Parkinson’s disease
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
is a progressive neurologic disorder that primarily affects movement à characterized initially by unilateral hand tremor that progresses to include bilateral tremor, rigidity, bradykinesia, and postural instability
Decrease patient’s quality of life and increase dependence
Parkinson disease (PD)
Dopamine is a brain neurotransmitter that regulates voluntary movement, reward-seeking behavior, memory/learning, attention, sleep, affect, and many other functions
Dopamine and acetylcholine must be balanced to produce smooth movement à when dopamine neurons are degenerated, acetylcholine signaling is increased, causing an imbalance that contributes to the clinical manifestations of PD
Pathophysiology
Unknown heredity or combination of genetics and environmental toxins, and/or sporadic
Etiology
Increased age
Gender
Environmental factors
Heredity/genetic mutation
Risk Factors
No definitive way to prevent
suggested prevention techniques: Reduce caffeine, healthy diet
Prevention
Symptoms of PD are mild at beginning; gradually worsen over time
Motor symptoms include 4 “classic symptoms” à tremor, rigidity, bradykinesia, and postural instability
Nonmotor symptoms include cognitive deficits, emotional changes, and sleep problems
Clinical Manifestations
5-10% of individuals with PD have “early-onset” (or “young-onset”) PD in which onset begins before the age of 40
Women with early onset may need referral
Lifespan Considerations
Motor symptoms begin unilaterally progresses bilaterally
Tremor early sign of PD
Most prominent at rest
“pill-rolling” motion à thumb and fingers gently rub together
Tremors of hands, arms, legs, jaw, and face can occur with disease progression
Tremors may worsen with stress or excitement
Motor Symptoms
Rigidity (resistance to movement) involuntary contraction of muscles. Muscles remain contracted instead of relaxing which prevents movement. Leads to muscle aches or weakness
Muscle stiffness of trunk and limbs, Limits ROM, causes pain, Passive ROM causes short jerky movements (Cogwheel)
Bradykinesia (slowed movement)
Voluntary - ADLs, bathing, dressing
Automatic: Arms may not swing, Blink rate, Stand from seat position, Steps become shorter, Difficulty with speech/swallowing/chewing, Hypophonia
Motor Symptoms Rigidity and Bradykinesia
Postural instability: stooped posture that leads to balance problems and falls. Retropulsion-topple backward
Parkinsonian gait: small, shuffling steps; steps may be characterized by bradykinesia, or steps may be rapid as if the patient is trying to run (festination). When walking, the whole foot typically strikes the ground simultaneously (or the toes strike first)
Freezing → individual with PD feels as though feet are stuck to the floor; can increase risk of falling forward
Parkinsonism
Festination - patient is not going anywhere but it looks like they are trying to go fast
Motor Symptoms Parkinsonism
Sleep problems - Insomnia, Daytime sleep attacks, Restless leg syndrome, Parasomnias
Non-motor symptoms
No cure for PD, chronic progressive disease
Treatment requires a multidisciplinary approach:
Nursing
Primary Care Provider
Neurologist
Physical Therapy
Occupational Therapy
Collaboration
Physical examination
Neurological examinations
Medical history
Sign and Symptoms
Dopamine Transporter Scan(Da T scan)
Rule out - CT scan, MRI, Blood tests
Diagnostic Tests
injection of radioactive iodine binds to dopamine transporters in the brain; allows visualization of dopaminergic neurons à patients with degeneration of dopamine neurons will show less uptake of radioactive iodine; results are evaluated by trained neurologist
DaT scan
Advanced disease
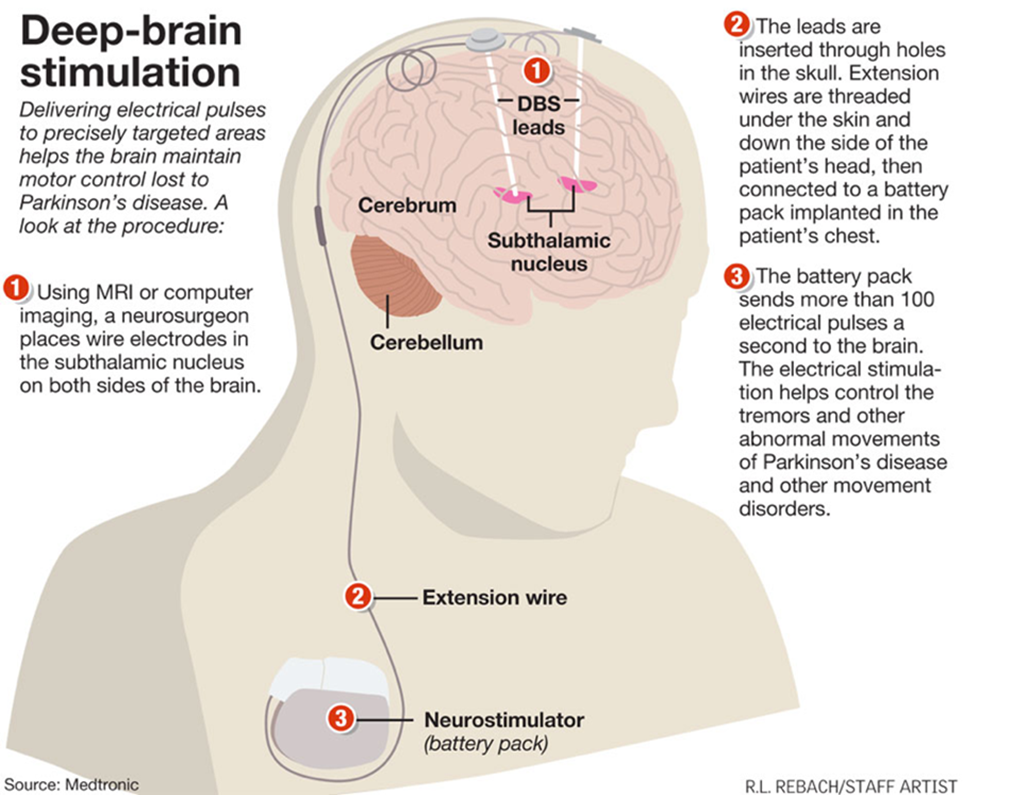
Deep brain stimulation (DBS) is most common surgical procedure à neurostimulator and electrodes are implanted into patient to send electrical signals to one of three brain regions: Subthalamic nucleus, Globus pallidus, Thalamus
Pallidotomy or Thalamotomy may also be used
Surgery
Allows patients to decrease dosage of levodopa medication à decrease side effects such as dyskinesia
Complications of surgical procedure: hemorrhage, infection, stroke
Complications of DBS: misplacement/dislodging of leads, component failure, and stimulation-related side effect
Deep Brain Stimulation
No pharmacologic cure is available for PD à reducing severity of symptoms
Goals of pharmacologic treatment are to: Improve the quality of life, Reduce disability, Maintain ability to work
Medications: Levadopa/Carbidopa (increases dopamine, reduces tremors. Effectiveness decreases over time and can cause diskinesia), Dopamine Agonists, MAO-B Inhibitors (can be given early, enhance Levadopa), COMT Inhibitors (slow breakdown of Levadopa in brain, increase availability), Anticholinergics- benztropine (Cogentin) (reduce tremor and rigidity, brings cdocolin back down, side effects: dry mouth, confusion)
Pharmacologic Therapy
Exercise is most important, especially combination of walking and strength training. Exercises that promote flexibility, balance, and posture (i.e., yoga, t’ai chi)
Physical Therapy (helps with grooming/cooking), Occupational Therapy (helps with cooking), Speech Therapy (swallowing/talking)
Nonpharmacologic Therapy
It is essential for nurses to:
Evaluate progression of patient’s PD
Monitor ability of ADLs and ambulate independently. Patient teaching and emotional support
Nursing Process
Observation, patient interview, physical exam
Affect, mood, and speech pattern, presence and degree of tremor, note movement and characteristics of posture and gait
Past medical history and current complaints/symptoms, ADLs, assistive devices, effectiveness of medication regimen, sleeping habits, and memory issues
Noticing/Assessment
Actual or potential problems may include:
Impaired mobility, impaired swallowing, impaired verbal communication, impaired sleep pattern, risk for injury/falls
Goals for patients with PD may include:
Maximize functioning and mobility, remain free from injury/falls, participate in speech therapy to improve speech pattern and swallowing function
Identifying problems and planning care

Optimize Mobility
Best strategy for mobility is encouraging patient to walk daily and participate in an exercise program
Aerobic exercises and strength training increase muscle strength, balance, and coordination
ROM exercises increase joint mobility and function, and help prevent contractures
For patients who cannot ambulate independently nurse or caregiver should help patient walk several times daily
Participation in Physical and Occupational Therapy is vital for helping patients with PD maintain mobility as long as possible
Nurses should: Providing ongoing emotional support and encouragement is essential à as disease progresses, patients can experience fear, anxiety, and depression
Promote independence
Deficits in performing ADLs is a major burden for patients with PD, as well as their caregivers
Use of assistive devices is key to helping patients maintain independence in performing ADLs (i.e., shower seat, eating utensils with large handles, electric toothbrush, reachers/grippers)
Vocal training may be provided by Speech Therapy for patients with voice changes
Nursing Interventions
Routine assessments using the UPDRS to determine patient’s level of disability significant changes in the UPDRS score may indicate need for modification of pharmacologic, nonpharmacologic, or surgical therapy
Individuals with PD who have been taking levodopa for a long time may notice changes in effectiveness of the medication, or may experience intensified side effects as dosage is increased routinely assess patient’s understanding of medication regimen, potential side effects, and efficacy of drugs
As disease advances and symptoms intensify, patients may experience hopelessness and depression routinely evaluate patient’s emotional status and make referrals as necessary
Assess patient’s support system and resources at each stage of disease progression and make appropriate referrals
Evaluation