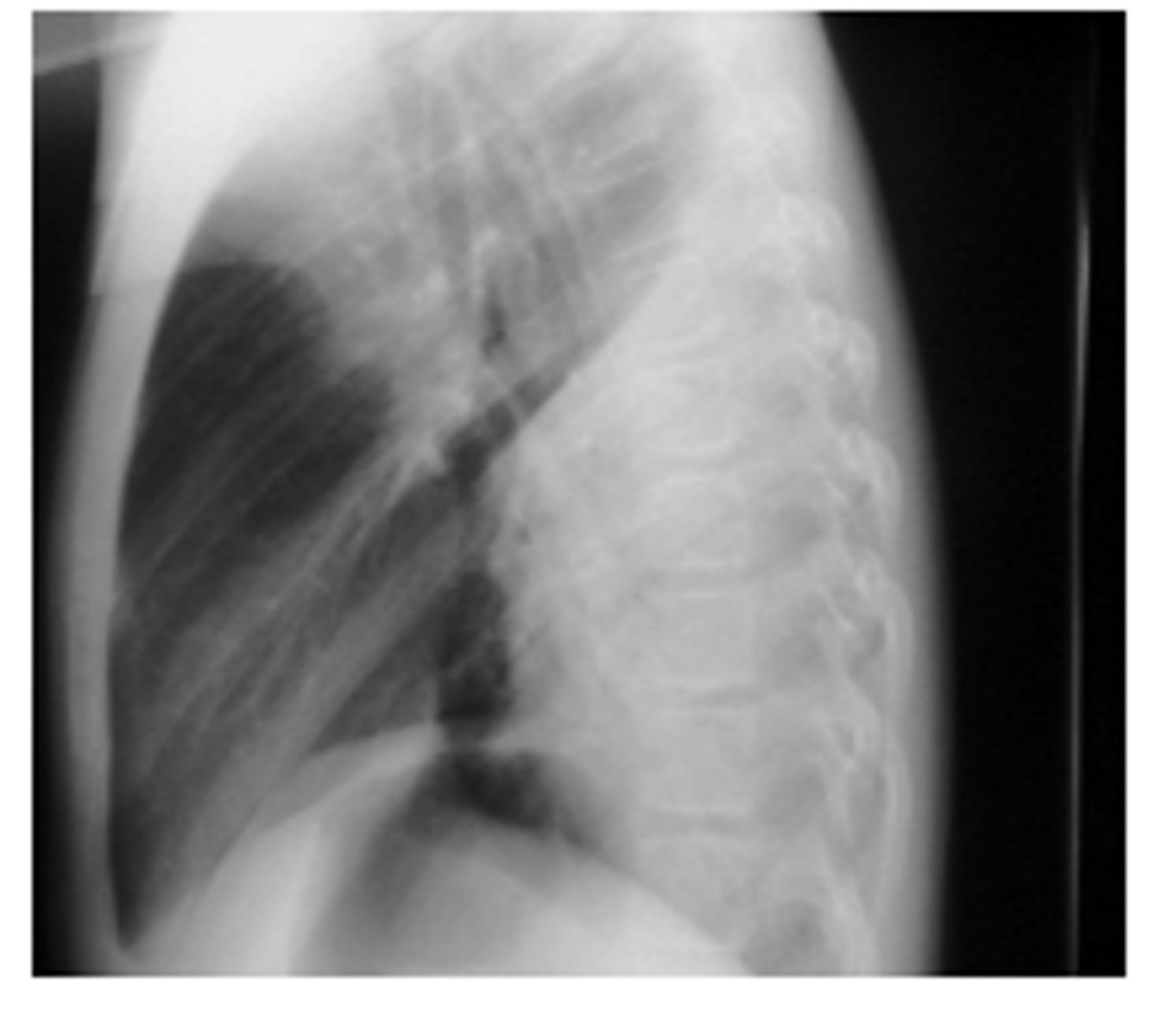
ID sign on back and finding
RML pneumonia obscuring the cardiac border but not the R hemidiaphragm. Note the triangular density on the lateral view.
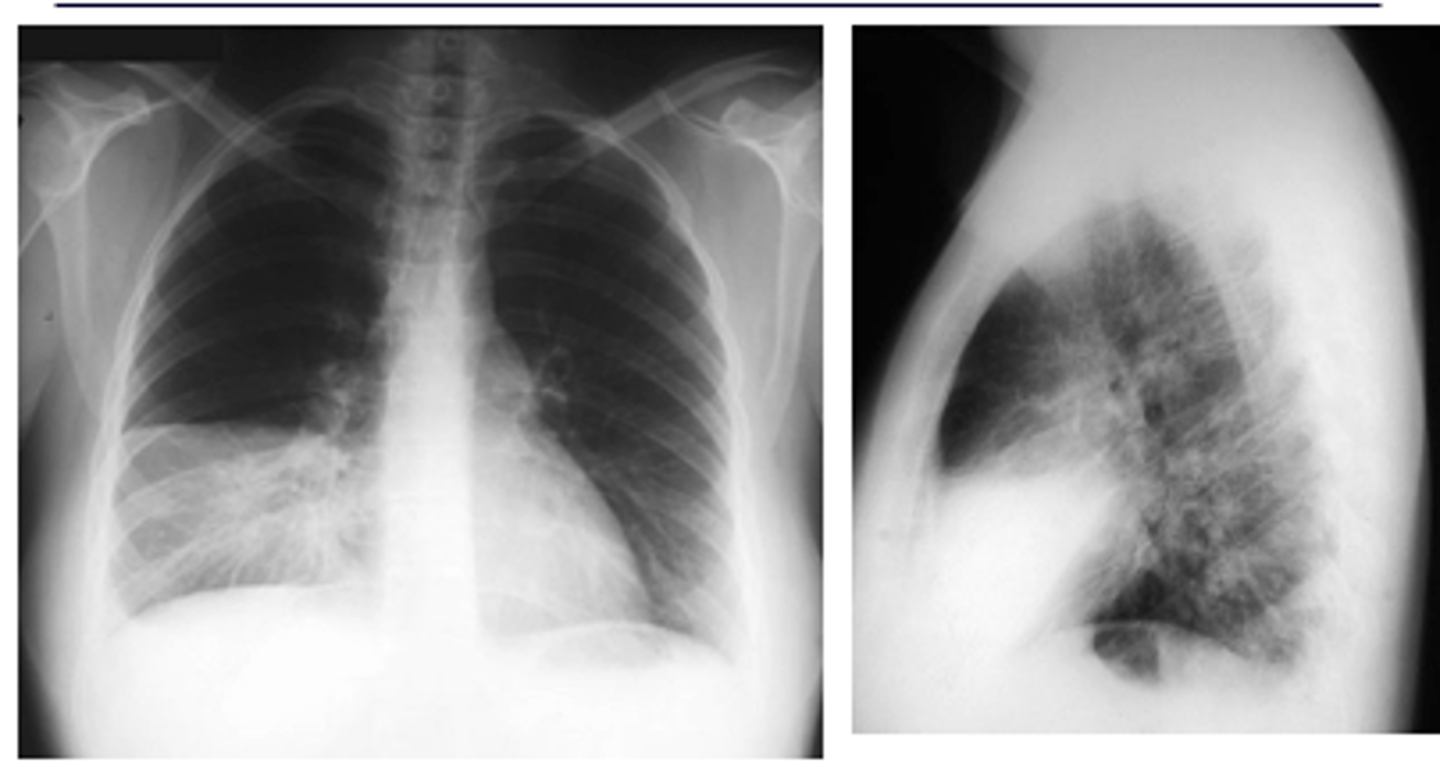
What is spine sign?
oSpine sign = vertebral bodies are lighter (white) than normal
What x-ray findings indicate atypical pneumonias caused by mycoplasma, viruses or pneumocystis? Most common pathogen
Pneumonias that are interstitial and symmetrically diffuse in both lungs
Path: mycoplasma
What x-ray finding is indicative of CAP and is more common in children than adults? What can this be mistaken for?
Round pattern
oCan simulate a mass lesion such as a neoplasm.

What type of pneumonia is commonly find in immunocompromised pts? How will the x-ray pattern evolve with dz progression?
oPneumocystis jiroveci pneumonia (PJP) evolves from a normal CXR to an interstitial pattern (diffuse) to an alveolar pattern (localized).
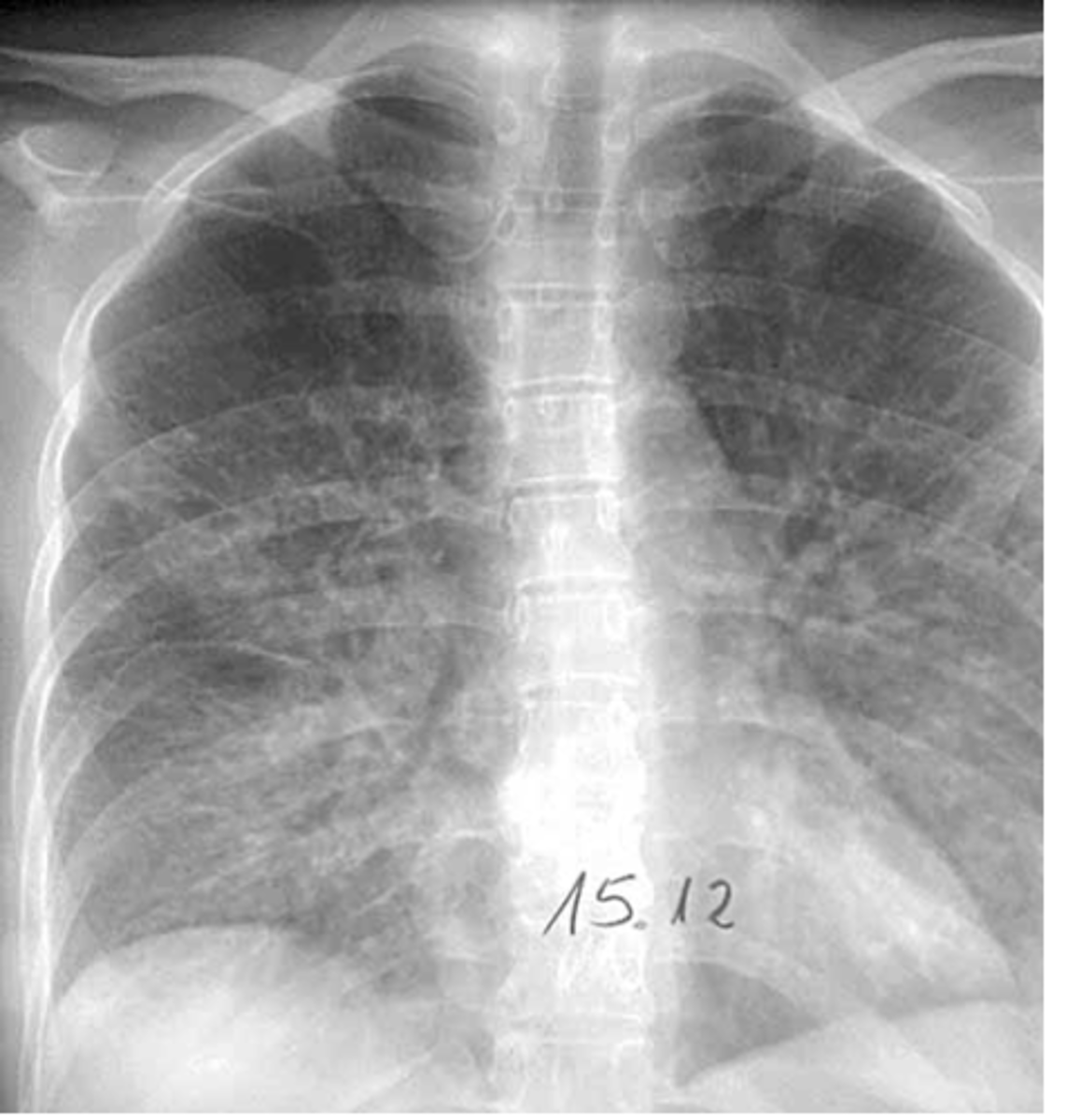
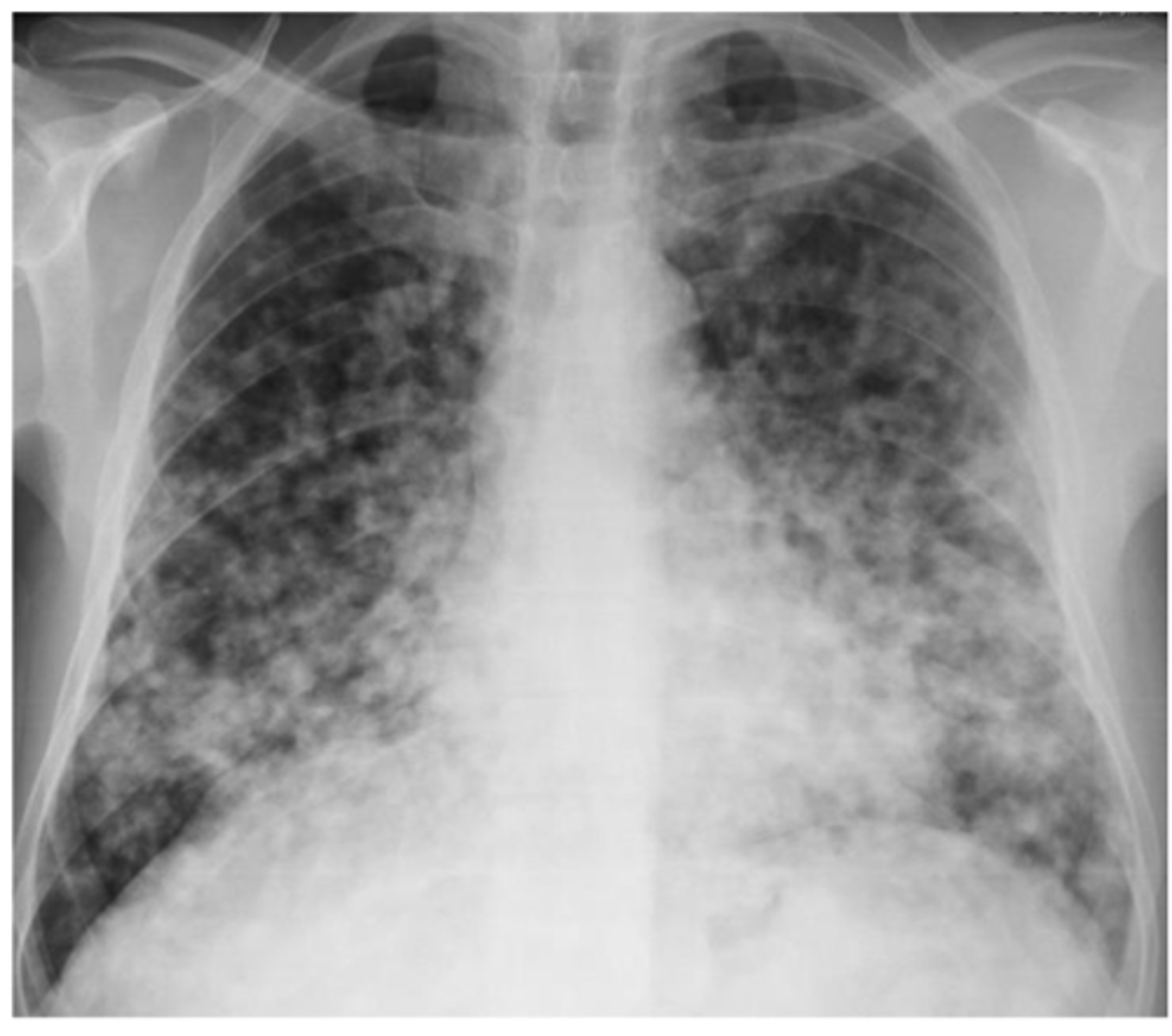
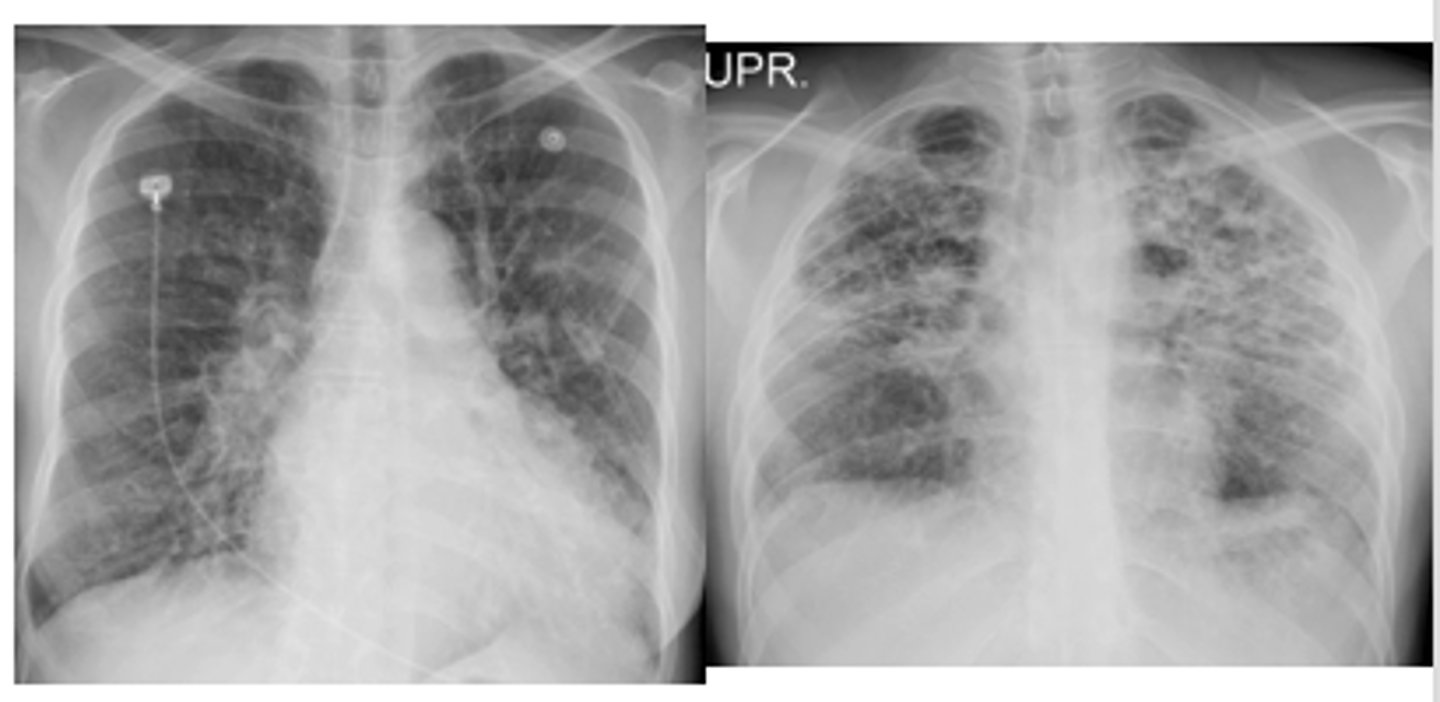
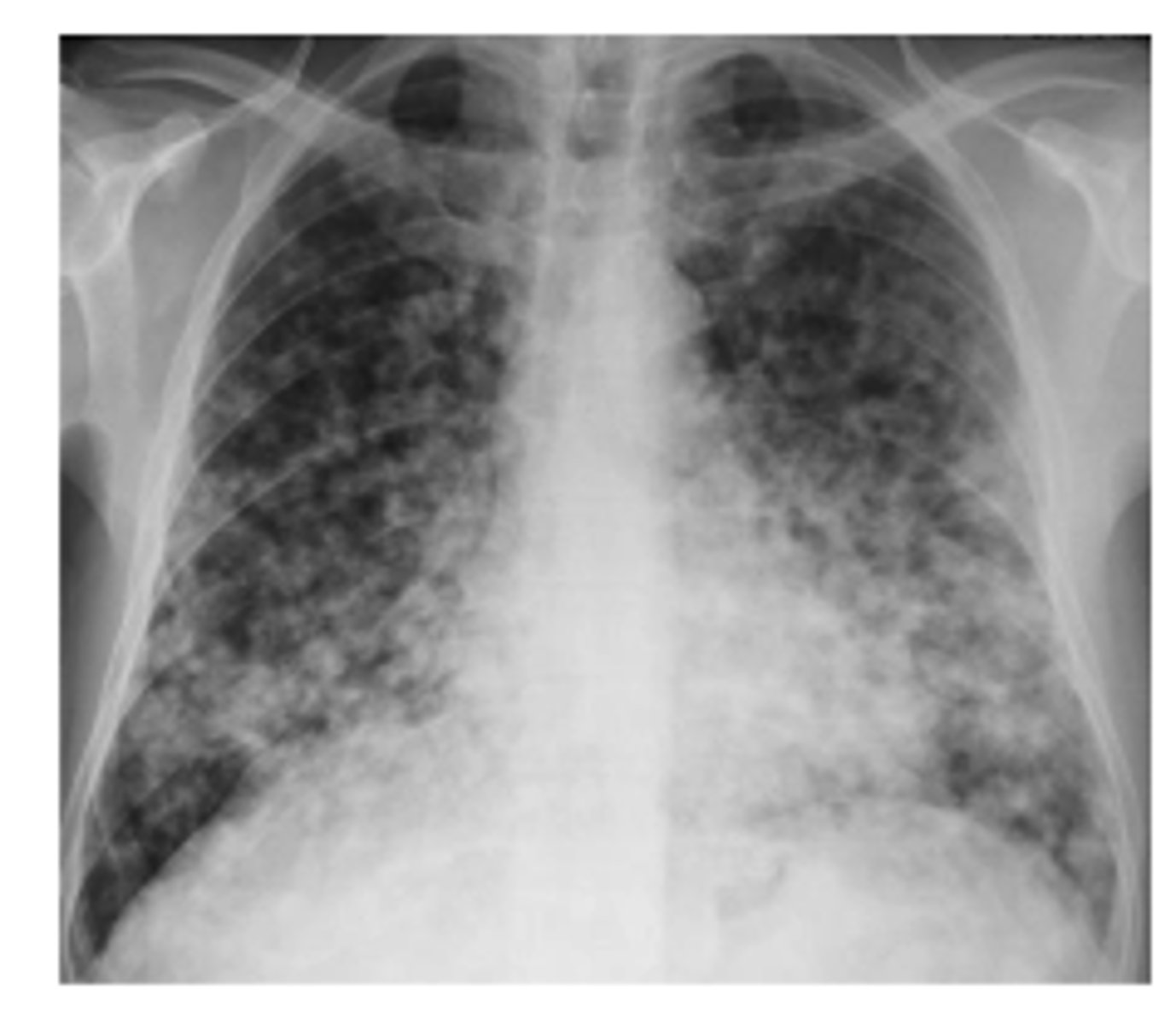
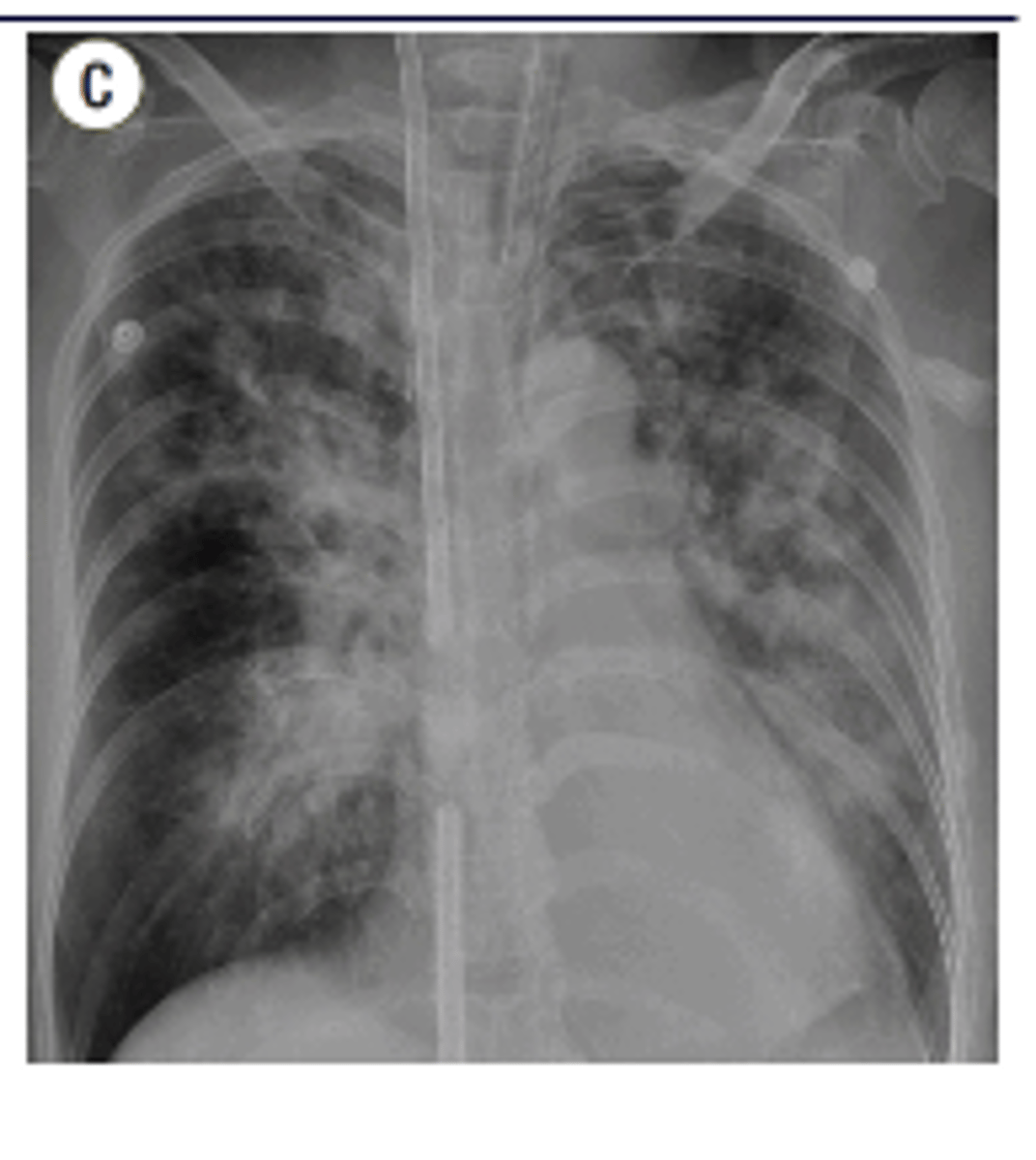
What is the pattern on the image of the back of the card?
Cystic PJP - PA chest radiograph shows diffuse bilateral reticulonodular interstitial infiltrates

What is aspiration pneumonia? What x-ray finding will be seen?
Gastric contents or other bodily fluids can be aspirated into the lungs
patchy, alveolar infiltrate
Common x-ray finding of primary active TB
oEnlargement of hilar or mediastinal lymph nodes is present about 95% of the time in primary active TB.
oCalcification usually occurs at the site of infection or in the node or both.

Common x-ray finding of military TB. What makes military TB particularly deadly?
diffuse bilateral infiltrates with very small nodules
-late phase of TB: potentially fatal form of the disseminated disease due to the hematogenous spread of tubercle bacilli to the lungs, and other organs.

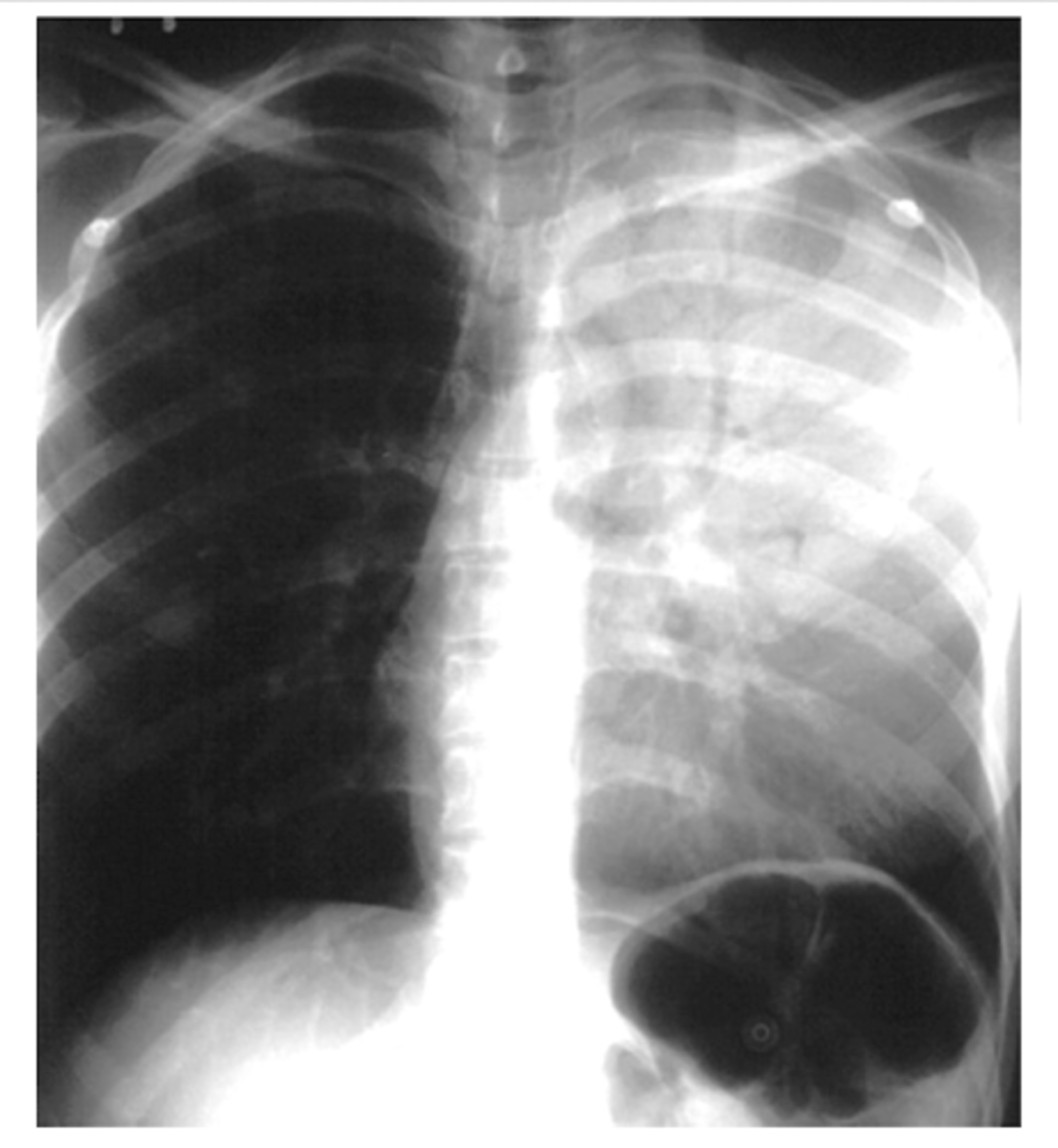
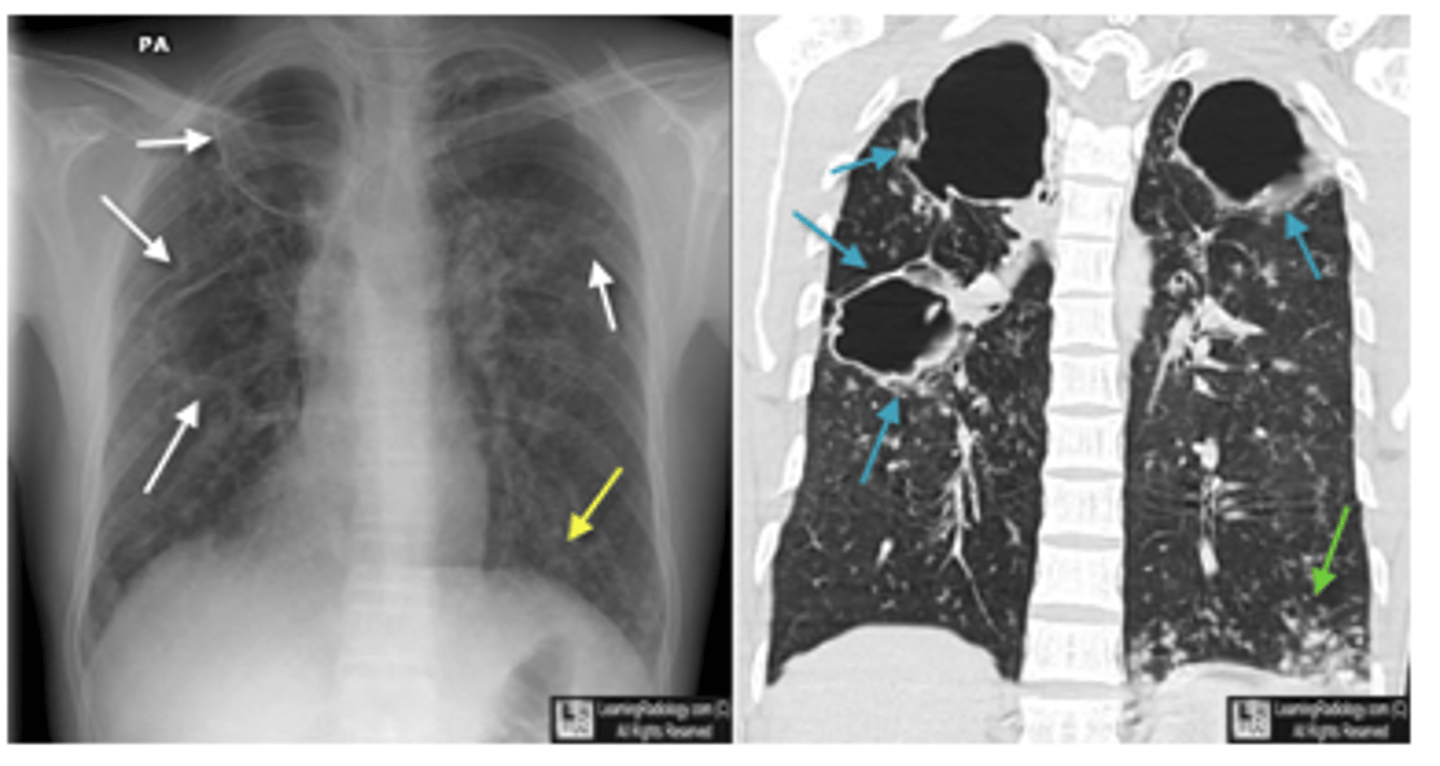
What is cavitary TB? What will X-ray look like?
oCavitary TB is also a late phase of TB.
oHealing leads to fibrososis and calcifications which may pull the hilum up on the affected side.
X-ray will have dark spots indicating holes/cavities
What are the key differences between ghon and ranke complexes?
Key Differences:
Stage of Disease:
1. Ghon complex: Represents the active or primary stage of TB infection.
2. Ranke complex: Indicates a healed or inactive stage of TB.
Calcification:
1. Ghon complex: May or may not be calcified.
2. Ranke complex: Is fully calcified.
Clinical Significance:
1. Ghon complex: Shows an active or recently acquired TB infection.
2. Ranke complex: Suggests the patient has had TB in the past, and the infection has resolved.
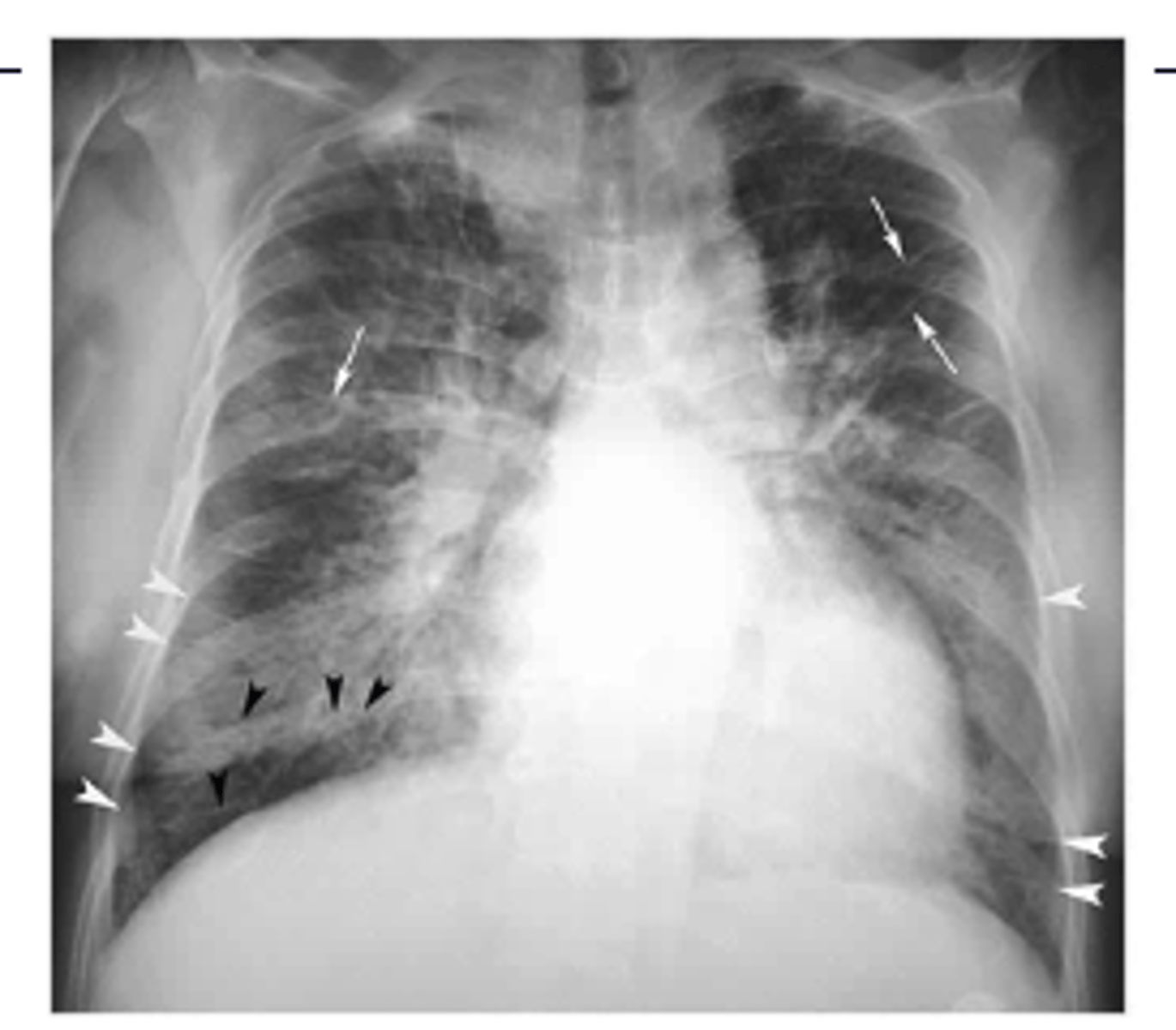
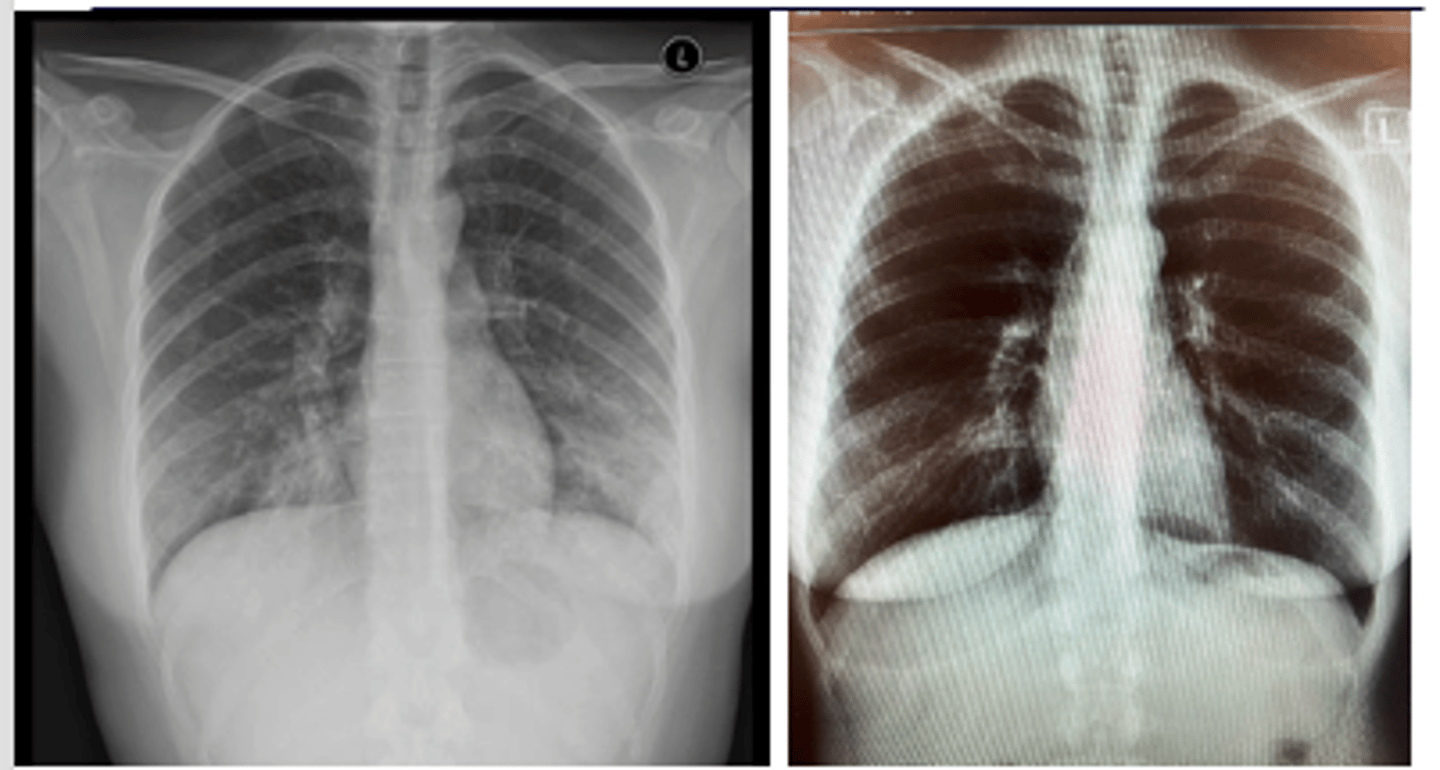
ID Ghon and Ranke complexes on xray
There is a combination of a calcified peripheral granuloma (black arrow) and a calcified hilar lymph node (white arrow) on the same side. Several other, small calcified granulomas are seen in the right mid-lung field - ranke complex
ranke typically more dense

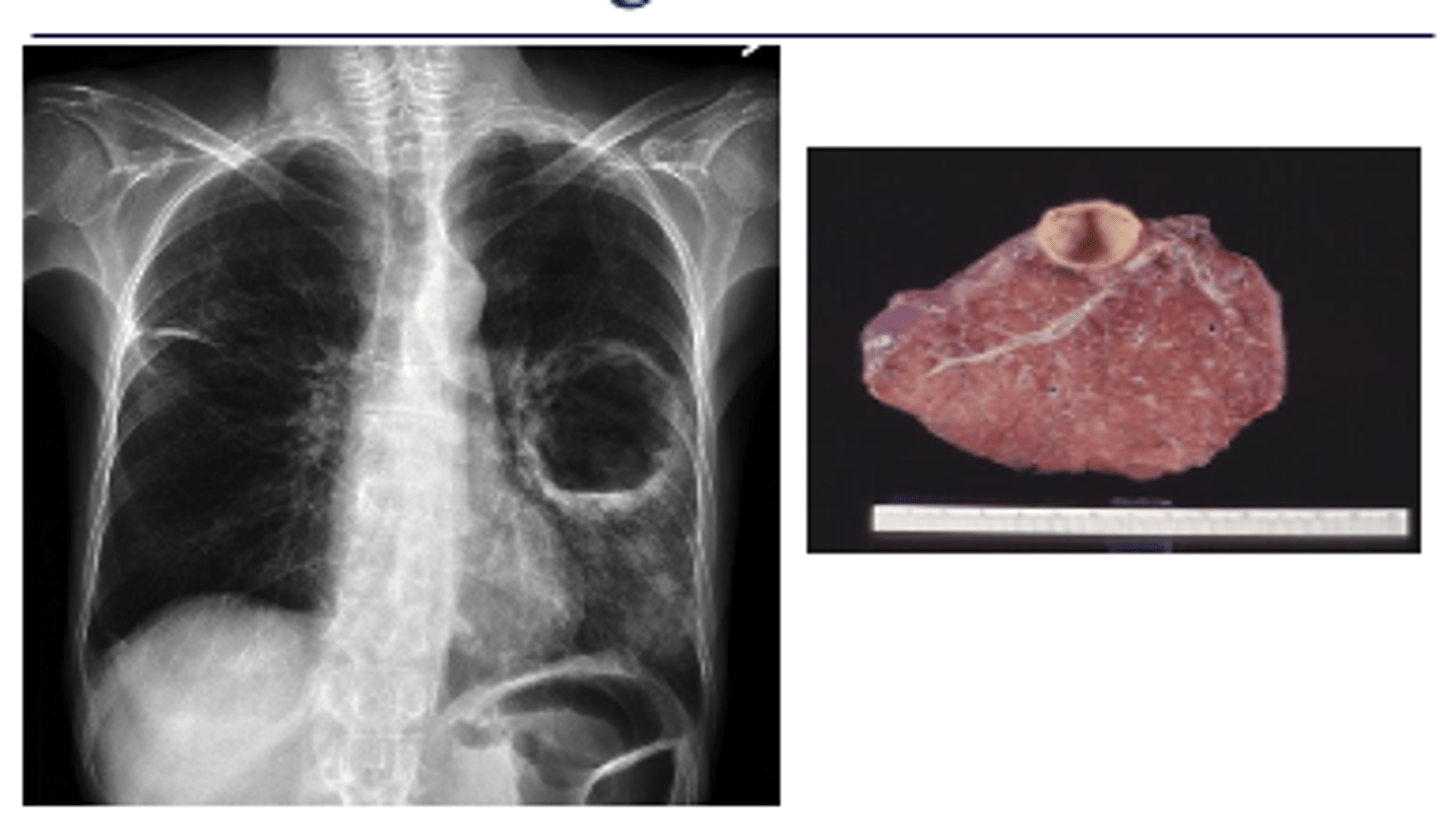
What would a lung abscess look like on x-ray?
oMay appear solid or cavitary with an air fluid level and a thick wall.
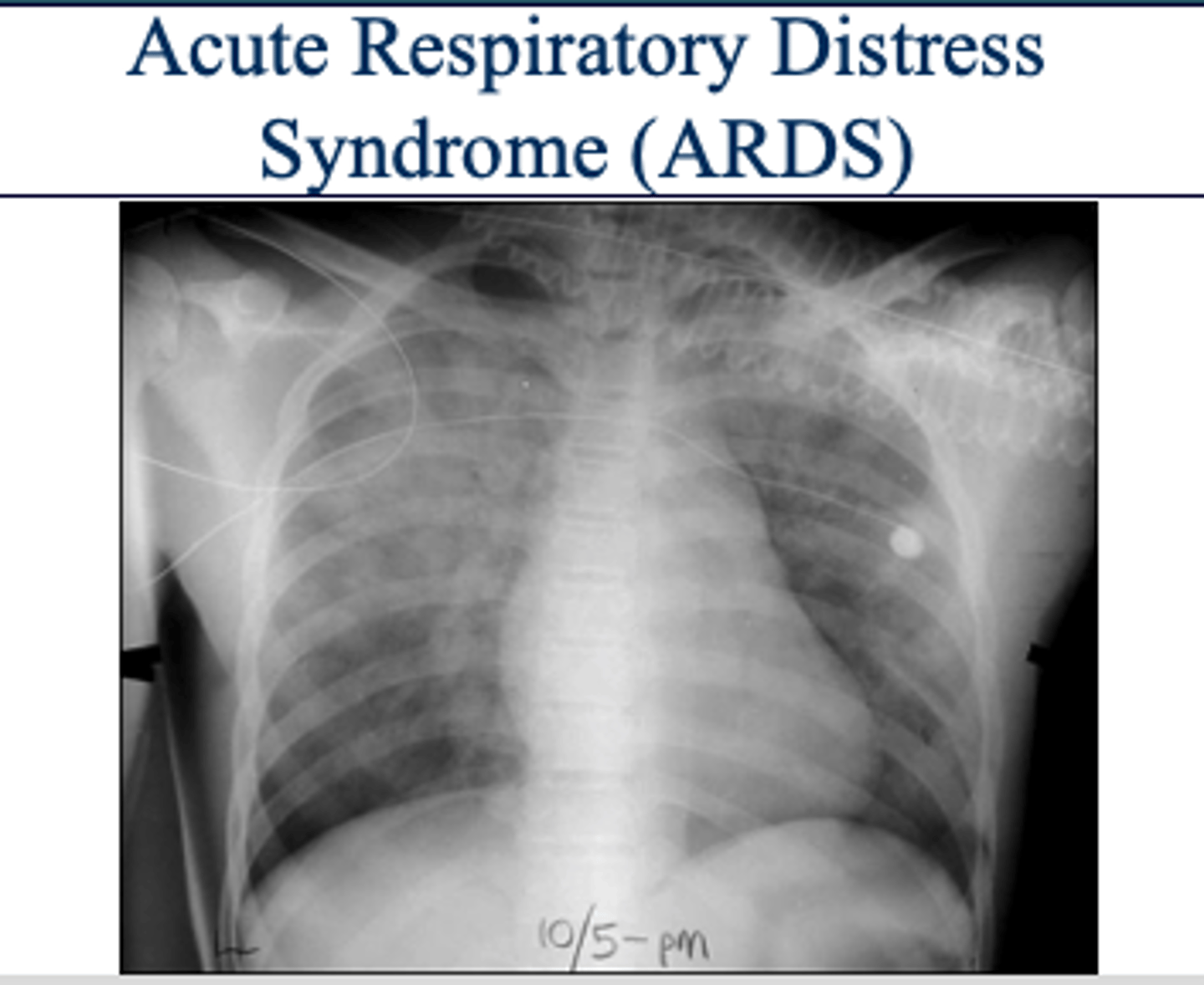
What is ARDS and what is the etiology?
oCapillaries are "leaky" and fluid shifts into the lungs from the blood supply through the capillaries - alveolar infiltrates.
oInitial insult to the alveoli usually caused by either alveolar or vascular damage.
oIncreases the permeability of the capillaries surrounding the alveoli and causes protein-rich fluid to fill the alveolar sacs.
ARDS x-ray appearance
"white out appearance" sometimes with sparing of costophrenic angles
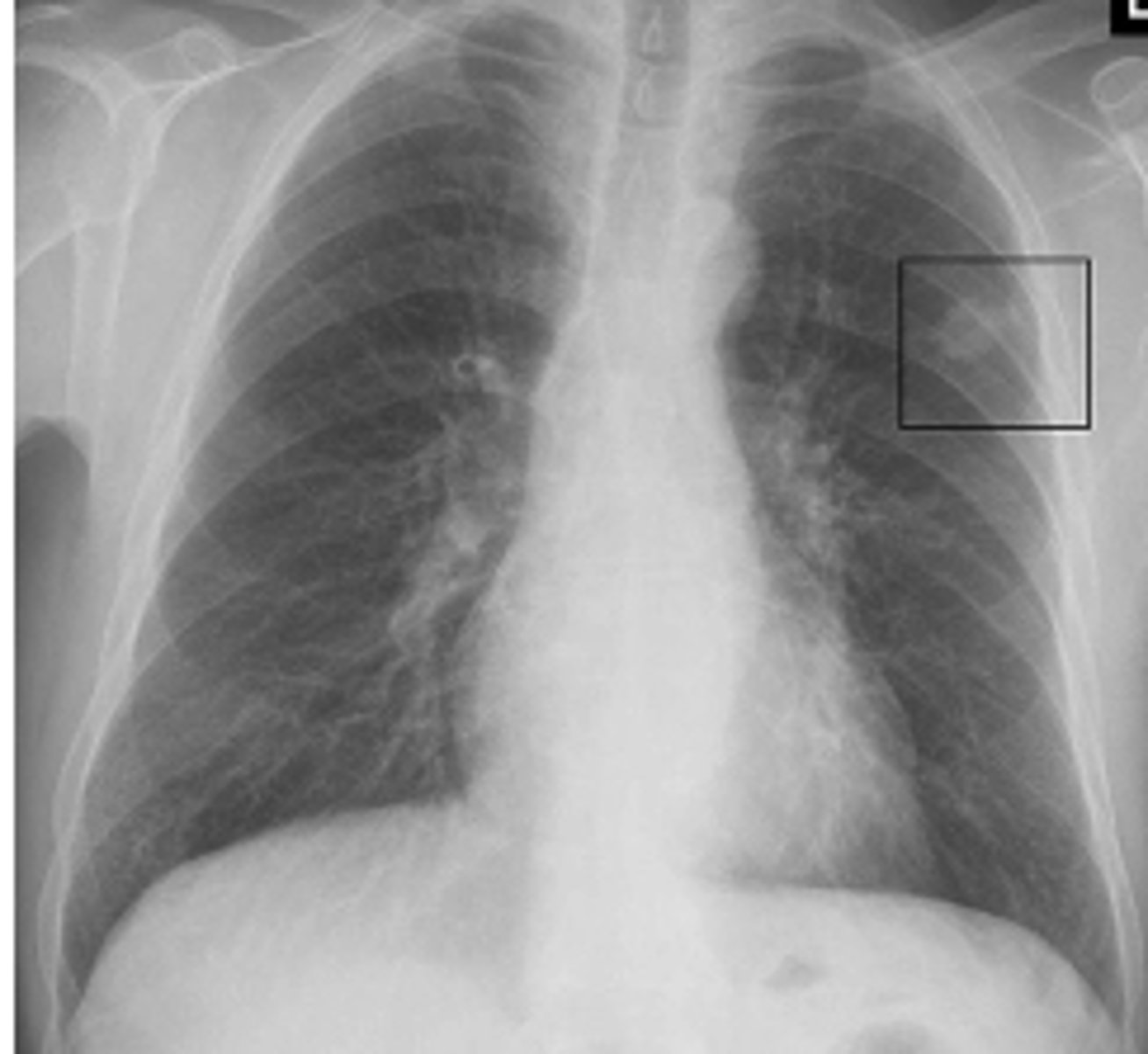
What are pulmonary nodules? How do they appear on x-ray?
Small, round opacities within the lung parenchyma.CXR Findings:Solitary or multiple nodules. Well-defined or irregular borders.
Benign vs malignant pulm nodules
oBenign Nodule
Less than 3 cm
Calcified
Round, well-defined borders
Solid - no cavity
oMalignant Nodule
Greater than 3 cm
Not calcified
Irregular shape, poorly defined borders, ground glass
Cavitated
Growth in past 2 yrs
CT scan indications for lung mass
-New or larger lesion when compared to previous films.
-size greater than 3 cm in patient less than 35 yrs old.
-Any size in patient greater than 35 yrs old.
-Hilar enlargement
Adenocarcinomas
are the most common type of lung CA and usually occur peripherally.

Squamous cell carcinomas
usually occur centrally and tend to cavitate.

Small cell carcinomas
often present as an indistinct hilar or mediastinal mass. (pic: R hilar and paratracheal region)
Non-small cell carcinomas
can occur peripherally or centrally and grow rapidly with early metastases - poor prognosis.

Pancoast tumor
-Arise in the superior sulcus of the lung as an apical soft tissue mass.
-Frequently invade the chest wall and the brachial plexus. Rib destruction common.
-Symptoms may include shoulder, arm and hand pain or weakness – T1 distribution most commonly.

What will metastatic dz look like on radiograph?
Nodular pattern resulting from multiple small metastases to the lung from a colonic adenocarcinoma
