Oral Health
1/89
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
90 Terms
Why can an older adult experience a complete tooth fracture or deep decay without feeling any pain?
There is an overall decreased sensitivity of the tooth due to a decrease in pulpal cell density/activity and the thickening of dentin and cementum.
What happens to the dental pulp as a person ages?
Pulpal cells decrease in density and functioning, and the pulp size constricts due to the continuous deposition of secondary dentin.
What are the age-related changes to tooth enamel and appearance?
Enamel becomes more brittle (leading to cracks), and teeth commonly darken with age.
What should be a routine part of the Review of Systems (ROS) regarding oral health in an H&P?
The clinician should ask about specific dental problems, the date of the last dental visit, and the presence of any dental pain.
What is the first step in the physical examination of the mouth for a patient with dentures?
The dentures must be removed to allow for a full inspection of the underlying tissues.
Which areas must be visualized during an oral examination using a tongue blade?
The buccal mucosa, gingiva, palate, floor of the mouth, and all surfaces of the tongue.
What 'red flag' findings during an oral exam warrant a dental referral?
Inflammation, white or red patches, ulcerations, or the presence of broken and decayed teeth.
Is 'Dry Mouth' (xerostomia) considered a normal part of the aging process?
No. Dry mouth is an abnormal finding that affects health and nutrition; patients should be urged to seek therapeutic care.
What is the primary responsibility of a non-dental clinician regarding oral health?
The clinician does not need to provide a specific dental diagnosis but must be able to recognize when 'something does not look right' and refer accordingly.
Why is oral health particularly critical for frail or nutritionally at-risk older adults?
Dysfunction and disease in the mouth directly affect social functioning and the ability to maintain adequate nutritional intake, which can worsen frailty.
What is the primary cause and clinical process of dental caries?
Caries is a bacterially caused demineralization and cavitation of the teeth that can occur throughout a person's entire lifespan.
Define 'Recurrent Caries' and 'Root Caries,' which are common in the elderly.
Recurrent caries occurs at the interface of a dental restoration (like a filling or crown) and the tooth. Root caries occurs on the exposed root surfaces of the teeth.
Why are recurrent and root caries particularly dangerous in geriatric patients?
They are often asymptomatic, meaning the decay can become advanced and destroy much of the tooth before it is ever discovered.
What is a potential systemic complication of untreated dental infections?
Bacterial Endocarditis. Alpha-hemolytic (viridans) streptococci from the oral cavity are implicated in one-third of endocarditis cases in the US.
What can happen if advanced dental decay is left untreated, even if it is not painful?
It may result in necrosis of the pulp, leading to a dental abscess. It must be treated to eliminate the source of infection.
What are the three main pillars of daily oral hygiene for preventing decay?
1. Brushing twice daily with fluoride-containing toothpaste. 2. Cleaning between the teeth (flossing). 3. Removing dentures before cleaning any remaining natural teeth.
What dietary modification is essential for preventing caries?
Limitation of sugar exposure on the teeth.
How is early-stage demineralization treated without surgery?
Through the application of topical high-potency fluoride for remineralization.
What treatments are required once dental caries involves the dental pulp?
Root canal treatment or tooth extraction.
What professional interventions help prevent and treat early decay?
Routine professional cleanings (prophylaxis), regular dental examinations, and topical fluoride applications.
What are the three components that make up the periodontium?
The gingiva (gums), the alveolar bone, and the periodontal ligament.
How does periodontal disease begin and progress?
It starts when bacterial colonies (plaque) form on the teeth near or under the gingiva. If not removed, plaque hardens into tartar (calculus), which further irritates the gums.
Distinguish between Gingivitis and Periodontitis.
Gingivitis is an inflammatory reaction limited to the gums and is rapidly reversible. Periodontitis involves the destruction of the periodontal ligament and alveolar bone; while treatable, this damage is irreversible.
What are the primary risk factors for periodontal disease?
Advancing age, smoking, and poor oral hygiene.
Which demographic groups in the U.S. show a significantly higher prevalence of advanced periodontitis?
Black and Hispanic Americans have a significantly higher prevalence compared to white Americans.
What is the clinical term for the 'deep cleaning' used to treat periodontal disease?
Scaling and root planing.
How has the rate of edentulism (total tooth loss) changed in Americans >75 since the 1960s?
It has dropped significantly: from over 70% in the 1960s to less than 25% today.
What are the consequences of total tooth loss without prosthetic replacement?
Drastic changes in facial appearance, severely compromised chewing ability, and negative impacts on nutritional intake.
What is the limitation of removable dentures compared to natural teeth?
They are less predictable in restoring the full ability to chew and require periodic professional adjustments.
Should denture adhesives be used to fix poorly fitting dentures?
No, they should not be used to compensate for a poor fit; professional adjustment is required.
What are the primary functional and aesthetic benefits of removable dentures?
They aid in speech and restore facial contours that would otherwise collapse due to tooth loss.
How do dentures compare to natural teeth in terms of restoring the ability to chew?
They are less predictable in restoring full chewing function compared to natural teeth.
Why do dentures require periodic professional adjustment?
The underlying bone and soft tissue in the mouth change over time, which can lead to a poor fit, soreness, or instability.
What is the clinical rule regarding the use of denture adhesives?
They may be used for extra stability, but should never be used to compensate for a poorly fitting denture.
What is a more stable alternative to standard removable dentures?
Dental implants, which can be used to retain the dentures but require surgical placement.
How often should dentures be removed and cleaned?
They should be removed and cleaned after every meal.
What is the recommendation for 'rest time' for the oral tissues when wearing dentures?
Dentures should be removed for several hours each day; leaving them out overnight is considered the best practice.
What are the two main reasons a patient should see a dentist regarding their dentures?
1. If the dentures are fractured or broken. 2. If the patient experiences looseness or soreness.
What type of cleaners are appropriate for at-home denture care?
Over-the-counter (OTC) denture cleaners are acceptable for daily maintenance.
What is the clinical description and treatment for Angular Cheilitis?
Description: Red, cracked labial commissures. Treatment: Nystatin-triamcinolone cream.
Where are Aphthous Ulcers (canker sores) typically located and how are they treated?
Location: Nonattached (movable) mucosa. Treatment: Topical anesthetic or mild steroid.
How do you identify a Candidal Infection and what is a key step if the patient wears dentures?
Identification: White plaques that are easily wiped away or mucosal erythema. Key step: Treat the dentures as well as the oral mucosa with antifungal agents.
What characterizes a Geographic Tongue and what is the required treatment?
Description: Irregular smooth patches on the tongue. Treatment: No treatment is required.
What is the primary difference between Herpes Simplex and Aphthous Ulcers regarding location?
Herpes Simplex is found on attached mucosa, whereas Aphthous Ulcers are on nonattached mucosa.
What are the 'red flag' characteristics of an Oral Malignancy?
Indurated (hard) ulcer, exophytic mass, irregular borders, and long duration.
What is a Parulis (gum boil) and how is the underlying cause treated?
A solitary, soft nodule on the gingiva associated with a nonvital tooth. Treatment: Root canal therapy or extraction of the involved tooth.
How do you distinguish Gingivitis from Periodontal Disease in a clinical description?
Gingivitis is limited to gingival inflammation. Periodontal Disease includes both gingival inflammation and alveolar bone loss.
What is a Torus (tori) and what is the management plan?
A bony exostosis on the palate or lingual surface. Management: No treatment is required.
What is the clinical approach to a Traumatic Ulcer?
Identify and remove the offending etiology and apply topical anesthetic for comfort.
What is Burning Mouth Syndrome and who does it typically affect?
It is a chronic oral-facial pain disorder, usually without clinical signs. It typically affects women ≥50, with particularly high rates in Asian Americans and Native Americans.
How is Burning Mouth Syndrome treated?
Treatment is empirical and symptomatic, as causes can range from nutritional deficiencies and xerostomia to psychiatric disorders.
What is the clinical appearance of an oral malignancy?
It can appear as painless red, white, or mixed red/white areas of the mucosa that may be ulcerated or indurated (hard).
Distinguish between Erythroplakia and Leukoplakia regarding malignancy risk.
Erythroplakia (red/mixed lesions) displays cellular atypia in up to 93% of cases and requires immediate biopsy. Leukoplakia (white lesions) is malignant <10% of the time but requires a biopsy if not healed in 14 days.
Does healthy aging naturally cause a significant decrease in saliva production?
No. While salivary glands undergo histologic changes, longitudinal studies show saliva production remains essentially unchanged in healthy aging.
What makes salivary glands more susceptible to hypofunction in extreme old age?
Factors such as dehydration or drug-induced hypofunction (e.g., from anticholinergics or TCAs).
Name three systemic diseases that can decrease salivary flow.
Sjogren syndrome, poorly controlled Diabetes Mellitus, and Hypothyroidism.
What aggressive preventive measure is required for patients undergoing head and neck radiation?
They must start a program including daily fluoride application prior to the start of radiation to prevent rapid dental decay.
Which medications can be considered to help stimulate salivary flow?
Pilocarpine and cevimeline.
What lifestyle counseling should be provided to a patient with chronic dry mouth?
Limit sugar in the diet, optimize daily oral hygiene, and schedule more frequent dental examinations due to the high risk of oral disease.
How does olfactory (smell) function change with advancing age?
Olfactory function declines with age, typically affecting older men more than older women.
What are the practical safety risks associated with impaired olfaction in the elderly?
Increased risk of eating spoiled food, failing to notice gas leaks, or failing to detect smoke from domestic fires.
Which specific taste perceptions are most commonly 'blunted' in older adults?
The subjective perception of saltiness and sweetness.
What is the clinical significance of blunted taste perception in a geriatric patient's diet?
It may lead to a tendency to oversalt foods (risky for hypertension/HF) or crave excessive sweets.
How can a drug impair taste even if it has no primary effect on the taste buds?
By causing diminished salivary flow (xerostomia), which is necessary for the chemical molecules in food to reach the taste receptors.
Review these drugsxxx
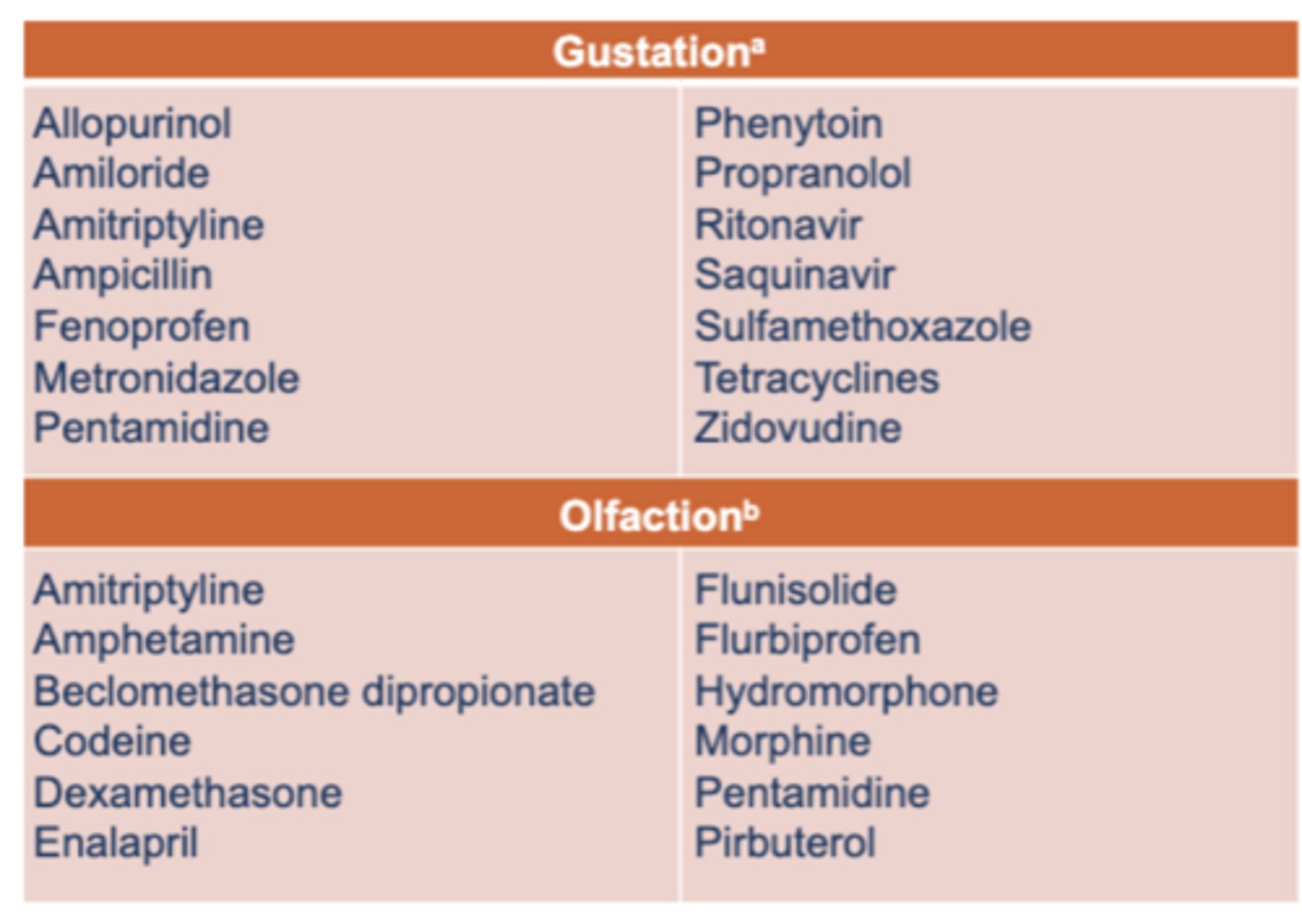
Name three common medications that interfere with BOTH Gustation and Olfaction.
Amitriptyline, Pentamidine, and various corticosteroids/NSAIDs.
What nutritional deficiencies are linked to gustatory (taste) dysfunction?
Vitamin B12, Niacin, and Zinc.
Which neurodegenerative and CNS conditions are nonpharmacologic causes of taste dysfunction?
Alzheimer disease, stroke, CNS tumors, and head trauma.
Name three endocrinopathies that can cause gustatory dysfunction.
Diabetes Mellitus (DM), Cushing syndrome, and Hypothyroidism (or adrenocortical insufficiency).
What oral conditions can lead to gustatory dysfunction by affecting afferent nerves or saliva?
Burning mouth syndrome, Candidiasis, Lacerations, Malignancy, and Therapeutic irradiation of the head.
Which three major systemic conditions are most strongly associated with periodontal disease?
Cardiovascular Disease (CAD, PVD, CVD), Pneumonia, and Hyperglycemia (Diabetes).
How does daily oral hygiene impact outcomes in hospitalized or institutionalized patients?
It reduces institution-acquired pneumonia, lowers mortality rates, and reduces the length of stay for patients on ventilators or in nursing homes.
What are the two proposed mechanisms linking periodontal disease to Cardiovascular Disease (CVD)?
1. Direct infection: Oral bacteria cause an inflammatory response leading to plaque in blood vessels. 2. Platelet aggregation: Periodontal pathogens can cause platelets to clump, resulting in clot formation.
Explain the 'vicious cycle' between Periodontitis and Diabetes.
Hyperglycemia impairs the body's ability to kill bacteria, worsening periodontitis. Conversely, the inflammation from periodontitis can cause hyperglycemia, making blood sugar harder to control.
What is the current recommendation for antibiotic prophylaxis in patients with prosthetic joint replacements before dental work?
Routine antibiotic prophylaxis is not indicated for individuals with prosthetic joint replacements.
When is antibiotic prophylaxis recommended for dental treatment?
Only in specific high-risk situations for individuals at elevated risk for infective endocarditis.
What is the standard protocol for patients on anticoagulants (like Warfarin) before an extraction?
Anticoagulants normally do not need to be discontinued. As long as the INR is ≤ 3.5, the risk of hemorrhage is minimal and outweighed by the benefit of anticoagulation.
Name three upper aerodigestive/respiratory causes of olfactory (smell) dysfunction.
Dental infection, Periodontal disease, and Sinusitis (also URI and tobacco use).
Which neurodegenerative disorders are nonpharmacologic causes of olfactory dysfunction?
Alzheimer's, Parkinson's, Lewy body disease, and multiple system atrophy.
What is Osteonecrosis of the Jaw (ONJ) and which medication class is most commonly associated with it?
ONJ is a condition where the jawbone is exposed and begins to starve from lack of blood; it is most frequently associated with high-dose bisphosphonates used for bony metastases.
Which gender and which jaw bone are more likely to be affected by ONJ?
Women are more likely to be affected than men, and the mandible (lower jaw) is more likely to be affected than the maxilla (upper jaw).
Is the use of bisphosphonates for standard osteoporosis likely to result in ONJ?
No. ONJ is unlikely to result from the standard anti-resorptive doses used for osteoporosis; it is primarily linked to the high doses used in cancer therapy.
What is the clinical recommendation for a patient about to start high-dose bisphosphonates for malignant disease?
The patient should complete all necessary dental care before the bisphosphonate therapy is started.
What is the main goal of providing daily oral care in long-term care (LTC) facilities?
To disrupt the plaque that accumulates on the teeth and to check for any new oral health problems.
Why are 'Proxabrushes' or interdental brushes often preferred over floss in LTC settings?
Flossing another individual is physically difficult and often poorly tolerated; interdental brushes are easier for caregivers to use and for residents to accept.
Why is it beneficial for a patient to 'spit but not rinse' after brushing with fluoride toothpaste?
Leaving the residual toothpaste in the mouth keeps the fluoride in contact with the teeth for a longer period, increasing its protective effect.
What is a safe way for a caregiver to keep a resident's mouth open during cleaning without using their fingers?
Use a second large-handle toothbrush, a stack of tongue blades, or a specialized mouth prop.
How should a caregiver approach oral hygiene for an individual with dementia?
Being directly in front of the individual allows them to see what is happening, which can reduce anxiety and be more beneficial for cooperation.
A 78-year-old woman has recently had difficulty eating and swallowing solid foods. When she tries to swallow, the food irritates her cheeks and roof of her mouth.
History includes: Hypertension, Diabetes mellitus
Kidney stones (recent), Depression
Current medications: Hydrochlorothiazide, Metformin
Fluoxetine
For the first time in many years, she has several cavities located at the roots of her teeth, identified at a recent dental examination
Which of the following is the most likely explanation for her dry mouth?
A. Normal aging
B. Salivary duct stones
C. Sjögren syndrome
D. Medications
D. Medications
A 72-year-old woman has pain at the site of a maxillary tooth extracted 8 months ago. She has a history of metastatic breast cancer and has been receiving intravenous bisphosphonate for the past 12 months.
On examination
The extraction socket has not healed
Gingival tissue is open, with bone protruding from the site
The area is erythematous, and some purulent drainage is apparent
Which of the following is the most likely diagnosis?
A. Osteomyelitis of the maxilla
B. Necrotizing periodontitis
C. Osteonecrosis of the jaw
D. Incomplete tooth extraction with residual root
C. Osteonecrosis of the jaw