OB Exam 3: Complications of labor
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
Define preterm labor:
how do healthcare providers diagnose preterm labor? (3)
regular uterine contractions that cause cervical changes b4 37 weeks
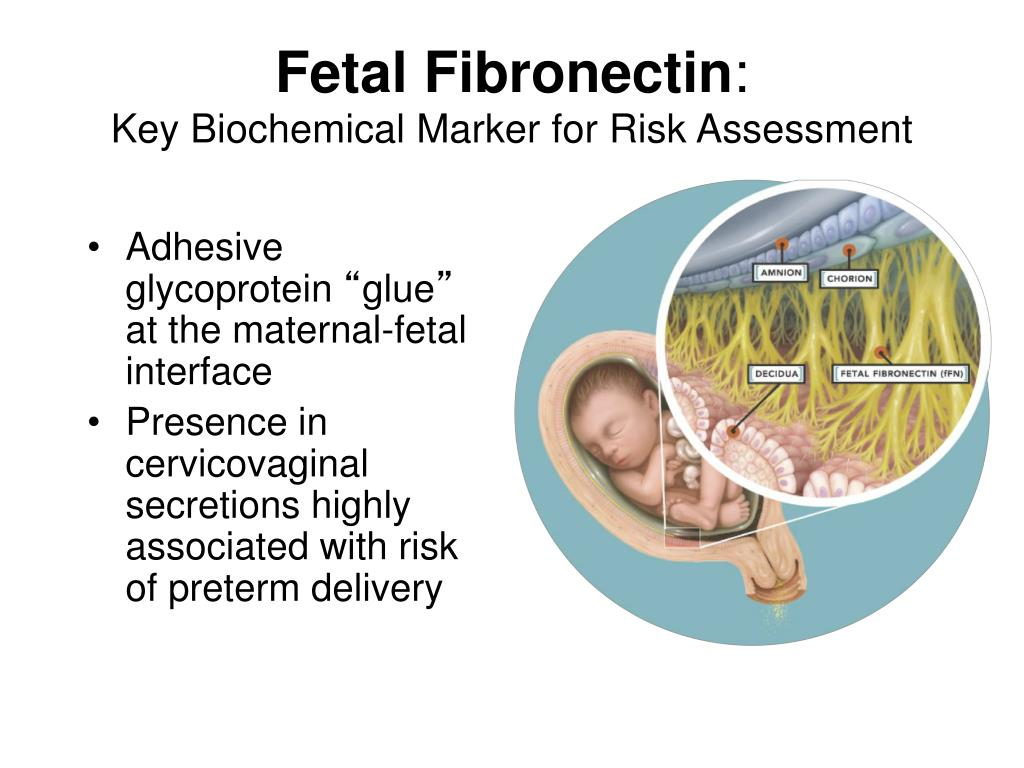
Fetal Fibronectin Test (fFN): looks for presence of the protein which acts like “glue” bw fetal membranes and uterine lining (vaginal swab)
NST
BPP/USN
How to manage preterm labor: (2)
Tocolysis (makes contractions go away and delay labor)
Cerclage (sew cervix shut)
What are the tocolytics used: (4)
terbutaline SubQ
give to stop contractions
oral nifedipine
relaxes smooth muscle ⬇contractions
mag sulfate IV
preeclampsia/neuroprotection
relaxes smooth muscle
betamethasone
lung maturity
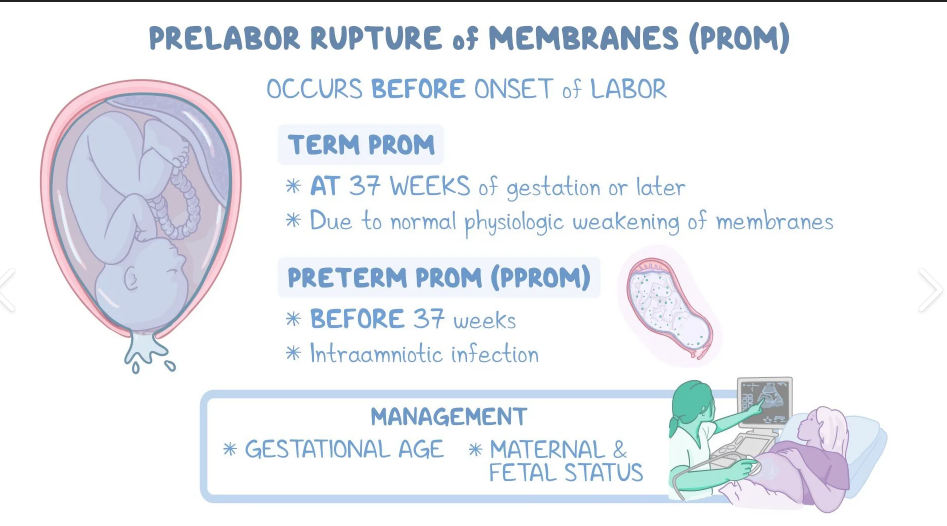
What is Prelabor/ Preterm rupture of membranes (PROM)
Prelabor-ROM: rupture of membrane b4 labor begins @ term (> 37 weeks)
PPROM: b4 labor and b4 37 weeks (< 37 weeks)
What should u monitor for when mom’s water breaks?
Sepsis!!
check temperature frequently!!
q1-2 hrs
FHR!!
PROM/PPROM diagnostic tests (4)
visual (color, odor, amt, time)
Fern test
Nitrazine test (turns blue)
Fetal Fibrinectin Test
Fetal fibronectin (fFN) is a protein that acts like a “glue” b/w fetal membrane and the uterine lining.
vaginal swab is taken
u want negative
Tx for PROM/PPROM (2)
tocolytics to make contractions go away
corticosteroids (speed up fetal lung maturity)
Terbutaline education: (7)
hold if mom HR >120 bpm
monitor signs of pulmonary edema
SOB
HA
palpitations/tachycardic
tremors
hyperglycemia
Mag Sulfate education: (4)
monitor for ⬇DTR
respiratory depression
oliguria
calcium gluconate antidote
Chorioamnionitis clinical manifestations: (4)
due to prolonged rupture of membrane
maternal fever > 100.4F x2, 30 mins apart
mom and baby tachycardia
uterine tenderness
foul smelling amniotic fluid
What is the difference between augmentation and induction of labor?
Induction:
starting labor ARTIFICIALLY b4 it begins (Pitocin or mechanical techniques)
Augmentation:
help labor progress AFTER it starts
What are the contraindications for using oxytocin (Pitocin) during labor? (5)
placenta previa
umbilical cord prolapse
prior cesarean
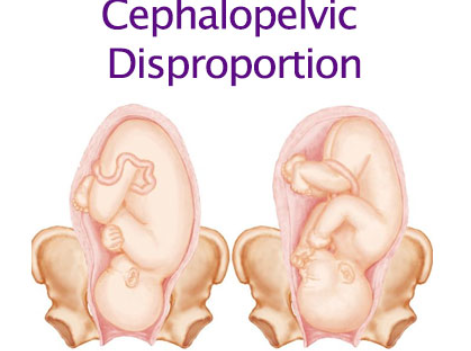
cephalopelvic disproportion(baby’s head too big to fit through pelvis)
fetal distress (breech)
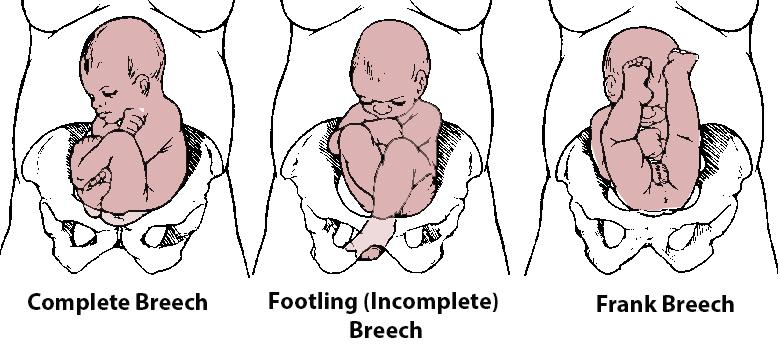
Types of breech presentations (3):
frank breech: butt first, legs up
complete breech: butt first, knees flexed
footling breech: one or both feet first
How do providers respond to non-reassuring fetal heart patterns? (5)
ex: late or prolonged decels, minimal or absent variability, bradycardia
Reposition LEFT side!!!
STOP oxytocin
give O2
IV fluids
emergent delivery if needed
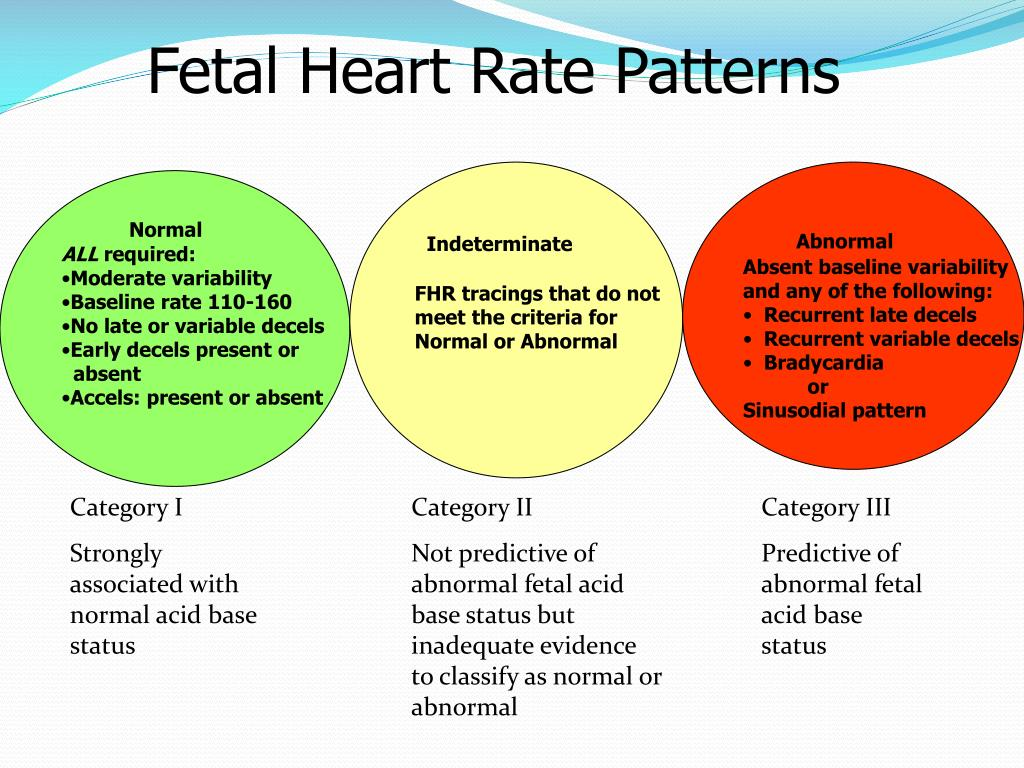
Category I-III FHR patterns:
baseline
variability?
decels?
I: good
baseline 110-160 bpm
moderate variability
no late or variable decels
has accelerations
II: needs monitoring
recurrent late/variable decels
minimal variability
prolonged decels
III: bad
absent variability w/ recurrent late decels
absent variability w/ recurrent variable decels
bradycardia
sinusoidal pattern!!!
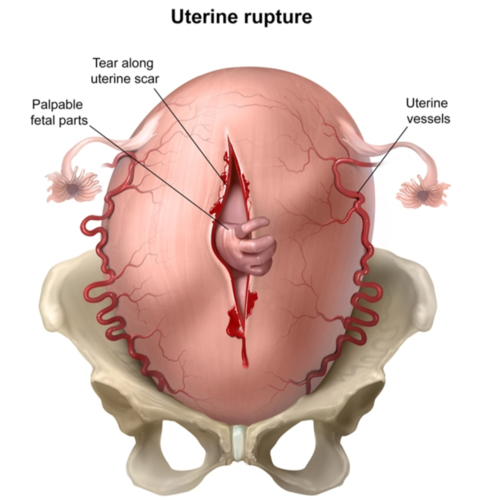
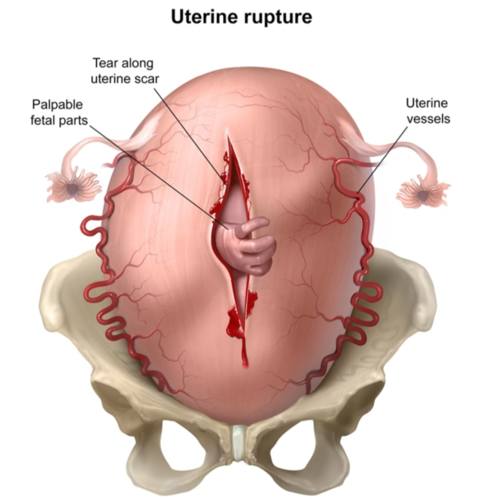
Describe the s/s of uterine rupture (5)
uterine atony (loss of contractions on palpation)
loss of fetal station
change in shape of uterus
referred shoulder/CP
abnormal contraction patterns
What factors contribute to these findings:
tachycardia
bradycardia
minimal variability
variable decels
early decels
late decels
tachycardia: mom has fever
bradycardia: cord compression
minimal variability: baby sleeping
variable decels: cord compression
early decels: head compression
late decels: placental insufficiency, fetal hypoxia
Hallmark Placental Abruption signs: (2)
painful, dark red bleeding (hypovolemia)
rigid/board-like abdomen
start tocolytics (stop contractions)
signs of uterine rupture: (4)
loss of uterine contractions on palpation/monitor (uterine atony)
loss of fetal station/ cant feel presenting part (where’d baby go?")
referred shoulder/CP
sudden change in shape of uterus
Emergent nursing actions for uterine rupture: (6)
move on left side
stop Pitocin
non rebreather @ 10L/min
2 #20 gauge IV lines
indwelling cath
prep for hysterectomy
emergent c-section

Explain prolapse cord and know the nursing responses: (5)
umbilical cord slips through cervix b4 baby
response:
lift presenting baby off cord w/ sterile hand (prevent kinks)
pt in knee to chest
Trendelenburg
stop Pitocin
emergent c-section

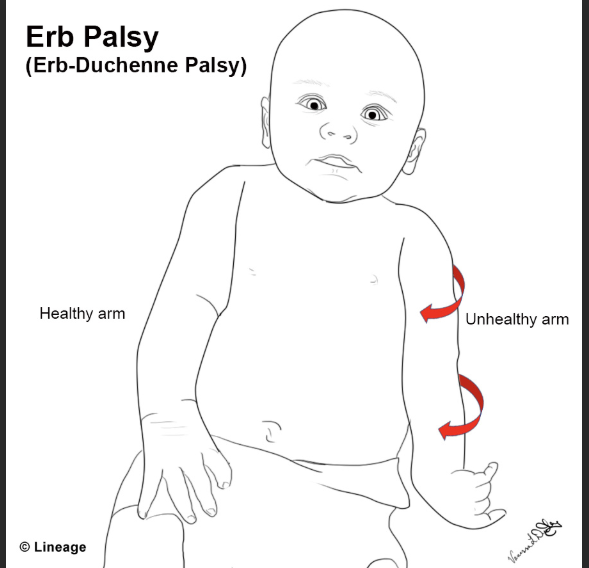
What is Shoulder Dystocia: (2)
complications: (3)
baby’s shoulder stuck behind moms pubic bone
“turtle sign”- head goes out, in, out…etc)
→ can cause
Erb Duchenne palsy (disabled arm)
uterine rupture
hemorrhage etc
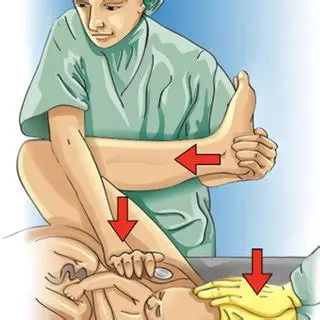
Tx shoulder dystocia: (6)
Apply suprapubic pressure (avoid fundus to attempt to free shoulder)
Mvmt of babys arm across head to dislodge shoulder
Pt on hands and knees
Prep for Episiotomy
McRoberts maneuver: push mom legs to chest
Rotate fetus manually
Define amniotic fluid embolism and s/s (3):
amniotic fluid enters moms bloodstream post birth → clotting
s/s:
sudden SOB
hypotension
altered LOC