Pharm E3- Urology
1/114
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
115 Terms
How does the blood flow in an erection?
Increased arterial flow IN & decreased venous flow OUT
What is testosterone converted into?
DHT by 5a reductase
Estradiol by aromatase
What antidepressants can cause ED (in order of most likely to and least like to)?
TCAs > SSRIs > SNRIs > bupropion
What anticholinergics can cause ED?
Antihistamines (can use 2nd gen), antiparkinsonian agents, TCAs, phenothiazines
How can dopamine antagonists (phenothiazine & metoclopramide) cause ED?
Dopamine blockade increases prolactin levels → decreases testosterone production
What drugs can cause ED by suppressing testosterone mediated libido stimulation?
Estrogens, anti androgens, digoxin, spironolactone, ketoconazole, cimetidine
What CNS depressants can cause ED by suppressing perception of psychogenic stimuli?
Benzodiazepines, opiates, large doses of ethanol, anticonvulsants
What agents can cause ED by decreasing penile flow which reduces arteriolar flow to corpora?
Diuretics, BBs, central sympatholytics (methyldopa, clonidine)
What antihypertensive agents are less likely to cause ED?
ACEi, ARBs, CCBs
What other miscellaneous drugs can cause ED?
Finasteride, dutasteride, lithium carbonate, MAOIs, gemfibrozil
ED treatment algorithm
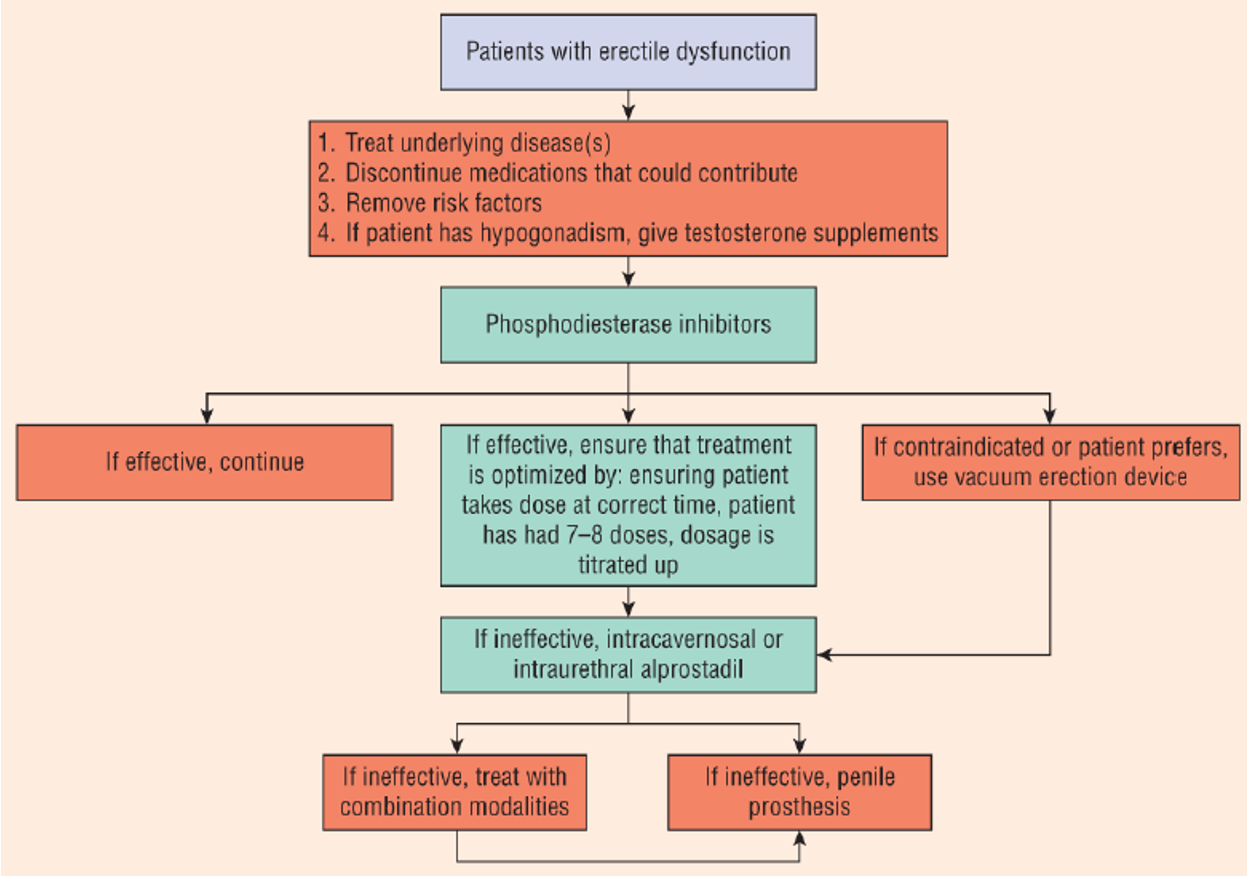
How do vacuum erection devices work to treat ED?
Pump generates negative vacuum pressure to draw arterial blood into cavernosa
*onsets 3-20 minutes
In what ED patients would it be good to use a vacuum erection device?
Can’t use PDE-5i or other oral agents
can be used in combo or before surgery; effective but not discreet
How do phosphodiesterase inhibitors (PDEi) work to treat ED?
inhibits metabolism of cGMP → increases cGMP → less Ca gets into cells → more vasodilation → produces erection
What metabolizes cGMP into GMP (inactive) & inhibits erections?
Phosphodiesterase (PDE)
What drugs are phosphodiesterase inhibitors (PDEi)?
Sildenafil (Viagra)
Vardenafil (Levitra/Staxyn)
Tadalafil (Cialis)
Avanafil (Stendra)
Which PDEIs inhibit PDE-6 (in rods & cones of eye)?
*test Q
Sildenafil
Which PDEI inhibits PDE-11 (striated muscle)?
*test Q
Tadalafil
Which PDEI’s have a delayed onset if taken within 2 hours of a fatty meals if taken w/in 2 hours (pt needs to take earlier)?
** test Q
Sildenafil & Vardenafil
Which PDEI has a slower onset but the longest duration of 24-36 hours?
** test Q
Tadalafil
What is first line for ED, especially in younger patients?
PDE inhibitors
What is likely to cause a failure of PDEIs when using for ED?
*try atleast 5-8 doses
Comorbid conditions (DM, PVD, etc), excess alcohol, food interactions
In what patients should PDEIs be avoided due to risk of priapism?
Healthy patients (no issues with erections), sick cell, leukemia, multiple myeloma, currently taking other ED meds
Which PDEIs are more likely to have to have ocular symptoms (blurred vision, cyanosis)?
Sildenafil > vardenafil = avanafil > tadalafil
Which PDEI is most likely to cause myalgias?
Tadalafil
How are PDEIs metabolized?
CYP3A4
*sildenafil & tadalafil need renal adjustment
What SEs are seen with PDEIs?
Vasodilation → HA, facial flushing, dyspepsia, nasal congestion, dizziness
8-10 mmHg drop in SBP (avoid if on multiple antihypertensives, nitrates & high risk cardiac patients)
The following SE is caused by what drug?
nonarteritic anterior ischemic optic neuropathy (NAION)
drop in blood flow to optic nerve → sudden U/L painless blindness
emergency! → irreversible
Sildenafil
What reversible ocular SEs are seen with sildenafil?
Photophobia, blurred vision, loss of blue green color discrimination
Which PDEI is more likely to cause QTc prolongation?
Vardenafil
How should the dose of PDEI be adjusted if a patient is also taking a CYP3A4 inhibitor?
Decrease dose
Why are nitrates CI in a patient who took a PDEI?
Severe hypotension from too much cGMP
*treat w/ trendelenburg position & fluids
How long must a patient wait to take a nitrate after taking a PEDI?
24 hours (48 hours for tadalafil)
What drug is a synthetic prostaglandin E1 used to treat ED by intracavernosal injection or intraurethral insert?
Alprostadil
What ED medication is good for patients with an impaired nitric oxide pathway (DM, prostatectomy, failed PDEI tx)?
Alprostadil
How does alprostadil work to treat ED?
Stimulates adenyl cyclase → increased cAMP production → dec intracellular Ca → smooth muscle relaxation → erection
*not nitric oxide dependent
Which is alprostadil preferred in ED over other vasodilator intracavernosal agents (papaverine, phentolamine, atropine)?
Less risk of prolonged erections & priapism
How should alprostadil be administered?
5-10 min before intercourse → T ½ of 1 minute
Duration < 1 hr (12-44 minutes)
Inject into 1 cavernous w/ aseptic technique
Why might alprostadil be a a better option for ED in high risk cardiac patients?
Less systemic absorption → less SEs
Would psychogenic ED or vasculogenic ED respond to lower doses of alprostadil?
Psychogenic ED
What SEs are seen with intracavernosal alprostadil?
Local burning/dull pain, injection site infection, cavernosal plaques or fibrotic areas (switch injection site around), priapism (rare)
What are SEs of alprostadil intraurethral suppository?
Urethral damage, stricture, difficulty voiding, fibrosis
*less bioavailability than intracavernosal
What is the MC adverse effect of penile prostheses / implant (malleable or inflatable)?
Post op infection
What are treatment options for BPH?
Watchful waiting, alpha 1 antagonists, 5a reductase inhibitors, PDEIs, anticholinergic, surgery
What stimulates the epithelial (glandular) tissue of the prostate?
Androgens (DHT)
What stimulates the stromal (smooth muscle) tissue of the prostate?
a1 adrenergic receptors (NE, estrogen)
Static or dynamic factors of BPH?
size → prostatic enlargement physically blocks bladder neck & obstructs urinary flow
slower changes
can be caused by
androgen stimulation on epithelial tissue
estrogen stimulation on stromal tissue
Static
Static or dynamic factors of BPH?
squeeze → excessive a-adrenergic tone on stromal tissue, bladder neck & posterior urethra
prostate can be normal in size
faster changes
can be triggered under stress or pain
Dynamic
What medications can worsen symptoms of BPH?
Testosterone replacement → inc DHT, more prostate growth
Adrenergic agonists (pseudoephedrine, ephedrine, phenylephrine) → activates stromal tissue
Anticholinergics (antihistamines, phenothiazines, TCAs) → dec detrusor muscle contraction, inc urinary retention
A patient with a history of BPH recently had a cold and took OTC pseudoephedrine. What symptom would you expect them to experience?
*example from lecture
Difficulty voiding bc pseudoephedrine is an adrenergic agonist & stimulates stromal tissue, causing constriction
BPH treatment algorithm
test questions!!!
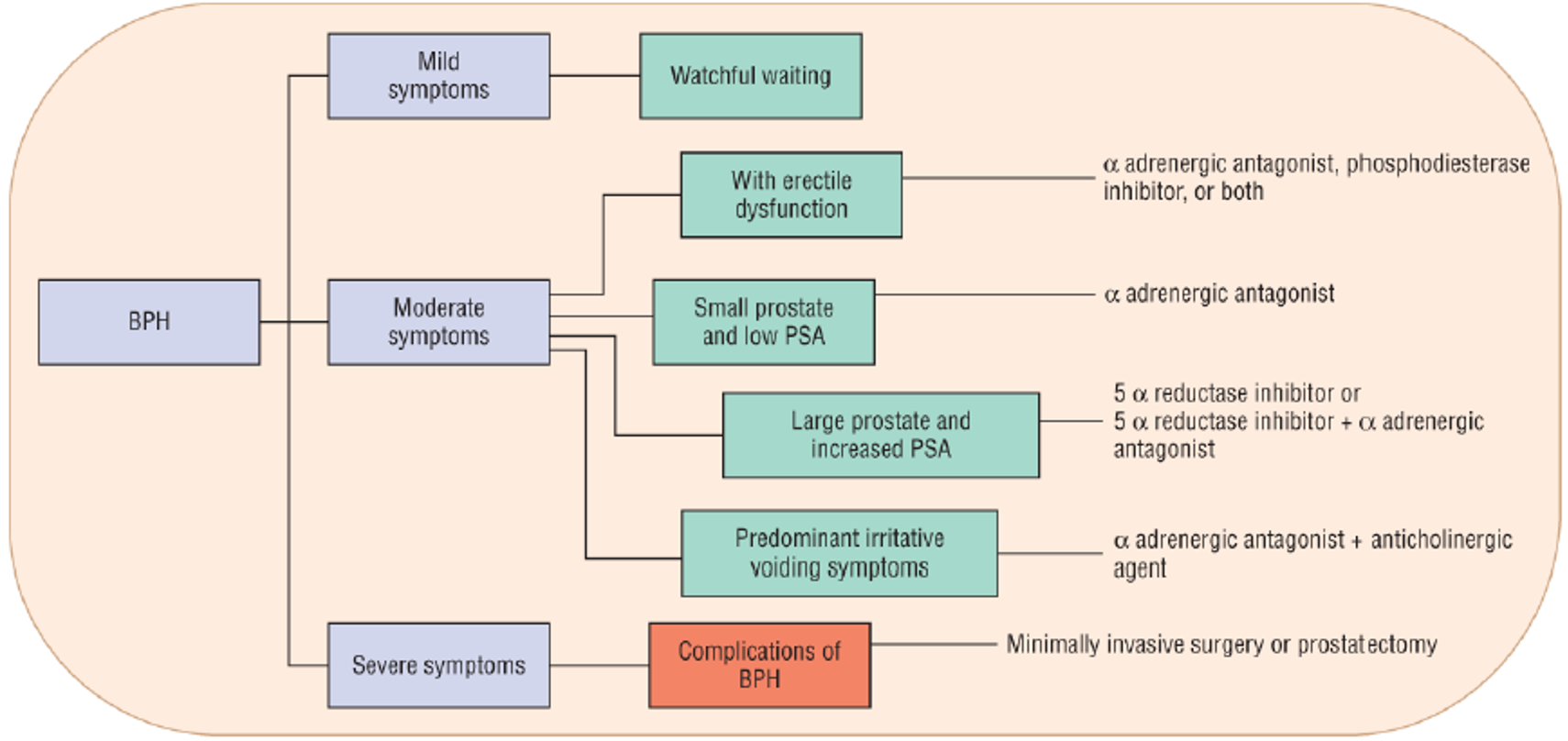
A patient with an enlarged prostate (BPH) and history of ED comes in to the office. What medication do you start them on?
**test Q
PDEI and/or a adrenergic antagonist
A patient with BPH has an enlarged prostate and increased PSA. What medication do you start them on?
**test Q
5 a reductase inhibitor +/- a adrenergic antagonist
A patient with BPH has a small prostate and low PSA. What medication do you start them on?
**test Q
a adrenergic antagonist
A patient with BPH has predominant irritative voiding symptoms (frequency, urgency, bedwetting, nocturia). What medication do you start them on?
**test Q
a adrenergic antagonist + anticholinergic
The following sx are seen in what condition?
Obstructive: bladder outlet obstruction, dec flow rate, incomplete & slow bladder emptying, hesitancy, bladder overdistension
Irritative: bladder hypertrophy & hypersensitivity, urinary frequency, urgency, bedwetting, nocturia
Lower urinary tract sx (LUTS): neurogenic bladder, UTI
BPH
What are the pharmacologic treatment options for BPH?
Dynamic sx → a1 blockers to relax smooth muscle
Static sx → 5 a reductase to inhibitors to dec testosterone stimulation, shrink prostate
irritative sx → antimuscarinics to relax detrusor
What meds are generally first line for BPH because they are rapid acting and have fewer SEs?
a1 antagonists
What meds are preferred for BPH in CV patients or significantly enlarged prostates?
5a reductase inhibitors
What must you ensure a BPH patient does not have before prescribing anticholinergics?
High post void residual (relaxes bladder & increases urinary retention)
What drug is a first generation a1 adrenergic antagonist that is generally avoided in BPH treatment due to tachycardia & arrhythmia SEs?
Phenoxybenzamine
Which generation of alpha 1 adrenergic antagonists are better for BPH because they are euro-selective for blocking a1A receptors (less SEs)?
Third generation
Do a1 adrenergic antagonists affect prostate size?
No
What drugs are second generation a1 adrenergic antagonists?
Prazosin (Minipress)
Terazosin (Hytrin)
Doxazosin (Cardura)
Alfuzosin (UroXatral)
What are the main SEs of second gen a1 blockers?
First dose syncope, orthostatic hypotension, dizziness
(dose at nighttime to avoid)
Which 2nd gen a1 blocker is the shortest acting, requires BID-TID dosing, & has the most significant CV effects?
Prazosin
Which 2nd gen a1 blockers are the longest acting & have lower average serum concentrations?
Doxazosin & alfuzosin
Which 2nd gen a1 blocker has the lowest risk of systemic SEs and does not require dose titration?
Alfuzosin
What drugs are 3rd generation a1 adrenergic antagonists?
Tamsulosin (Flomax)
Silodosin (Rapaflo)
Which 3rd gen a1 blocker is used most often, needs to be taken on an empty stomach, & should be avoided in a sulfa allergy?
Tamsulosin
What SEs are seen with 3rd gen a1 blockers?
Flu like sx, nasal congestion, inability to ejaculate
*no orthostasis/dizziness
What is the safest combo of PDEIs & a1 blockers to use in BPH?
*least likely to cause cause synergistic drops in BP
Tadalafil & tamsulosin
What drugs are 5a reductase inhibitors?
Finasteride (Proscar) - type II inhibitor
Dutasteride (Avodart) - non selective
What drug for BPH is good for patients who cannot tolerate a1 blockers and ma reduce the prevalence of prostate cancer over time?
5a reductase inhibitors
What should be used in BPH for enlarged prostates > 40 g to shrink prostate by blocking the conversion of testosterone into DHT?
5a reductase inhibitors
What drug is 2nd line for BPH in sexually active men due to the increased incidence of sexual SEs (gets rid of DHT which is potent form of testosterone)?
5a reductase inhibitors
Which has a slower onset, a1 blockers or 5a reductase inhibitors?
5a reductase inhibitors
Why is it necessary to continue use of 5a reductase inhibitors long term for BPH?
Prostate size & sx will return if stopped
What SEs are associated with 5a reductase inhibitors?
ED, decreased libido, ejaculation disorders, HA, N, abd pain, gynecomastia, pregnancy category X
How do PDEIs work to treat BPH?
Prevent breakdown of cGMP and cause smooth muscle relaxation around prostate & bladder neck
Which PDEI is preferred to use in BPH treatment?
Tadalafil
What is the gold standard treatment for moderate to severe BPH unresponsive to drug therapy?
Prostatectomy
What is stress urinary incontinence?
Urethral underactivity→ inadequate urethral closing pressure causes episodic low volume leakage with activity (sneeze, exercise, etc)
What drugs aggravate urethral under activity (stress urinary incontinence)?
Alpha antagonists → releases smooth muscle & decreases closing pressure
ACEI → can cause coughing
A patient with stress urinary incontinence is started on an ACEI, but experiences increased coughing. Which drug should they be switched to?
ARB
What is urge urinary incontinence?
bladder overactivity → leakage w/ urgency (desire to void) due to involuntary contractions of detrusor
What can worsen urge urinary incontinence (bladder overactivity)?
Diuretics & alcohol
What is overflow incontinence?
Leakage d/t filled bladder unable to empty (chronic urinary retention)
urethral hyperactivity (MCC BPH) & bladder under activity (outlet obstruction, DM, etc)
What medications can worsen urethral hyperactivity (overflow incontinence)?
TCAs→ anticholinergic properties
Alpha-agonists→ squeezing on a receptors to close urethra
What medications can decrease bladder contractility (overflow incontinence)?
Anticholinergics, TCAs, CCBs, antipsychotics
What kind of urinary incontinence has the following presentation?
leakage with physical exertion
Stress UI (urethral UNDERactivity)
What kind of urinary incontinence has the following presentation?
urinary frequency (>8 times a day)
urgency
Urge UI (bladder OVERactivity)
What kind of urinary incontinence has the following presentation?
lower abdominal fullness
hesitancy
incomplete bladder emptying
± frequency & urgency
Overflow UI (urethral OVERactivity & bladder UNDERactivity)
What is the first line treatment for mild-mod UI?
Non pharmacologic- behavioral interventions, lifestyle mods, toilet scheduling regimens, pelvic floor rehabilitation
What drugs are anticholinergics used to treat urge UI?
Oxybutynin
Tolterodine
Trospium
Solifenacin
Darifenacin
Fesoterodine
What is first line RX for urge UI?
Anticholinergics
How do anticholinergics work to treat urge UI?
Antagonize muscarinic receptors & suppress premature detrusor contractions → allows bladder to relax & accommodate bigger volumes of urine
What SEs are seen with anticholinergics?
Blind as a bat: mydriasis, blurred vision
Mad as a hatter: AMS
Red as a beet: flushing/vasodilation
Hot as a hare: hyperthermia, dec sweating
Dry as a bone: dry mouth, skin, mucus membranes
Bowel & bladder lose their tone: urinary retention, constipation
Heart runs alone: tachycardia
What are CIs to anticholinergics?
Urinary retention, gastric retention, decreased GI motility, uncontrolled narrow angle glaucoma, MG
Why are anticholinergics not good for elderly?
AMS, falls