ch 7 mood disorders
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
60 Terms
mood
feelings state that color our psychological lives
mood disorders
people who experience disturbances in mood that are unusually severe or prolonged and impair their ability to function in normal responsibilities
depressive disorders
persistant depressive disorder (dysthmia)
premenstrual dysmorphic disorder (PMDD)
major depressive disorder (MDD)
bipolar disorders
bipolar disorder
clyclothymic disorder
mood thermometer
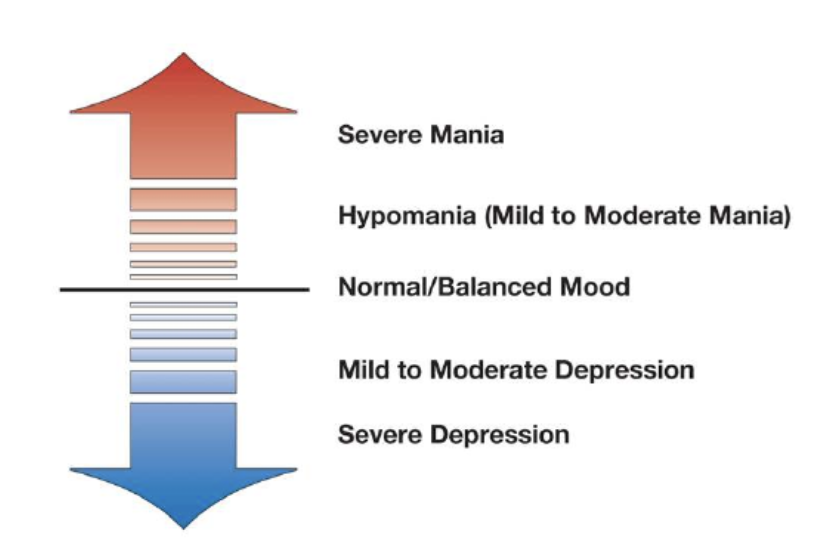
Major depressive disorder
based on the occurrence of atleast one major depressive episode in the absence of a history of mania or hypomania
period of 2 weeks of symptoms
mania
state of unusual elation, energy, and activity
hypomania
a relatively mild state of mania
MDD DSM-5 criteria
5 or more of the following symptoms present for 2 1eeks and represent a change from previous functioning. atleast one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
depressed mood most of the day, nearly every day, as indicated by either subjective report or observation made by others
markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation)
significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day
insomnia or hypersomnia nearly every day
psychomotor agitation or retardation nearly every day
fatigue or loss of energy nearly every day
feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day
diminished ability to think or concentrate, or indecisiveness nearly every day
recurrent thoughts of death , recurrent suicidal ideation without a specific plan, or a suicide attempt or specific committing suicide
- the symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
- the episode is not attribute to the physiological effects of a substance or to another medical condition
- the occurrence of the major depressive episode is not better explained by schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder, or other specified and unspecified schizophrenia spectrum and other psychotic disorders
- there has never been a manic episode or a hypomanic episode
prevelance rates for MDD
latinos, asian americans, non-hispanic black americans are less likely than non-hispanic white americans to receive treatment for depression
MDD affects 20.6% of adults in their lifetime
1 in 10 adults experienced MDD in the past year
women (26.1%) men (14.7%)
estimated 330 million people in the world
risk factors of MDD
age
socioeconomic status
marital status
gender (women)
history of child sexual abuse
family history of MDD
seasonal affective disorder
seasonal changes might affect availability or use in brain of the mood regulating nuerotransmitter serotonin during winter months
SAD features
affects 3-10% of population
women twice as effected
causes unknown—possibility that seasonal changes in light affect bodys underlying biological rhythms that regulate processes such as body temp and sleep wake cycles
SAD treatments
phototherapy (artificial light)
anti depressants
cbt
postpartum depression
persistant and severe mood changes that occur after childbirth
10-15%
depressed mood and crying spells, disturbed sleep, changes in appetite, low self esteem, difficulties maintaining concentration or attention, and difficulty bonding with the infant
high rates in south african women and chinese women from hong kong
postpartum psychosis
new mother loses touch with reality and experiences symptoms such as
hallucinations, delusions, and irrational thinking
PPD treatment
cbt
interpersonal therapy
antidepressants
Persistent depressive disorder
a chronic type of depressive disorder that lasts for atleast 2 yrs
either chronic major depression or dysthymia (milder form)
dysthymia 2.5% pop, derives from greek roots meaning bad spirit
double depression- concurrent MDD and dysthymia
premenstural dysphoric disorder
more severe form of premenstrual syndrome where women experience a
range of significant psychological symptoms in the week before menstruation
premenstural DD symptoms
mood swings, sudden tearfulness or feelings of sadness, depressed mood or feelings of hopelessness, irritability or anger, feelings of anxiety, tension, being on edge, greater sensitivity to rejection negative thoughts about oneself
PMDD facts
introduces as a diagnostic cat in DSm-5 intended to draw greater attention to the problem of mood swings and delivery services
1/5 women
bipolar disorder
psychological disorder characterized by mood swings between states of extreme elation and depression
2 types of bipolar disorder
bipolar 1 disorder
atleast one full manic episode
extreme mood swings between manic and major depressive episodes
possible to not have a depressive episode, but is common
bipolar 2 disorder
both hypomanic episodes and atleast one major depressive episode
no full blown manic episode
Bipolar disorder prevelence
1%
develops around age 20
some not all bipolar 2 patients develop bipolar 1
rapid cycling- a person experiences 2 or more full cycles of mania and depression within a yr without any intervening normal periods
michaelangelo, vincent van gough all had
manic episode
sudden elevation or expansion of mood
unusually cheerful or euphoric
extremely sociable → sometimes to point of becoming overly demanding and overbearing
increased energy and activity
poor judgement: argumentative, overly generous, etc
rapid speech
inflated ego and self esteem
distractible
lavish spending, reckless driving, sexual escapades
severe cases: delusions, hallucinations
cyclothymic disorder
a mood disorder characterized by a chronic pattern of less severe mood swings than are found in bipolar disorder
period of at least two years where person has numerous periods of hypomanic and depressive symptoms but not severe enough to meet the criteria for a hypomanic episode or major depression
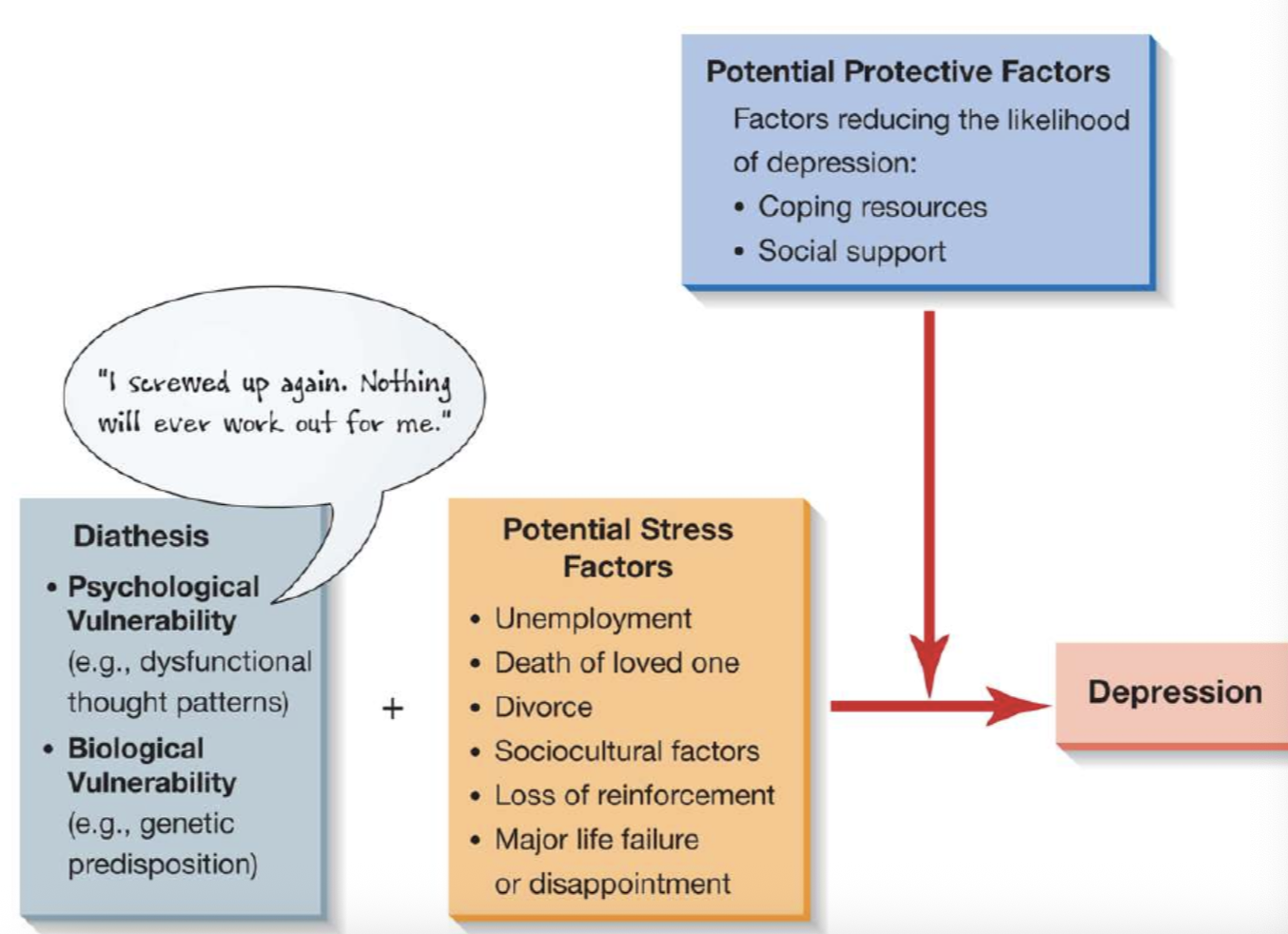
stress and depression role in mood disorders
stressful life events increase risk
loss of loved one, breakup, prolonged unemployment, serious physical illness, marital or relationship problems, separation or divorce, exposure to racism and discrimination, living in unsafe distressed neighborhoods
early life experiences
lack of secure attachments to parents, parental divorce, physical abuse
psychological factors as buffers against stress
strong marital relationship for example
psychodynamic theories on mood disorders (freud)
depression represents anger directed inward rather than against significant others
mourning is healthy process → pathological mourning does not, fosters lingering depression
to preserve psychological connection to lost object, people introject a mental representation of the object → anger is turned inward, against the part of self that represents the inward representation of the lost person
freud and bipolar psychodynamic theories
represents shifting dominance of individuals personality between ego and superego
in depressive state, superego is dominant producing exaggerated notions of wrongdoing and flooding an individual with feelings of guilt and worthlessness
ego rebounds and asserts supremacy, producing feelings of elation and self confidence that characterize the manic phase
stress focusing model (psychodynamic theories)
considers how people allocate their attentional processes after a loss such as the death of a loved one or personal failure or significant disappointment → depressed people have difficulty thinking about anything other than themselves and the loss they experienced
research evidence for psychodynamic theorists in mood disorders
people become depressed when they cannot imbue their existence with meaning and make authentic choices that lead to self fulfillment
guilt may arises when people believe they have not lived up to their potential
focus on loss of self esteem that can occur when people lose friends or family members or suffer occupational setbacks
when role identities are lost, our sense of purpose and self worth can be shattered
learning theories of mood disorders
learning theorists emphasize situational factors such as the loss of positive reinforcement
lack of reinforcement for ones efforts can sap motivation and induce feelings of depression
secondary source of reinforcement- people relieving depressed person from responsibilties
changes in life circumstances may alter balance of effort and reinforcement
physical activity can help depressionreinforcement.
interactional theory of mood disorders
problems in interpersonal relationships may help explain lack of positive reinforcemnt
stressful living situation
recipricol interaction - our behaviors influence how others respond to us, anger can lead to depression
low social skills
cognitive theories of mood disorders
cognitive triad of depression
negative beliefs about oneself
negative beliefs about environment
negative beleifs about future
greater risk of becoming depressed
beck views these concepts of the self and world as mental templates that are adopted in childhood and on the basis of early learning experiences
children may find nothing they do is good enough
cognitive disortions, all or nothinng thinking, overgeneralization, mental filter, jumpting to conclusion, magnification and minimization, emotional reasoning, learned helplessness
cognitive specificity hypothesis
proposes that different disorders are characterized by different types of automatic thought
certain types of negative thoughts are associated with depression while others to anxiety
humanisitc theories on mood disorders
humanistic theorists focus on the loss of self esteem that can occur when people lose firends, or family members or sufffer occupational setbacls
learning theories of mood disorders
learning therorists emphasize situational factors such as the loss of positive reinforcement
peter lewisohn proposed that depression results from an inbalance between behavior and reinforcement
biological factors of mood disorders
genetic factors
interactions of genetic and environmental factors in major depression and other mood disorders
runs in family
biochemical factors and brain abnormalities
lack of serotonin or norpinephrine
unlikely the only cause
casual factors of mood disorders
genetic factors
higher risk associated with higher paternal age (55)
family history
stressful life events may trigger episodes
psychosocial
social support can enhance levels of functioning
helps speedy recovery form mood episodes and reduces likelihood of recurrent episodes
learned helplessness theory
proposes that people may become depressed because they learn to view themselves as helpless to change their lives for the better
(martin seligman)
failing to learn to escape when escape is possible
some forms of depression in humans might result from exposure to apparently uncontrollable situations → “why try?”
attributional style
when bad things occur, we explain them in characteristic ways
blaming ourselves, circumstances, typical events, isolated events, broader problems, evidence of precise and limited shortcomings
internal factors: failures reflect personal inadequacies
global factors: failures reflect sweeping flaws in personality
stable factors: failures reflect fixed personality factors rather than unstable factors or beliefs that the factors leading to failures are unchangable
treatment of mood disorders
depressive disorders are typically treated with psychotherapy in the form of psychodynamic therapy, behavior or cognitive therapy, or with biomedical treatments such as antidepressants or electroconclusive therapy
psychodynamic treatments of mood disorder
traditional psychoanalysis aims to help depressed people understand underlying ambivalent (conflicting) feelings toward important people (objects) in their lives whom they have lost or whose loss was threatened
modern psychoanalysis focuses on unconscious conflicts but are more direct, relatively brief and focus on present as well as past conflicted relationships
interpersonal therapy (psychodynamic)
brief therapy (no more than 9 to 12 months) that emphasizes the role of interpersonal issues in depression and help clients make healthy changes in their relationships
similar to traditional psychodynamic approaches but focuses on clients current relationships rather than unconscious internal conflicts of childhood origin
behavior therapy (psychodynamic)
focus on helping depressed patients develop more effective social or interpersonal skills and increasing their participation in pleasurable or rewarding activities
____ activation encourages patients to increase their frequency of rewarding or enjoyable activities
often used along with cognitive therapy (CBT)
CBT
distorted thinking or cognitive distortions play a key role in the development of depression
cognitive therapy is also brief 14 to 16 week
biomedical treatment antidepressants
tricyclics (TCAs)
imipramine (Tofranil)
antitriptyline (Elavil)
desipramine (Norpramin)
doxepin (Sinequan)
monoamine oxidase (MAO) inhibitors
selective serotonin-reuptake inhibitors (SSRIs)
fluoxetine (Prozac)
setraline (Zoloft)
serotonin-norepinephrine reuptake inhibitors (SNRIs)
venlafaxine (effexor)
SSRIs are less toxic and have fewer cardiovascular side effects than tricyclics and MAO inhibitors
ketamine
when used under medical supervision, has significant therapeutic benefits
helps reduce suicidal ideation within hours
electroconclusive therapy
shock therapy
6-12 treatments
only used for people who dont respond to antidepressant meds
lithium and mood stabilizers
lithium helps reduce mania and stabilizes mood in bipolar patients → many patients either fail to respond to the drug or cannot tolerate it
other drugs
carbamazepine (Tegretol)
divalproex (Depakote)
lamotrigine (Lamictal)
anticonvulsant drugs are especially help in cases in which bipolar patients have not esponded to lithium or cannot tolerate its side effects
diathesis stress model
suicide risk factors
mood disorders
schizophrenia
suicide in older adults
highest among middle aged or older adults
suffer from mourning, leading to isolation
gender and ethnic differences in suicide
most common among white americans, american indians, and alaskan natives
white americans are twice as likely to take their own lives as african amerians
hopelessness and exposure to others who have attempted or committed may contribute to increased risk among AI/AN youth
greater risk tend to be reared in communities that are laregely isolated from us society
percieve themselves as having few opportunities to gain the skills necessary to join a workforce in a large society
suicide risks cont
prior suicide attemps
role of stress
screen time - 50% of teens who spend 5 or more hours on device reported suicidal behavior
psychodynamic model on suicide
suicide represents inward directed anger that turns murderous
seek to vent their rage against internalized representation of the love object
emilie durkheim on suicide
people who experienced anomie (who feel lost, without identity, rootless) are more likely to commit suicide
higher levels of social support result in lower levels of suicidal thoughts
learning theorists on suicide
focus on lack of problem solving skills for handling significant life stress
social cognitive theory on suicide
suggest suicide is motivated by personal experiences
potential modeling effect of observing suicidal behaviors in others
social contagion- spreading of suicide in a community
biological and casual factors of suicide
Biological factors
genetic and neurotransmitter imbalances involving the mood regulating chemical serotonin
causal factors
motivated by desire to escape from unbearable emotional pain
preventing suicide
behavioral clues
suddenly sorting out affairs
purchase gun
suddenly feel at peace
increased suicidal risk include substance abuse, financial problems, recent crisis, medical problems, relationship problem