Practical 22: Neoplasms of Squamous Epithelium
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
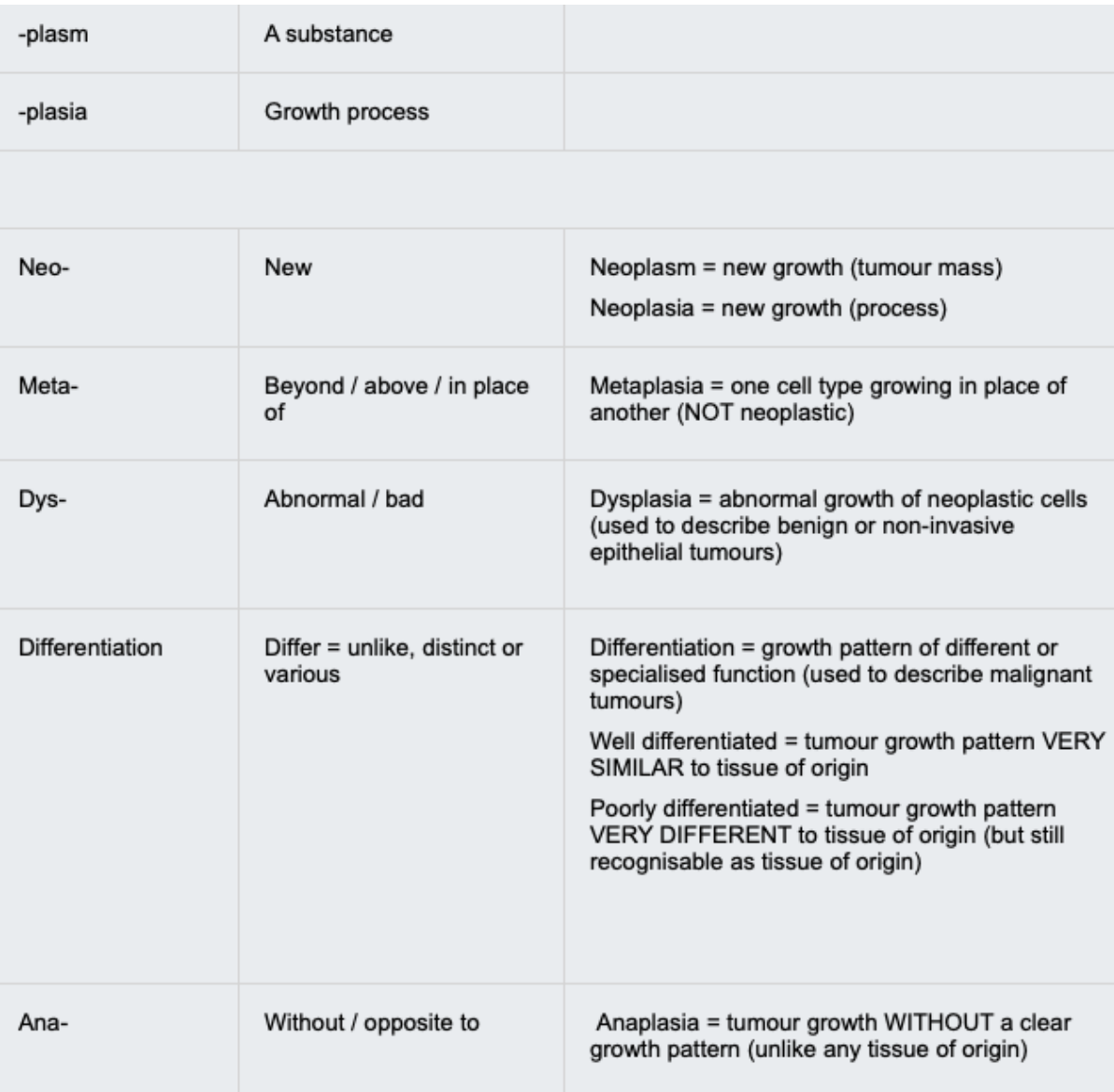
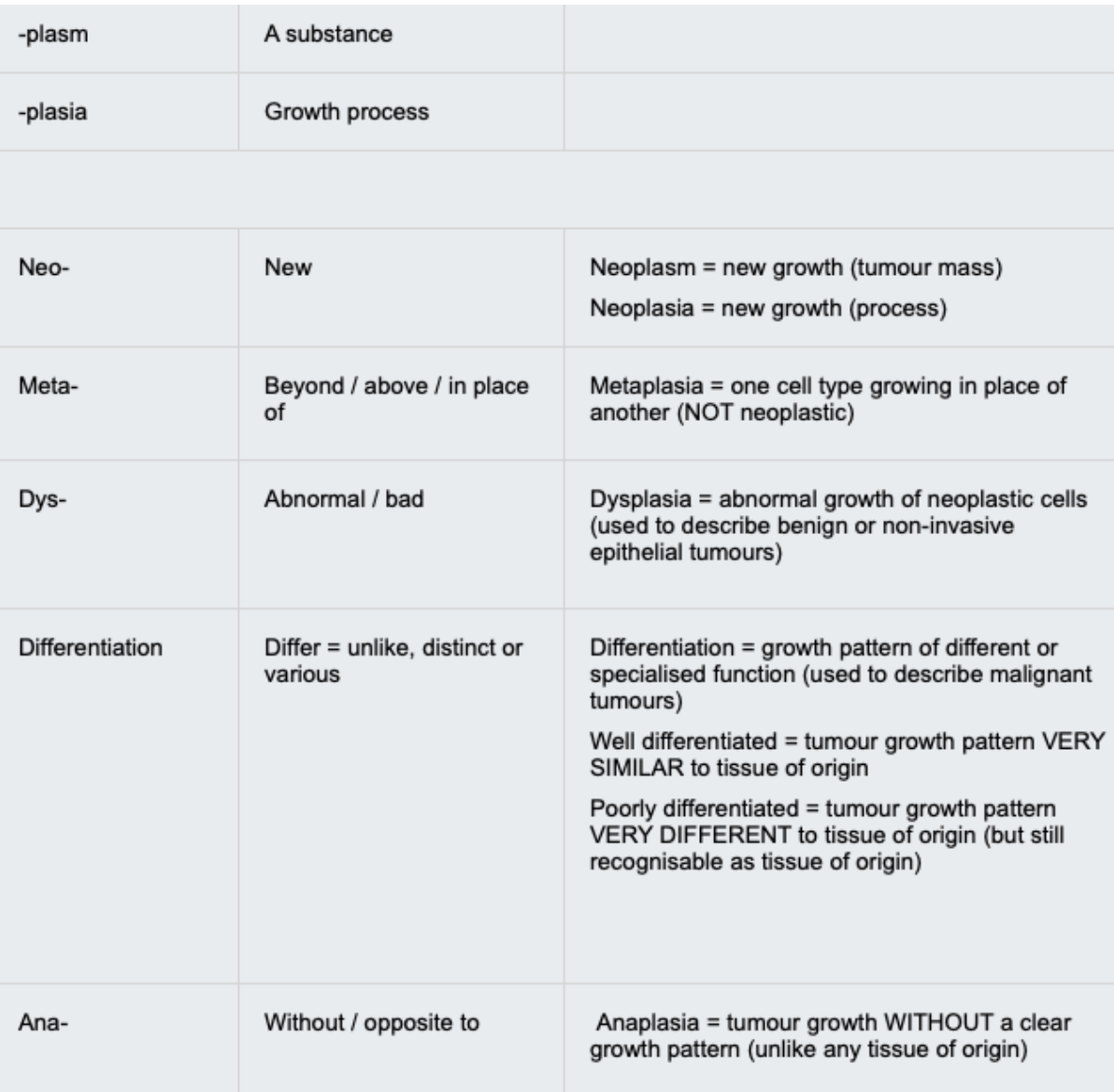
Hyperplasia
Hyperplasia is a physiological increase in cell number in response to a stimulus.
Metaplasia
Metaplasia is a reversible, physiological change from one normal differentiated cell type to another normal differentiated cell type.
Dysplasia
Dysplasia is the presence of abnormal cells that may represent pre-malignant disease which is not invasive.
Increased red blood cell production to compensate for relative hypoxia at altitude →
hyperplasia
Abnormal looking cells in the bronchus →
dysplasia
A change from respiratory pseudo-stratified epithelium to squamous epithelium in the bronchus →
metaplasia
A change from glandular to squamous epithelium in the endocervix in response to pH →
metaplasia
Pleomorphic, non-invasive squamous cells in the cervix →
dysplasia
Relationship of metaplasia to neoplasm
Metaplasia can precede neoplasia. In these cases, it is the persistent presence of the underlying stimulus, rather than the metaplasia, that drives development of neoplasia.
• Chronic cellular injury by cigarette smoke → metaplasia in the bronchi
• Chronic cellular injury by the reflux of acid from the stomach → metaplasia in the oesophagus
• Chronic cellular injury due to pH being lowered by the metabolism of glucose to lactic acid by bacteria → metaplasia in the uterine cervix
Neoplasms of Squamous Epithelium
Benign and malignant neoplasms can arise from any squamous epithelium, from metaplastic processes or otherwise. This includes the epidermis of the skin, vaginal canal and parts of the cervix and gastro-intestinal tract.
Important principles of neoplasia
• Neoplasms often show a stepwise development and a sequence of events can be followed (such as in the CIN-carcinoma sequence)
• Infectious agents can play a role in the development of certain neoplasms
• The use of screening can detect pre-cancerous neoplastic cells and allow early treatment to prevent cancer
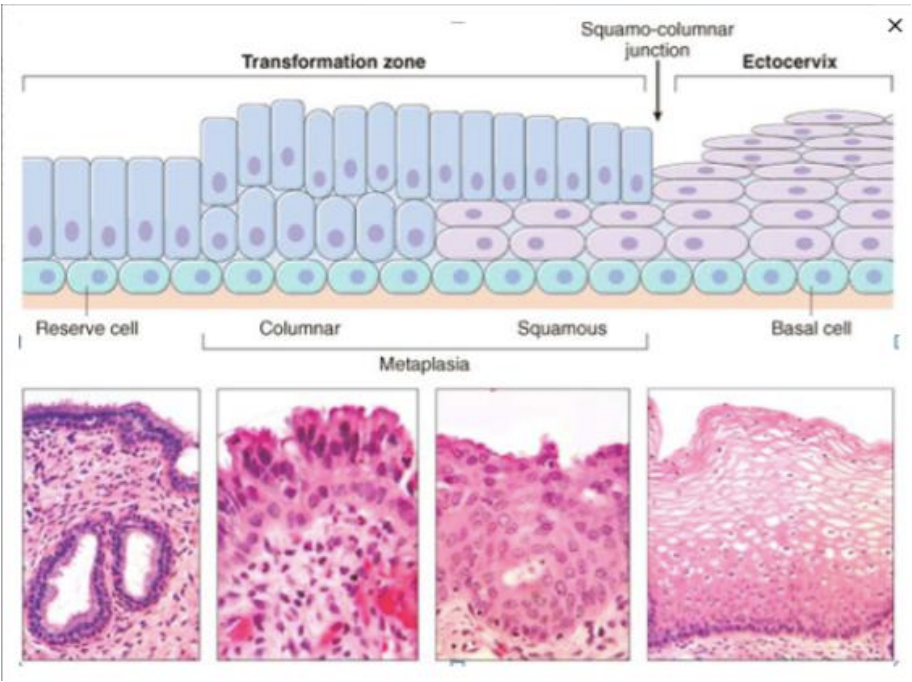
The Transformation Zone of the Normal Adult Cervix: Squamous Metaplasia
The lining of the cervix varies depending on the location. The endocervical canal is lined with single-layered, columnar glandular epithelium, whereas the ectocervix (the part that projects into the vagina) is lined with squamous epithelium.
Endocervical glands
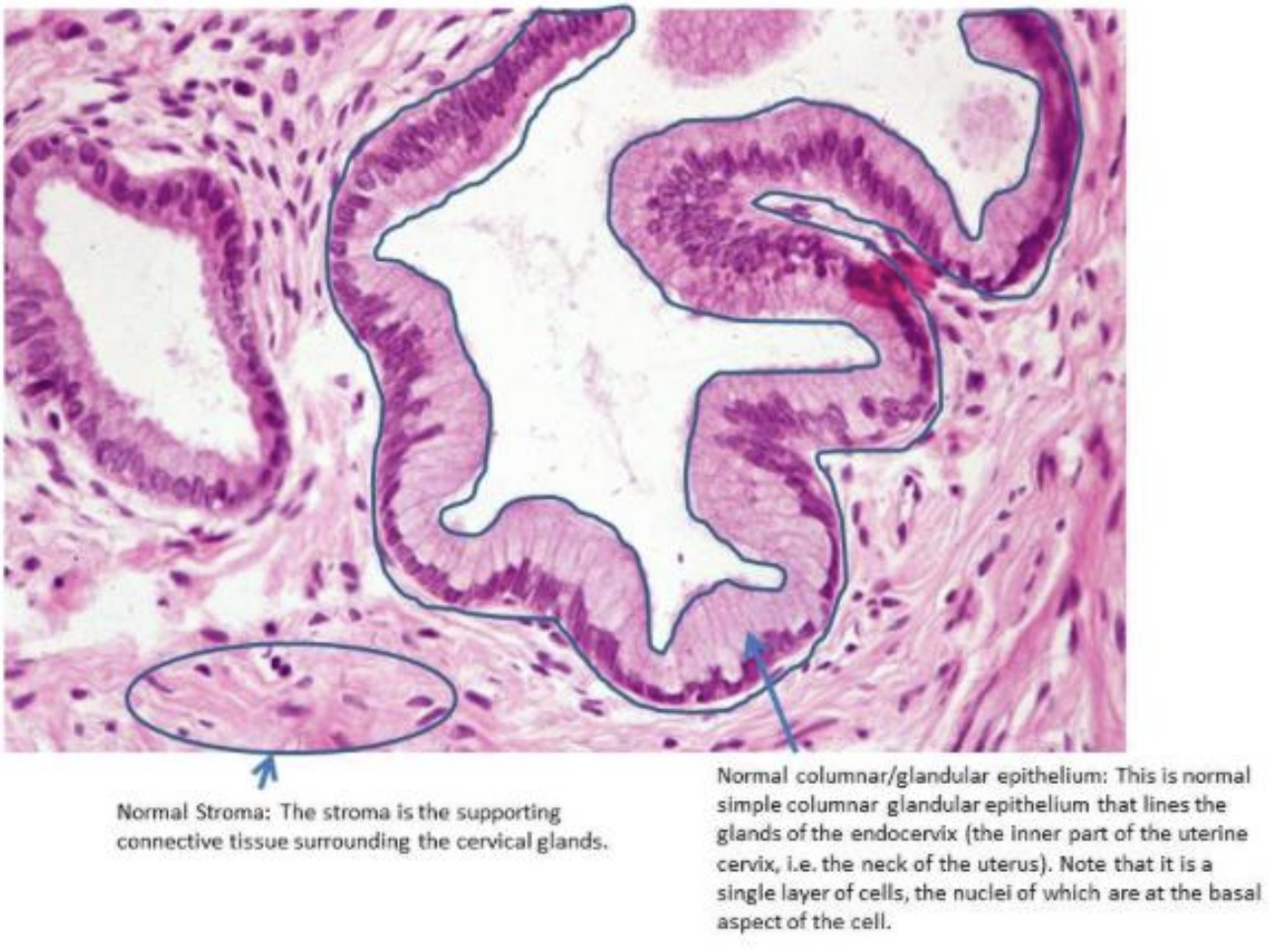
Ectocervical squamous epithelium
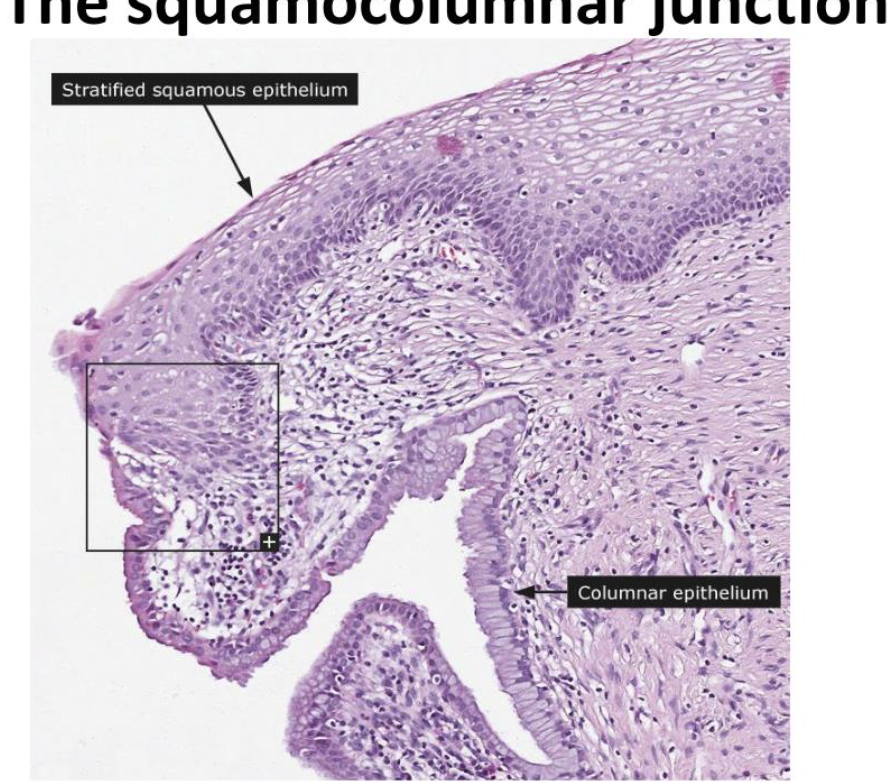
squamo-columnar junction (SCJ)
The region of the cervix where the epithelium of the endocervix meets the epithelium of the ectocervix is called the squamo-columnar junction (SCJ). The position of the SCJ is fixed during development.
What can trigger metaplasia of the endocervical columnar epithelium
With the onset of puberty, hormonal stimuli cause metaplasia and it begins a gradual transformation into squamous epithelium.
This is a normal physiological process and a new SCJ is formed as a result.
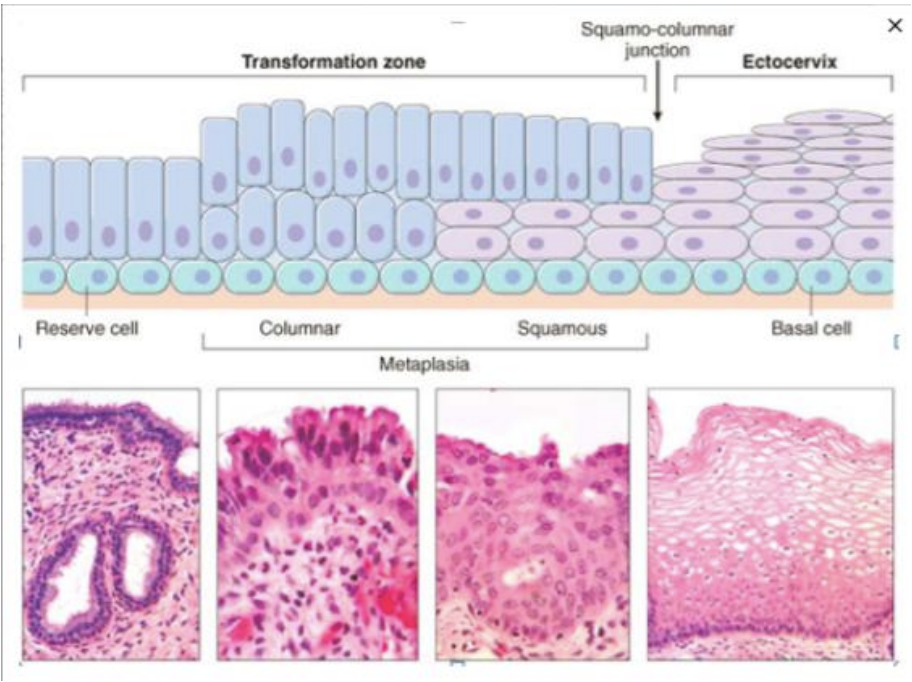
The transformation zone
The transformation zone is the area between the original (fixed, pre-pubertal) SCJ and the new (post-pubertal) SCJ where the columnar epithelium has been replaced and/or is being replaced by new metaplastic squamous epithelium.
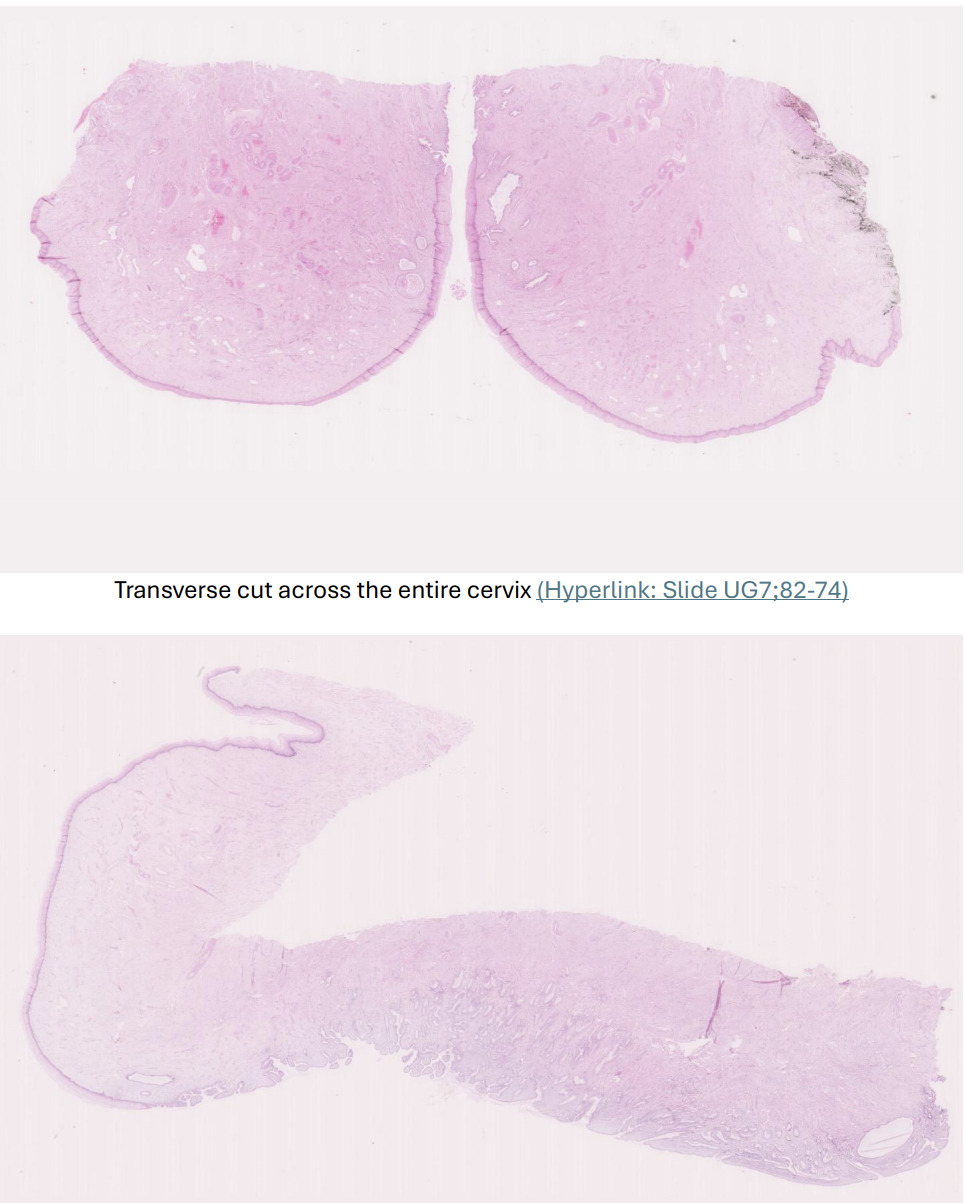
Normal adult cervix
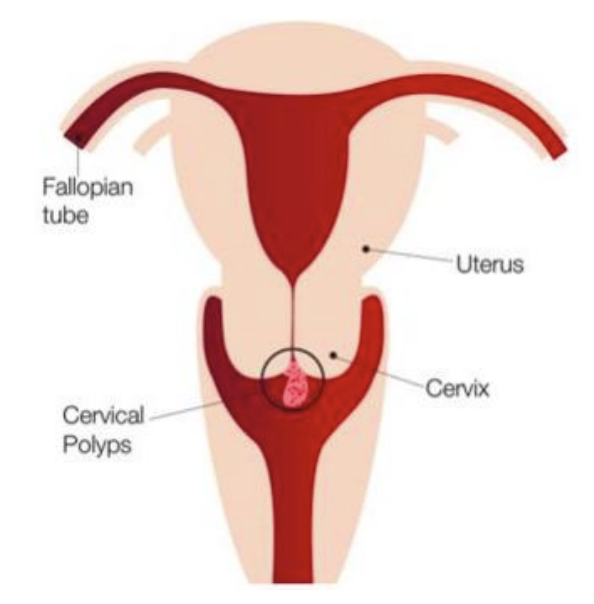
polyp
A polyp is a projection of tissue, usually on a stalk.
Endocervical Polyp: Squamous Metaplasia
Another example of squamous metaplasia can occur when an endocervical polyp (a polyp of endocervical tissue) projects down into the ectocervix and lies across the transformation zone.
As the polyp is now sitting in the ectocervix, its epithelium may respond to this change in environment by undergoing squamous metaplasia, changing from the single-layered, columnar glandular epithelium of the endocervix, into the squamous epithelium of the ectocervix. This metaplasia abundantly found on surface rather than within the glands.
NOTE: polyp will not have a transformation zone or SCJ as it is not anatomically derived from the area of the cervix where they are found. Instead, it will simply have some foci of squamous metaplasia, changing the polyp's native glandular epithelium to squamous epithelium.
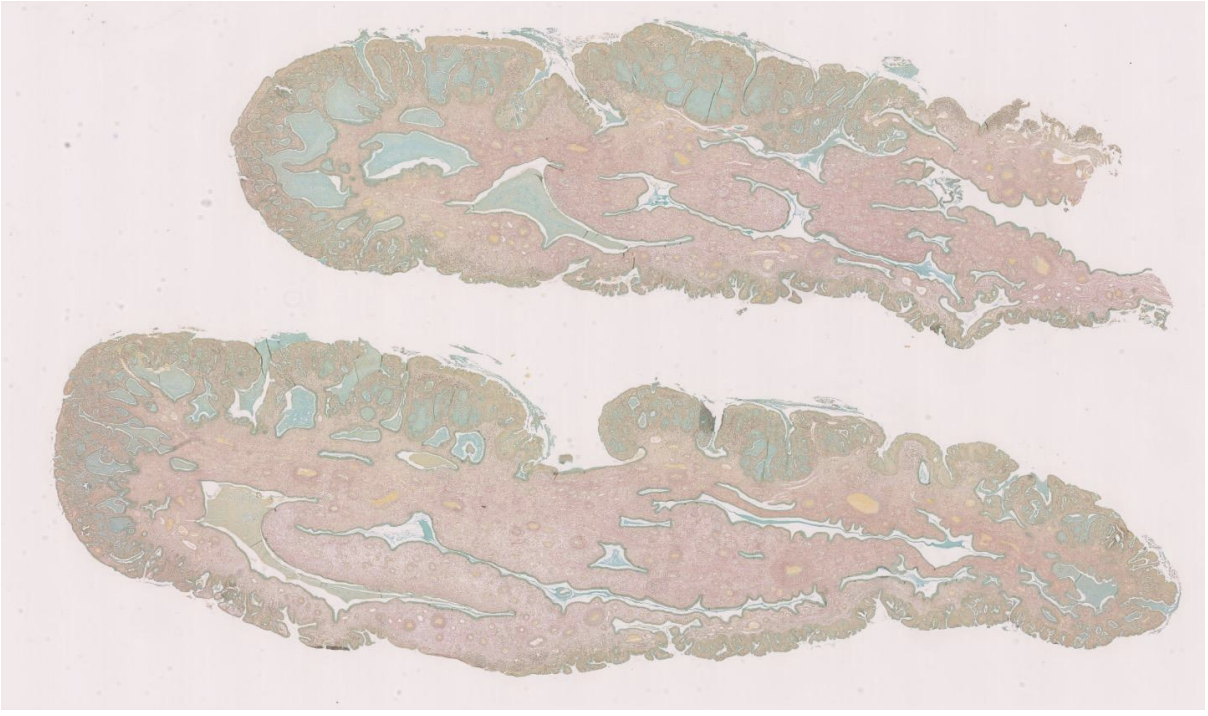
Endocervical Polyp: Alcian blue stain
The polyp has been bisected (cut into two pieces) and you are looking at the two pieces of tissue that made it up. This is not the cervix.
Alcian Blue highlights mucin by staining it blue. Mucin can be seen in large pools within the endocervical glands but can also be seen in individual columnar epithelial cells. It is not present in the metaplastic epithelial cells as they now show squamous differentiation. In places, you can see metaplastic squamous epithelial cells forming layers beneath cells that have differentiated into columnar epithelium.
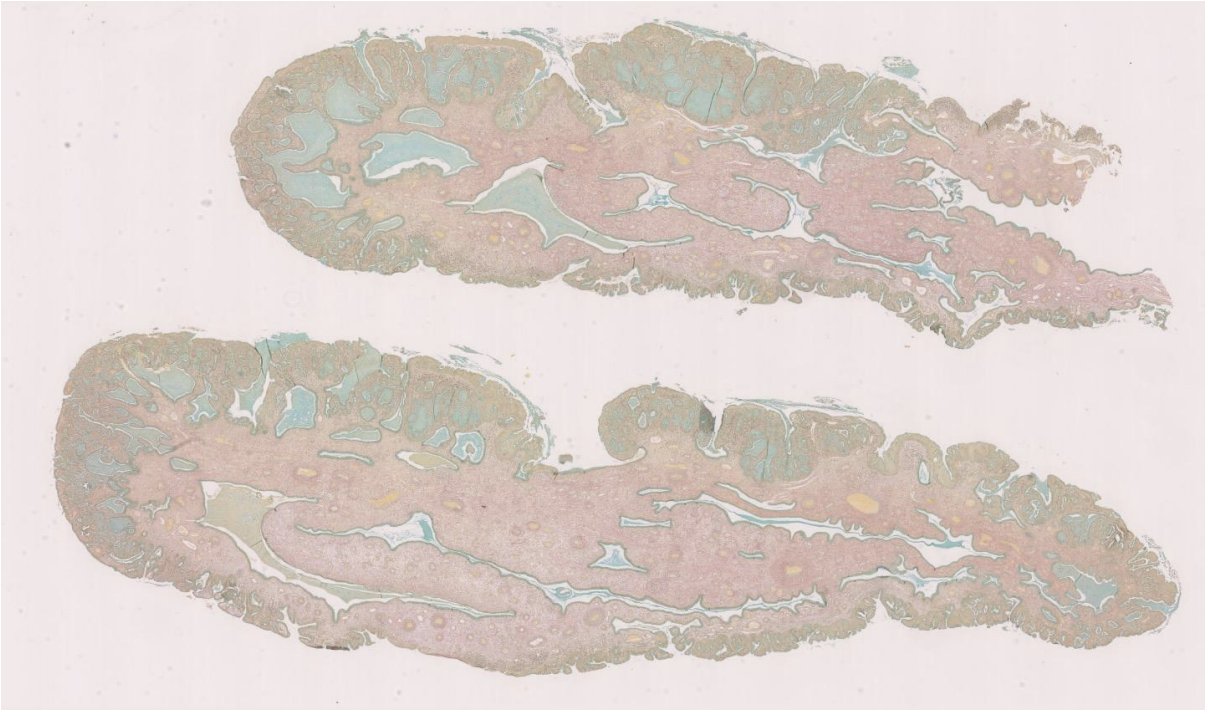
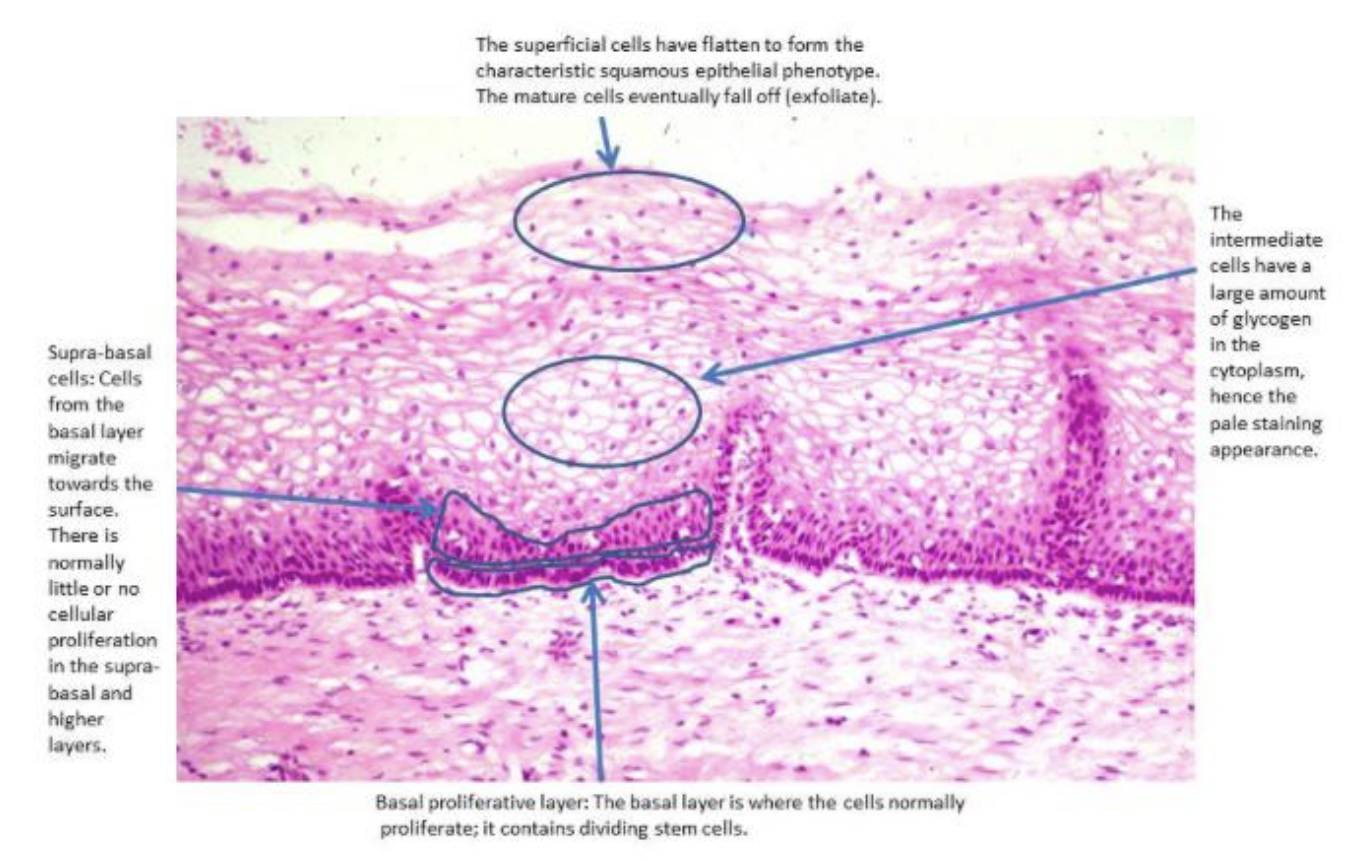
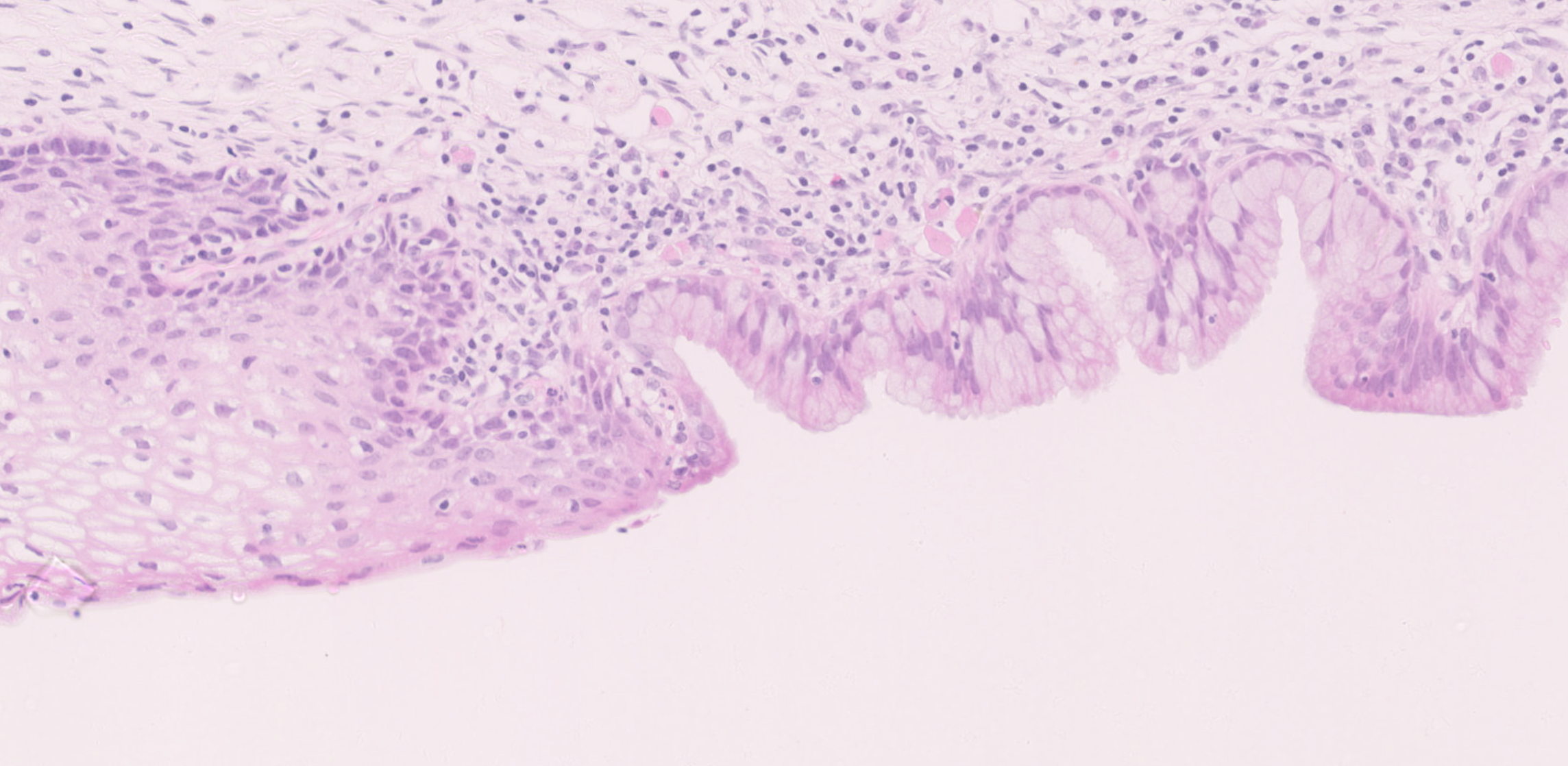
Compare the mature squamous epithelium of the ectocervix with the metaplastic squamous epithelium at the transformation zone. How do they differ?
The metaplastic squamous epithelium may lie under columnar cells within the transformation zone. Immature metaplastic squamous cells resemble those near the base of mature squamous epithelium; they are smaller, with higher nuclear-tocytoplasmic ratios, and are more rounded.
What is the commonest form of cervical cancer?
Squamous cell carcinoma of the cervix which arises within metaplastic squamous epithelium.
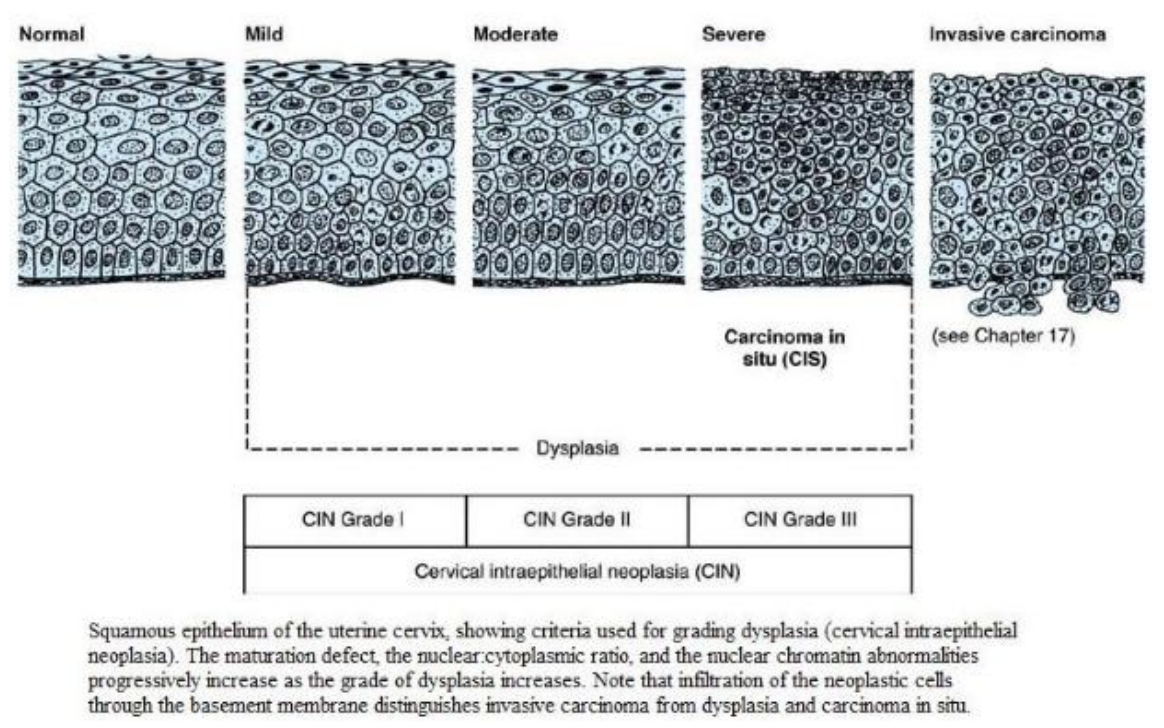
Cervical cancer involves progression from a pre-malignant dysplastic stage called cervical intraepithelial neoplasia (or CIN) to an invasive squamous carcinoma.
Almost all cases of cervical cancer are associated with human papillomavirus (HPV).
HPV
HPV preferentially infects squamous cells in the lower layers of metaplastic squamous epithelium.
Squamous metaplasia itself is not a premalignant change, but a physiological process in the endocervix from the onset of puberty
HPV can induce loss of growth control (leading to cell proliferation and reduced apoptosis) and genetic instability which facilitates the acquisition of additional 9 mutations potentiating progression towards cancer. This is why CIN and cervical carcinoma generally occur at the transformation zone.
The epithelium becomes increasingly dysplastic (cervical intraepithelial neoplasia or CIN) before invasion (carcinoma) occurs.
What is the use of acetic acid on cervix?
Applying a small amount of acetic acid can cause dysplastic cervical epithelium to appear white. This is used in clinical practice to identify sites for biopsy, although the mechanism by which it works is unclear.
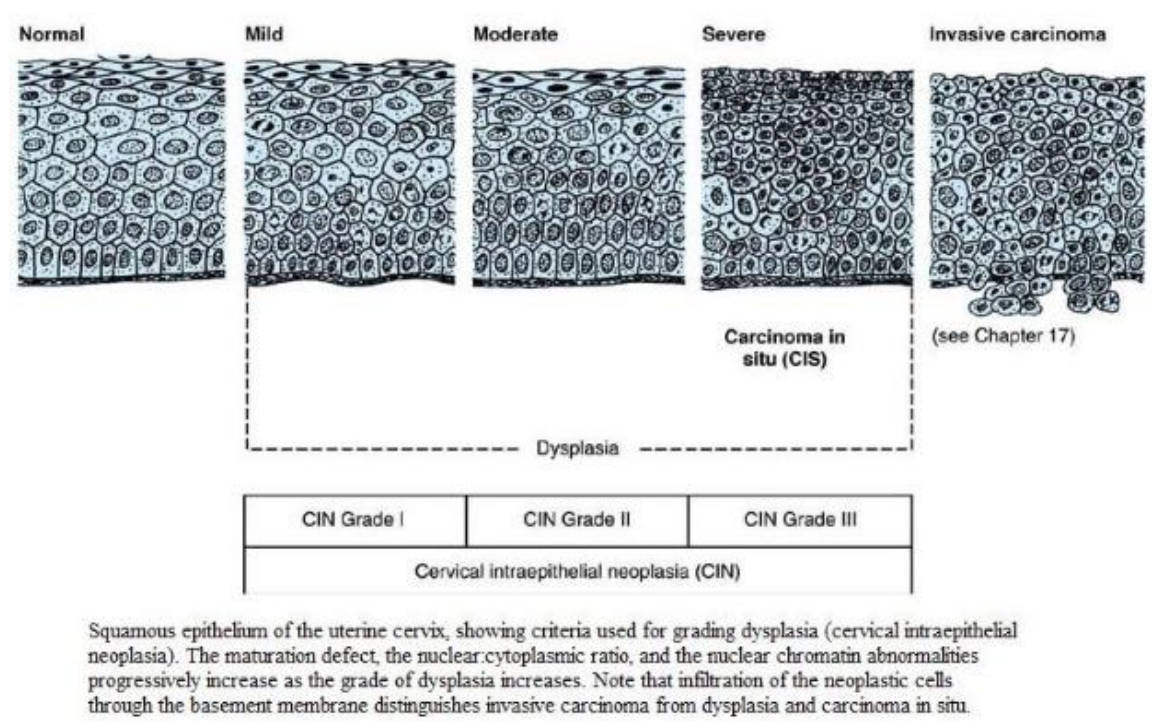
• CIN 1- dysplasia is confined to the lower one-third of the epithelium. Regression is common.
• CIN 2- dysplasia involves the lower two-thirds of the epithelium.
• CIN 3- the full thickness of epithelium contains dysplastic cells. CIN3 has the highest risk of progression to cervical carcinoma.
• Cervical carcinoma- Neoplastic cells penetrate the basement membrane (invasion) and/or are found at a distant sites (metastasis); usually squamous cell carcinoma.
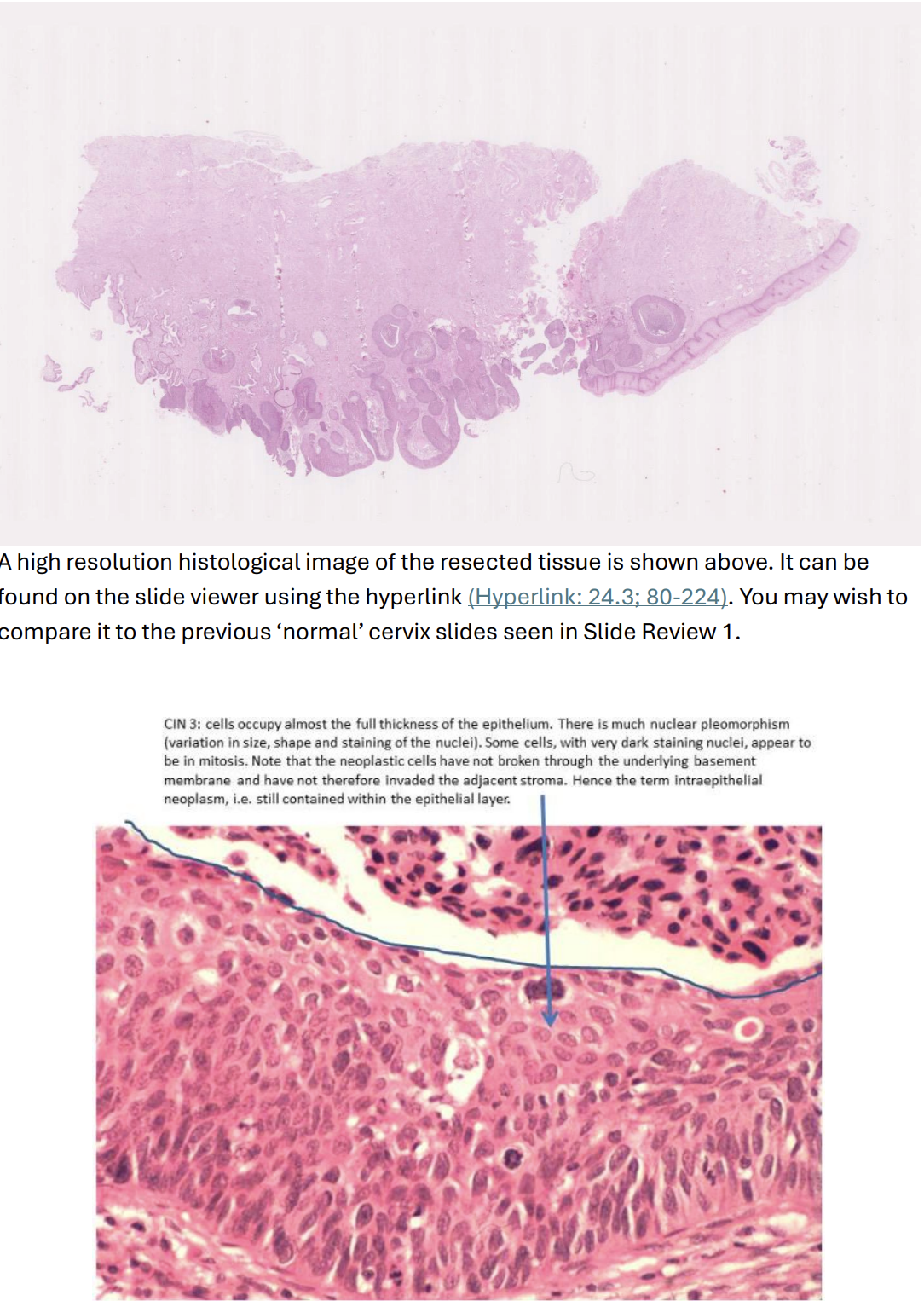
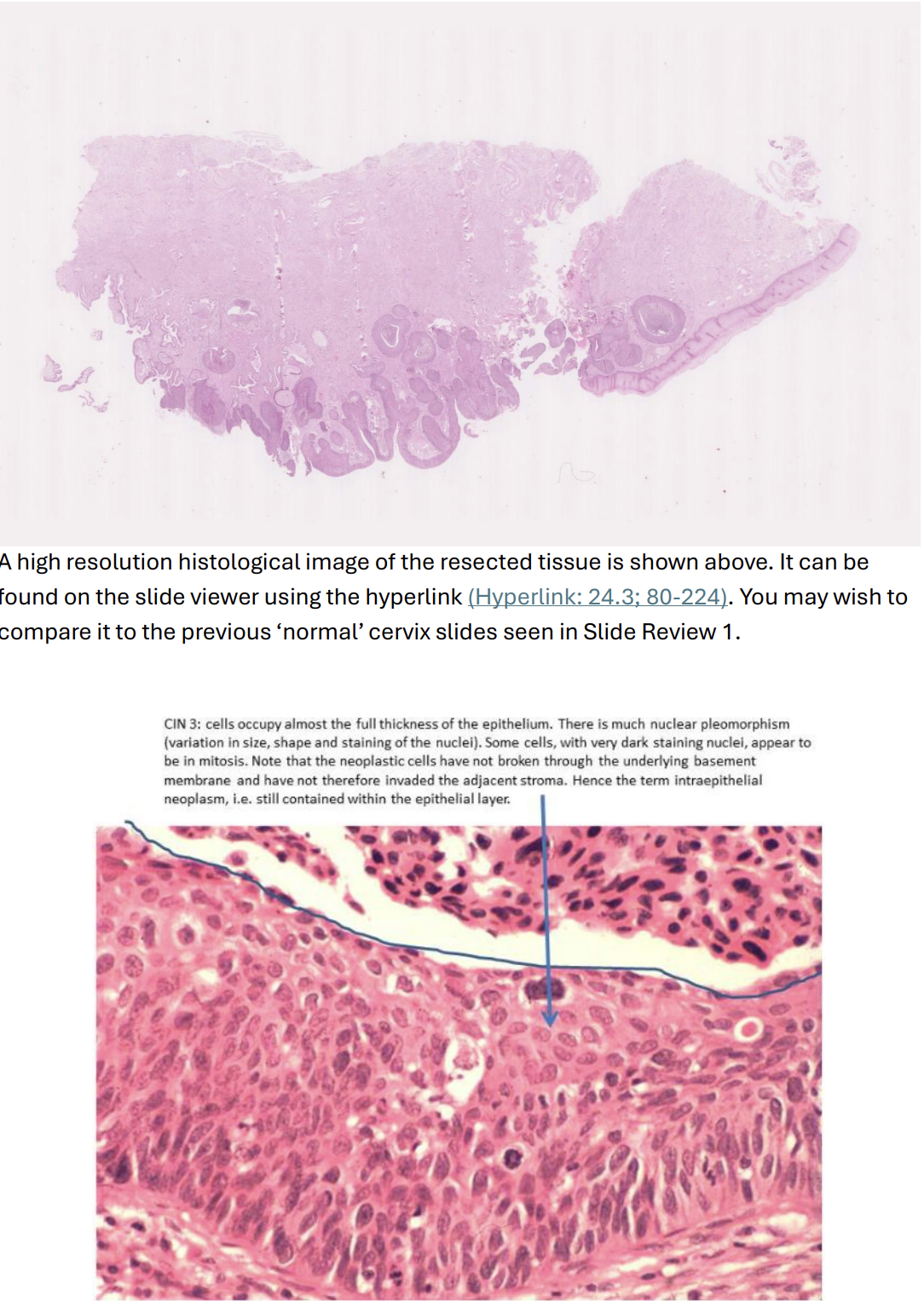
After the discovery of abnormal cells in the cervical smear of a 39-year-old woman, her uterus was removed. A high power histological view of the resected cervical tissue includes an area of full-thickness dysplasia, confined to the epithelium (CIN 3).
The section of cervix in the high resolution image shows extensive full-thickness dysplasia, confined to the epithelium (making it CIN 3) which extends downwards into 12 the endocervical glands.
(Note that this is the same distribution as the squamous metaplasia in the previous sections).
CIN 3 looks much darker than the normal non-keratinised ectocervical epithelium, which is present at one end of the tissue section. This is because the full-thickness of the epithelium is occupied by far more nuclei (which are often larger, pleomorphic and more darkly staining than normal); the cells are abnormally orientated, often appearing to stream towards the surface; and there are mitotic figures at all levels of the epithelium (in normal squamous epithelium only the basal layer contains mitotic figures).
All the areas with metaplastic squamous epithelium show features of CIN3 in this particular example.
Neither the endocervical glands nor the ectocervical squamous epithelium show dysplasia.
Squamous Cell Carcinoma
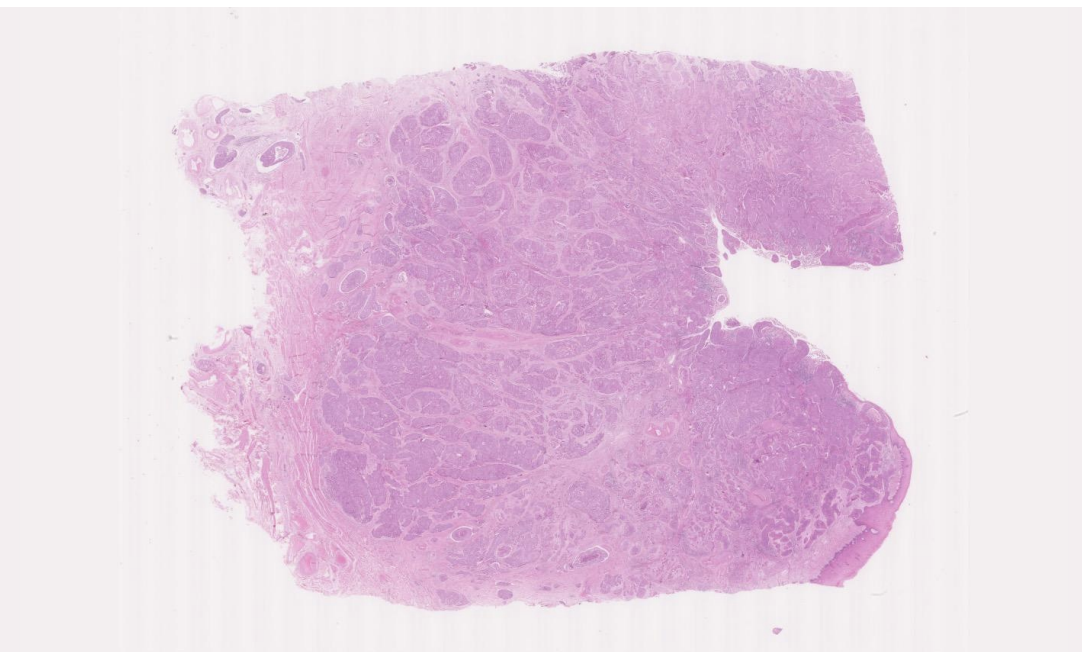
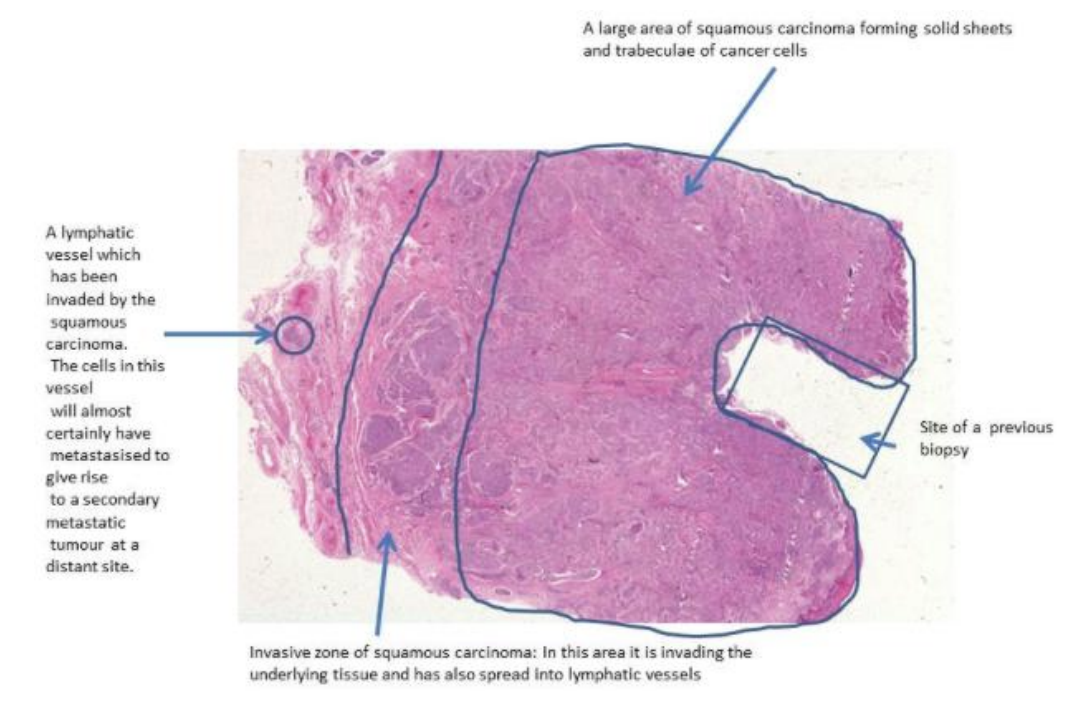
Resected uterus of a 47 year old woman who had noticed some irregular vaginal bleeding. She had never had a cervical smear screening examination, but already had invasive carcinoma by the time she presented to her doctor. This is a squamous cell carcinoma of the cervix.
The carcinoma has invaded down from the epithelium deeply into the connective tissue stroma of the cervix, forming islands, tongues, and some solid sheets of cancer cells. Around the deepest invasive edge, the carcinoma has invaded into some lymphatic vessels.
Metastases might be found in local lymph nodes, if the carcinoma is invading lymphatics.
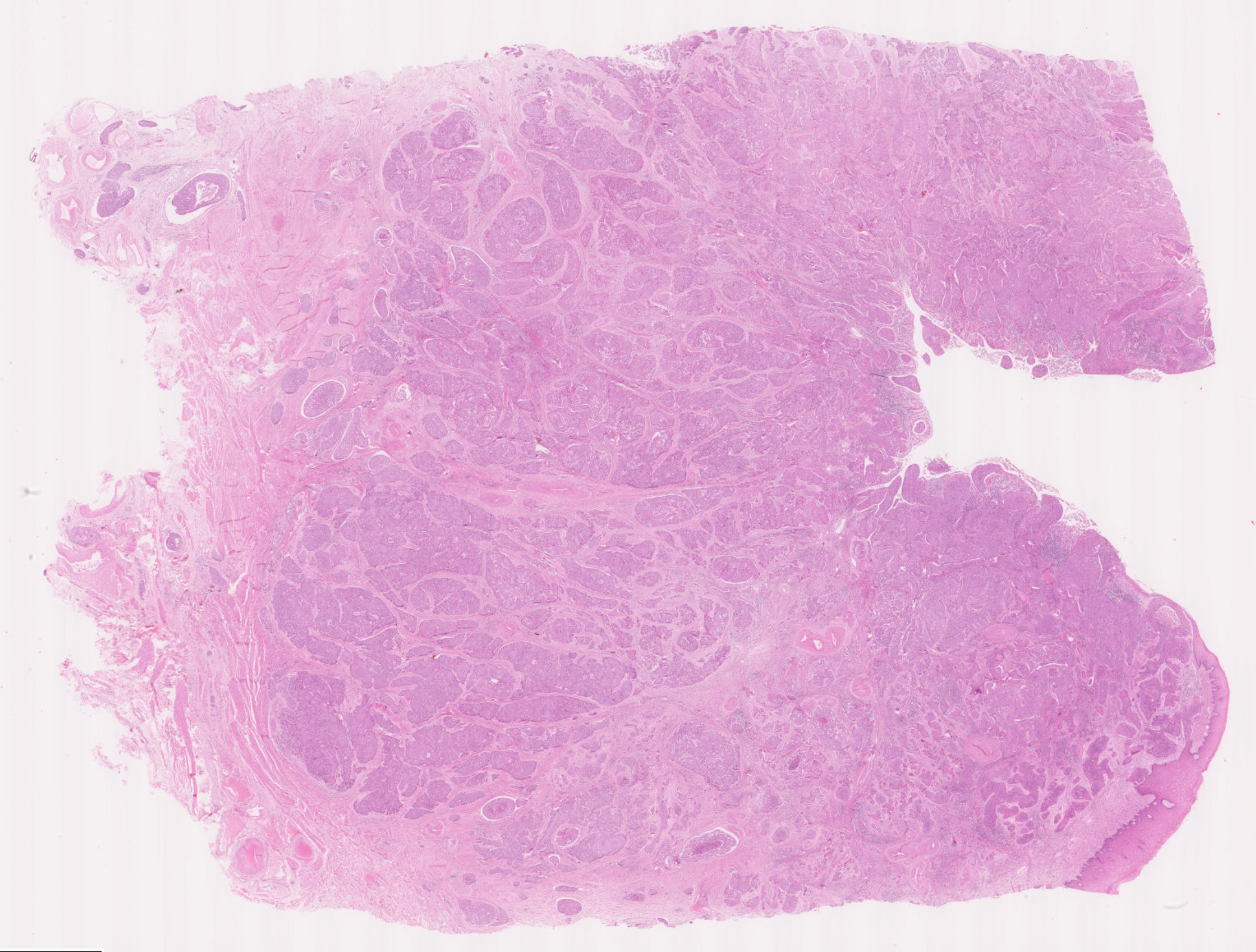
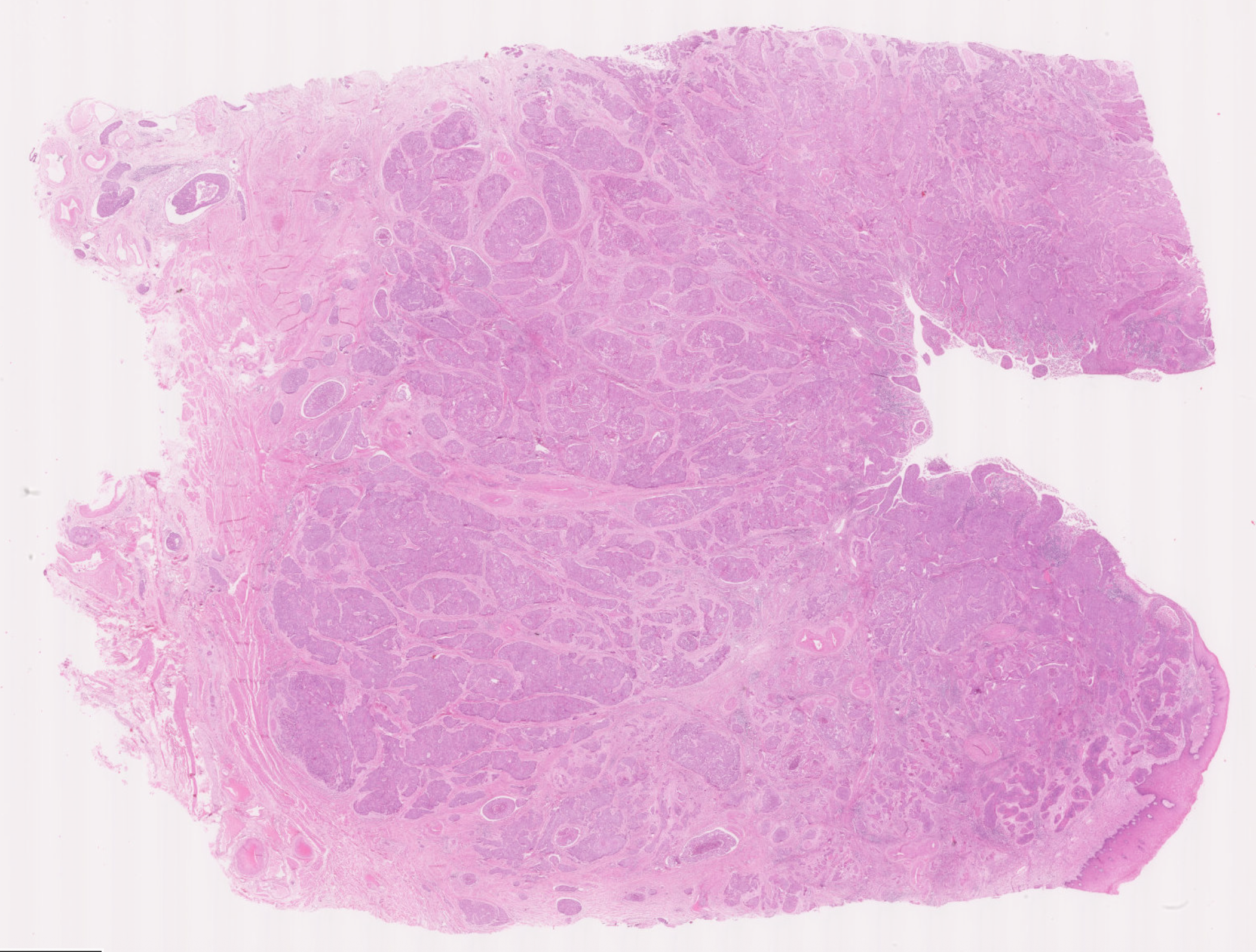
Uterine Cervix
Invasion is seen through the basement membrane into the underlying stroma.
Inflammatory cells (mostly lymphoid cells and other chronic inflammatory cells) can be seen around the invasive cancer edges and some within the carcinoma.
Invasion involves tissue destruction, which excites an inflammatory response. There is also an immune response against the cancer cells.
What features can you recognise to determine the pattern of differentiation of this neoplasm (and therefore its histogenesis, i.e., the cell type it is derived from)?
Squamous differentiation can be seen in places (mostly as prickle cell formation in some areas, however there is very little keratinization in this cancer). Skin cancers often exhibit keratinization with formation of “keratin pearls” of pink whorled keratin.
What does the abbreviation CIN stand for?
Is CIN non-invasive or invasive?
Cervical Intraepithelial Neoplasia
It is pre-malignant, i.e. is currently non-invasive. Should HPV infection and subsequent dysplasia persist, it may progress and become invasive (squamous cell carcinoma).
How would you recognise CIN histologically?
Dysplastic cells within the squamous epithelium, occupying anything from the basal third (CIN 1) to the full epithelial thickness (CIN 3). These cells show disorganized orientation of nuclei with nuclear enlargement, pleomorphism and hyperchromasia, with increased mitotic figures (some of which would look abnormal) above the basal layer.
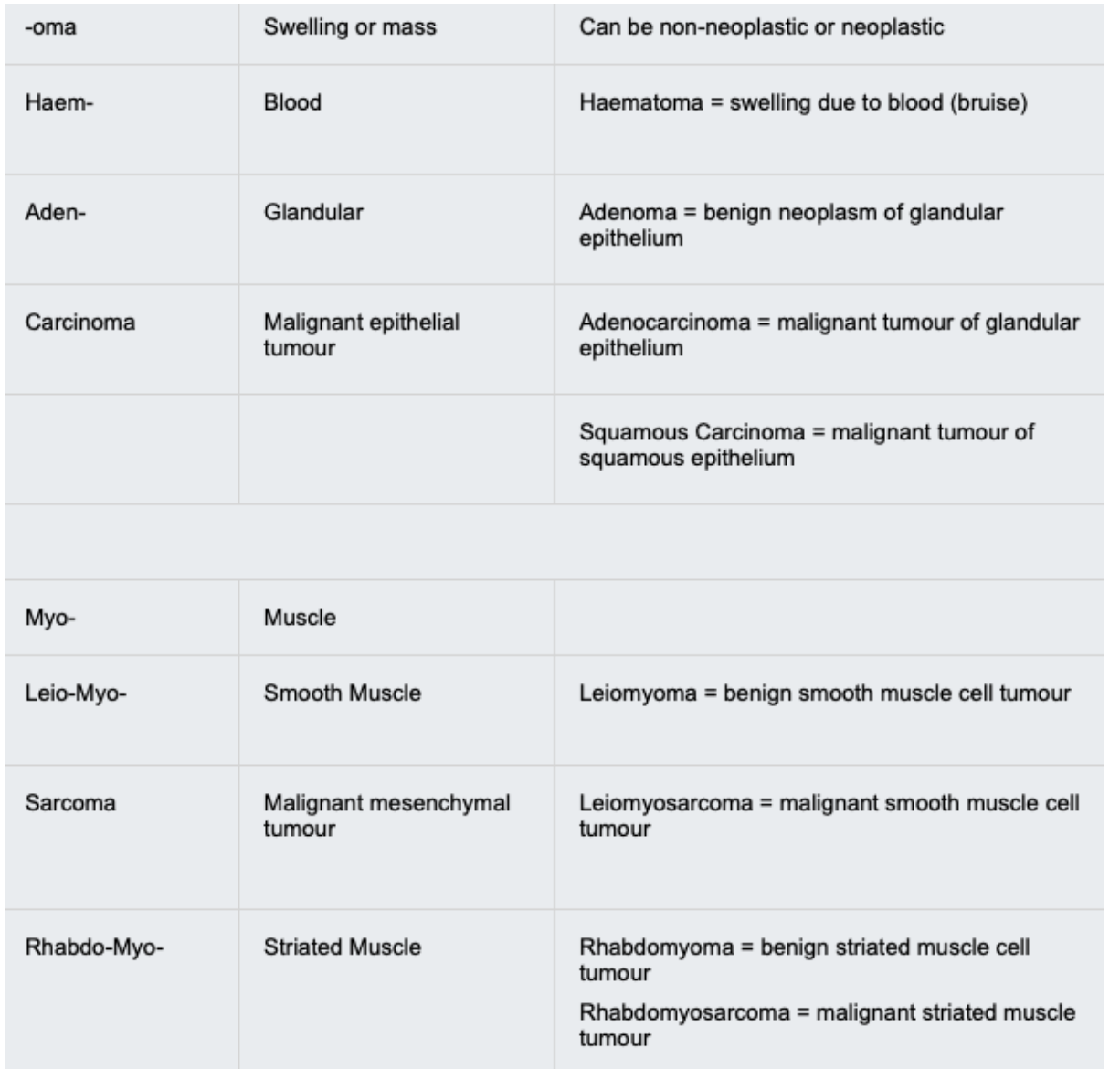
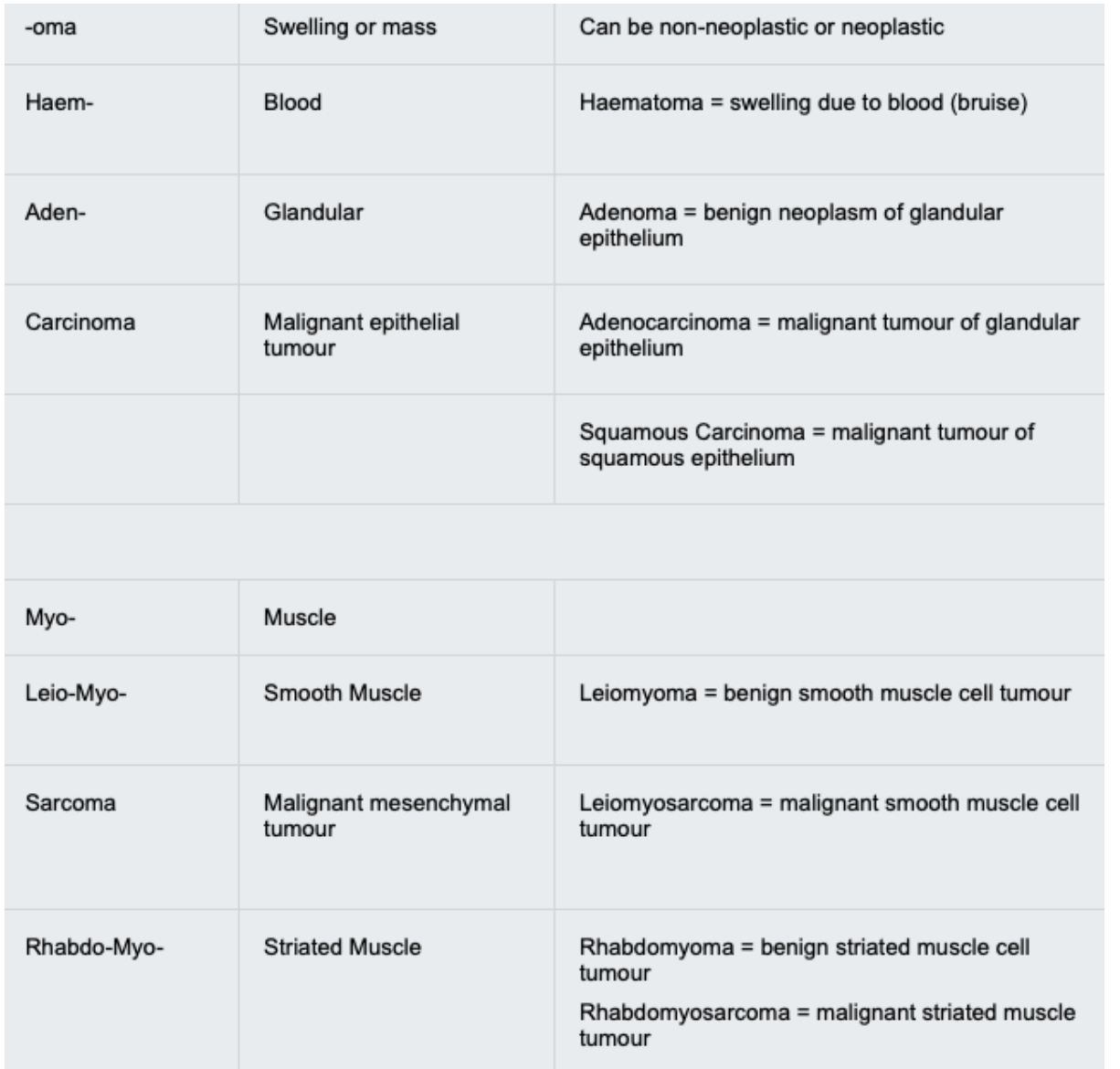
What type of vessel do Carcinomas usually invade earliest?
Lymphatics
NB: these are general rules, there are exceptions
What type of vessel do Sarcomas usually invade earliest?
Blood vessels
NB: these are general rules, there are exceptions
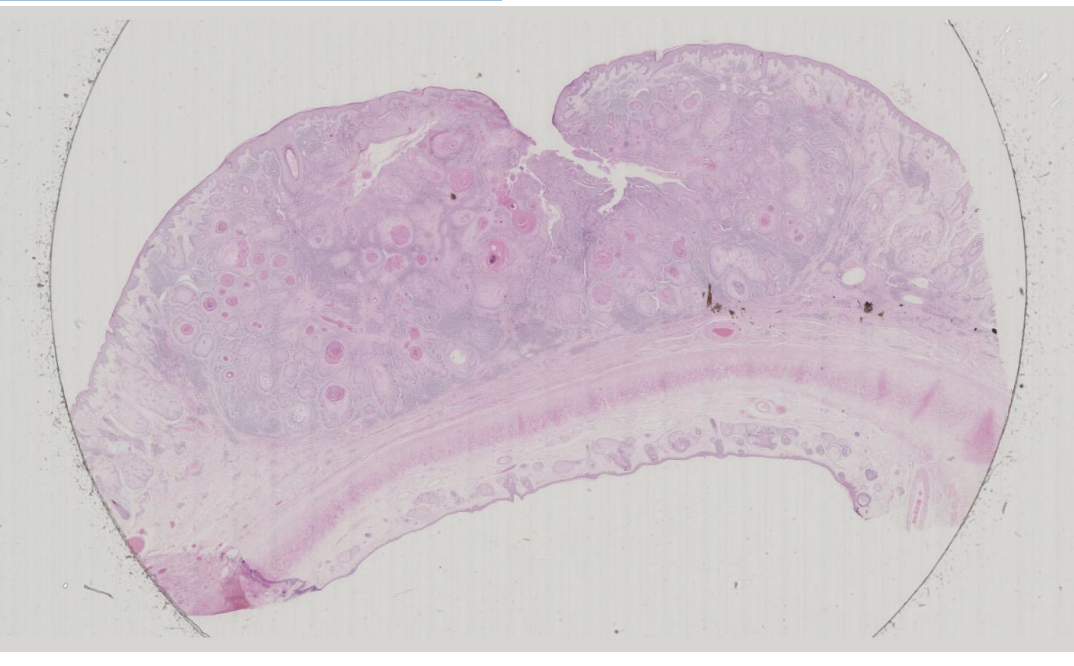
Skin: Squamous Cell Carcinoma
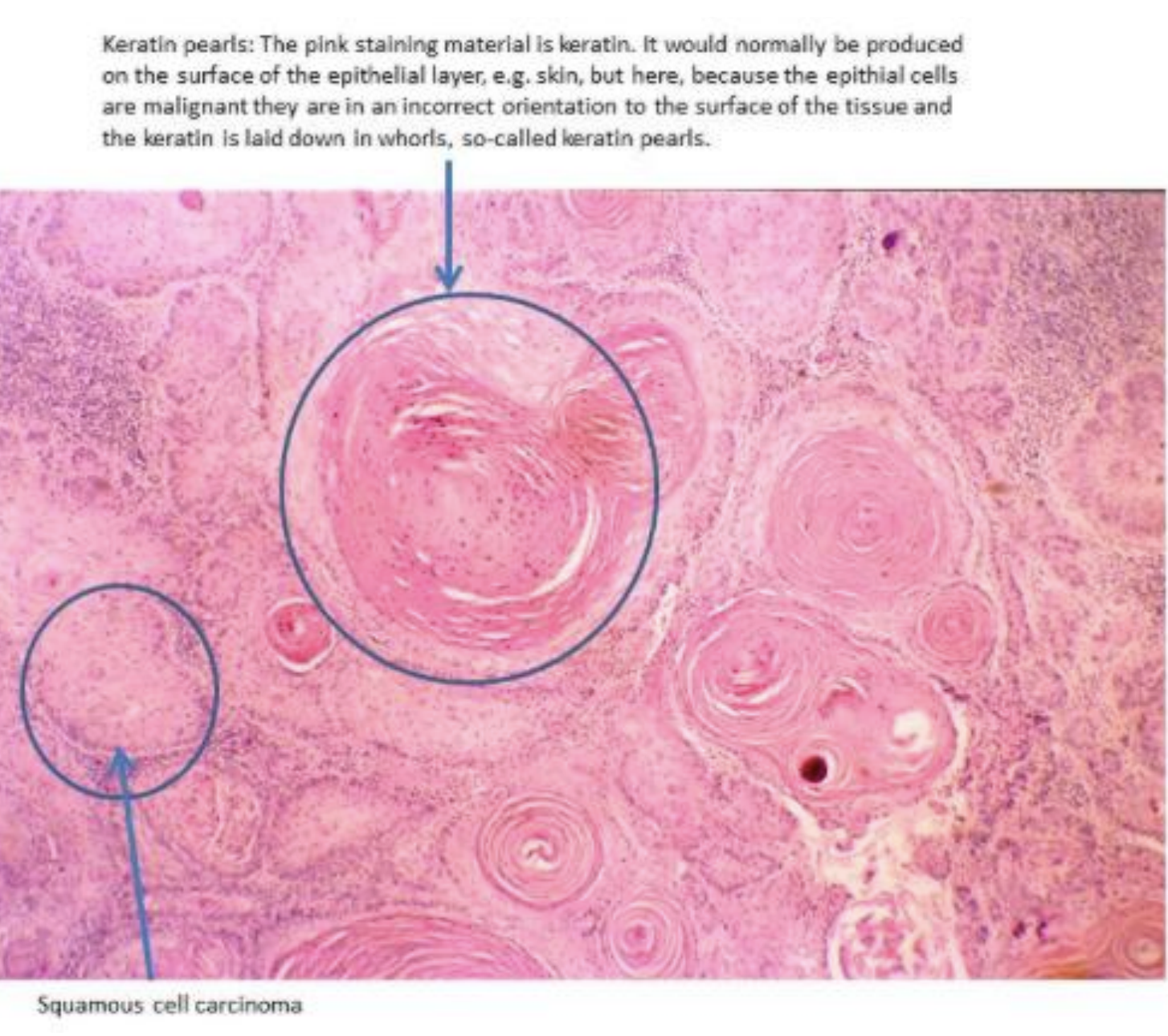
Islands of tumour cells are infiltrating through the dermis of this skin specimen. Many of these islands show central areas of keratin deposition (in H&E preparations this shows up as a bright pink protein).
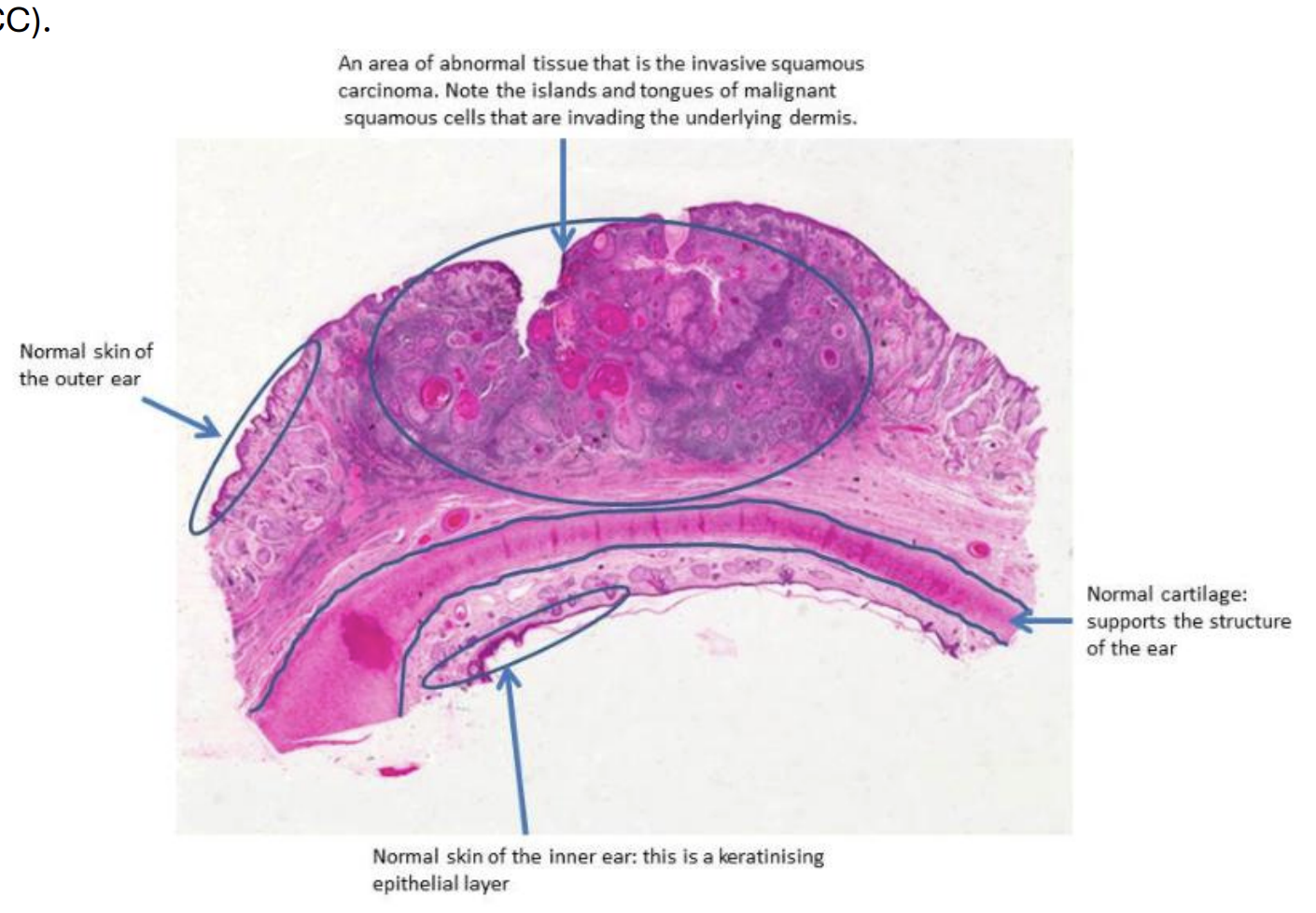
Keratinisation
When keratin deposition forms ovoid shapes, they are referred to as “keratin pearls”. “Keratinisation” is clear evidence of squamous differentiation in the tumour, indicating its squamous histogenesis.
What do you think the main risk factor for the development of this carcinoma is likely to have been? What other risk factors for squamous cell carcinoma can you think of?
On the ear, the most likely risk factor is sun exposure (UV light): incidence is proportional to degree of lifetime exposure
Other risk factors for SCC include:
• Chronic immunosuppression, e.g. chemotherapy or suppression following organ transplant
• Industrial carcinogens, e.g. tar
• Radiation exposure
• Chronic inflammation, e.g. a non-healing, chronic ulcer
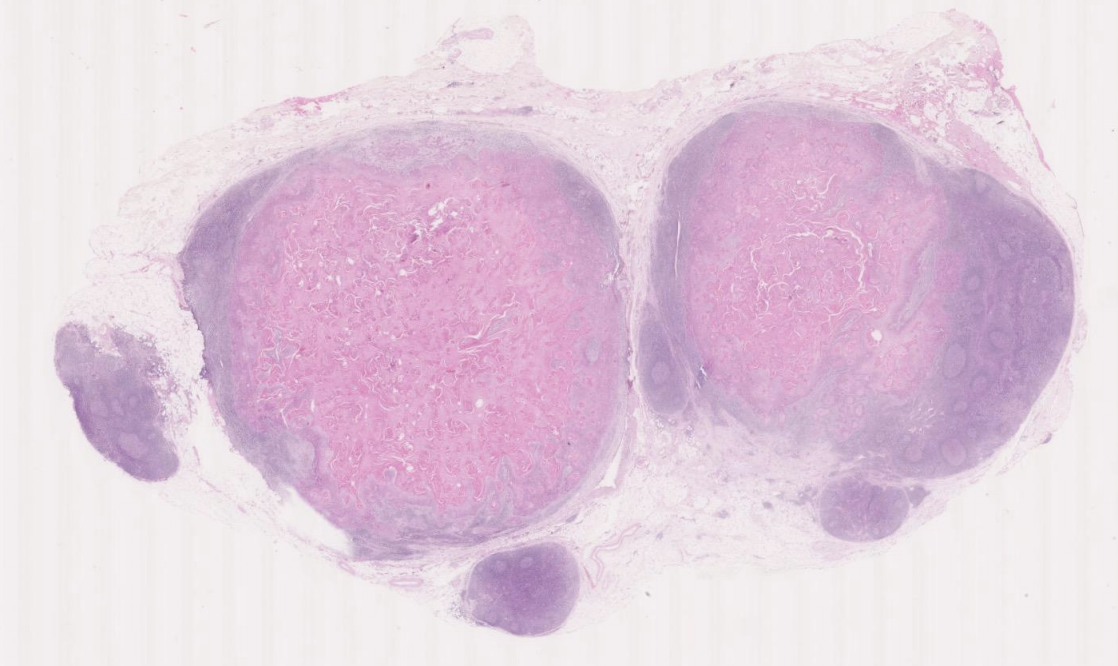
The slide below (which you can view using the hyperlink) shows two enlarged lymph nodes from the neck of a 67 year old man
The two larger lymph nodes are extensively replaced by abnormal tissue in which there is deep pink laminated material, often arranged as whorls; this is keratin and it is immediately surrounded by large cells with features of neoplastic squamous cells. Some contain keratohyaline granules, which are usually seen in the granular layer of keratinised squamous epithelium. At the edges of the epithelial areas, the cells resemble the basal cells of the skin but have nuclei that are quite pleomorphic and contain frequent mitotic figures
The primary tumour was present in the area drained by these nodes, for example in the neck where nodes drain the region including the ear and this might represent spread from the ear skin. However, in a neck lymph node, it is also possible that squamous cell carcinoma might be derived from the upper aerodigestive tract or bronchus (lung cancer)
The appearance is that of metastases of well differentiated, keratinising squamous cell carcinoma.