Dr Clarke Essential Medicine - Rheumatology and Endocrinology
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Feature of inflammatory arthropathy (S/S)
Symptoms:
Early morning stiffness
Worse with rest, better with movement
Signs:
Soft tissue swelling eg loss of valleys between Knuckles
(Raised ESR,CRP)

Features or rheumatoid arthritis
Symmetrical, inflammatory arthritis
Small joints of hands and feet
Also hips, elbows and knees
Young adults, F>M
HLA DR4 associate

What is rheumatoid factor
IgM against your own IgG
Lots of normal people have it
Lots of people with classic rheumatoid do not have it
High titres associated with progressive disease
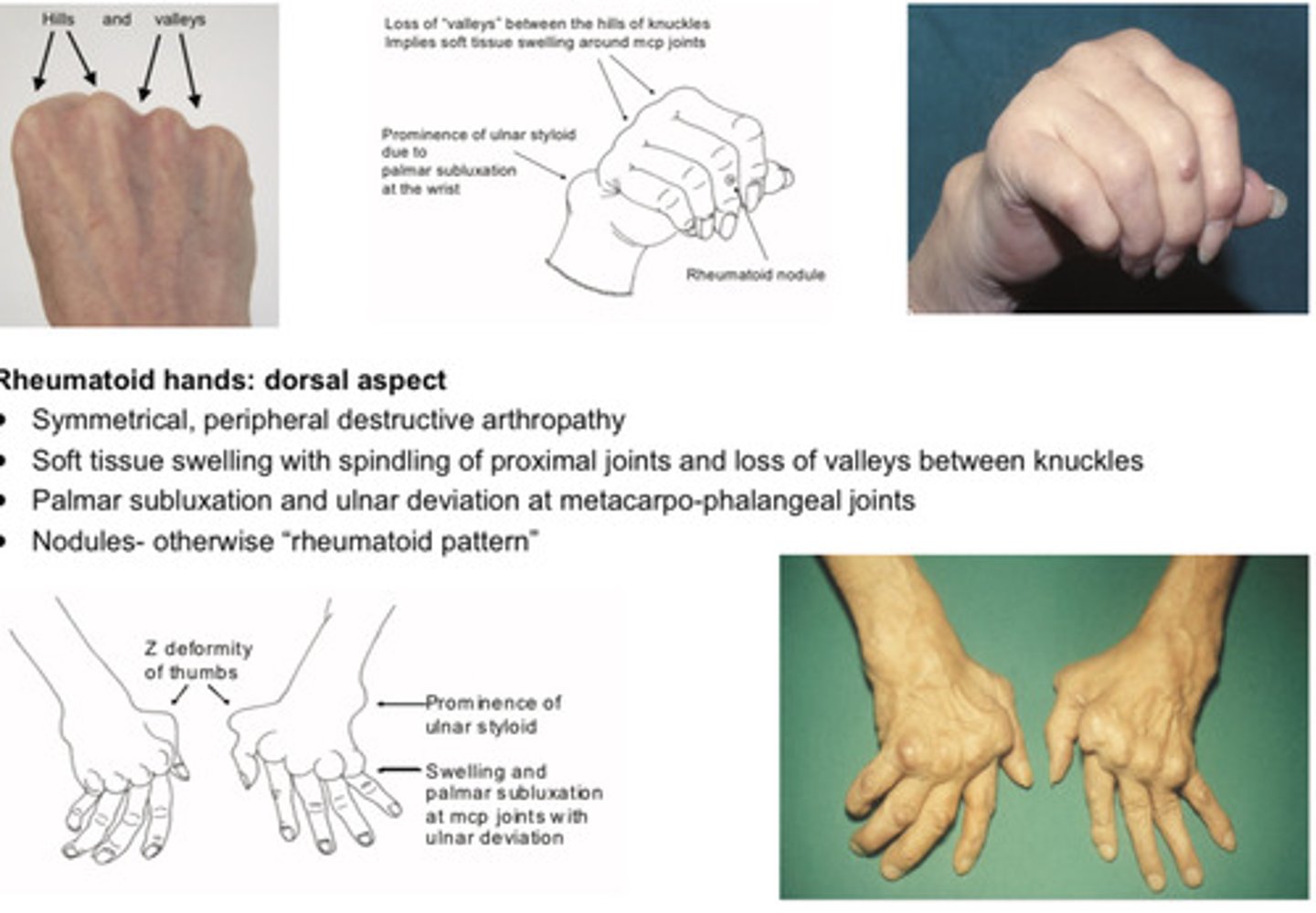
Features of the rheumatoid hands (dorsal aspect)
Symmetrical, peripheral destructive arthropathy
Soft tissue swelling with spindling of proximal joints and loss of valleys between knuckles
Palmar subluxation and ulnar deviation at metacarpo-phalangeal joints
Nodules- otherwise "rheumatoid pattern"
Features of rheumatoid hands (Palms)
Palmar erythema
Wasting of thenar eminence- carpal tunnel syndrome
Fixed flexion contracture
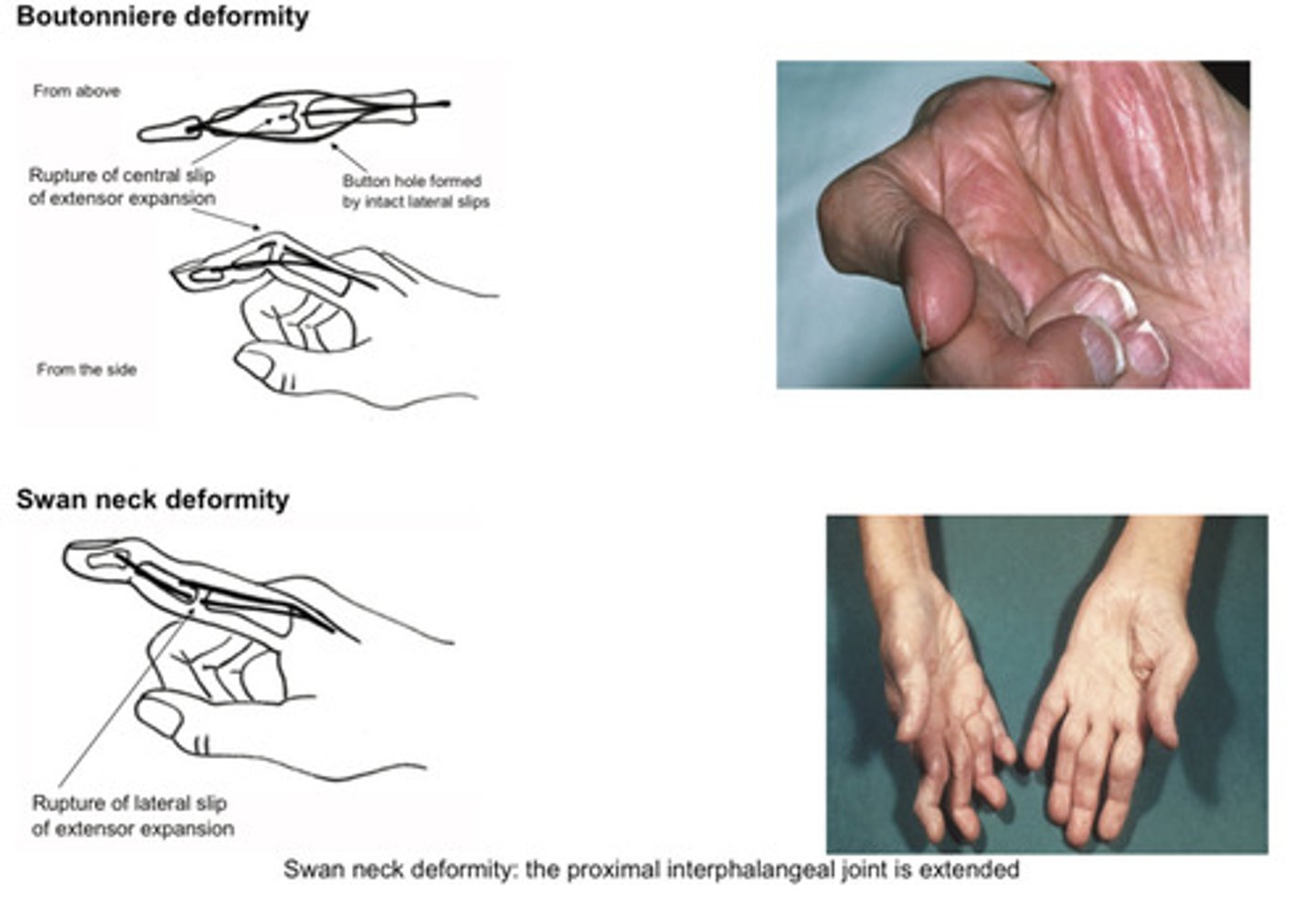
Specific abnormalities- swan neck, button hole, z thumb
Due to "rheumatoid tenosynovitis"
What causes Positive prayer sign in early inflammatory arthropathy
Rheumatoid tends synovitis

What is seronegative rheumatoid
One third of patients are seronegative
Identical disease presentation to seropositive in most respects, but unlikely to have nodules or extra-
articular features
Most have some non-classical rheumatoid factors (IgG vs IgG)
40% have antibodies to cyclic citrillinated peptide (CCP); if so, more likely to be rapidly progressive
Investigations for suspected rheumatoid arthritis
FBC, CRP
Renal and liver function tests (baseline)
Rheumatoid factor
Anti-CCP abs (if positive, more likely to be rapidly progressive)
X-ray hands and feet (if erosions present at baseline, more likely to be rapidly progressive)
Refer even if all these are negative
DMARDS
"Treat to target" strategy
• Start conventional DMARD asap
• Three first line drugs: methotrexate, leflunomide and sulfasalazine
• May need "bridging treatment" with steroids
• Target: remission or low disease activity
• Intensive monthly monitoring until achieved
• CRP and disease activity score (DAS 28) at each visit
• If not winning, escalate dose
• If still not winning after 6 months, step-up to dual DMARD
• If still not winning and high level of disease activity, offer biological
What are the first line DMARDs
Methotrexate
Leflunomide
Sulfasalazine
When is bridging treatment offer while using DMARDs
What are the bridging drugs
If severe
Bridge with steroids (DMARDs take about a month to work)
What is the target with DMARDs
Remission/ low disease activity
Intensive monthly monitoring until achieved
(CRP and disease activity scoring (DAS28) at each visit)
What to do if DMARDs not working sufficiently
Escalate dose
After 6 months still not sufficient: dual DMARD
Still not sufficient: biological
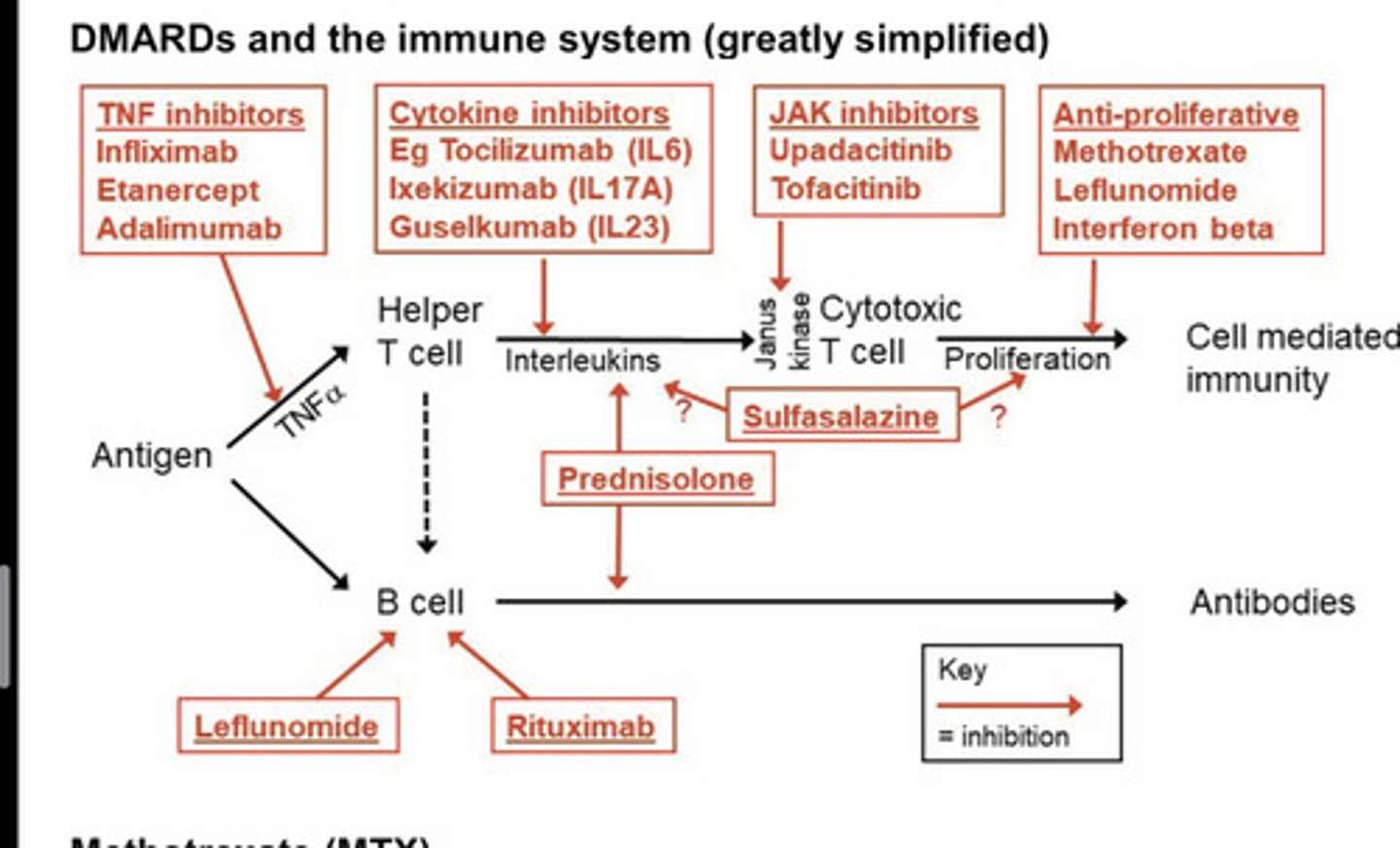
DMARDS and the immune system mind map
How does methotrexate work
Once weekly
Anti proliferative / anti folate
Examples of TNF inhibitors
Infliximab
What is given with methotrexate
Folate - to decrease hematological/GI and hepatic side effects (given on a non methotrexate day)
Complications of methotrexate
GI SEs
Bone marrow suppression
Liver and renal toxicity (rare)
Pneumonitis/pulmonary fibrosis (rare)
What drug is contraindicated with methotrexate
Trimethoprim (both anti folate drugs)
Excretion can be inhibited by NSAIDs
What bloods need to be checked prior to methotrexate
FBC
EGFR
LFT
What test need to be done prior to starting biological
Tuberculin skin test/ interferon gamma release assay
CXR
+/- Hep B/C and HIV
Treat latent tuberculosis
Warm patient that risk of serious infection (2% per annum)
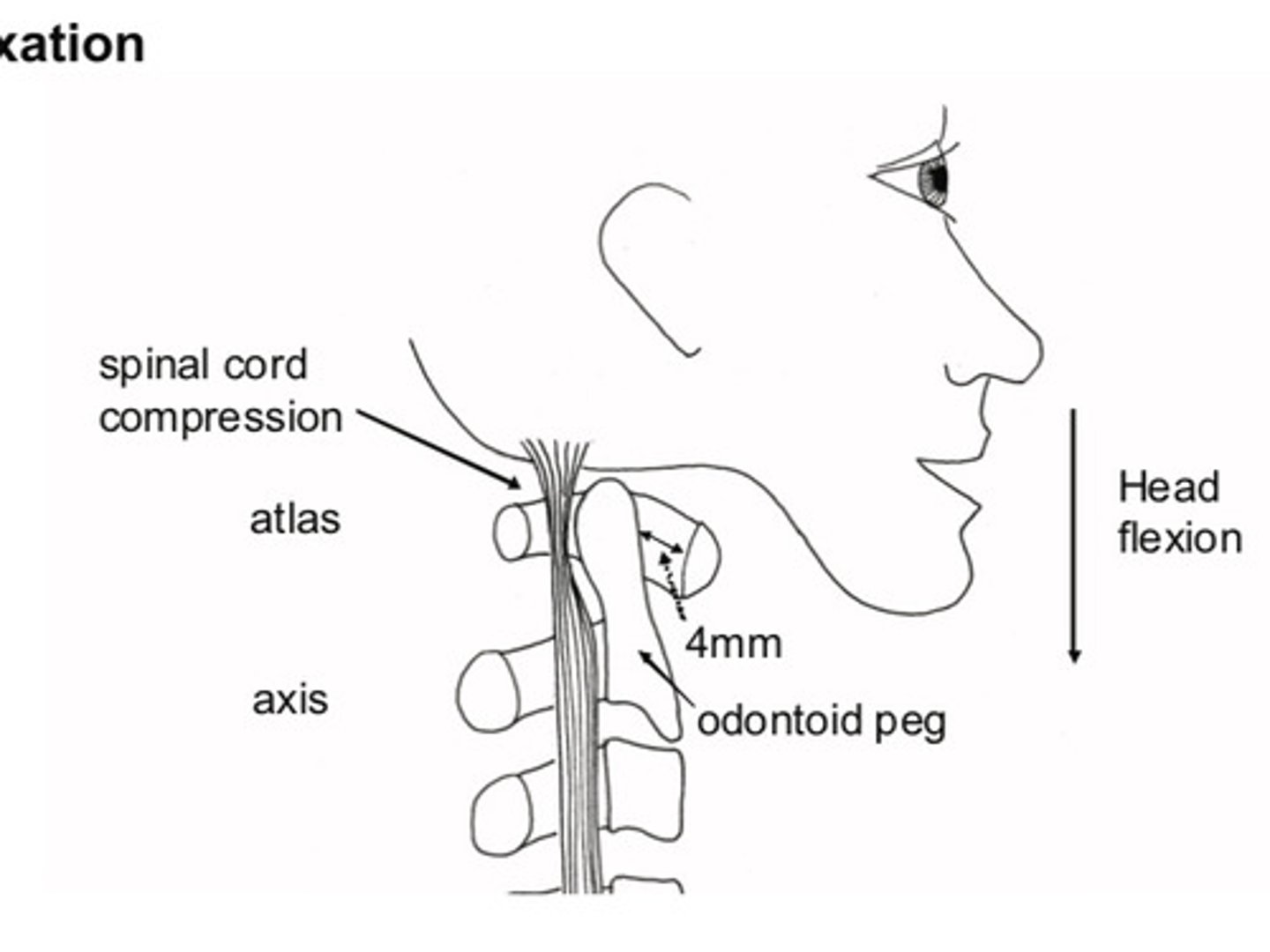
Atlantoaxial subluxation
Tendons at the top of the cervical spine can be weakened by rheumatoid tenosynovitis
If odontoid peg subluxation backwards over days or week = compress upper cervical cord = progressive spastic tetraparesis
Sudden = rapid output of inhibitory impulses down vagus +/- cardiac arrest
Differential diagnosis for rheumatoid hands
Rheumatoid arthritis
Psoriasis arthropathy
Systemic lupus
Osteoarthritis with inflammatory component
Types of psoriatic arthropathy
Oligo arthritis (70%)
Distal (15%)
Rheumatoid (15%)
Arthritis mutilans (telescoping; rare)
Sarcoiliitis (may be associated)
Treatment options for psoriatic arthropathy
Sulfasalazine
Methotrexate
TNF inhibitor (eg adalimumab)
Interleukin inhibitors (ixekizumab)
Janus kinase inhibitors (eg upadacitinib)
Radiographic changes in rheumatoid arthritis
SPADES
S - soft tissue swelling
P - peri articular osteoporosis
A - absent osteophytes
D - deformity
E - erosions
S - subluxation
Radiographic changes in osteoarthritis
LOSS
L - loss of joint space (cartilage thinning)
O - osteophytes
S - subchondral cysts
S - subchondral sclerosis
Extra articular manifestation of rheumatoid
FACEBOOKS
F - feltys syndrome
A - Atlantoaxial subluxation
C - Caplin syndrome and pulmonary nodules
E - effusions
B- blood (normochromic normocytic)
O - olecranon bursitis
O - oral dryness (sicca syndrome)
K - kidneys (amyloid, gold and penicillamine)
S - sensory neuropathy and scleromalacia
Feltys syndrome
RA, splenomegaly, neutropenia
Caplans syndrome
rheumatoid nodules in the lungs
Olecranon Bursitis
inflammation of the bursa located over the olecranon process of the elbow
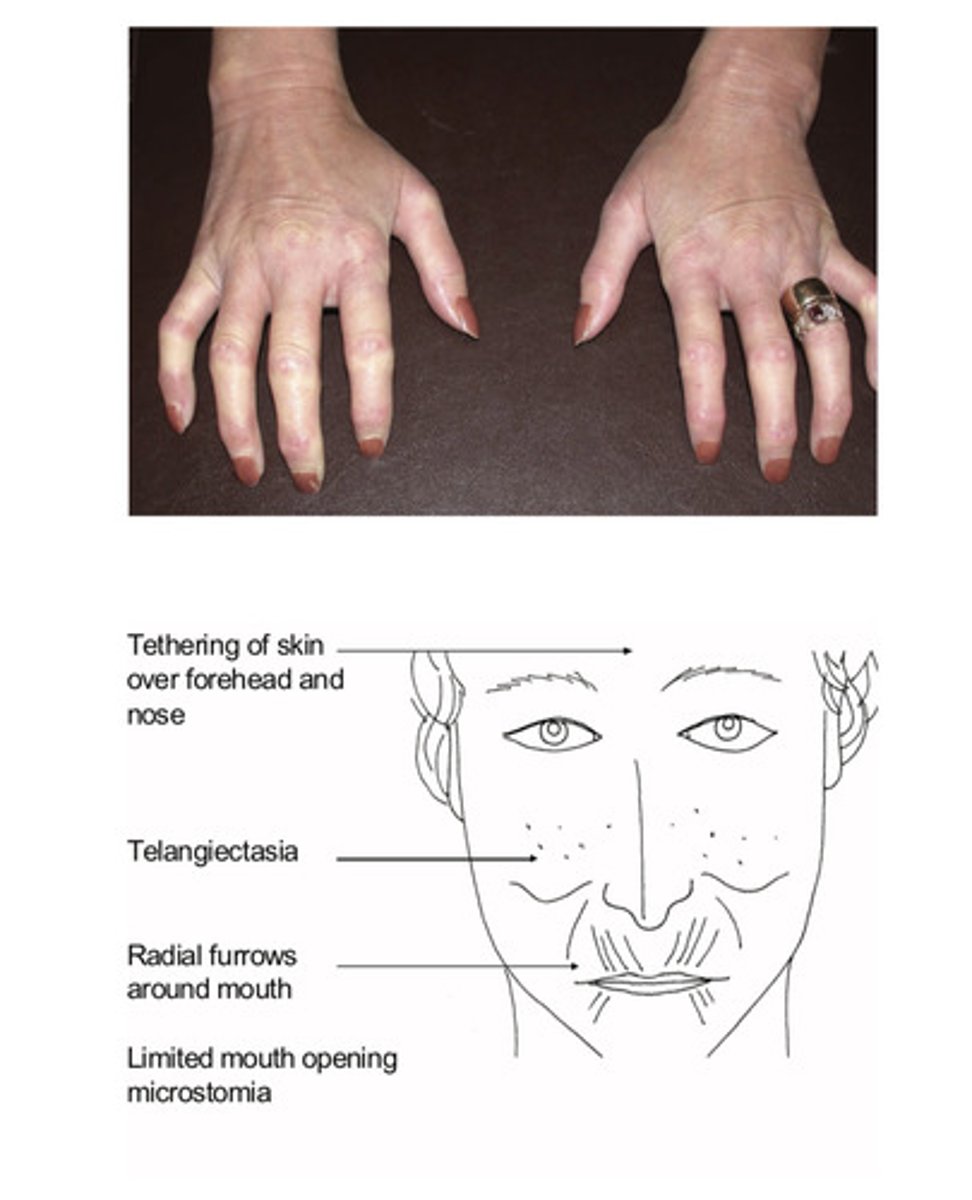
Features of scleroderma
Hands:
Sclerodactylty
Telangiectasia
Raynauds
Evidence ulceration (knuckles, finger tips)
Prayer test
Subcutaneous calcifications
Skin tethering:
Face , upper arms, chest (diffuse cutaneous scleroderma)
Telangiectasia
Mouth opening reduced; (microstomia)
Test with three finger test
Pathophysiology of vasculitis in scleroderma
Intimal vasculitis

Spectrum of systemic sclerosis
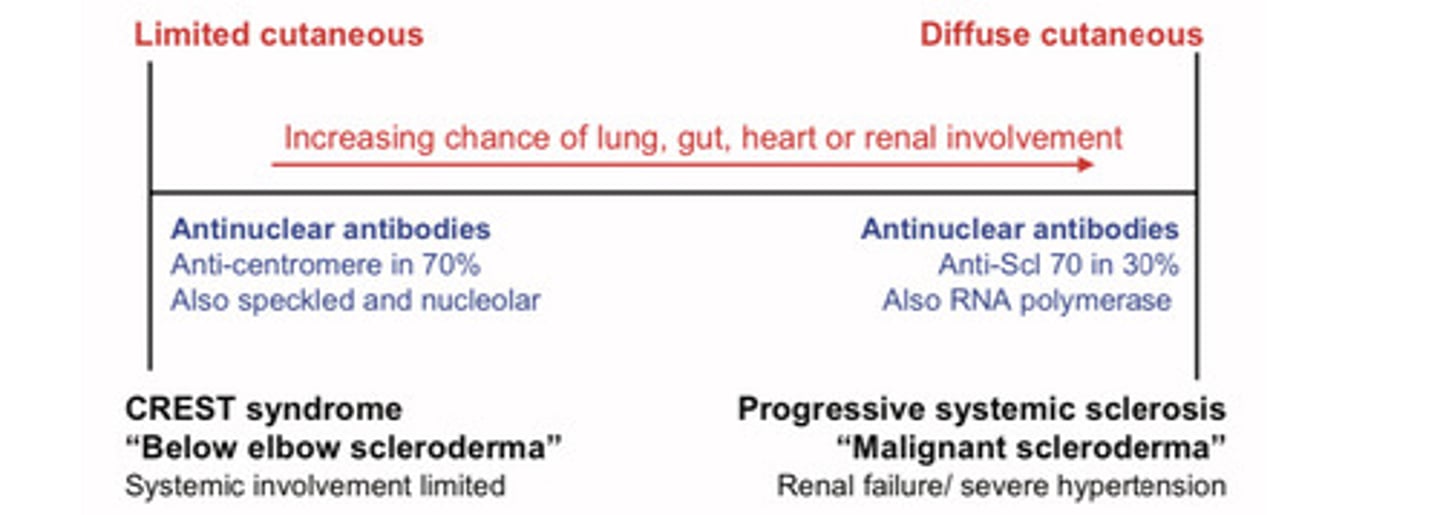
CREST syndrome
Calcinosis, Raynaud's, esophageal dysmotility, Sclerodactyly, Telangiectasia
Features of diffuse cutaneous scleroderma
More extensive with internal organ involvement
Mask like facies, wrinkled skin, microstomai
Tethering of skin over nose
Interstitial pulmonary fibrosis (restrictive ventilatory defect)
Renal involvement (hypertension, impaired renal function)
Atonic oesophagus (reflux and aspiration)
Three questions to ask in the patient with suspected scleroderma
Do you hands change colour in the cold (white, blue, red)
Do you get breathless? (Scleroderma affecting chest wall or interstitial fibrosis)
Do you get indigestion or heart burn
Scleroderma treatment
Digital ulcer: bosentan or IV prostanoids
Skin: methotrexate
GI: PPI
Renal crisis: ACE-I
Pulmonary hypertension: bosentan or sildenafil
Raynauds: nifedipine
Key points in rheumatology
Examine the hands means- examine the hands and the elbows and the ears
Common exam cases: rheumatoid arthritis and scleroderma
Don't forget to check hand function
Name the hormones which are insulin antagonists
Adrenaline
Glucagon
Cortisol
Growth hormone
(Ie when there is less insulin in the body, these hormones come into action)
Signs of hypoglycaemia
Low blood pressure
Tachycardia
Pale, cold, clammy
Seizures
Thodds paraesis
ABCD approach to unconscious patient with hypoglycaemia in hospital
Airway:
Guedel airway to prevent obstruction by tongue
Breathing:
give oxygen
Circulation:
check pulse and BP;
get IV access;
send bloods and check bedside glucose stick testing.
Glucose <4mmol/l;
Give IV glucose and then IM glucagon
Recheck glucose in 10 minutes. (IV glucose eg 200ml 10% dextrose over 15 minutes)
Disability:
check response eg response to voice, pain or unresponsive
D2:
don't ever forget glucose in an unconscious patient
Neuroglycopenia
deficiency of sugar that interferes with normal brain activity
<3mmol/l
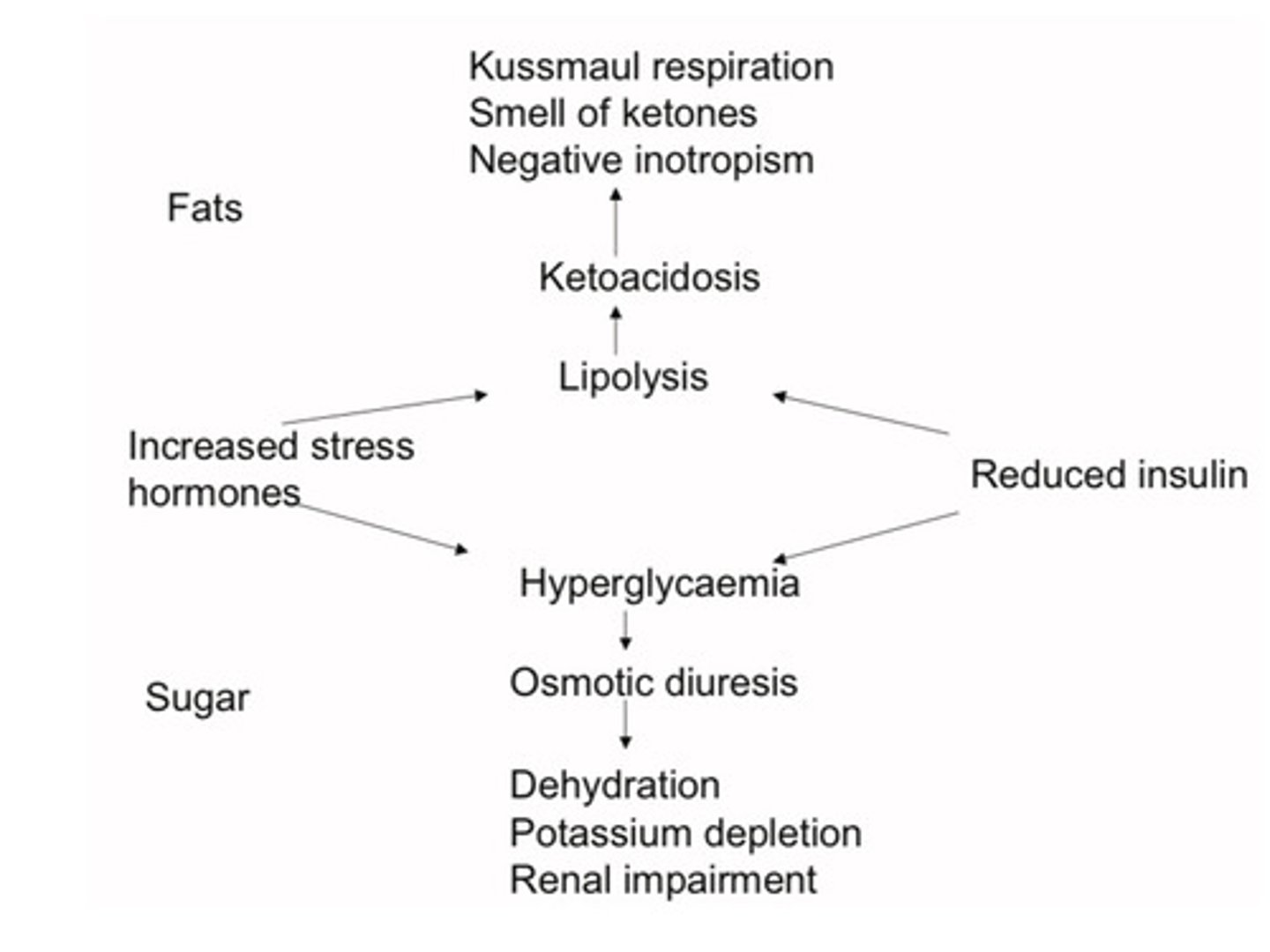
Ketoacidosis diagnostic triad
Hyperglycaemia (>11mmol/l or known diabetic)
Ketonuria (blood ketones >3mmol/l)
Acidosis (pH <7.3, or bicarbonate <15mmol/l)
Lower limit of normal for blood glucose
4mmol/l
(Four is floor)
Features of ketoacidosis
Dehydration (hypokaelamic):
Tachycardia and hypotension
Kussmaul respiration-acidosis
Sweet ketone smell
Vomit + abdominal pain
Signs of precipitating cause (eg infection, MI, etc)
Prinicples of treatment for diabetes.
Gastric aspiration
Rehydration
Insulin replacement
Potassium replacement
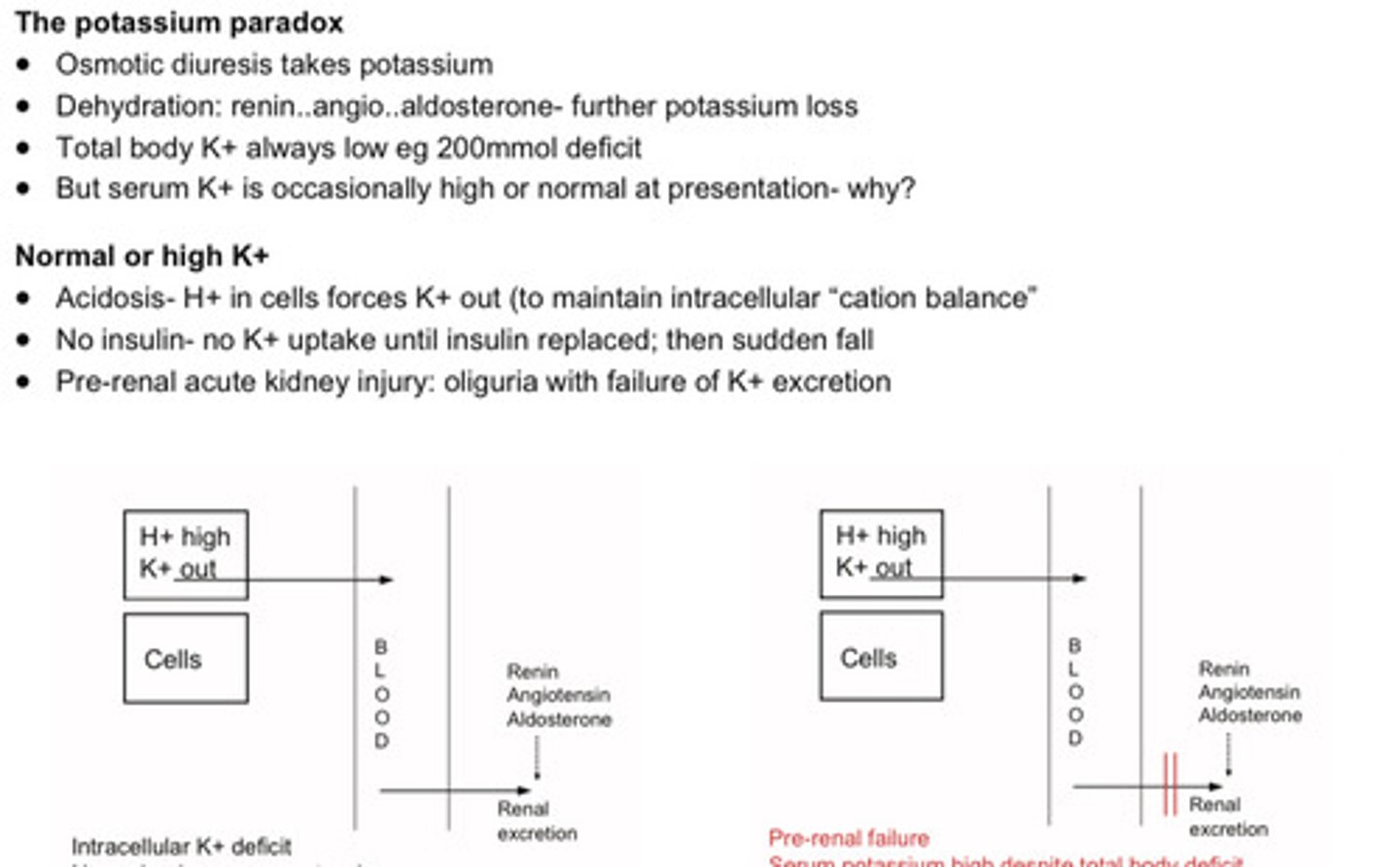
The potassium paradox in ketoacidosis
• Osmotic diuresis takes potassium
• Dehydration: renin..angio..aldosterone- further potassium loss
• Total body K+ always low eg 200mmol deficit
• But serum K+ is occasionally high or normal at presentation (serum potassium is high because there is a pre renal AKI = no excretion + anuria)
What should be done in the first hour in regards to ketoacidosis (PANICS)
P - Potassium- measure hourly: omit if anuria suspected or serum level >5.5mmol/l
A - Acidosis: check venous pH and ketone levels
N - "Normal saline": 500ml over 15 minutes if systolic <90mm; otherwise 1litre in first hour
I - Insulin by infusion (weight based, fixed rate, soluble insulin: 0.1 units/kg/hour)
C - Catheter and cultures; urine, blood etc
S - Stomach aspiration if drowsy; endotracheal tube first if no gag reflex
Examination of diabetic foot
Inspect- including heels
Palpate- capillary refill and pulses
Light touch- finger, cotton wool or monofilament
Avoid pin prick testing (risk of infection introduction)
Vibration sense
Ankle jerks
Buzz words "Loss of protective sensation"
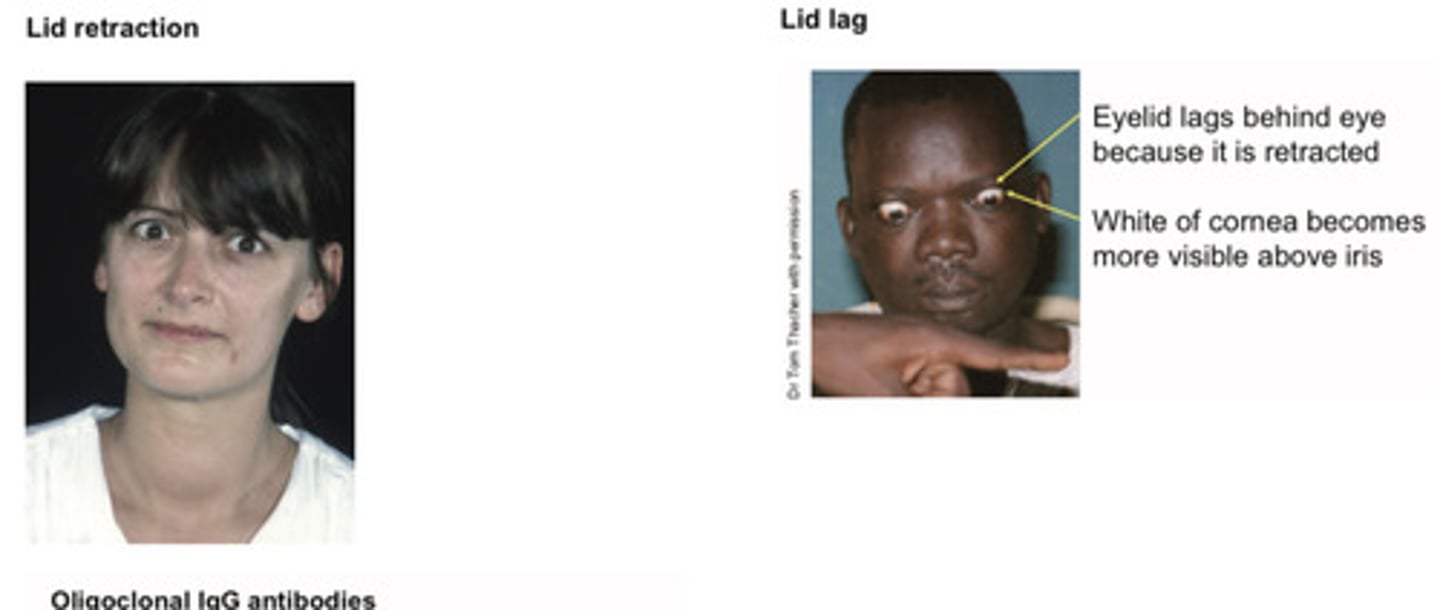
Triad for Graves' disease
Goitre
Eye signs (lid retraction + lid lag)
Thryotoxicosis
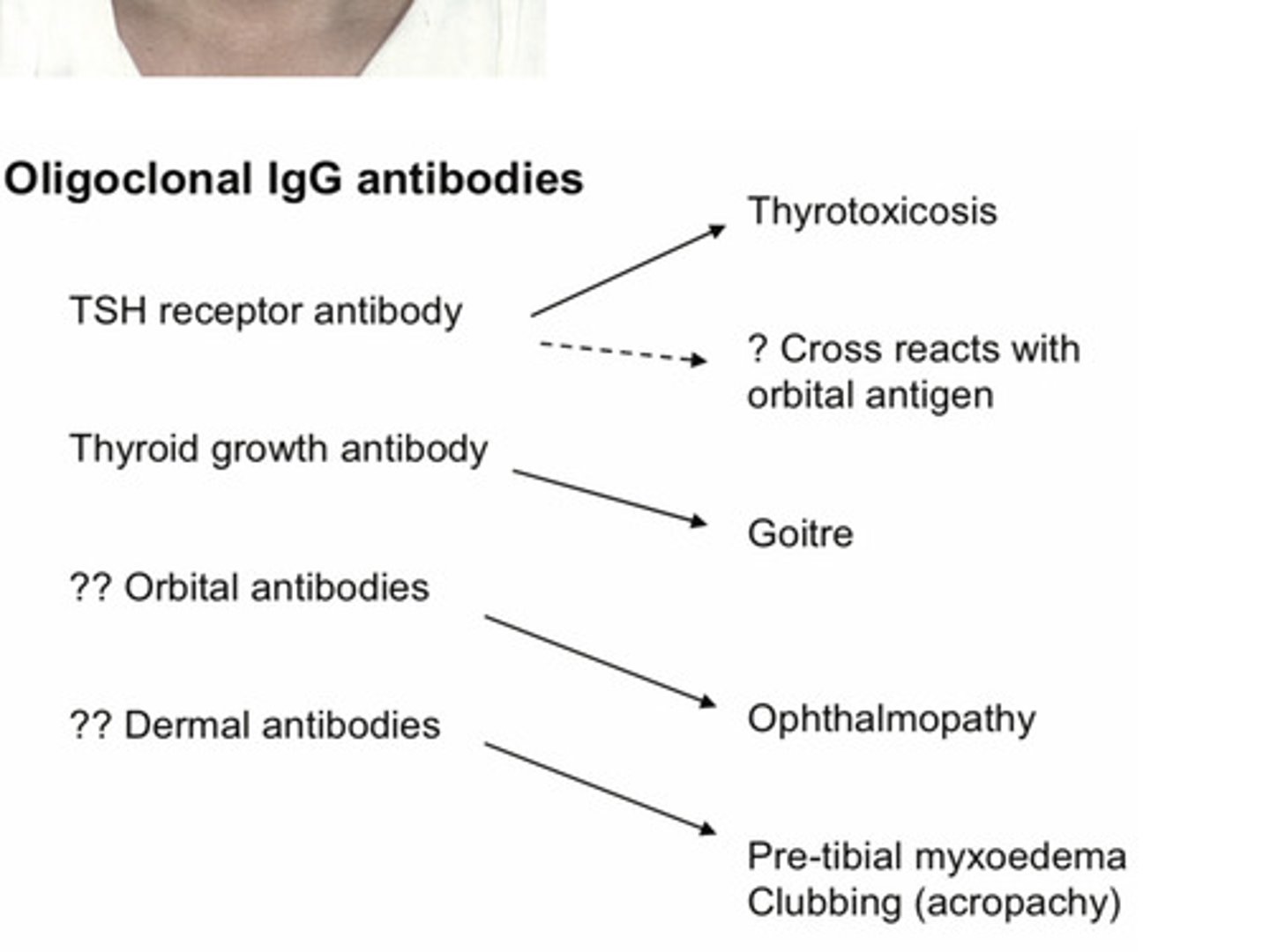
Oligoclonal IgG antibodies in Graves' disease
Peripheral thryoid signs
• Lid retraction and / or lid lag
• Clubbing and onycholysis
• Fine tremor, moist palms
• Tachycardia, atrial fibrillation
• Biceps reflex
• Slow relaxation- hypothyroid
• Proximal myopathy
• Pre-tibial myxoedema = Thyroid dermopathy (non-pitting)
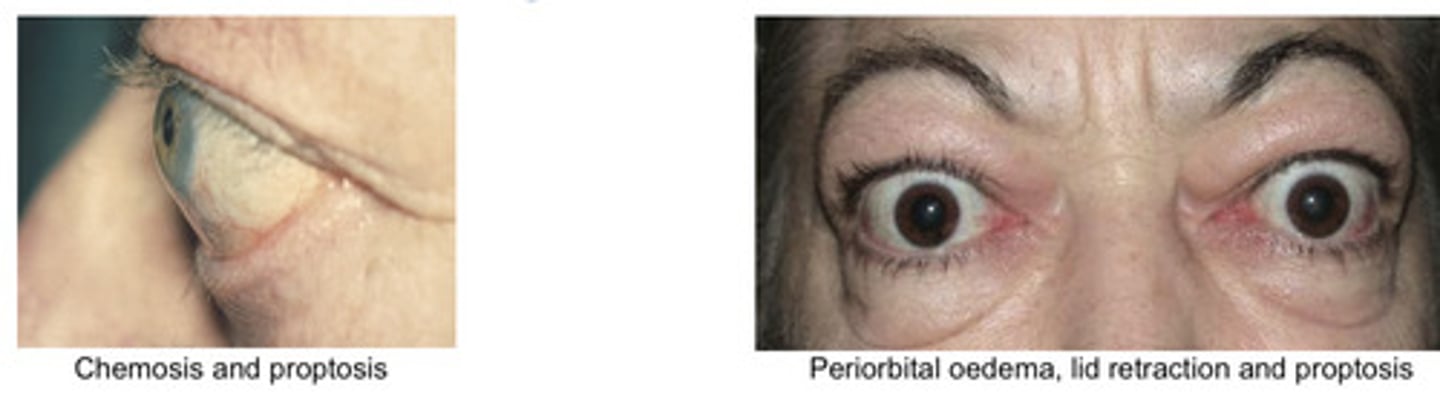
Graves eye disease features
Oedema (periorbital and chemosis)
Proptosis (best assessed from the side)
Retraction (autonomically mediated)
Exposure keratopathy
Ophthalmoplegia (upgaze palsy)
Graves' disease treatment options
Carbimazole low dose
Treat and block
Surgery
Radioiodine
Features of hypothryoidism
Gruff voice, slow cerebration
Coarse facial features
Dry cold scaly skin
Slow pulse and slow relaxation biceps jerk
May have goitre (Hashimoto's disease)
May have myxoedema (soft tissue swelling= oedema of the myxos)
Typical face of a person with hypothyroidism
Pale or yellow appearance "Peaches and cream" complexion Puffy face with periorbital oedema Dry,coarse hair
Diffuse hair loss
Loss of lateral eyebrow hair
(poor reliability)
Thickened dry flaking skin
Deep hoarse voice

Myxoedema in hypothryoidism
Severe hypothyroidism
with swelling of subcutaneous tissues
Typically around eyes and the backs of the hands
Often has a purplish tinge Tight rings
Tight rings

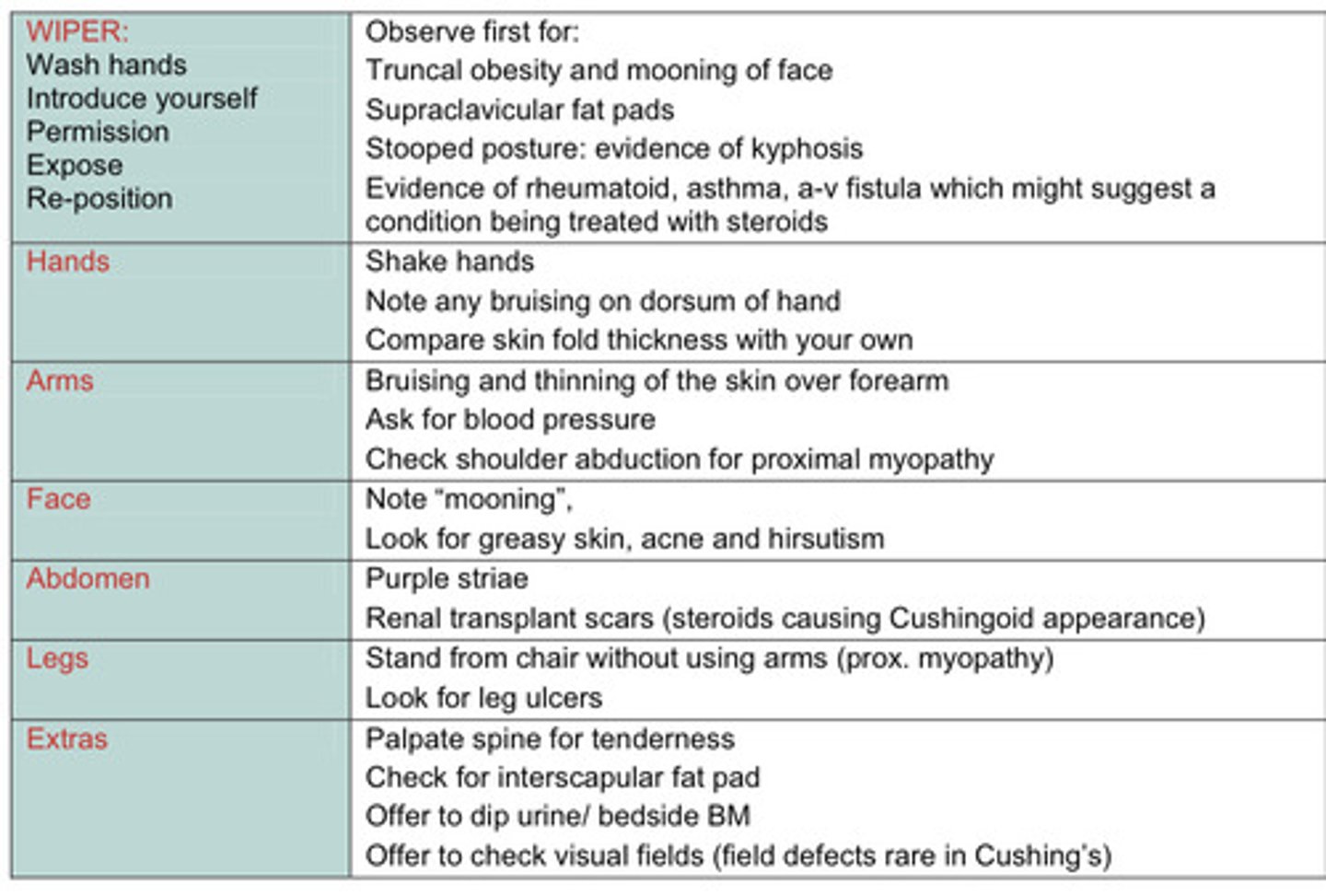
Cushing's syndrome features (catabolic, glucocorticoid and mineralocorticoid effects)
Catabolic:
Myopathy
Striae
Bruising
Osteoporosis
Glucocorticoid:
Diabetes
Obesity
Mineralocorticoid:
Hypertension
Hypokalaemia
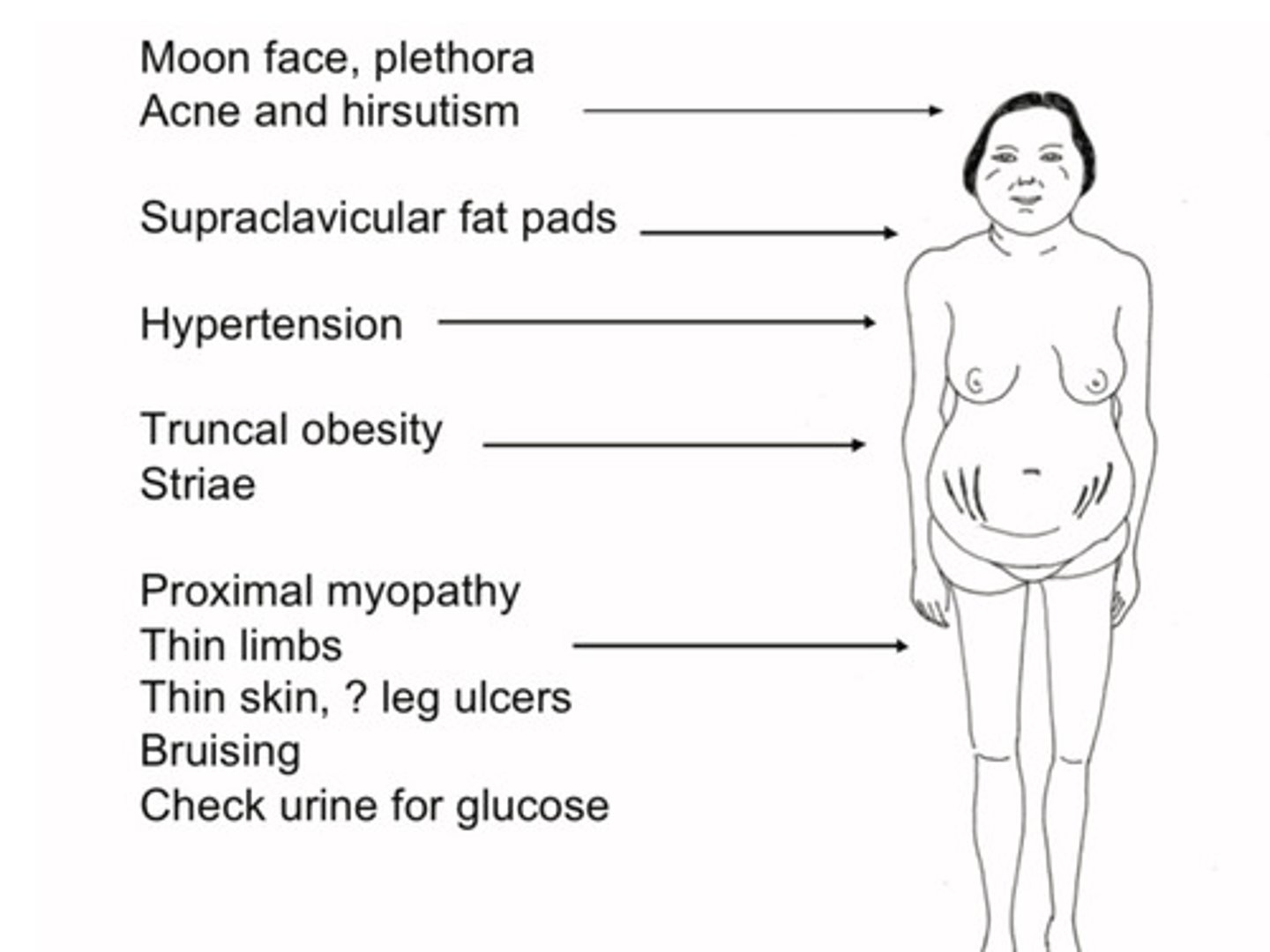
Examination schematic for cushings patient
SWEDISH Mnemonic
S - spinal tenderness
W - weight (central obesity)
E - easy bruising
D - diabetes
I - interscapular fat pad
S - striae
H - hypertension
Causes of Cushing syndrome
Iatrogenic Cushing (from corticosteroid therapy)
Adrenocortical adenoma (secretes excess cortisol)
ACTH-secreting pituitary adenoma
Paraneoplastic Cushing (due to ACTH secretion by tumors)
Investigations for hypercortisolaemia
24 hour urinary free cortisol
Loss of diurnal rhythm
Low dose dexamethasone test (no suppression of endogenous cortisol)
How differentiate adrenal from pituitary disease (cushings)
ACTH levels high in pituitary (cushings)
ACTH level low in adrenal (cushings)
(ACTH assay is tricky though and high dose dexamethasone test is to have poor reliability)
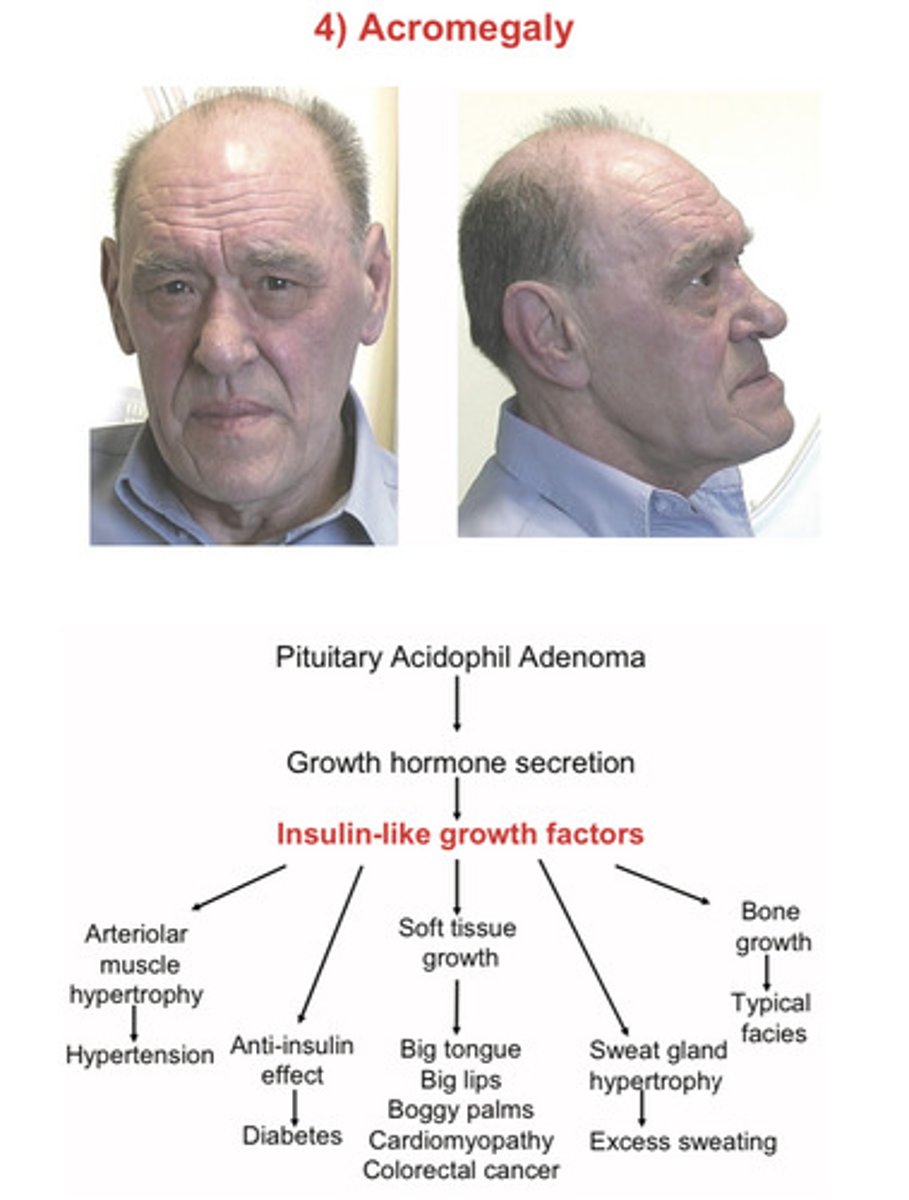
Acromegaly
enlargement of the extremities
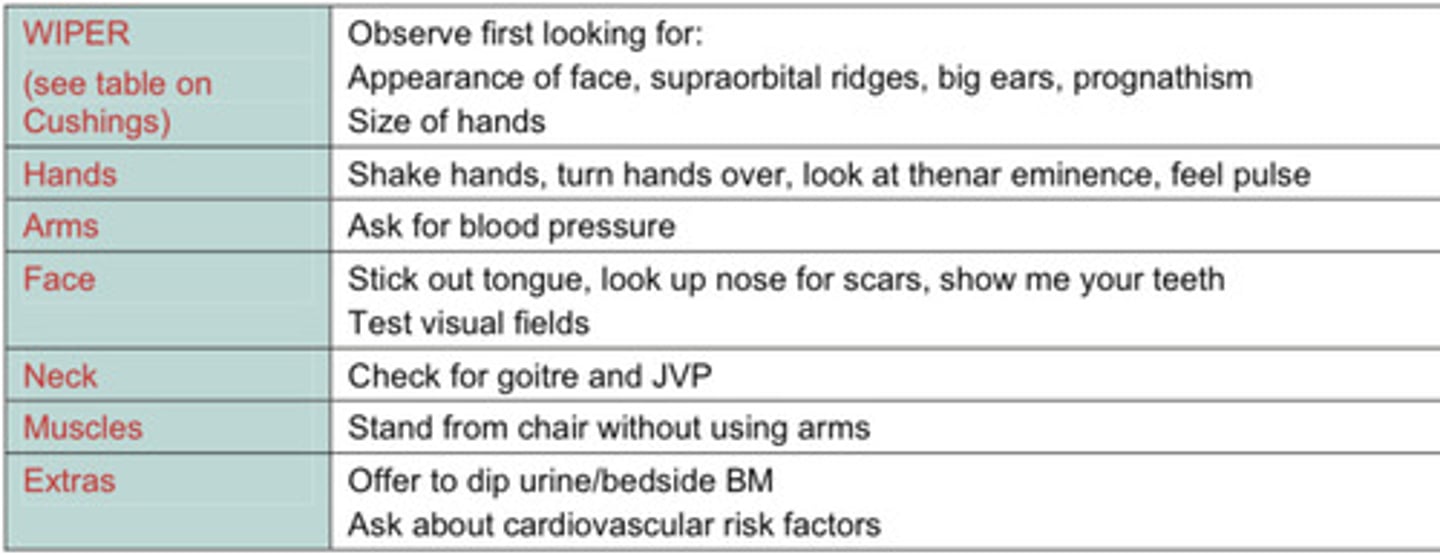
Hand features of acromegaly
Increase size
Thenar eminence: wasting if carpal tunnel syndrome
Check sensation in median distribution
Hyperhydrosis (palms)
Bogginess of palms
Skin fold thickness increased in active disease
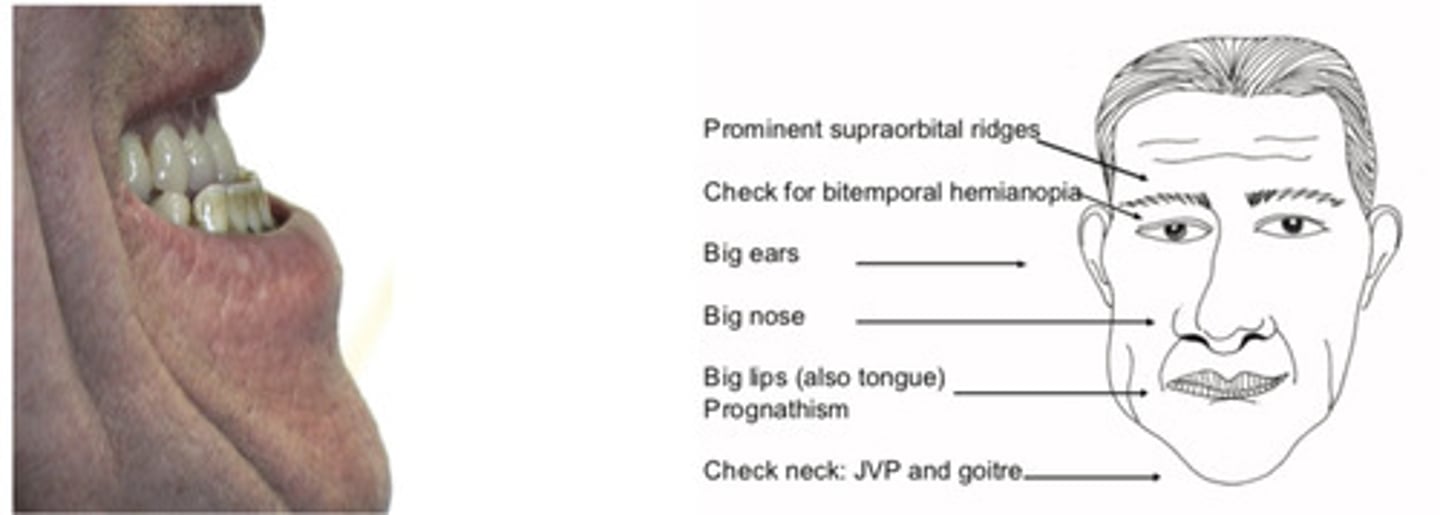
Facial features of acromegaly
Prominent supraorbital ridges,
Big ears, nose and lips
Macroglossia
Prognathism (from the size) (pro- gnathism= translates as "forward gnashers" ie protrusion of jaw due to overgrowth of the mandible; also leads to wide separation of the teeth)
Ask patient "Show me your gums" to demonstrate wide separation of teeth and that lower jaw teeth are in front of upper teeth (reversal of normal)
Mnemonic for acromegaly
Boggy sweaty ABCDEF
Boggy sweat = active
A - arthropathy
B - BP
C- carpal tunnel
D - diabetes
E - englahred tongue, heart, thyroid
F - field (bitemporal hemianopia)
How is acromegaly confirmed
Insulin like growth factor levels
Failure of suppression of GH levels during oral glucose tolerance test
(GH is an insulin antagonist and is normally suppressed by glucose)
Average hourly growth hormone levels
Examination schematic for acromegaly
Rx for acromegaly
Surgery
Radiotherapy
Medical treatment( in prep for surgery)
What screening test is NB in acromegaly
Colonoscopy from age 40