1.2 Cognitive Behavioral Therapy - General Process
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
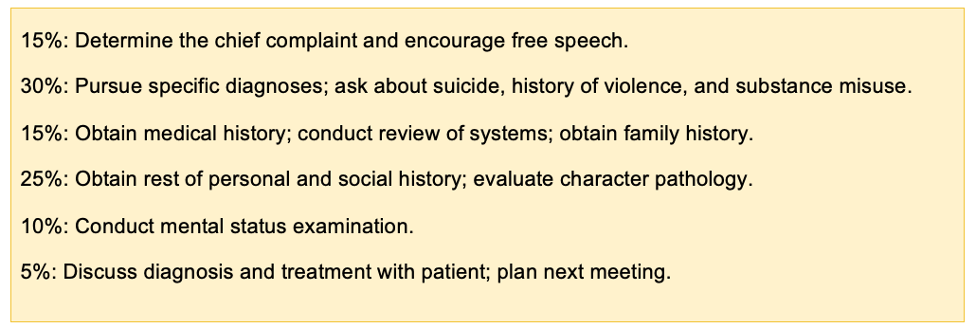
Which 6x parts are involved during an Intake Evaluation? Name them and add each the percentage of focus
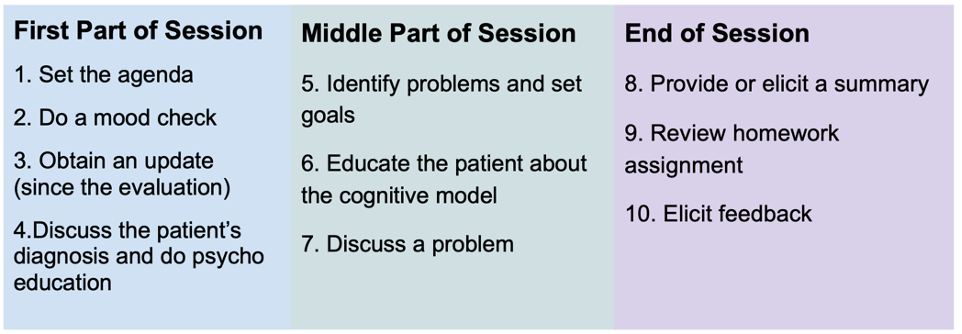
How should your First Therapy Session be structured regarding tasks and order in the …
- First Part of Session:
- Middle Part of Session:
- End Part of session:
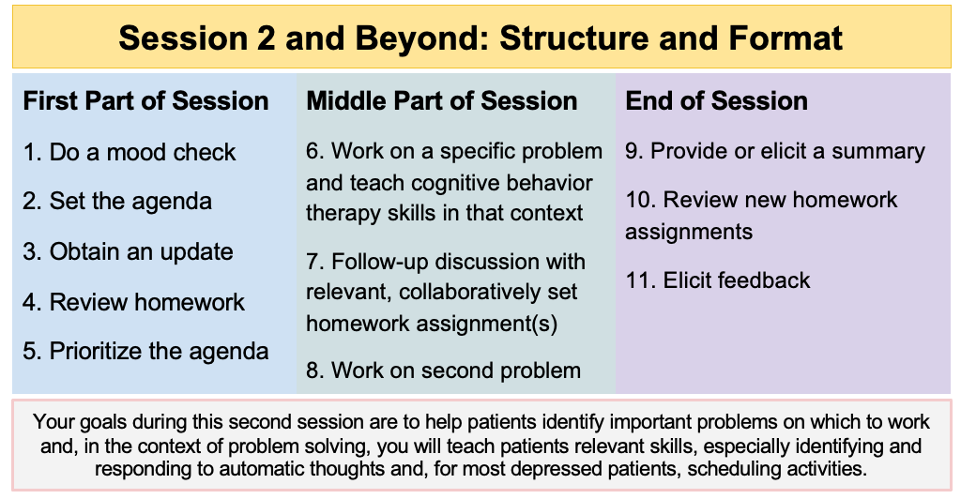
How should your second Therapy Session and beyond be structured regarding tasks and order in the …
- First Part of Session:
- Middle Part of Session:
- End Part of session:
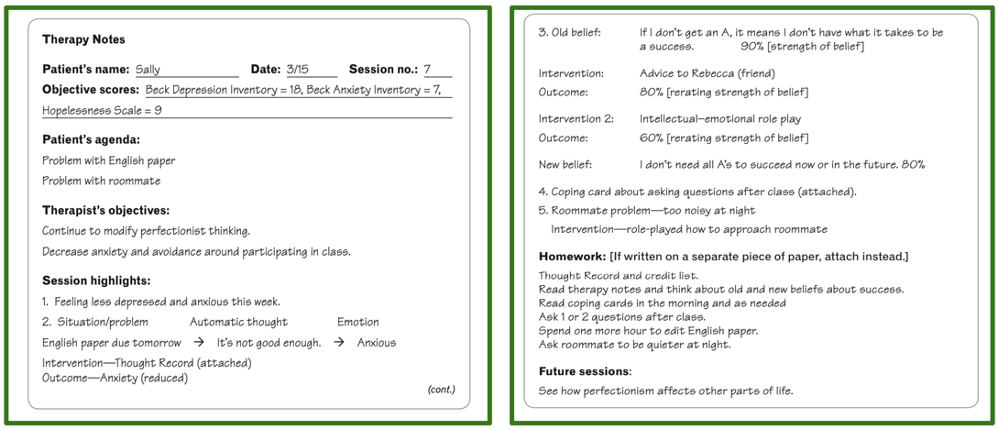
How could your Therapy Notes from Session 2 and beyond structured and look like?
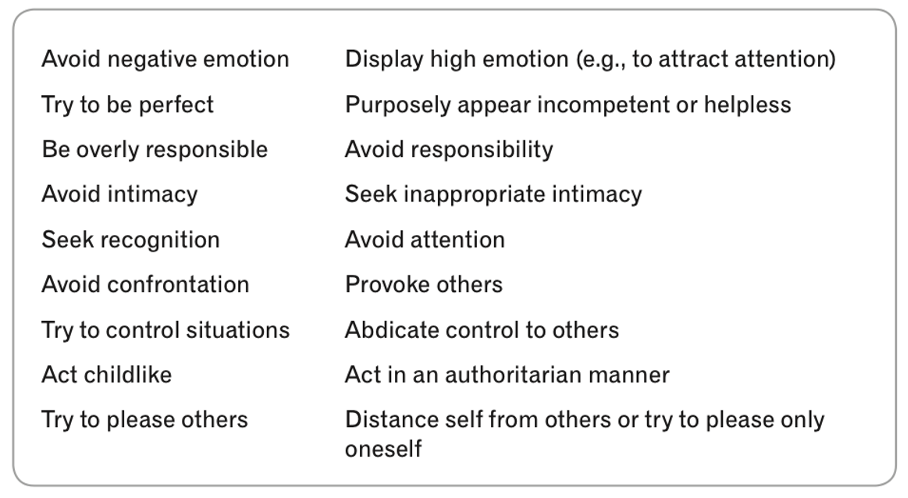
Name 9x typical coping strategies used by persons
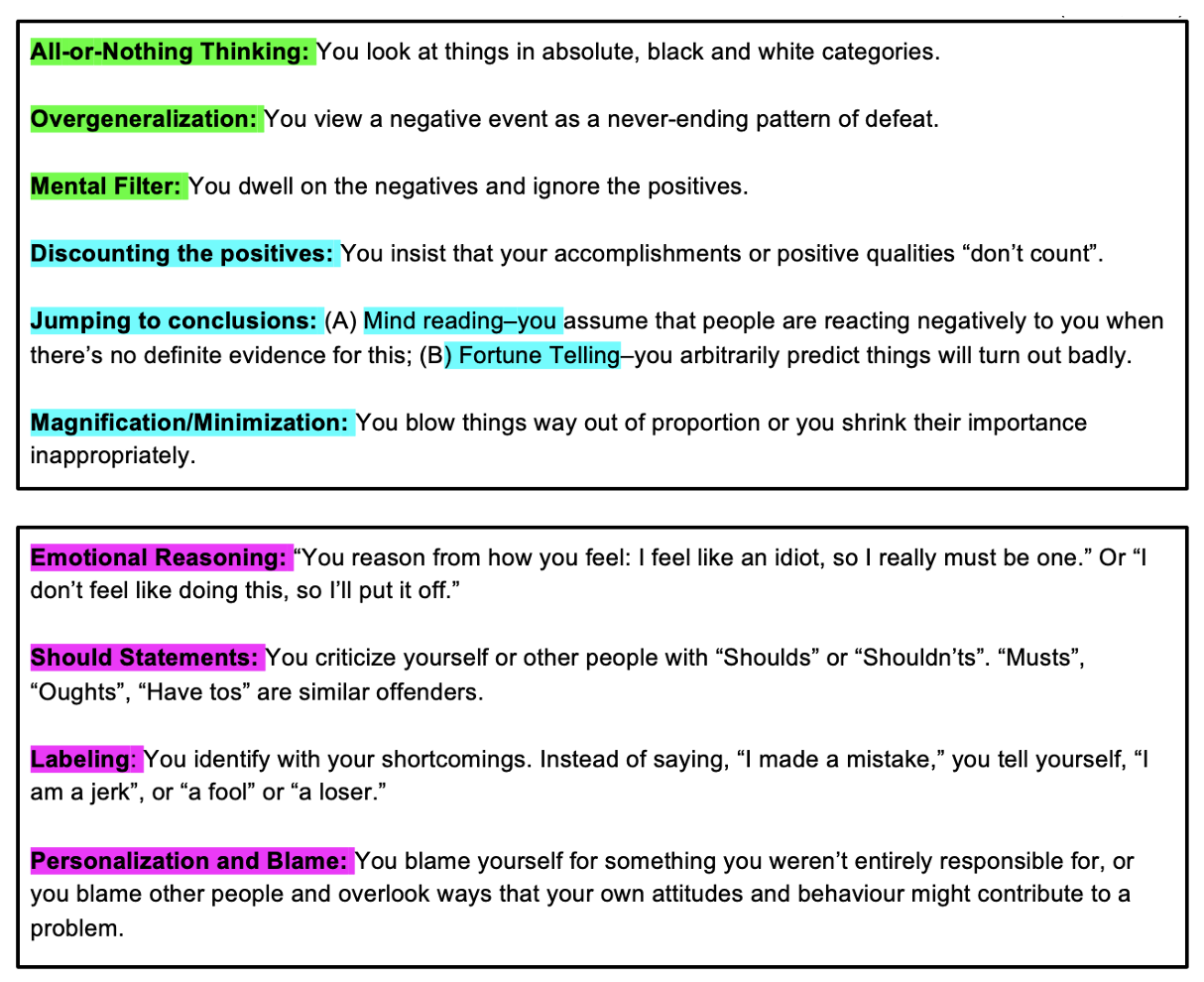
Explain what cognitive distortions are in general and name 10x common key distortions.
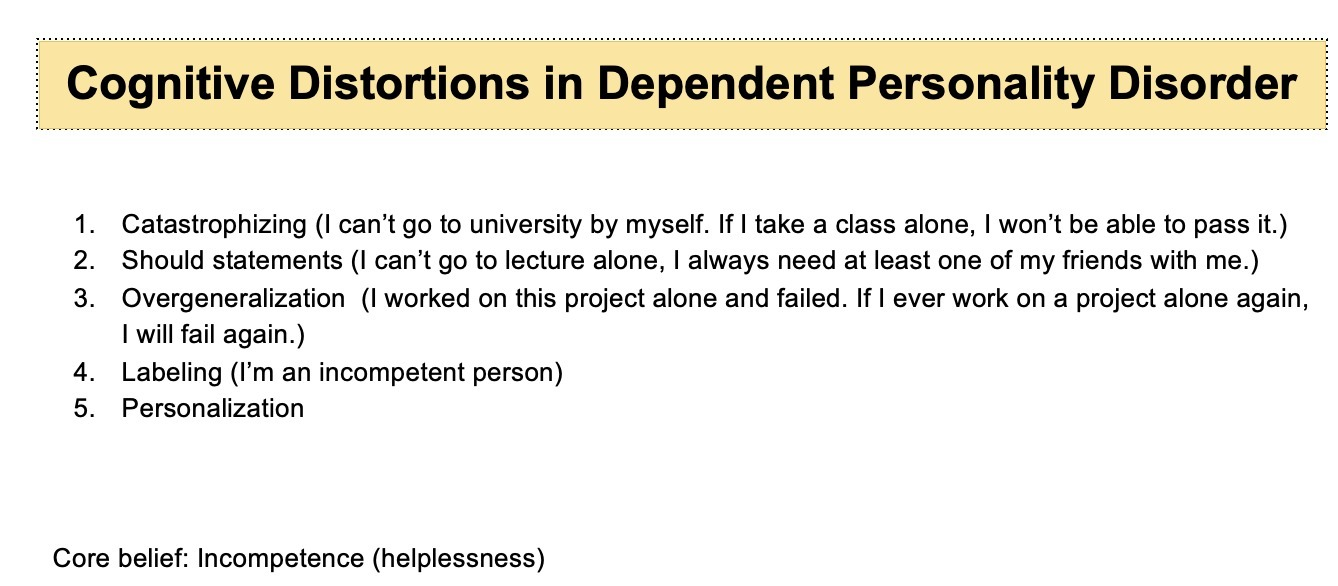
Which cognitive distortions can you expect in Dependent Personality Disorder?
Which cognitive distortions can you expect in Depression?
Negative Filtering: This involves selectively focusing on negative aspects of situations while ignoring or discounting any positive elements. It perpetuates feelings of hopelessness and worthlessness.
Overgeneralization: Similar to PTSD, individuals with depression tend to generalize negative experiences, believing that one negative event or aspect applies to all areas of their life. This can contribute to a pervasive sense of despair and helplessness.
All-or-Nothing Thinking (Black-and-White Thinking): Viewing situations in extremes, where everything is either perfect or a total failure, amplifies feelings of inadequacy and contributes to a distorted perception of reality.
Which cognitive distortions can you expect in OCD?
Catastrophizing: Individuals with OCD often catastrophize the potential consequences of not engaging in their compulsive behaviors. They may believe that something terrible will happen if they don't perform their rituals, leading to heightened anxiety and reinforcement of the compulsive cycle.
Thought-Action Fusion: This distortion involves believing that having a thought about a negative event is morally equivalent to actually carrying out that event. Individuals with OCD may interpret intrusive thoughts as indicative of their true desires or as omens of impending harm, leading to heightened distress and an increased urge to perform rituals to neutralize the thoughts.
Perfectionism: OCD is often associated with an extreme need for things to be "perfect" or "just right." This perfectionist thinking can lead to an excessive focus on details, repeated checking, and an inability to tolerate uncertainty, all of which contribute to the maintenance of OCD symptoms.
Which cognitive distortions can you expect in Social Anxiety?
Mind Reading: Individuals with social anxiety often believe they know what others are thinking about them, usually assuming negative judgments or criticisms. This distortion heightens self-consciousness and intensifies anxiety in social situations.
Fortune Telling: They frequently engage in predicting negative outcomes in social interactions, assuming that things will inevitably go wrong or that they will embarrass themselves. This anticipation of failure reinforces avoidance behaviors and perpetuates anxiety.
Magnification (Catastrophizing) and Minimization: Magnification involves blowing potential negative outcomes out of proportion, such as fearing that making a small mistake will lead to total humiliation. Minimization, on the other hand, involves downplaying positive aspects of social interactions or personal attributes, reinforcing feelings of inadequacy and low self-worth. Both distortions contribute to the maintenance of social anxiety symptoms.
Which cognitive distortions can you expect in Panic Disorder?
Catastrophizing: Individuals with panic disorder tend to catastrophize physical sensations, interpreting them as signs of imminent danger or medical emergencies. This cognitive distortion amplifies the intensity of panic attacks and perpetuates the fear of future attacks.
Selective Abstraction: They may selectively focus on bodily sensations associated with panic attacks, while ignoring contextual information or evidence that contradicts their catastrophic interpretations. This selective attention reinforces the perception of threat and maintains panic symptoms.
Jumping to Conclusions: Individuals with panic disorder often jump to conclusions about the meaning of their physical sensations, assuming they are indicative of a catastrophic outcome (e.g., heart attack, loss of control). This cognitive distortion fuels anxiety and contributes to the cycle of panic attacks.
Which cognitive distortions can you expect in specific phobia like Agoraphobia?
Catastrophizing: Individuals with specific phobia or agoraphobia often catastrophize the feared situation or object, imagining the worst possible outcome if they were to encounter it. This distortion amplifies anxiety and avoidance behaviors, reinforcing the phobic response.
Overestimation of Threat: They tend to overestimate the likelihood and severity of harm associated with the feared stimulus. This cognitive distortion leads to heightened anxiety and avoidance behaviors, as individuals perceive the situation as more dangerous than it objectively is.
Safety Behaviors: Individuals with specific phobia or agoraphobia often engage in safety behaviors, such as carrying emergency medication or avoiding specific situations, to manage their anxiety. While these behaviors may provide temporary relief, they reinforce the belief that the feared stimulus is inherently dangerous and perpetuate avoidance patterns.
Which cognitive distortions can you expect in PTSD?
Catastrophizing: This distortion can exacerbate anxiety and fear, amplifying the perceived threat level of situations and memories.
Overgeneralization: Overgeneralizing can lead individuals to believe that the trauma will inevitably repeat itself in all situations, impairing their ability to feel safe and secure.
Emotional reasoning: When individuals believe that their emotions accurately reflect reality, it can perpetuate negative thoughts and feelings associated with the trauma, hindering recovery and coping mechanisms.
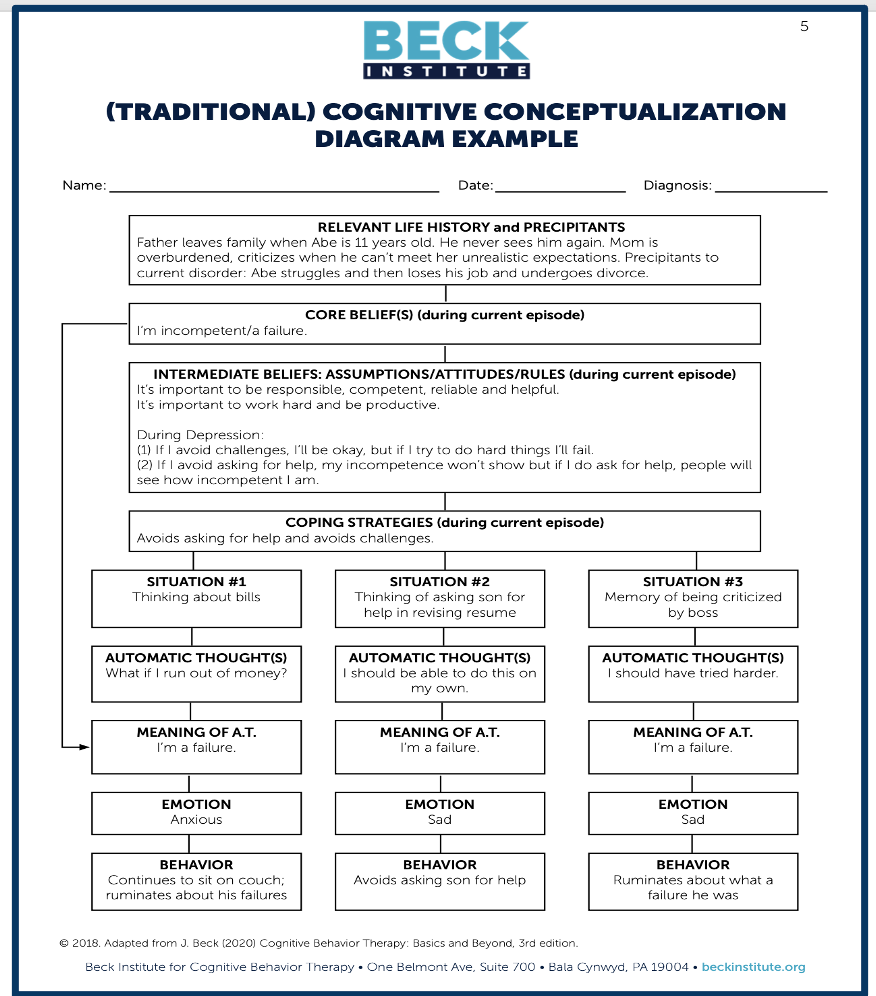
How does that belief system look like in the cognitive model? Think about an Overview.
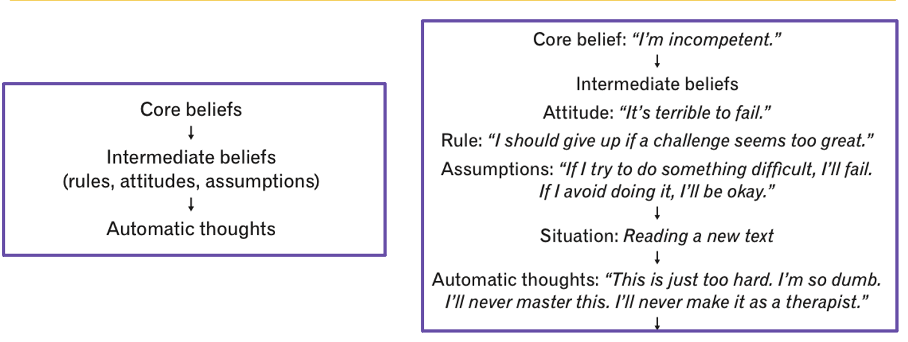
What are automatic (hot) thoughts?
= thoughts that are rapid, ingrained, and subconscious which influence a person's mood and behaviors.
quite brief, and patients are often more aware of the emotion they feel as a result of their thoughts than of the thoughts themselves
can provoke intense negative emotions.
may be in verbal form, visual form (images), or both
Are easier to modify, then intermediate and core beliefs
How does CBT works with automatic thoughts?
CBT mainly works with negative automatic thoughts, they are kind of cognitive distortions - e.g.:
“It’s all my fault.” (Personalization and Blame)
“This will never work out.” (Catastrophizing)
“Nobody really cares about me.” (Overgeneralization)
Most of the time we are barely aware of these thoughts, although with just a little training we can easily bring these thoughts into consciousness.
People usually accept their automatic thoughts as true, without reflection or evaluation.
People focus more on our feelings than on the thoughts triggering them.
However, it's usually these automatic thoughts that have the greatest impact on our emotional state, rather than the situation itself.
→ CBT focuses on making individuals recognize and assess negative automatic thoughts to understand their impact and validity for better coping with our emotions.
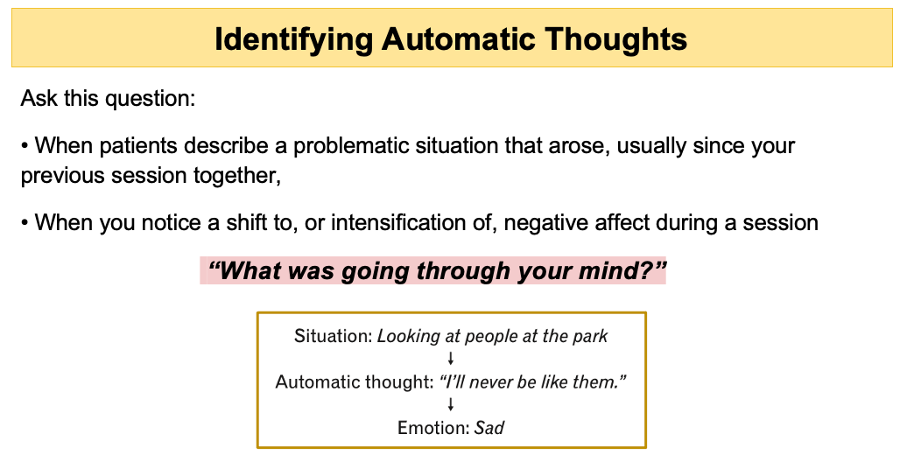
How can you identify automatic thoughts?
What are intermediate beliefs and how can you identify these?
= Composition thoughts of rules (e.g. “If-then” emerged of actual maladaptive coping strategies and cognitive distortions), attitudes, and assumptions
Not easily modifiable as automatic/hot thoughts, but more malleable than core beliefs.
Examples:
“It’s terrible to be helpless.”
“If I work extra hard, I can do okay. If I don’t work hard, I’ll fail.”
“It’s important to be responsible, competent, reliable and helpful.”
“I should figure things out for myself.”
“I should be great at everything I try.”
What are Core beliefs and how can they identified?
= are one’s most central ideas about the self (Shemas)
Beck differentiates the two by suggesting that schemas are cognitive structures within the mind, the specific content of which are core beliefs
People develop these beliefs from an early age, as children, with their genetic predisposition toward certain personality traits, interact with significant others, and encounter a series of situations
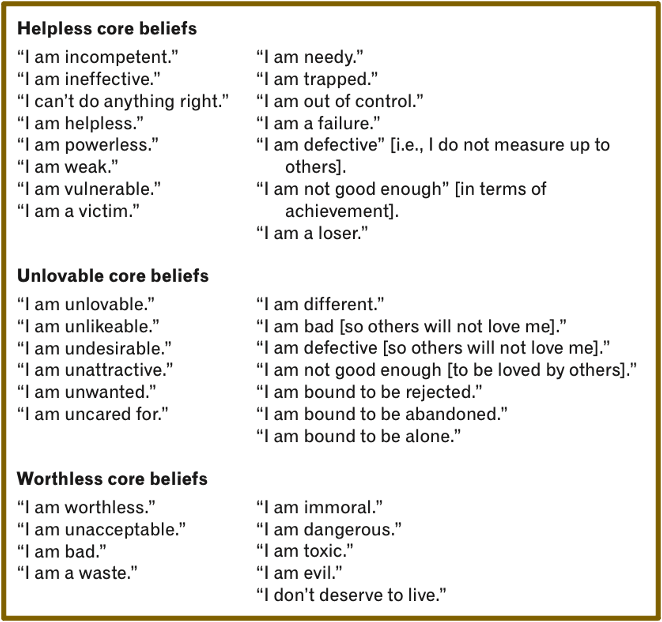
can be categorized in three negative core beliefs
can be identified by the Down-ward-arrow technique
→ Not the situation itself, but our interpretation of our core beliefs/self-assumptions is important.
Which 3x primary types of negative core beliefs regarding the self suggests Beck to identify?
Beliefs categorized as helplessness pertain to feelings of personal inadequacy, vulnerability, and inferiority.
Core beliefs associated with unlovability entail concerns about being unlikable and unable to establish intimate connections
worthlessness-themed beliefs revolve around the perception of insignificance and feeling burdensome to others.
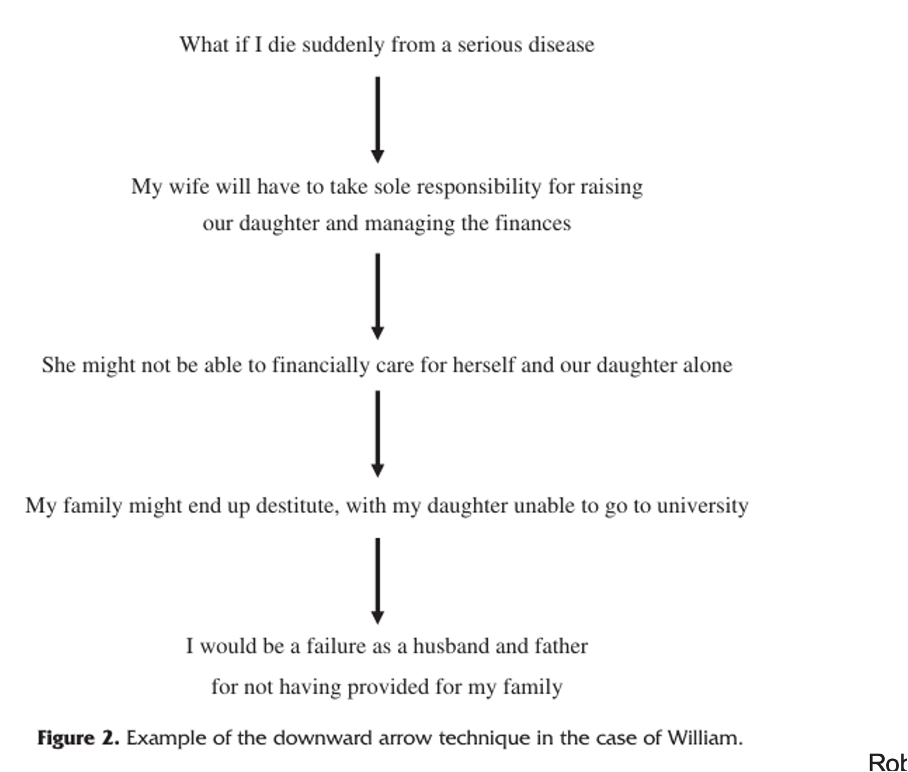
What is the Down-ward-arrow technique and the goal of it?
= strategy used to uncover the core beliefs behind negative responses to a situation.
It involves repeatedly asking questions regarding the primary three negative core beliefs, probing deeper with each response from the client.
“If that thought was true, what does it mean?”
“What’s so bad about that thought?”
“What does it say about you as a person?”
Not the situation itself, but our interpretation of it (core beliefs, assumptions).
“If that thought was true, what does it mean?”
“What’s so bad about that thought?”
“What does it say about you as a person?”
→ The therapist employs this technique to delve deeper than surface-level beliefs, seeking to comprehend why the client reacts to the situation in that manner.
The goal is for clients to gain insights into their core beliefs through this process.
What is the Socratic questioning - technique exactly?
= Methode des Fragens und der Diskussion, die vom antiken griechischen Philosophen Sokrates entwickelt wurde.
Fragender stellt eine Reihe offener Fragen, um kritisches Denken anzuregen, Ideen zu erhellen und zugrunde liegende Annahmen aufzudecken.
Anstatt direkte Antworten zu geben, ermutigt die sokratische Methode Personen dazu, durch begründete Argumentation und Selbstreflexion zu eigenen Erkenntnissen zu gelangen.
Beispiel 1: Lehrer, der die sokratische Methode verwendet, Fragen stellt Fragen wie "Warum glaubst du, dass das die richtige Antwort ist?" oder "Wie kommst du zu dieser Schlussfolgerung?" → Diese Fragen sollen dazu beitragen, dass die Schüler tiefer über das Thema nachdenken und ihre eigenen Gedanken besser verstehen.
Beispiel 2: Klienten dabei zu helfen, ihre eigenen Denkmuster und Überzeugungen zu erkunden. Ein Beispiel:
Therapeut: "Können Sie mir mehr darüber erzählen, warum Sie glauben, dass Sie in dieser Situation immer versagen?"
Klient: "Nun, ich denke, ich bin einfach nicht gut genug. Ich habe es in der Vergangenheit versucht und bin jedes Mal gescheitert."
Therapeut: "Verstehe. Welche Beweise haben Sie dafür, dass Sie nicht gut genug sind?"
Klient: "Nun, ich habe es versucht, aber es hat nie funktioniert."
Therapeut: "Das ist interessant. Können Sie mir von einer Zeit erzählen, in der Sie erfolgreich waren? Was war anders?"
→ Durch diese Art von Fragen hilft der Therapeut dem Klienten, seine eigenen Gedanken und Annahmen zu hinterfragen und möglicherweise zu erkennen, dass die zugrunde liegenden Überzeugungen nicht unbedingt wahr sind oder nuancierter betrachtet werden können.
How does a traditional cognitive Case Conceptualization and Formulation Questionnaire looks like?