Central Visual Pathways & The Perceived Visual Field
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
What is vision?
• Vision is the conscious perception of information from the eyes
Processed in occipital cortex (mammals)
What gives organisms the ability to process visual information?
• The visual system is the part of the CNS which gives organisms the ability to process information that is contained in visible light
What are some of the methods used to assess vision in a veterinary practice?
Assessment of vision in veterinary species limited because by inference of behaviour
• Observation, unfamiliar environment
• Ability to track (silent movement e.g. cotton balls)
• Visual placing (if small animal)
• Menace response (other reasons for failure)
Describe the order of information processing in the visual pathway.
Retina →
Optic nerve →
Optic chiasm (Crossing region) →
Optic tract →
Lateral geniculate nucleus (Within thalamus) →
Optic radiation (White matter between thalamus to occipital cortex) →
Occipital cortex →
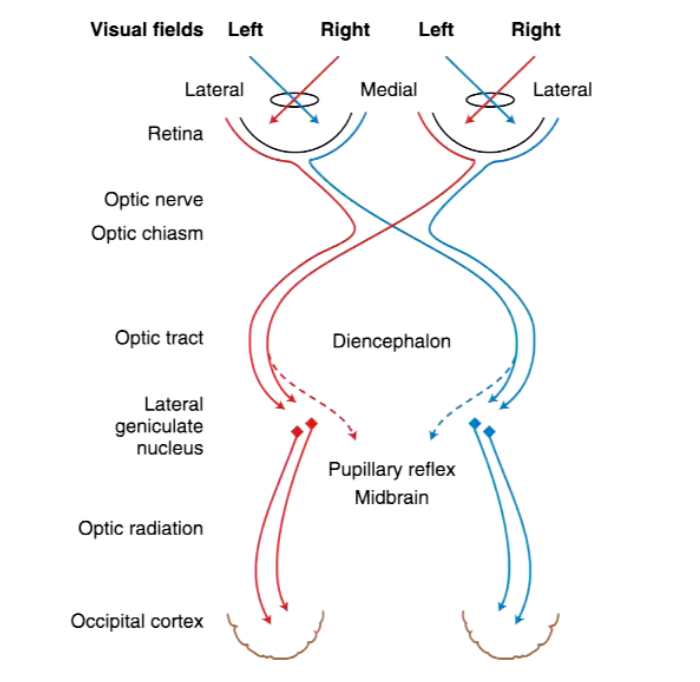
What is the visual field?
Visual field: The total area in which objects can be seen in the peripheral vision as you focus your eyes on a central point
Predators: large area ahead, small periphery, forward facing eyes
Prey: small area ahead, large periphery, lateral eyes
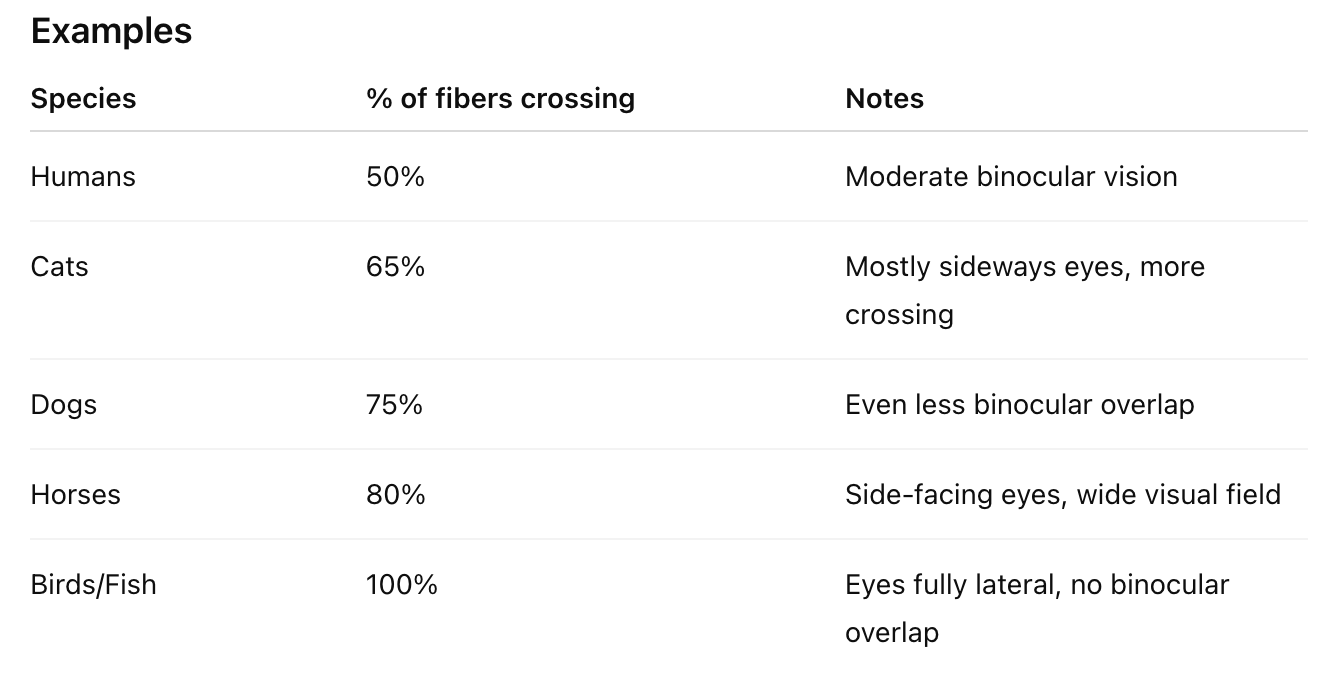
How does the cross over at the optic chiasm vary between species?
Optic Chiasm and Species Differences
The optic chiasm is where some of the optic nerve fibers cross to the opposite side of the brain.
Decussation = the crossing of fibers.
Key Points
Amount of crossing varies by species
Species with more lateral eyes (less binocular overlap) have more crossing.
Species with forward-facing eyes (more binocular vision) have less crossing.
Inverse relationship with binocular vision
More fiber crossover → less binocular vision.
Less fiber crossover → more binocular vision.
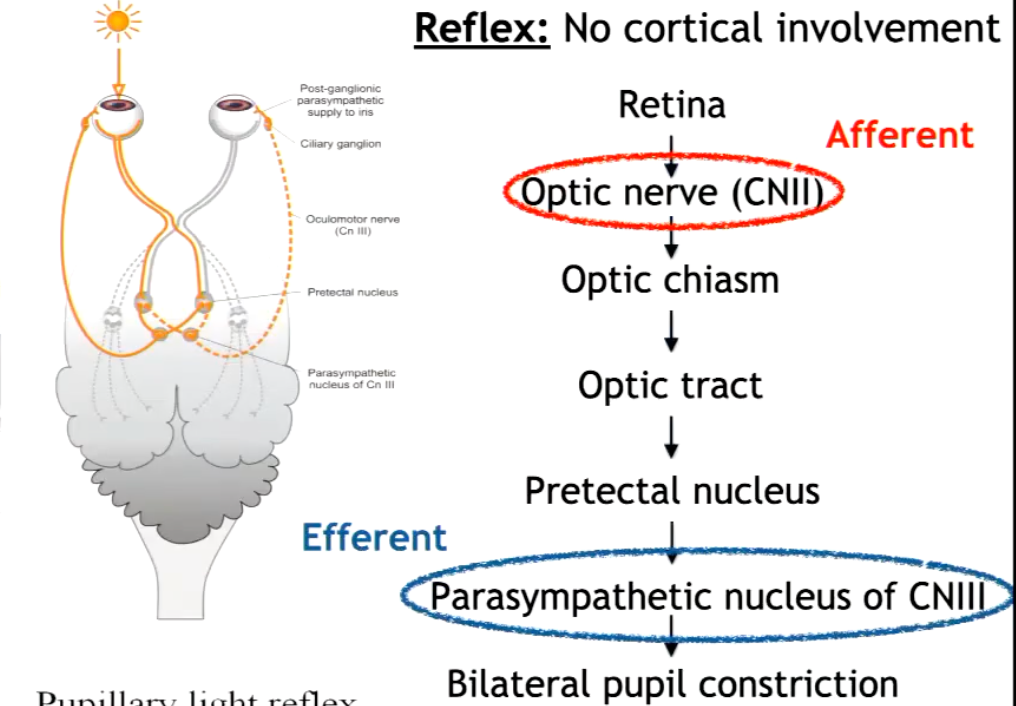
How do we test the visual pathway, specifically the pupillary light reflex?
Also note the pathway itself.
Shining a light into one eye, which should cause constriction on both sides, but increased on the eye with the light. It is a reflex, meaning no cortical involvement.
Afferent: Optic nerve (CN II) – detects light
Efferent: Oculomotor nerve (CN III) – constricts pupil (via sphincter pupillae)
Pathway: Retina → CN II → Pretectal nuclei → Edinger–Westphal nuclei → CN III → Ciliary ganglion → Pupil constriction
Response:
Direct: Same eye constricts
Consensual: Opposite eye constricts
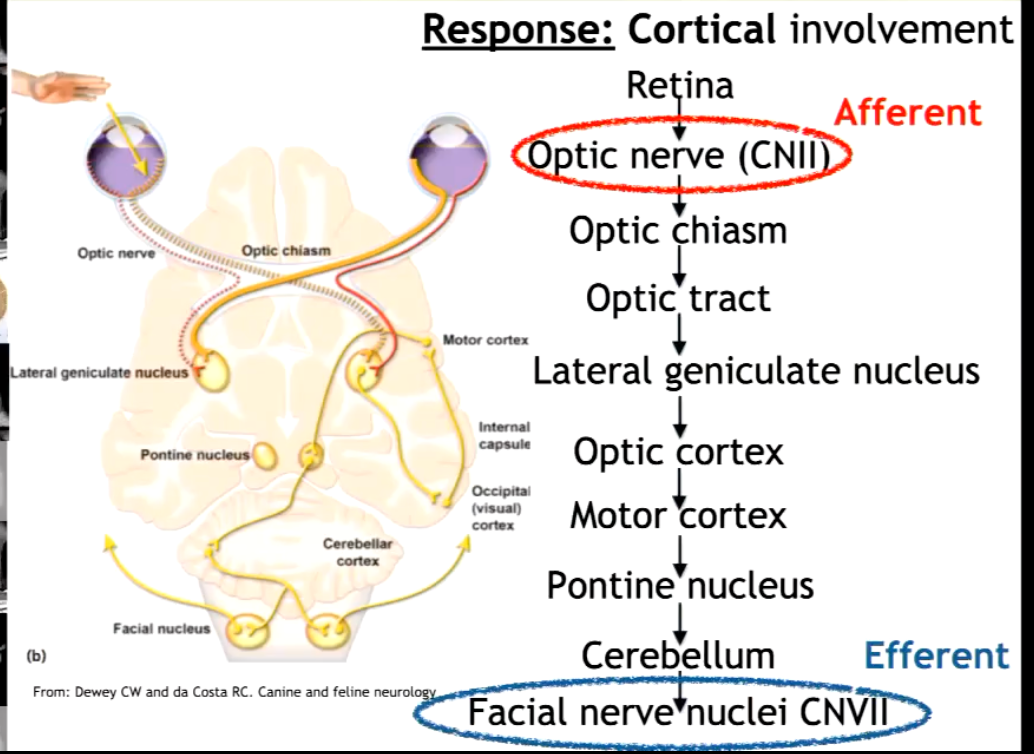
How do we test the visual pathway, specifically the menace response?
Also note the pathway itself.
Involves moving the hand in front of the eye, and monitoring for blinking and head movement, it is a response, meaning it requires cortical involvement.
The menace response is a blink reflex that occurs when a threatening gesture (like a quick hand wave) is made toward the eye — without touching it or creating air movement.
Visual stimulus (hand movement) → detected by retina
Signal travels via optic nerve (CN II) → optic chiasm → optic tract → visual cortex (occipital lobe)
Visual cortex processes the threat → sends signal to the motor cortex
Motor cortex → pontine nuclei → cerebellum and facial motor nucleus
Facial nerve (CN VII) → activates orbicularis oculi muscle → blink
What is central (Cortical) blindness (aka amaurosis)?
Where might lesions be found?
What are common clinical signs?
• Blindness without apparent lesion of the eyes
• Involves processing system
• Lesion in:
• Lateral geniculate nucleus
• Optic radiation
• Occipital cortex
• Clinical signs:
• Normal PLR
The PLR does not require visual (cortical) processing.
It’s a subcortical reflex, meaning it happens entirely within the midbrain — before signals reach the lateral geniculate nucleus (LGN) or visual cortex.
• Absent menace response
• Blind
What is peripheral (subcortical) blindness?
Where might lesions be found?
What are common clinical signs?
• Involves collection/distribution system
• Lesion in:
• Eye
• Optic neves
• Optic chiasm
• Optic tract
• Clinical signs:
• Absent PLR
• Absent menace response
• Blind
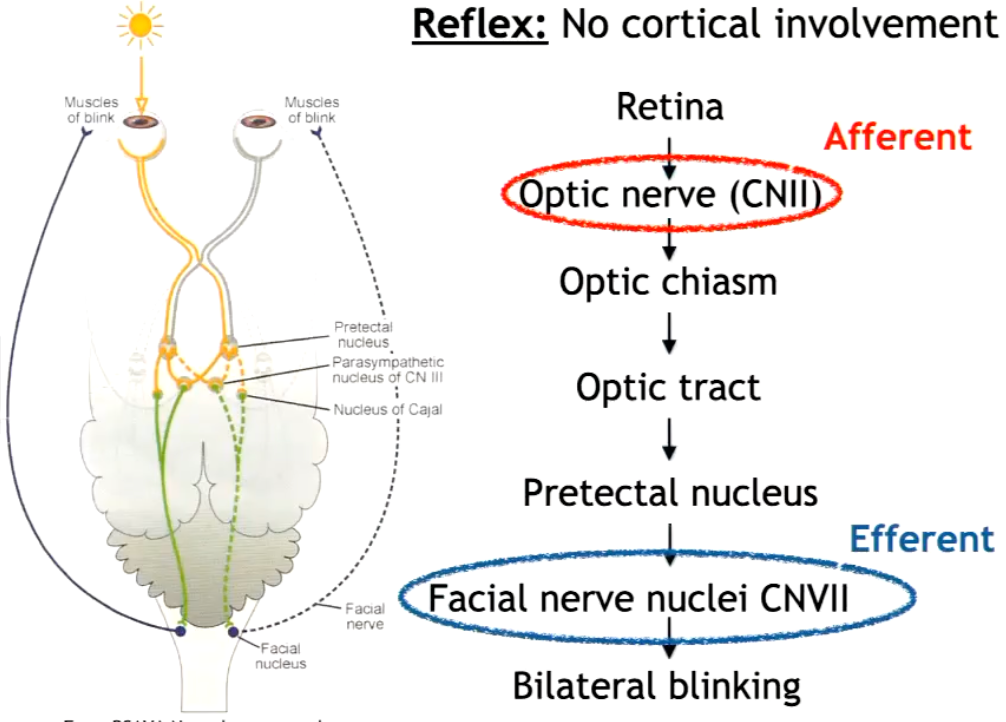
How do we test the visual pathway, specifically the dazzle reflex?
Also note the pathway itself.
Is a reflex (no cortical involvement), involves bilateral blinking by shining very bright light (Causing the eye to close to protect the retina).
The dazzle reflex is a subcortical blink response to sudden, intense light.
It’s a protective mechanism — the eyelids close involuntarily when a bright light is shone into the eyes.
Bright light stimulates retinal photoreceptors.
Signal travels via the optic nerve (CN II) → optic chiasm → to Optic Tract → Pretectal Nucleus
From there, fibers project to brainstem nuclei that control blinking:
Facial nucleus (CN VII) → activates orbicularis oculi muscle → bilateral blinking
Summarize the differences between peripheral (subcortical) and cortical blindness.
Peripheral Blindness
Caused by damage to the eye or optic nerve (the peripheral part of the visual system).
Examples: retinal disease, glaucoma, optic nerve injury.
Effect: Loss of vision in specific parts of the visual field, depending on which part of the retina or nerve is affected.
The brain is fine, so there’s no processing problem — the eye just can’t send signals.
Cortical Blindness
Caused by damage to the primary visual cortex (V1) in the occipital lobe.
Example: stroke, trauma, or lesion in V1.
Effect: Vision loss even though the eyes and optic nerves are intact.
Sometimes leads to “blindsight”, where patients can respond to visual stimuli without conscious awareness.
In short:
Peripheral blindness = problem with the eye or optic nerve.
Cortical blindness = problem in the brain’s visual cortex.
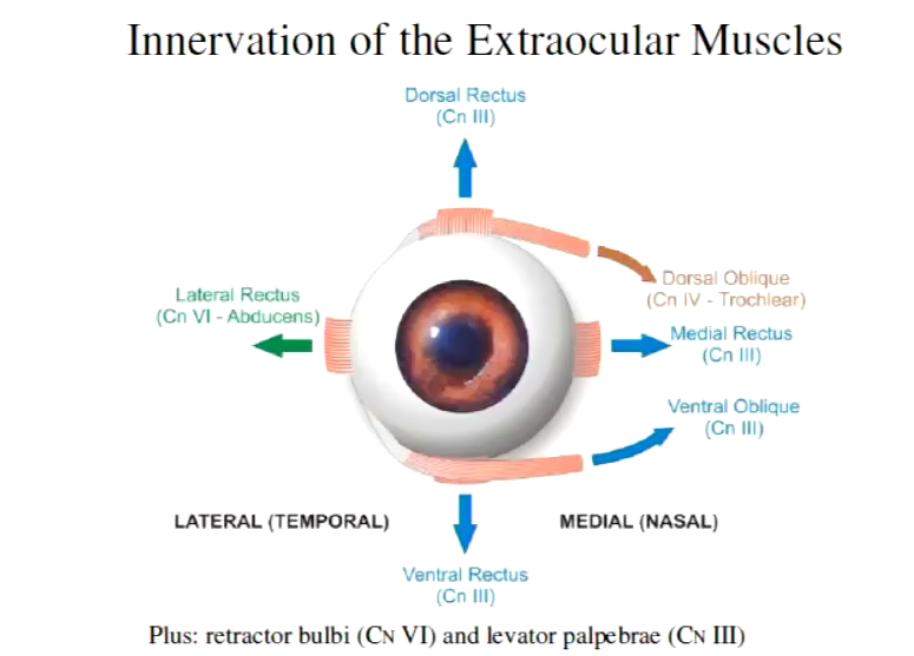
Summarize the innervation of the extraocular muscles.
1. Dorsal rectus
Action: Rotates the eye upward (elevation)
Innervation: Oculomotor nerve (CN III)
2. Ventral rectus
Action: Rotates the eye downward (depression)
Innervation: Oculomotor nerve (CN III)
3. Medial rectus
Action: Rotates the eye medially (adduction, toward nose)
Innervation: Oculomotor nerve (CN III)
4. Lateral rectus
Action: Rotates the eye laterally (abduction, away from nose)
Innervation: Abducens nerve (CN VI)
5. Dorsal oblique
Action: Intorts and depresses the eye (rotates the dorsal part medially and moves eye down when adducted)
Innervation: Trochlear nerve (CN IV)
6. Ventral oblique
Action: Extorts and elevates the eye (rotates the ventral part medially and moves eye up when adducted)
Innervation: Oculomotor nerve (CN III)
7. Levator palpebrae superioris
Action: Elevates the upper eyelid
Innervation: Oculomotor nerve (CN III)
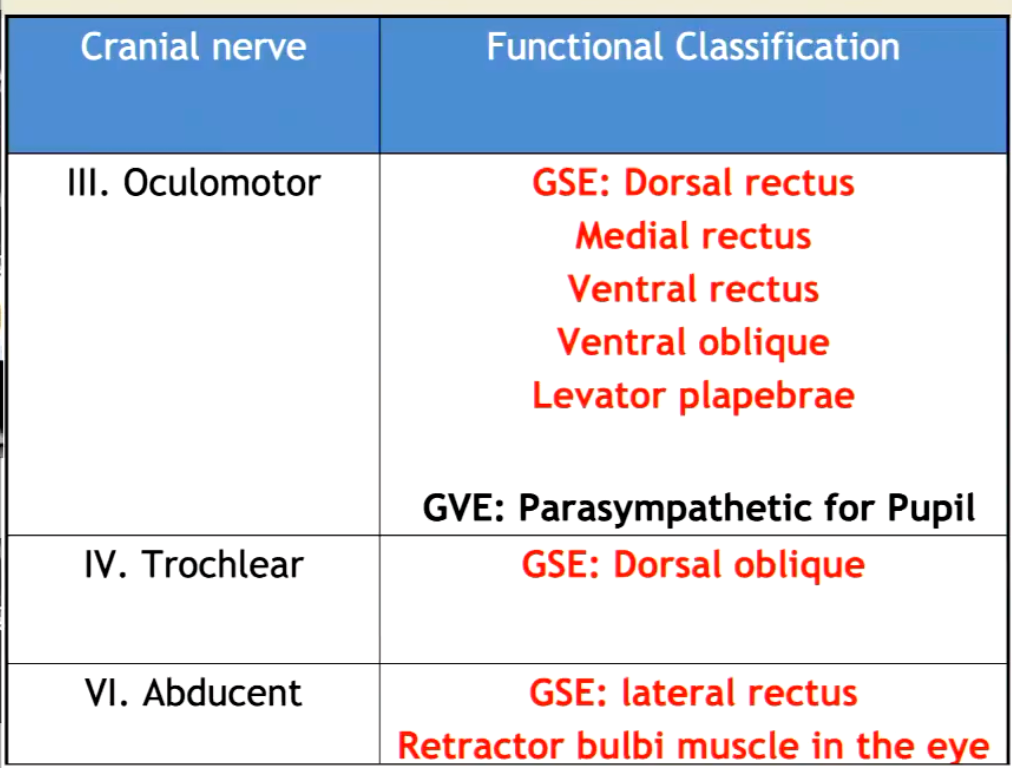
Describe the functional classification of nerves in the eye and those innervating the extra ocular muscles.
Lateral rectus → CN VI
Dorsal oblique → CN IV
All others → CN III
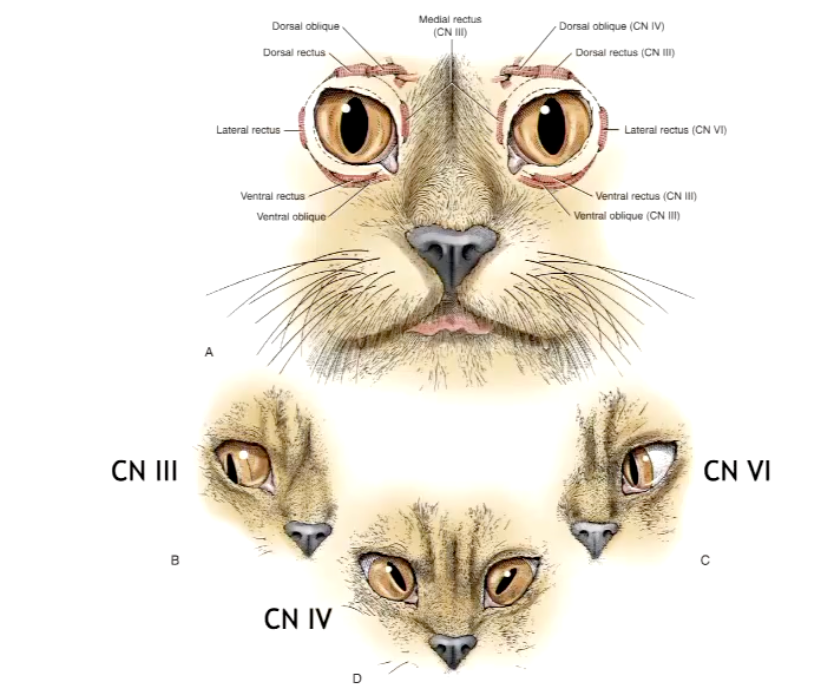
What is strabismus?
What position of the eye indicates issues with which nerve?
Strabismus is when the eyes are not properly aligned — one eye may turn inward, outward, upward, or downward while the other looks straight ahead.
CN III - eyes pulled laterally
CN IV - eyes pulled centrally
CN VI - eyes pulled medially
How do we assess eye movement?
using vestibulo-ocular eye movement tests
As eye position is also controlled by the vestibular system, as you move your head, you want your eyes to follow
Move head from one side to the other, should see physiological nystagmus
Can hold cat and move in a circle → eyes should flicker
Afferent: CN VIII (vestibular branch)
Efferent: CN III, IV, VI (eye movement)
Pathway: Vestibular apparatus → CN VIII → Vestibular nuclei → MLF → CN III/IV/VI → extraocular muscles
Tests: CN VIII + CN III, IV, VI + brainstem integrity
The vestibulo-ocular reflex stabilizes gaze during head movement — it keeps the eyes fixed on a target while the head moves.
It’s an automatic, brainstem-mediated reflex that links the vestibular system (balance) to the extraocular muscles (eye movement).