Benign and Malignant Liver Neoplasms
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
note location of mass related to the LIVER CAPSULE (2)
1. INTRAHEPATIC LESIONS can push OUTWARD toward the capsule causing IRREGULAR CONTOUR OR BULGING
2. EXTRAHEPATIC LESIONS can COMPRESS the capsule causing IRREGULAR CONTOUR AND INDENTATIONS
note the location of the mass related to SURROUNDING VASCULATURE (2)
1. lesions can cause EXTRINSIC COMPRESSION AND DISTORT NORMAL FLOW PATTERNS
2. vessel feeding the mass can aid in determination of mass origin
note the location of the mass related to BILIARY STRUCTURES (2)
1. EXTRINSIC COMPRESSION OF DUCTS can lead to DILATATION
2. CONNECTION TO BILIARY TREE can indicate BILIARY ORIGIN
note the presence/absence of
LYMPHADENOPATHY
hemangiomas facts (9)
1. #1 benign liver lesion
2. associated with FOCAL NODULAR HYPERPLASIA AND KASABACH-MERRITT SYNDROME
3. more common in FEMALES
4. usually found in RIGHT LOBE
5. usually SOLITARY, LESS THAN 3 CM
6. SUBCAPSULAR
7. most cases are ASYMPTOMATIC WITH NORMAL LFTs
8. can INCREASE SIZE with PREGNANCY and ESTROGEN THERAPY
9. differentiated from focal fatty replacement by the presence of MASS EFFECT
contrast US is very accurate for the eval of HEMANGIOMAS (4)
1. enhancement of the hemangioma THROUGHOUT the arterial and venous phases
2. BENIGN nodules usually demonstrate ISOVASCULAR ENHANCEMENT
3. MALIGNANT TUMORS usually demonstrate HYPERVASCULAR ENHANCEMENT
4. most MALIGNANT masses have contrast enhancement during ARTERIAL PHASE, but RAPID CONTRAST WASHOUT during VENOUS PHASE
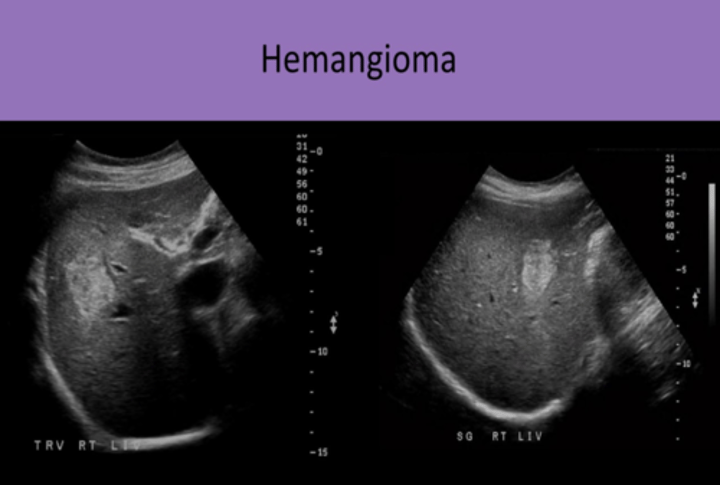
hemangioma sonographic appearance (6)
1. FOCAL concentration of blood vessels
2. HOMOGENEOUS, HYPERECHOIC, WELL DEFINED BORDERS, POSTERIOR ENHANCEMENT
3. areas of DEGENERATION, NECROSIS, AND FIBROSIS demonstrated as HYPOECHOIC
4. MASS EFFECT
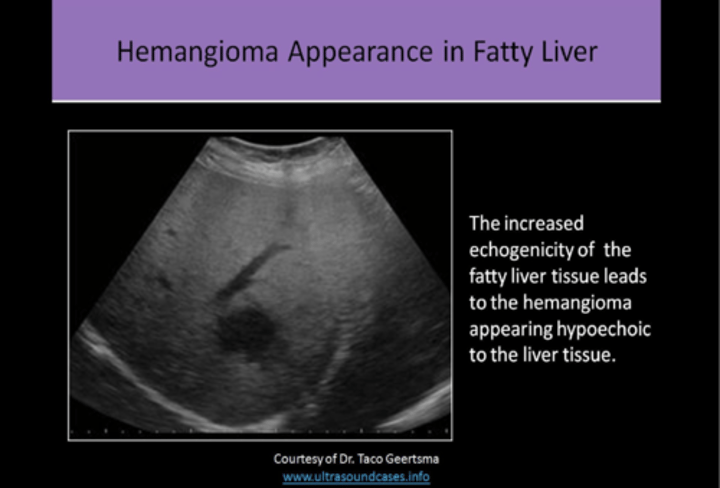
5. may appear HYPOECHOIC in a FATTY LIVER WITH INCREASED ECHOGENICITY
6. COLOR DOPPLER NOT USEFUL
Kasabach-Merritt Syndrome (5)
1. aka HEMANGIOMA THROMBOCYTOPENIA SYNDROME
2. seen in INFANTS with LARGE HEMANGIOMAS
3. SIGNIFICANT THROMBOCYTOPENIA
4. visible cutaneous BLUE or REDDISH-BROWN lesions usually present on extremities
5. HEPATOMEGALY OR JAUNDICE can be identified
Infantile Hemangioendothelioma (4)
1. MOST COMMON BENIGN VASCULAR TUMOR IN INFANCY
2. normally occurs within the FIRST 6 MONTHS OF LIFE
3. usually presents with HEART FAILURE EARLY IN LIFE due to AV MALFORMATION WITHIN THE TUMOR
4. SPONTANEOUSLY REGRESSES in most patients BEFORE AGE 2
Focal Nodular Hyperplasia (FNH) (6)
1. #2 MOST COMMON BENIGN LIVER MASS
2. contains all normal liver parenchymal components, EXCEPT NORMAL PORTAL VENOUS STRUCTURES
3. most common in FEMALES IN CHILDBEARING YEARS
4. NOT ENCAPSULATED
5. ASYMPTOMATIC, NORMAL LFTs
6. SULFUR COLLOID IMAGING (nm exam) used to detect FNH
sulfur colloid imaging (5)
1. nuclear medicine exam used to detect FNH
2. in most patients= WARM NODULE
3. warm nodule= FNH mass will absorb sulfur colloid AT THE SAME RATE as normal liver tissue
4. in some patients= HOT NODULE
5. hot nodule= FNH mass will absorb sulfur colloid AT A HIGHER RATE than normal liver tissue
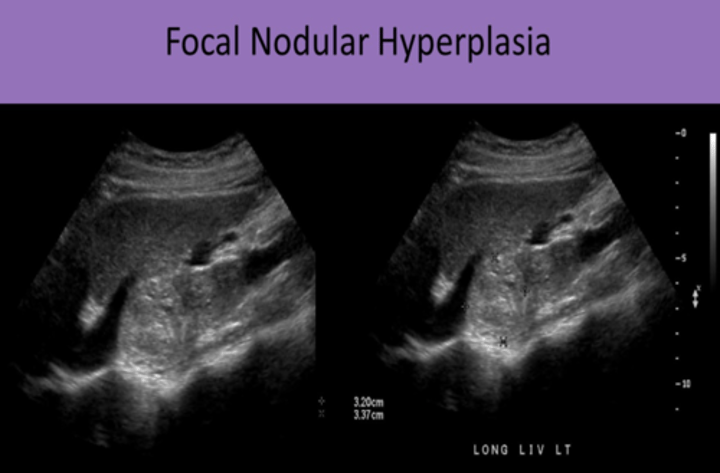
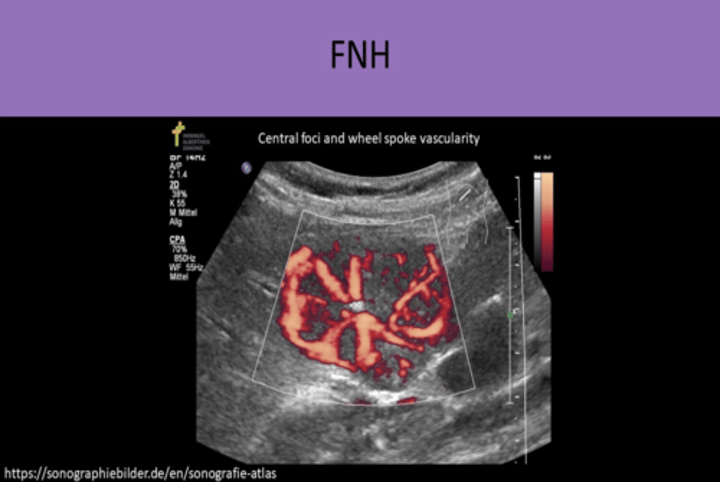
FNH sonographic appearance (7)
1. VARIABLE, can be ISOECHOIC TO LIVER
2. "STEALTH LESION" because it's difficult to differentiate from liver tissue
3. SOLITARY, LESS THAN 5 CM
4. CENTRAL SCAR with RADIAL VASCULARITY
5. looks like SPOKES ON A WHEEL (vascularity starts at a central location and branches radially)
6. mass may DISTORT LIVER SURFACE CONTOUR or may DISPLACE NORMAL BLOOD VESSELS
7. NOT ABLE TO DIAGNOSE ON US ALONE
FNH CONTRAST APPEARANCE (2)
1. CENTRIFUGAL ENHANCEMENT
2. contrast first fills centrally then moves peripherally
ADENOMA CONTRAST APPEARANCE (2)
1. CENTRIPETAL ENHANCEMENT
2. contrast first fills peripherally then moves centrally
liver cell ADENOMA (10)
1. UNCOMMON TUMOR
2. BILE DUCTS and KUPFFER CELL are ABSENT OR FEW IN NUMBER
3. ENCAPSULATED
4. more common in FEMALES
5. STRONG ASSOCIATION WITH ORAL CONTRACEPTIVES
6. also associated with GLYCOGEN STORAGE DISEASE
7. usually ASYMPTOMATIC, but MOST COMMON SYMPTOM is MASS IN RUQ
8. NORMAL LFTs
9. COLD NODULE on sulfur colloid imaging
10. SURGICAL INTERVENTION RECOMMENDED due to risk of hemorrhaging and malignant transformation
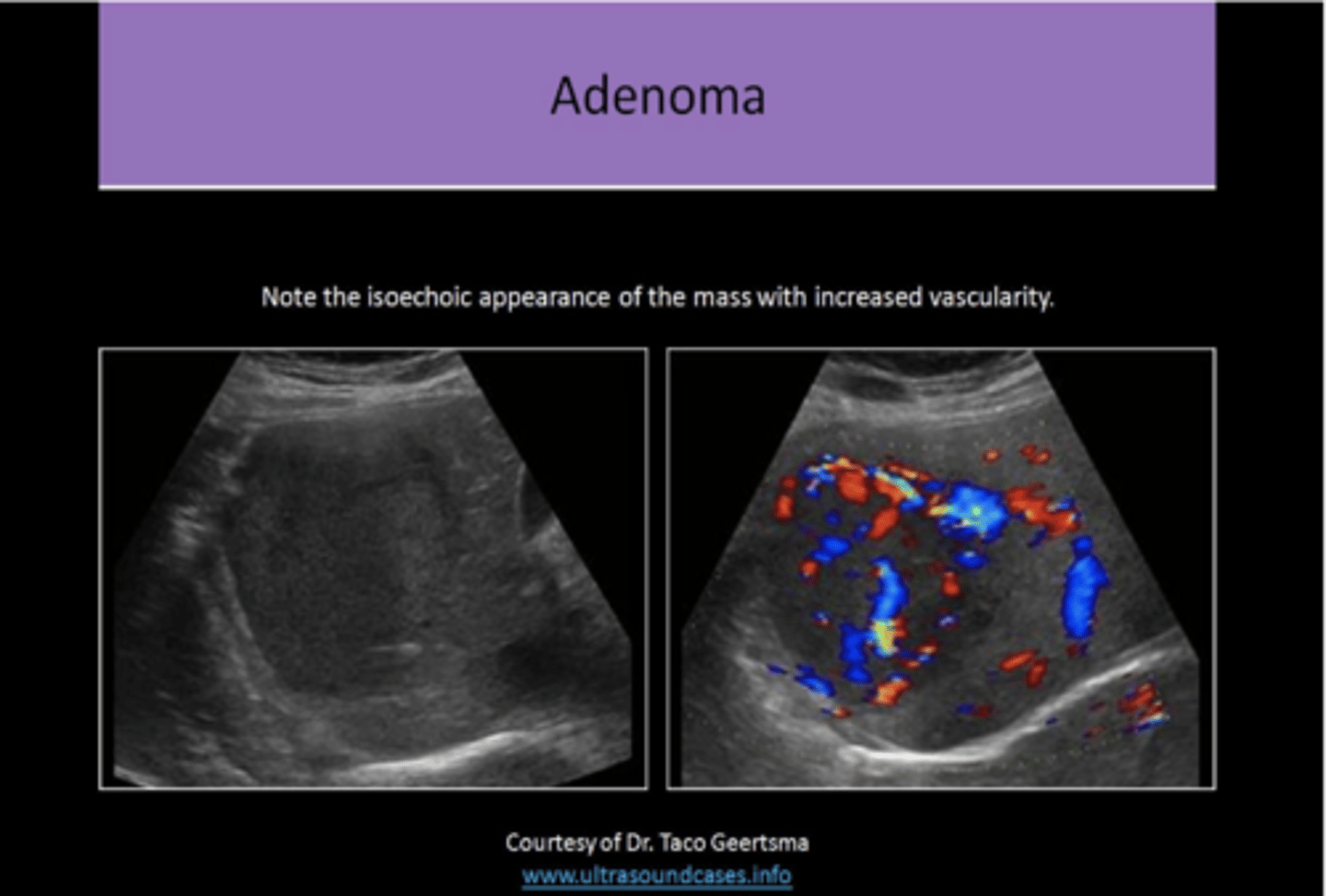
adenoma sonographic appearance (8)
1. KEY FINDINGS= HYPERVASCULAR, WITH OR WITHOUT HEMORRHAGE, IN YOUNG WOMEN ON ORAL CONTRACEPTIVES
2. solitary
3. well defined, solid mass
4. VARYING echogenicity, usually HYPOECHOIC
5. HETEROGENEOUS
6. increased vascularity with possible internal hemorrhage
7. cannot be differentiated from FNH on standard US exam
8. CENTRIPETAL enhancement
hepatic lipoma (6)
1. VERY RARE FINDING
2. associated with TUBEROUS SCLEROSIS
3. HYPERECHOIC
4. may see PROPAGATION SPEED ARTIFACT
5. BROKEN DIAPHRAGM posterior to lesion
6. CT is helpful in determining type of tissue in the hyperechoic mass
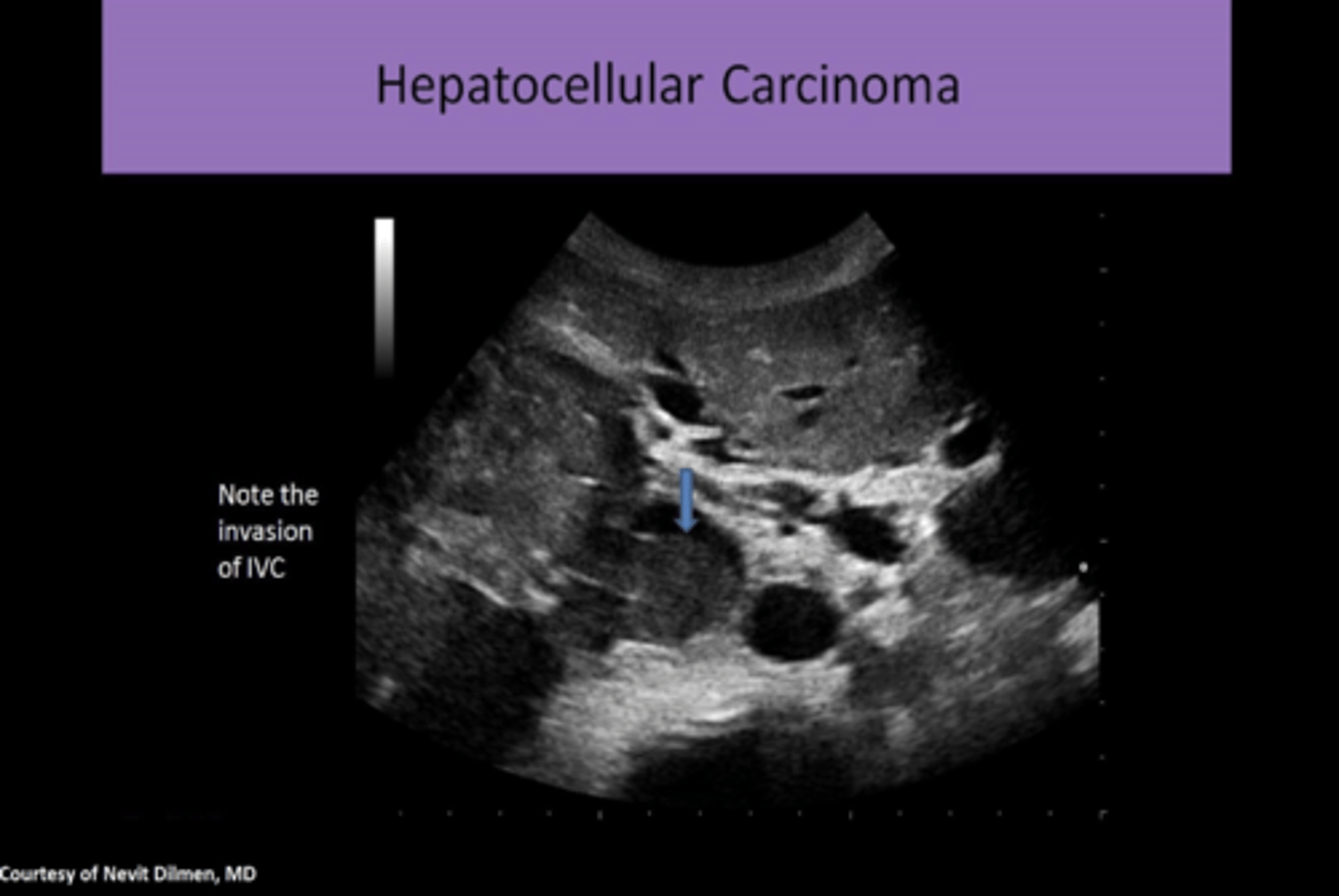
Hepatocellular Carcinoma (HCC) (11)
1. 4TH LEADING CAUSE OF CANCER DEATH
2. MOST COMMON PRIMARY MALIGNANCY of THE LIVER IN ADULTS
3. most common RISK FACTOR IN THE US= CIRRHOSIS
4. 80% of patients have pre-existing cirrhosis
5. also associated with CHRONIC HEPATITIS
6. leads to HEPATOMA FORMATION
7. more common in MALES
8. common COMPLICATIONS include BILIARY OBSTRUCTION, PORTAL HYPERTENSION, AND ASCITES
9. INVADES VENOUS VASCULATURE (HV, PV, IVC), MOST COMMONLY PORTAL VEIN
10. 3-4 MONTH SURVIVAL AFTER DETECTION
11. 1% 5 YEAR SURVIVAL RATE
HCC CLINICAL FINDINGS (5)
1. fever
2. hepatomegaly
3. palpable mass
4. ascites
5. weight loss
HCC LAB FINDINGS (5)
1. increased LFTs
2. AST
3. ALT
4. ALP
5. moderate levels of AFP
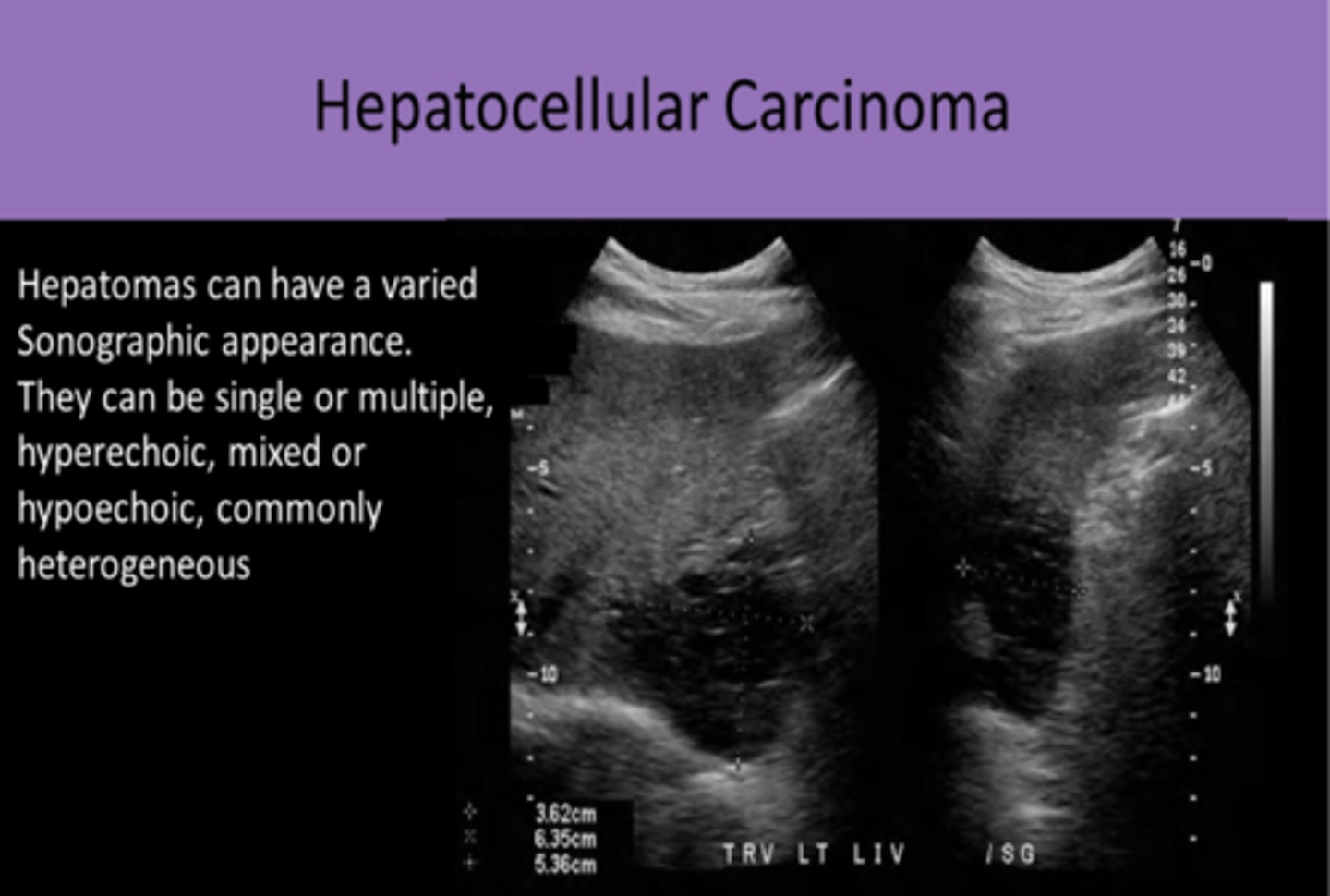
HCC sonographic appearance (11)
1. FOCAL or MULTIFOCAL or DIFFUSE INFILTRATION OF CANCER CELLS
2. SOLID nodules LESS THAN 5 CM
3. VARYING ECHOGENICITY with CENTRAL SCAR
4. as mass ages, FIBROSIS AND NECROSIS CAUSES INCREASED HETEROGENEITY
5. HALO EFFECT (hypoechoic ring surrounding a hyperechoic central area)
6. HYPERVASCULAR
7. PORTAL VENOUS INVASION/THROMBOSIS
8. use COLOR DOPPLER to differentiate tumor invasion from thrombus
9. most malignancies are constantly growing and invading so this requires CONSTANT CONTINUOUS FLOW THROUGHOUT THE CARDIAC CYCLE
10. HIGH VELOCITY FLOW WITH INCREASED DIASTOLIC FLOW (low resistance waveform)
11. CONTRAST US- enhancement in arterial phase (areas of absence of contrast in the arterial phase correspond with areas of NECROSIS) and washout in portal venous phase
Ultrasound Liver Imaging Reporting and Data System (US LI-RADS)(3)
1. standardized system for imaging technique, interpretation, reporting, and data collection
2. US screening and surveillance in patients at risk for developing HCC
3. CEUS LI-RADS incorporates standards related to CONTRAST US eval in patients at risk for developing HCC
Fibrolamellar Carcinoma (5)
1. SUBTYPE OF HCC found in ADOLESCENTS AND YOUNG ADULTS WITH NO COEXISTING LIVER DISEASE
2. NORMAL AFP
3. usually SOLITARY mass that can grow quite LARGE (6-22 cm)
4. WELL DIFFERENTIATED AND USUALLY ENCAPSULATED
5. PUNCTATE CALCIFICATION AND A CENTRAL SCAR help to differentiate from hepatoma
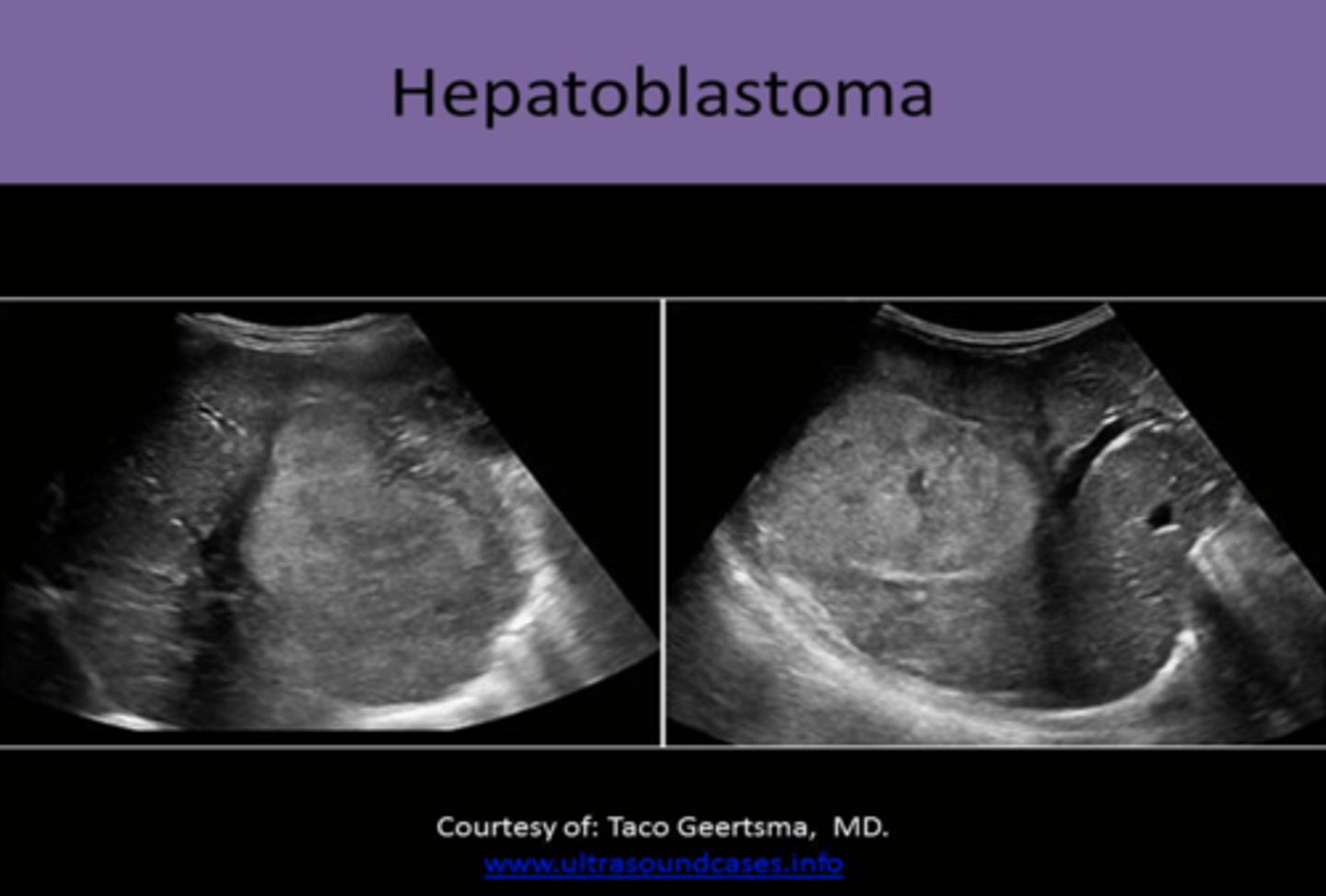
Hepatoblastoma (4)
1. #1 PEDIATRIC PRIMARY LIVER MALIGNANCY
2. usually occurs BEFORE AGE 2
3. GENETIC
4. associated with BECKWITH-WIEDEMANN SYNDROME or FAMILIAL ADENOMATOUS POLYPOSIS
hepatoblastoma clinical findings (3)
1. abdominal enlargement
2. palpable mass
3. hepatomegaly
hepatoblastoma lab findings (2)
1. abnormal LFTs
2. increased AFP
hepatoblastoma sonographic appearance (4)
1. SOLID, ECHOGENIC mass
2. may have some CYSTIC PORTIONS/SEPTATIONS
3. may contain CALCIFICATIONS
4. tendency to INVADE HEPATIC AND PORTAL VEINS
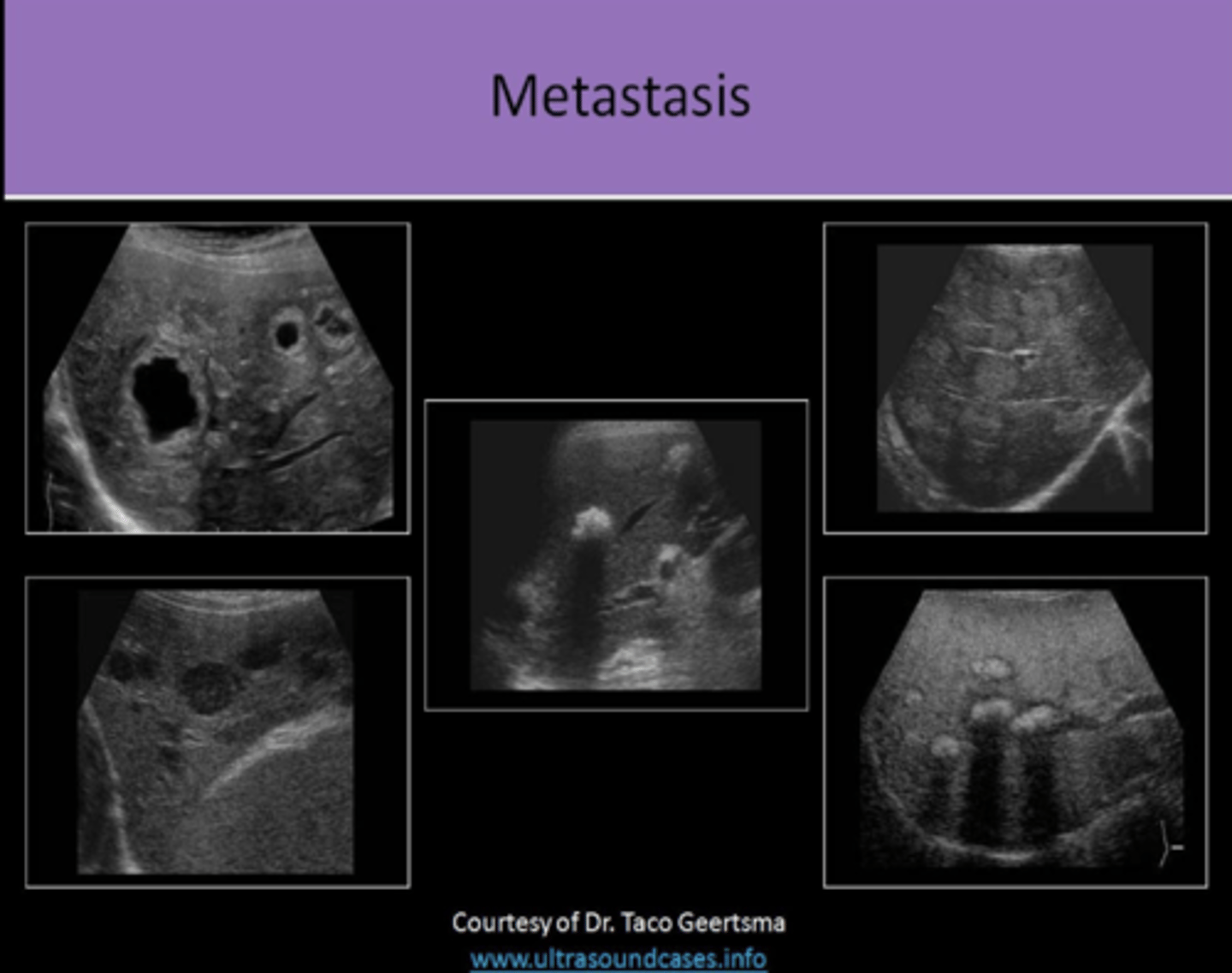
Metastatic Liver Disease (6)
1. LIVER IS #1 SITE
2. 20x MORE COMMON THAN PRIMARY LIVER CANCER
3. common primaries= GI TRACT (#1), PANCREAS, BREAST, LUNG, OVARY
4. primary cancers metastasized to the liver are carried by the PORTAL VEIN
5. contrast U/S will demonstrate rapid CONTRAST WASHOUT in the portal venous phase
6. sonographic appearance can suggest the origin of the primary tumor, but biopsy is required for diagnosis

metastatic liver disease clinical findings (6)
1. RUQ pain
2. weight loss
3. ascites
4. jaundice
5. palpable mass
6. nausea/vomiting
metastatic liver disease lab testing (4)
1. increased LFTs
2. increased ALP
3. increased AFP
4. increased DIRECT BILIRUBIN
metastatic liver disease sonographic appearance (12)
1. MULTIPLE masses
2. VARY IN SIZE
3. NECROSIS AT CENTER OF LESION as the blood supply is outgrown
4. if halo sign is identified around a liver mass, it should create strong suspicion of malignancy
5. HYPERECHOIC lesions usually related to GI TRACT PRIMARY OR HCC
6. HYPERECHOIC lesions WITH HYPERVASCULARITY usually related to RENAL CELL CARCINOMA
7. HYPOECHOIC lesions usually related to LYMPHOMA, LUNG, OR BREAST PRIMARY
8. CYSTIC lesions associated with SARCOMA
9. BULL'S EYE appearance UNCOMMON AND NONSPECIFIC, but usually related to LUNG OR COLON PRIMARY
10. CALCIFIED lesions usually related to MUCINOUS ADENOCARCINOMA OF THE COLON
11. INFILTRATED PATTERN related to BREAST, LUNG, AND MELANOMA PRIMARIES
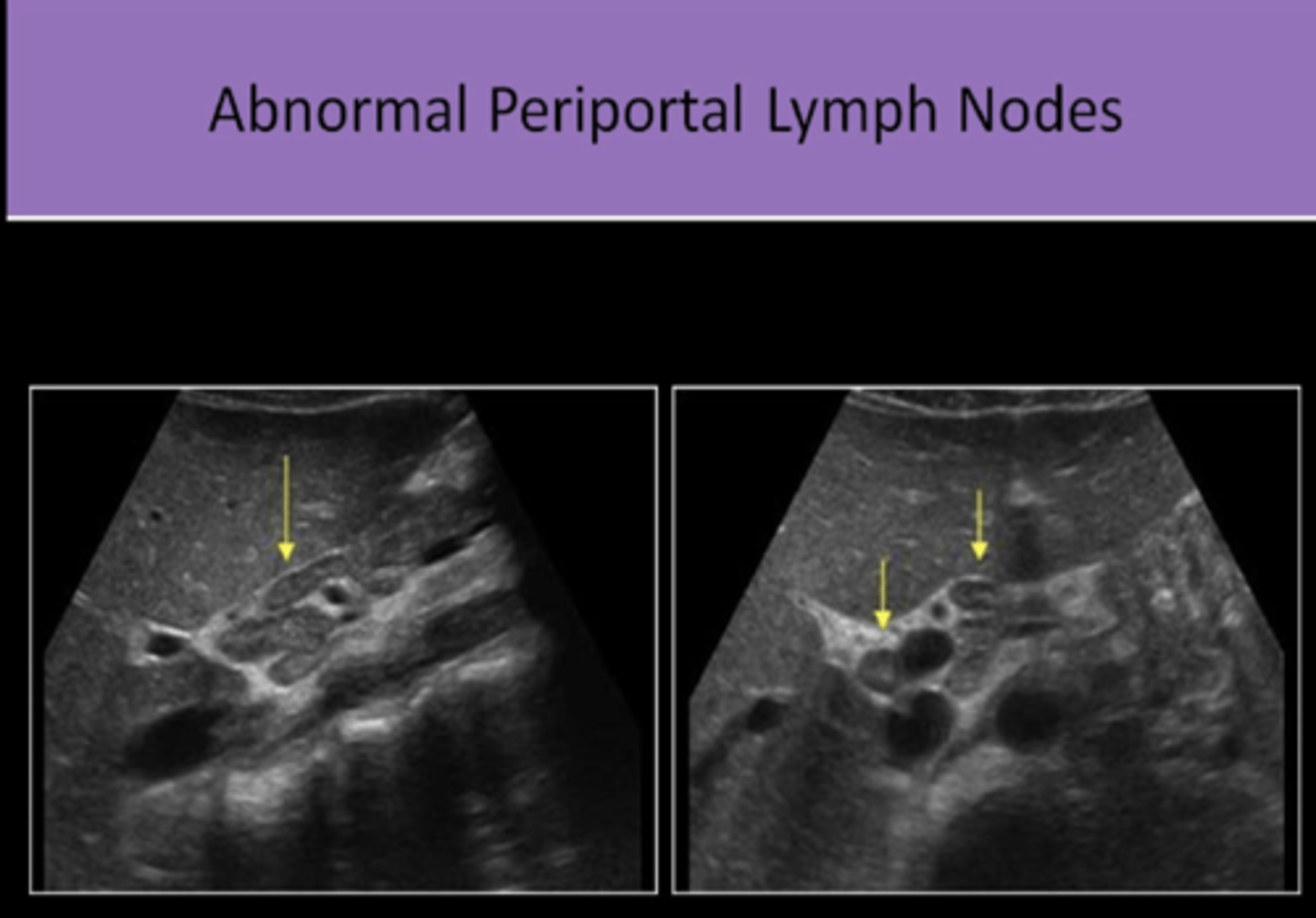
12. ABDOMEN should be evaluated for LYMPHADENOPATHY
patient history of a primary cancer in body + liver mass with halo
usually LIVER METASTASIS
patient history of chronic liver disease + liver mass with halo
usually HCC
potential area for ABN LYMPH NODES (4)
1. para-aortic
2. at the splenic hilum
3. at the renal hilum
4. at the porta hepatis
Kaposi Sarcoma (3)
1. malignancy of CONNECTIVE TISSUE in the body
2. may also involve= SKIN, LUNGS, GI TRACT, OTHER ORGANS
3. MOST COMMON LIVER MALIGNANCY SEEN IN PATIENTS WITH HIV/AIDs
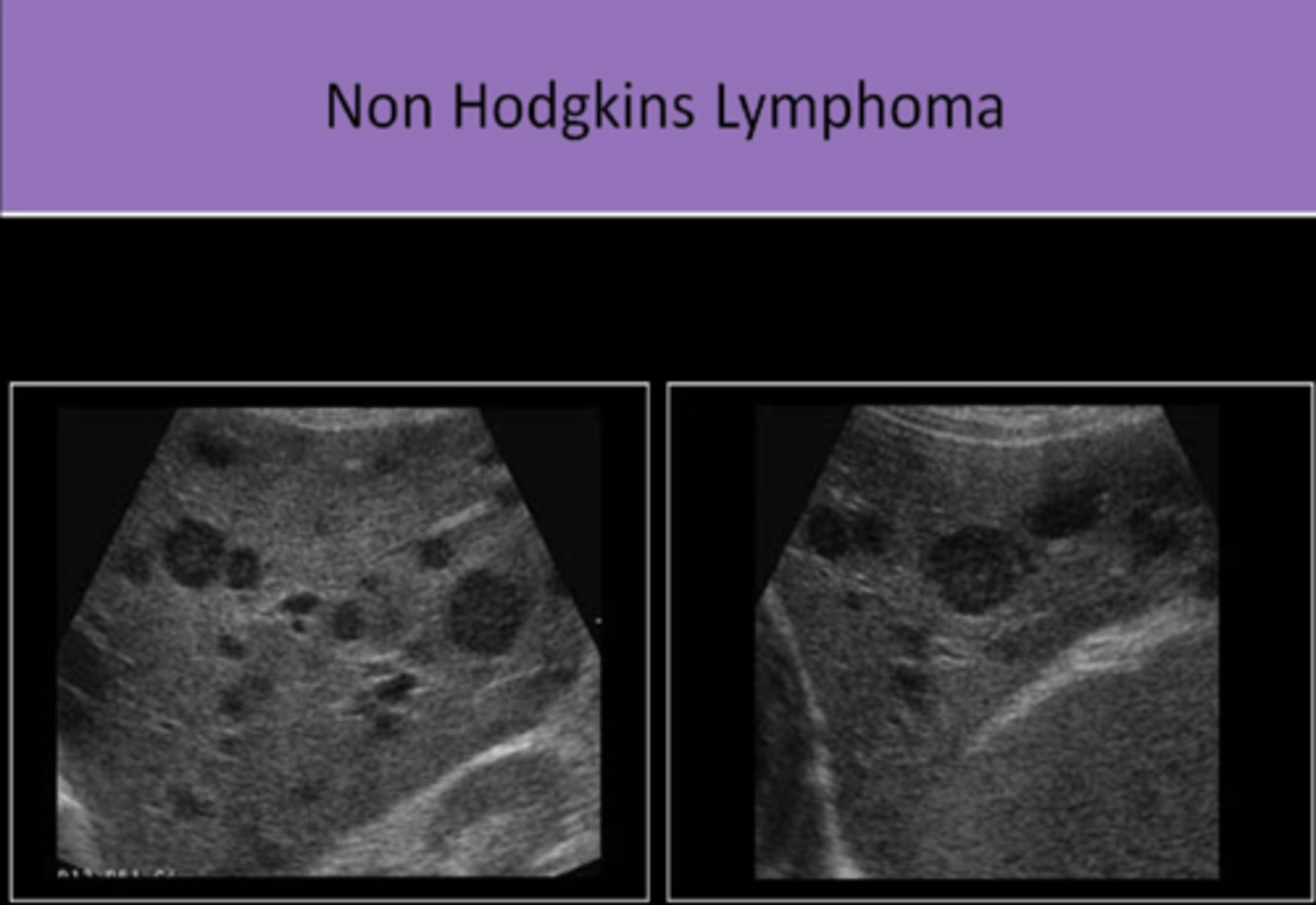
lymphoma (5)
1. malignancy of the LYMPHATIC SYSTEM
2. commonly associated with HIV/AIDs
3. SOLID
4. may be SINGLE OR MULTIPLE
5. HYPOECHOIC and/or COMPLEX appearance