Exam 1: (condensed) Validity Testing, Mesenteric Doppler, Liver Doppler, Liver Pathologies, Liver Transplant, Renal Doppler, Renal Transplant
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
Gold Standard for Vascular Imaging
Angiography
Validity
Ability of a test to distinguish between who has the disease and who does not
Sensitivity
Ability of test to correctly detect patients with disease compared to the gold standard - positive sonogram with positive gold standard
Specificity
Ability of test to correctly detect patients without disease compared to the gold standard - negative sonogram with negative gold standard
Positive Predictive Value (PPV)
Probability that a positive test result reflects the actual presence of disease
Portion of patients with a positive test that have disease
Negative Predictive Value (NPV)
Probability that a negative test result reflects the actual absence of disease
Portion of patients with a negative test that do not have disease
Accuracy
Degree of closeness of a test result to the actual value
Percentage of overall correct results
Must lie between sensitivity & specificity and PPV & NPV
Reliability
Consistency of obtaining similar results under similar conditions - reflects accuracy over time
Increasing Cut-Off Values
Improves specificity
More true negatives
Decreasing Cut-Off Values
Improves sensitivity
More true positives
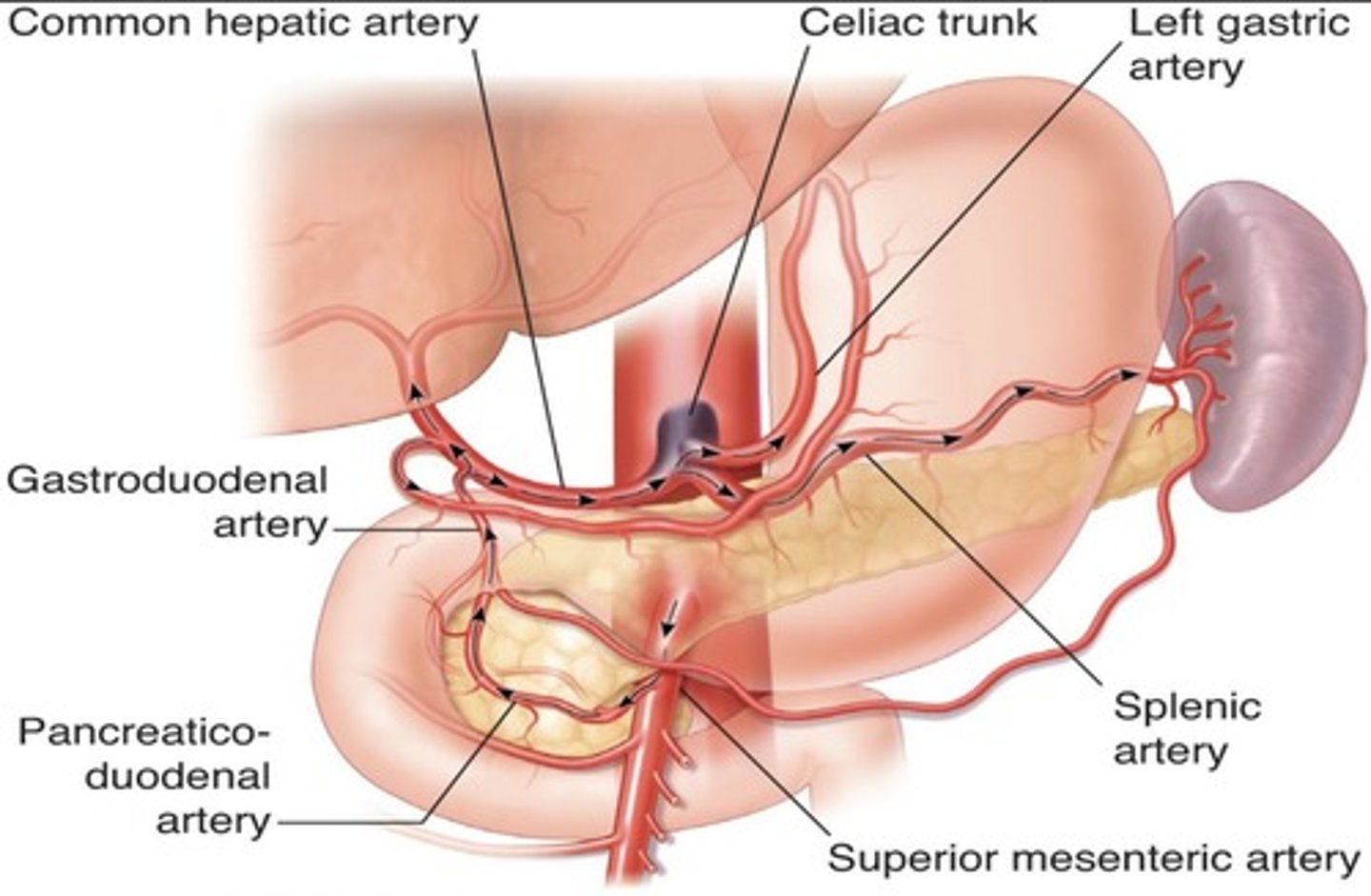
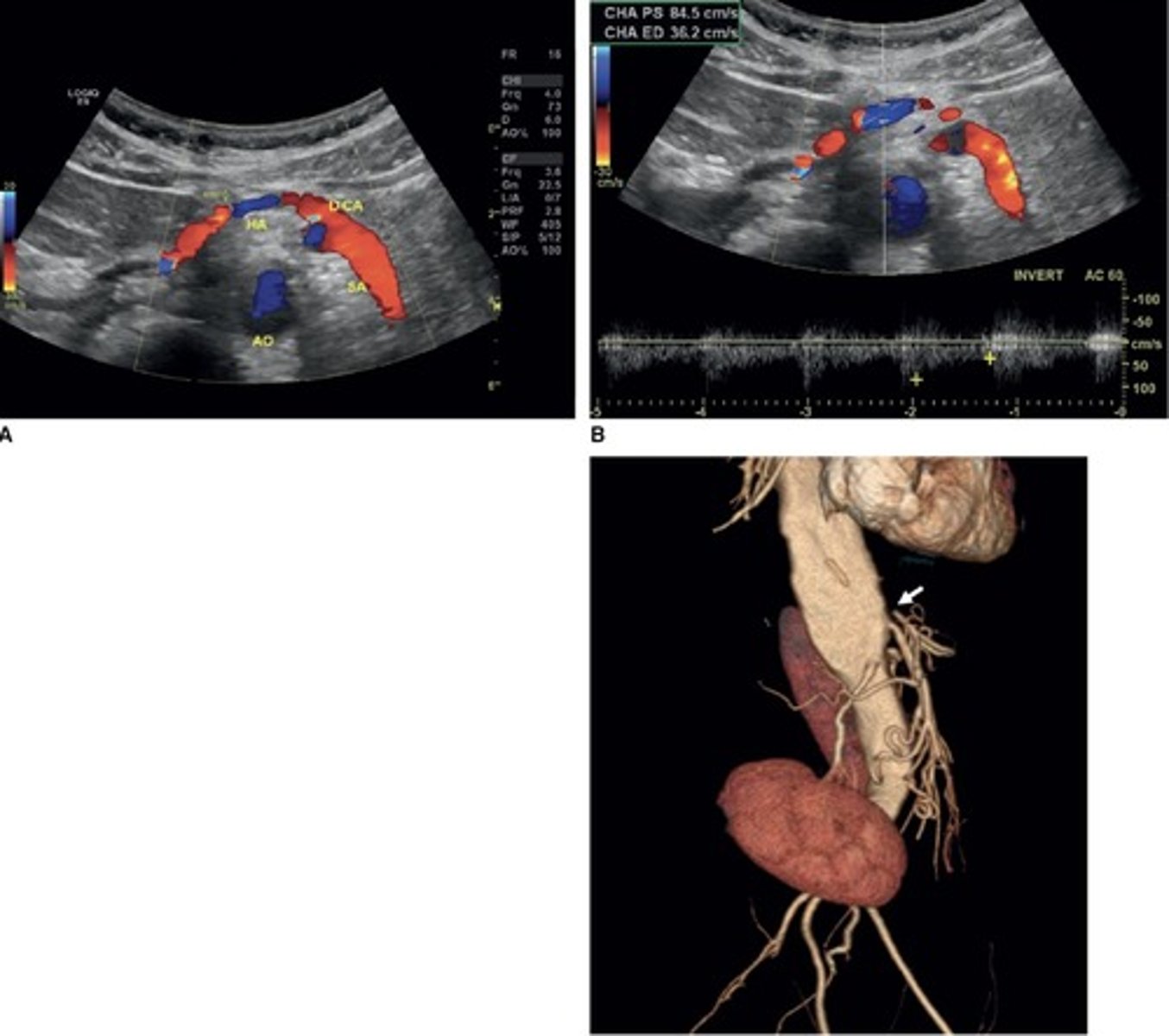
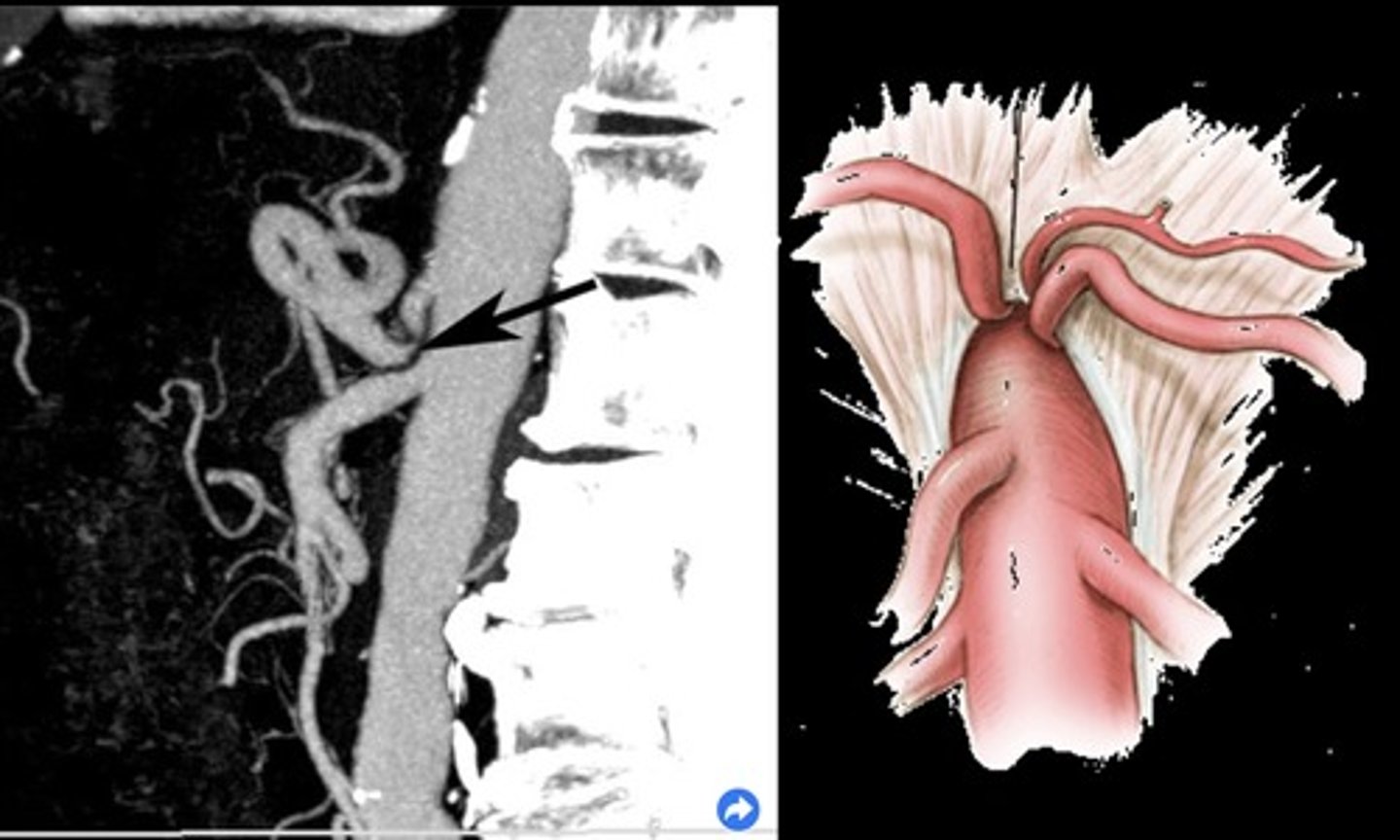
Celiac Artery Occlusion
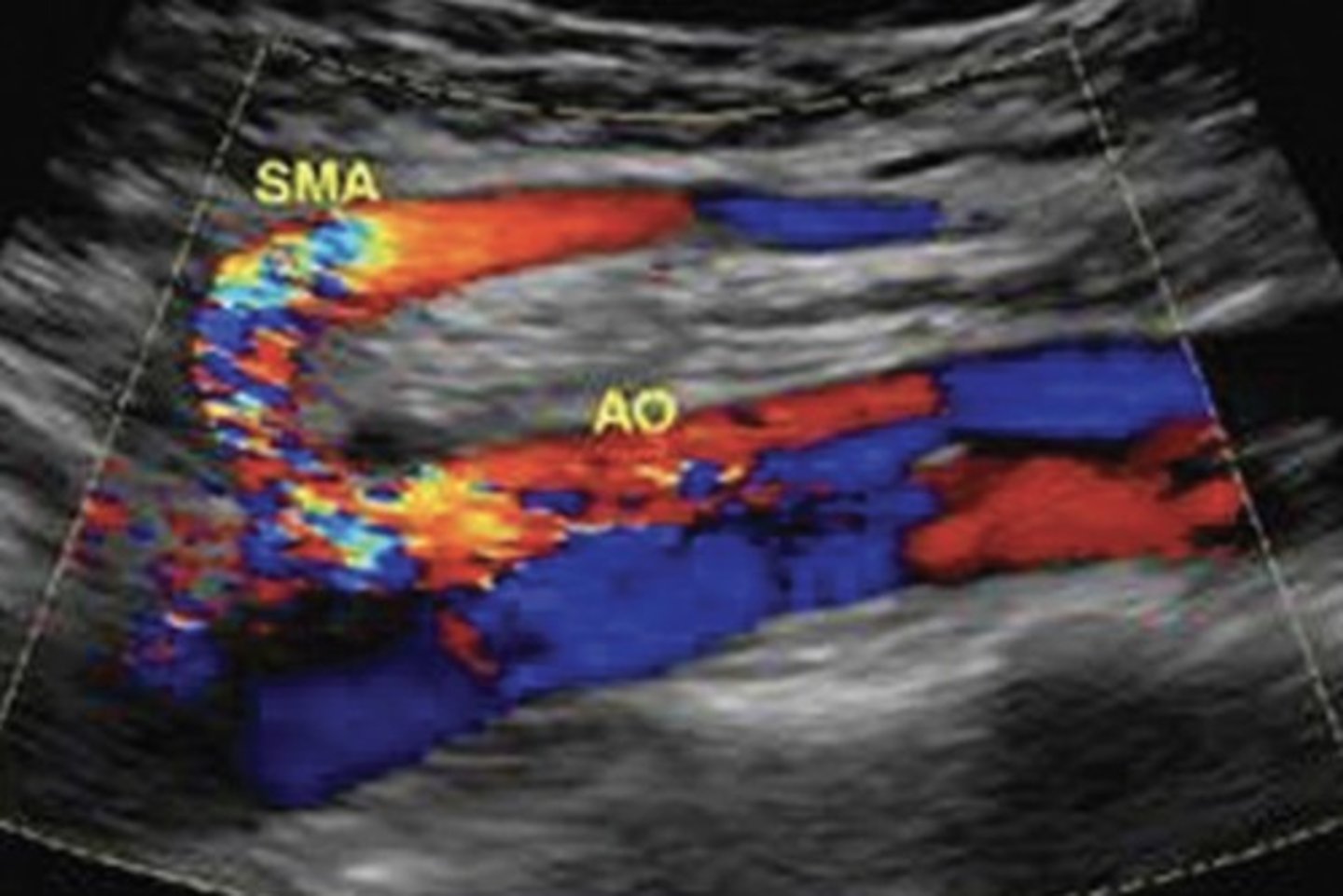
Results in SMA collaterals diverting blood through gastroduodenal artery toward the liver and spleen
Replaced Right Hepatic Artery
Right hepatic artery branches off something else besides celiac artery - usually SMA
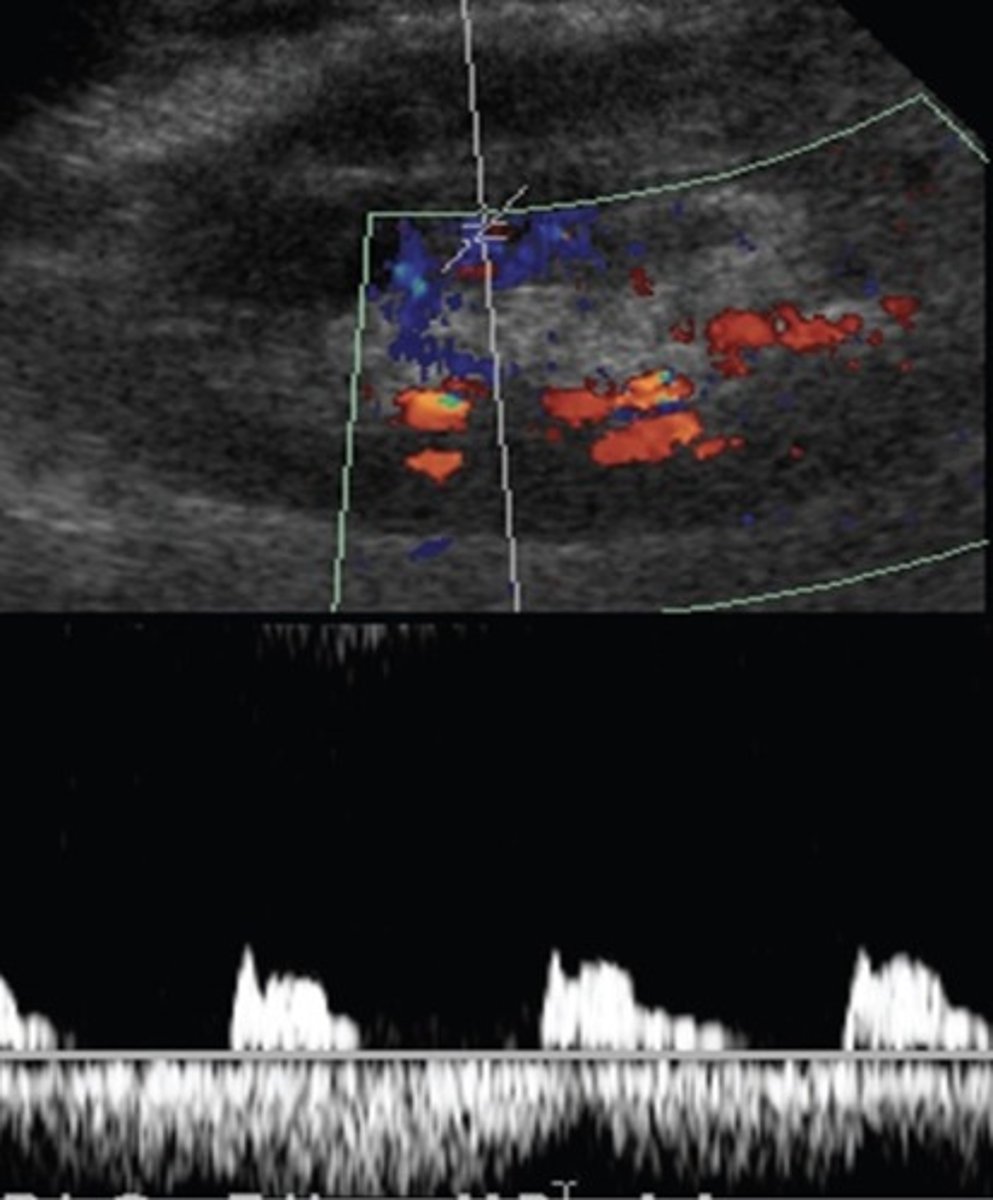
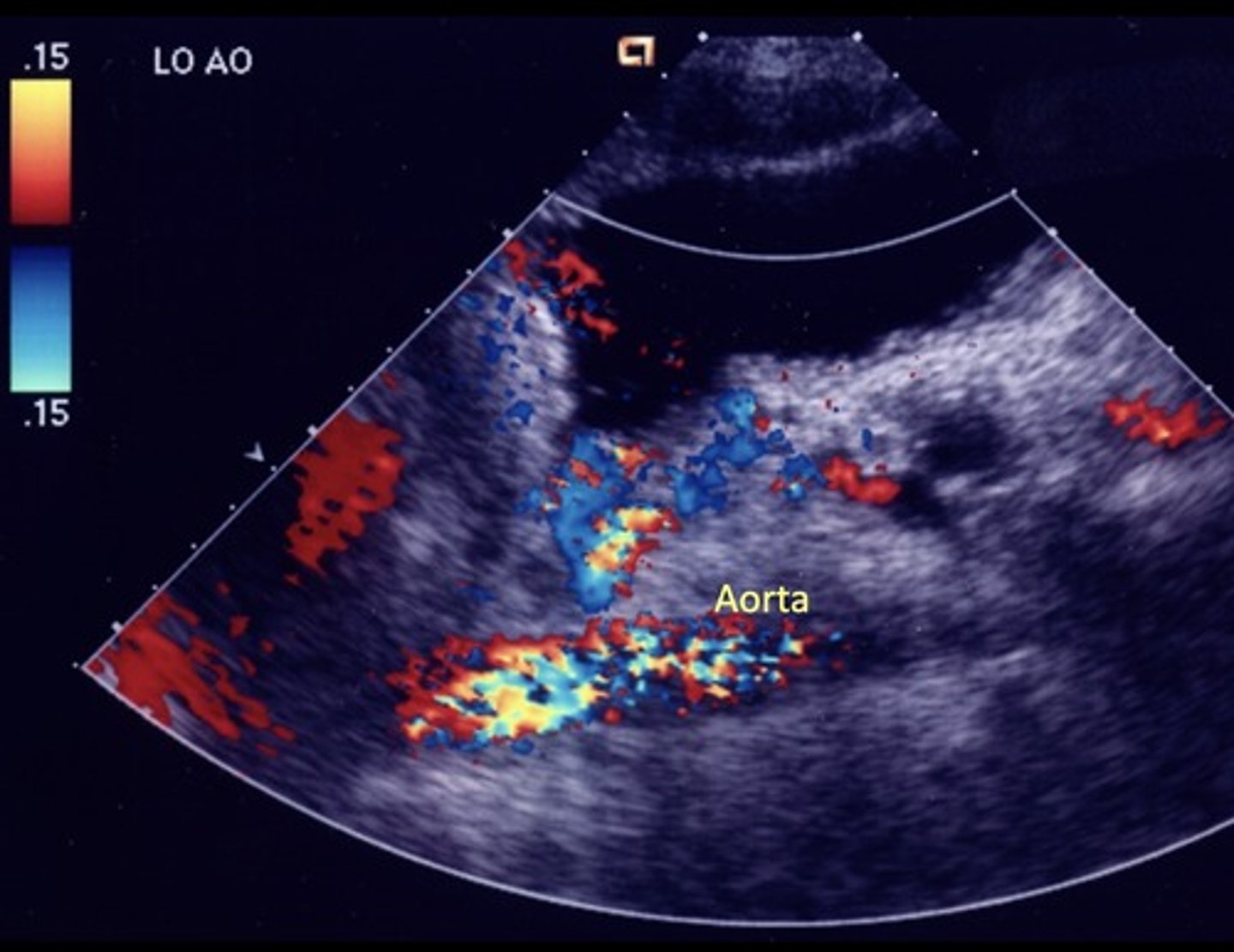
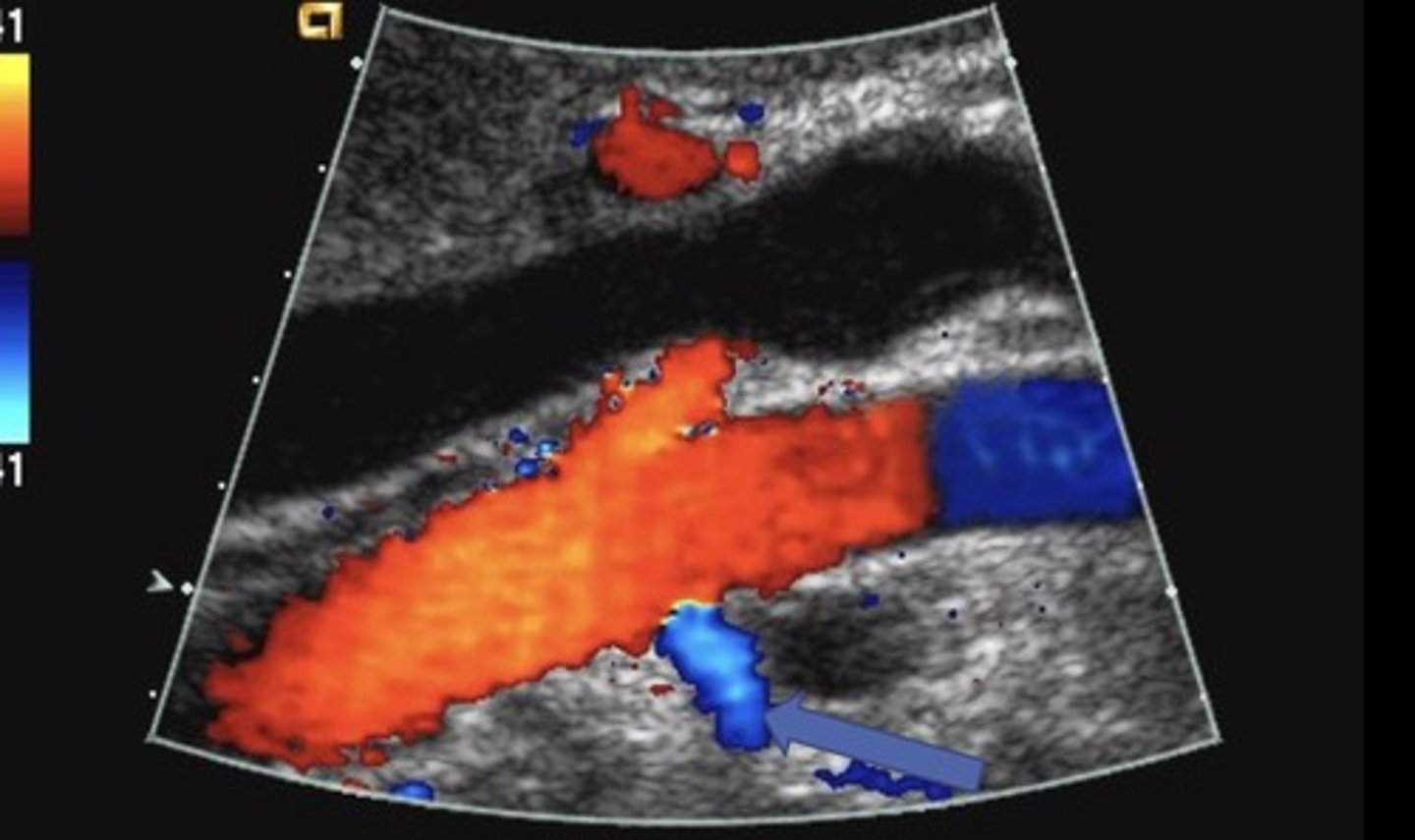
Hepatic Artery Retrograde Flow
Due to celiac artery occlusion
Blood flows towards splenic artery - RABT color pattern
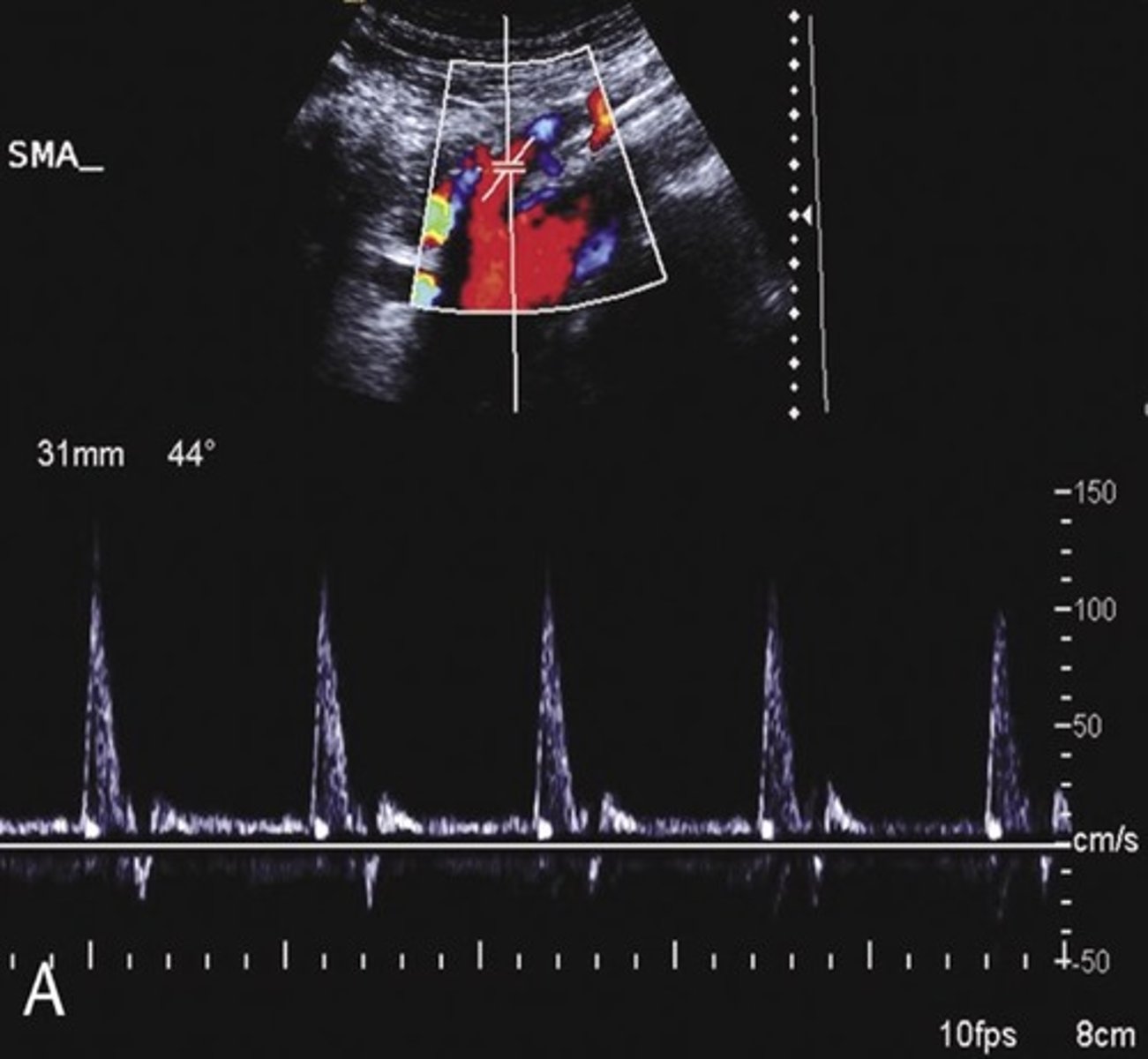
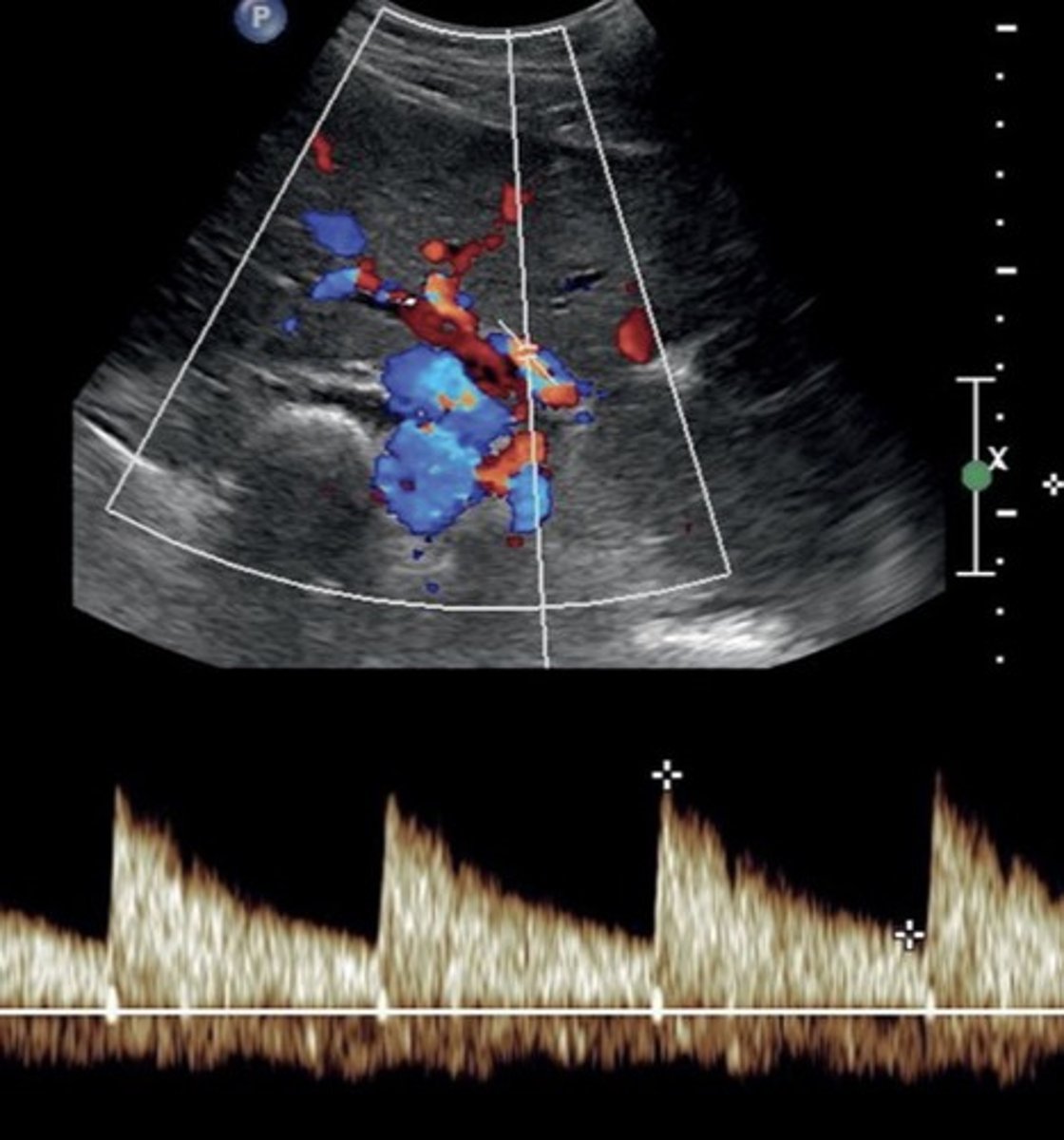
Pre-Prandial SMA Doppler
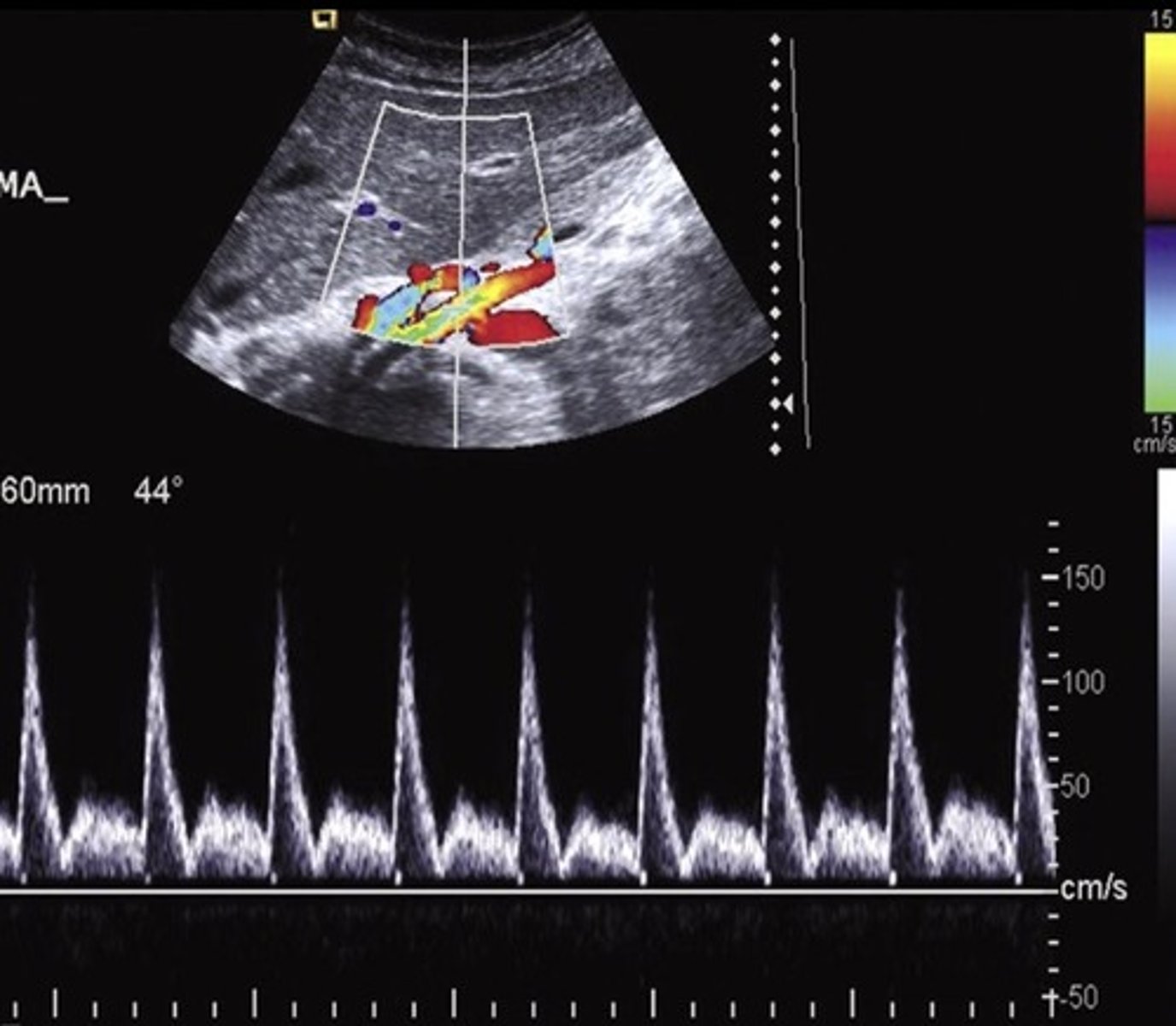
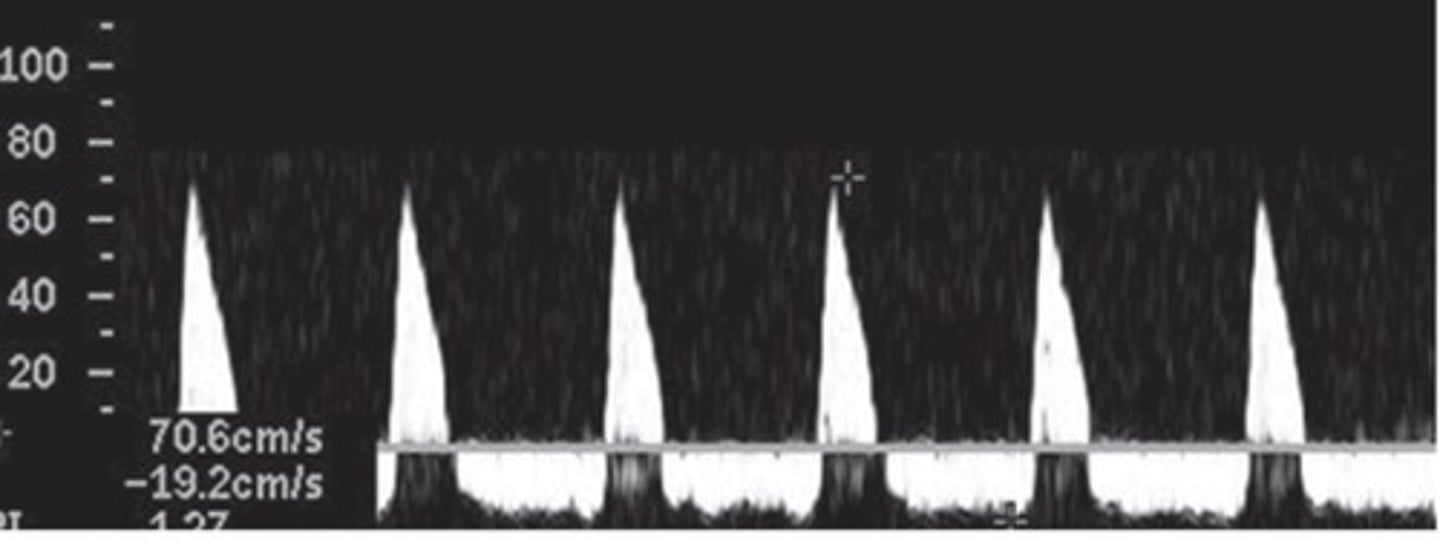
Post-Prandial SMA Doppler
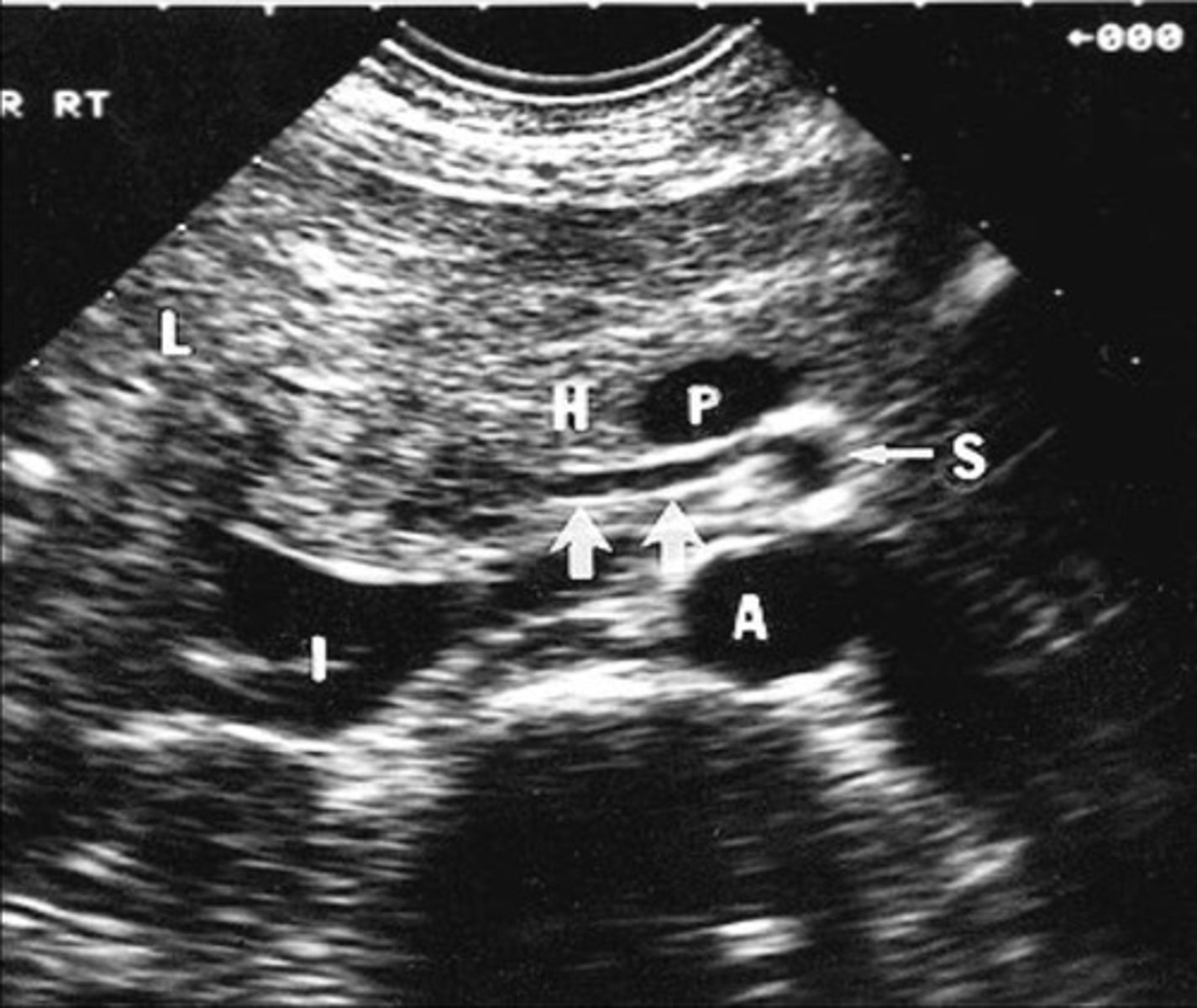
Common Trunk Variant
Celiac and SMA come off common trunk
Prominent IMA
Due to SMA occlusion
Acute Mesenteric Ischemia
Thrombosis of one or more mesenteric vessels
Life threatening - requires immediate intervention
Severe cramping/pain - disproportional pain
Chronic Mesenteric Ischemia
Low resistant pre-prandial doppler signals
70% occlusion of 2/3 splanchnic arteries required for diagnosis (celiac, SMA, IMA)
Epigastric pain after eating - fear of food, weight loss, decreased nutrition
Compensatory Flow
Elevated velocities in normal collateral vessels
No stenotic profile seen
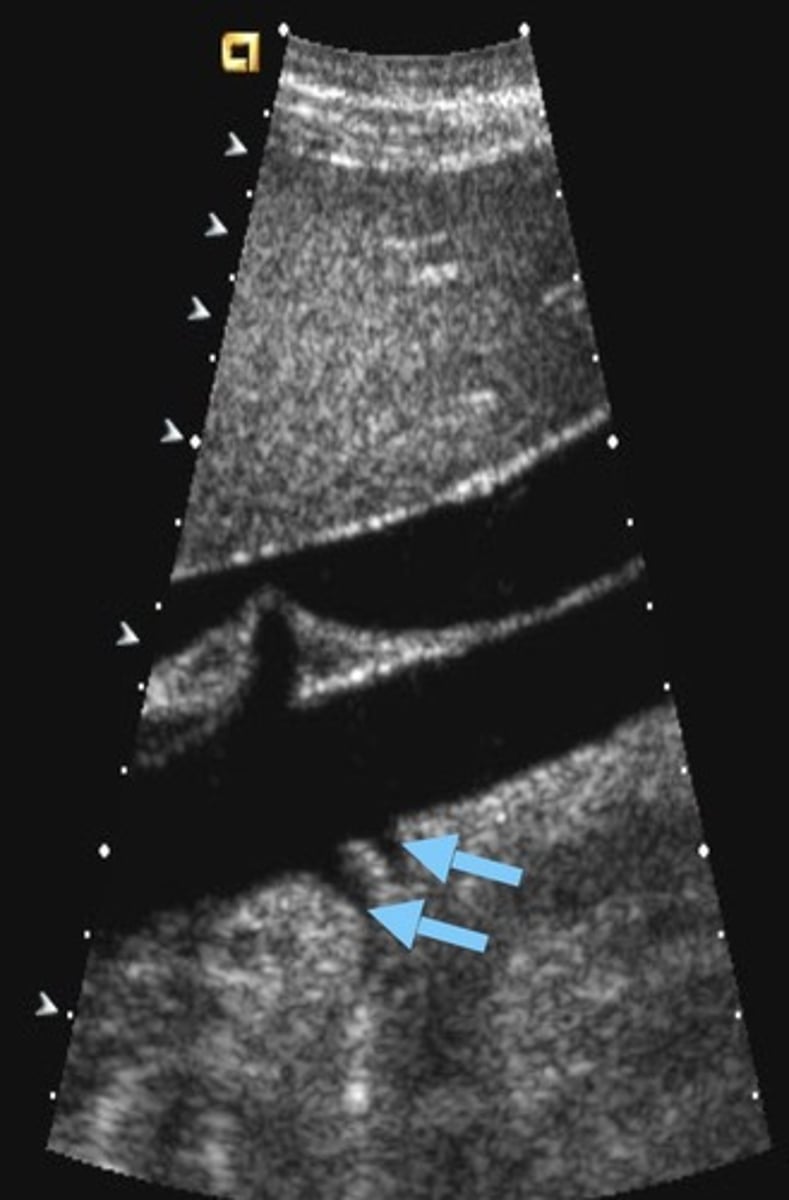
Dissection
Separation of channels - flap line
To and fro flow
Median Arcuate Ligament Syndrome (MALS)
Compression of celiac axis during exhalation by median arcuate ligament
Pain relieved by inhalation
Evaluate in supine & upright positions and with inspiration & expiration
Pre-Hepatic/Inflow Vessels
Portal Vein
Hepatic Artery
Intrahepatic/Sinusoidal Vessels
Sinusoids/capillaries
Hepatocytes
Post-Hepatic/Outflow Vessels
Central Veins
Sublobular Veins
Hepatic Veins
IVC
Left Gastric Vein (coronary vein) Doppler Flow
Hepatofugal
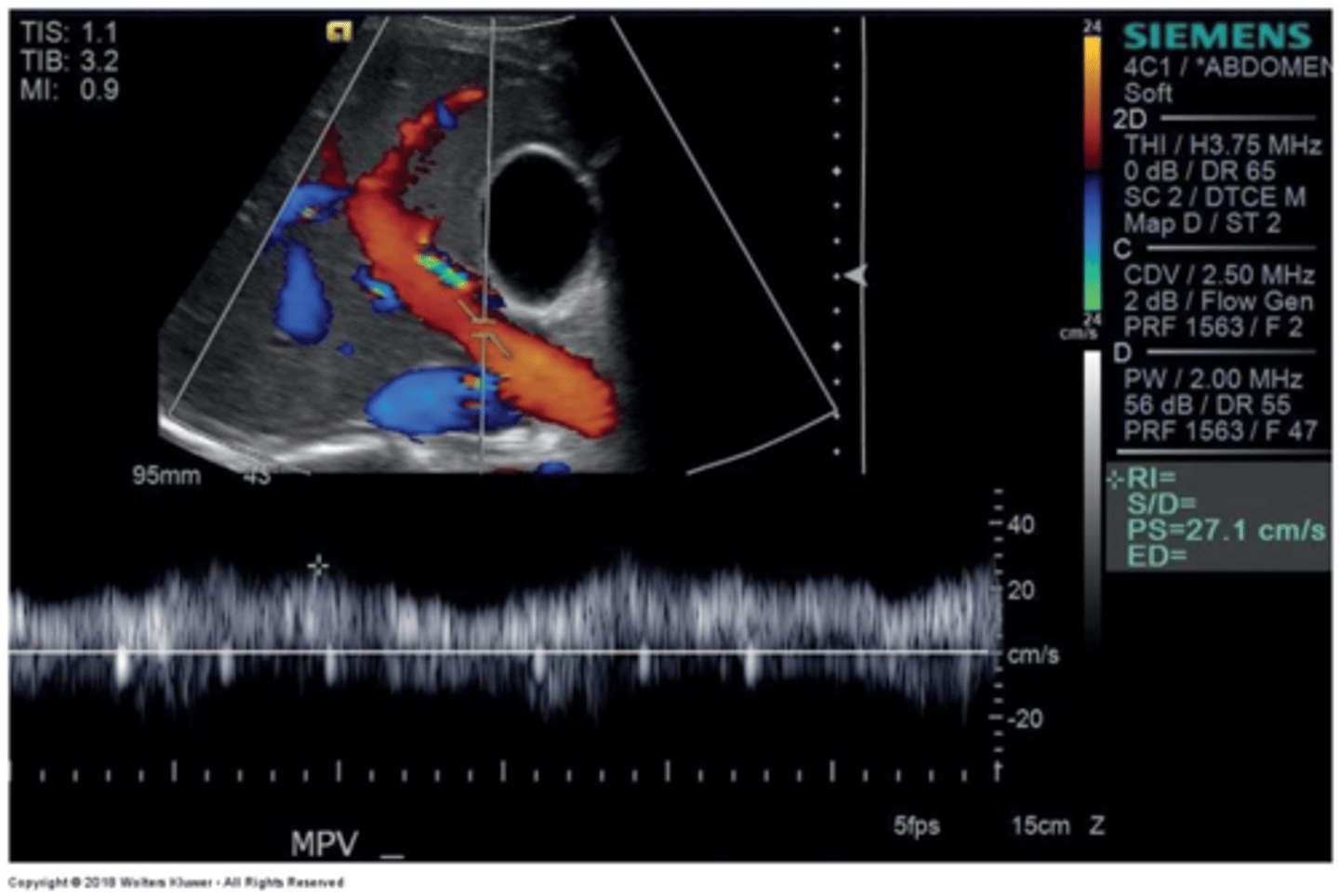
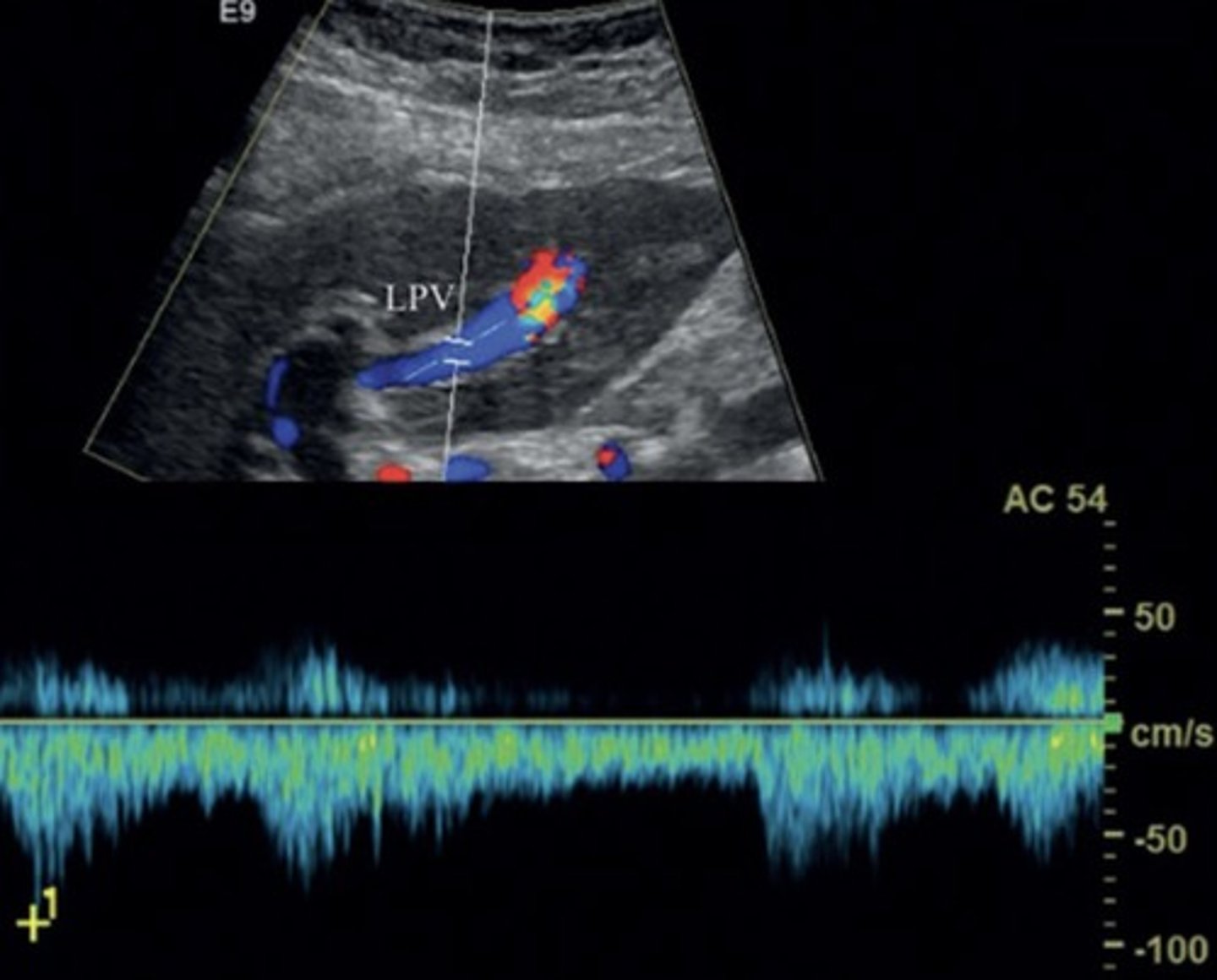
Main Portal Vein Doppler Waveform
Monophasic continuous waveform
Hepatopetal flow (antegrade flow)
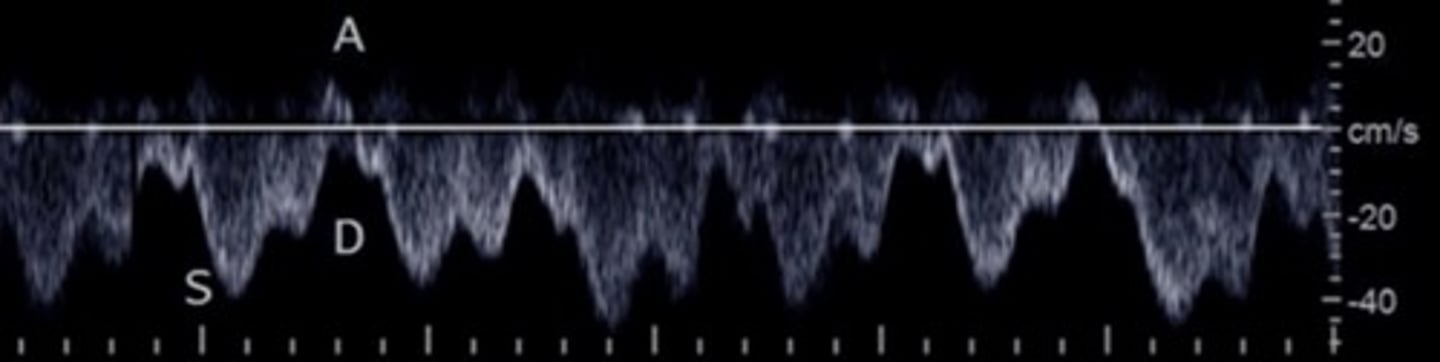
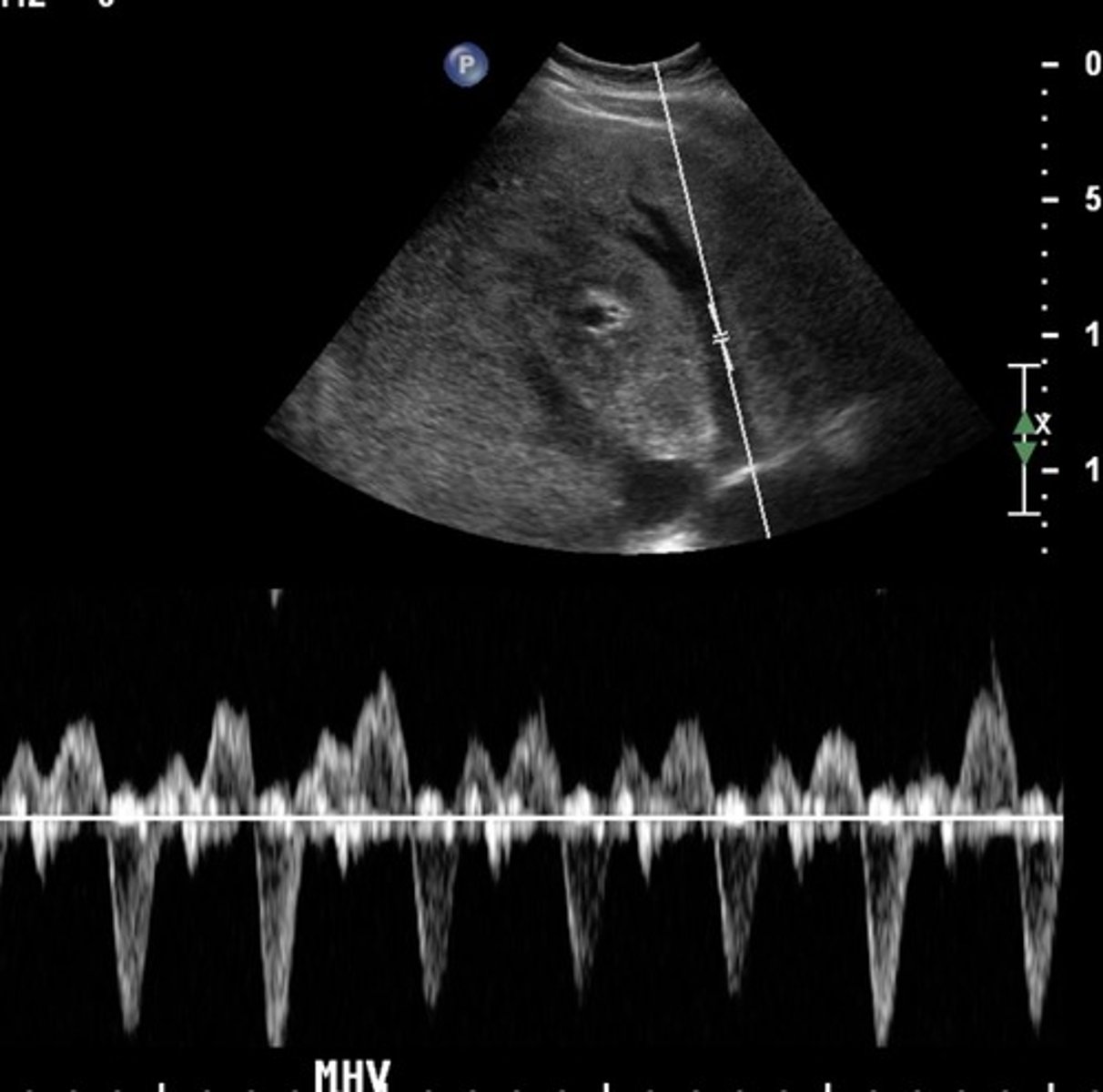
Hepatic Vein Doppler Waveform
Triphasic
Antegrade & retrograde flow - cardiac pressure changes
Hepatic Vein Doppler
S wave: ventricular systole
D wave: atrial filling
A wave: atrial contraction
Inspiration depresses systolic wave
Exhalation augments systolic wave
Valsalva diminishes pulsatility
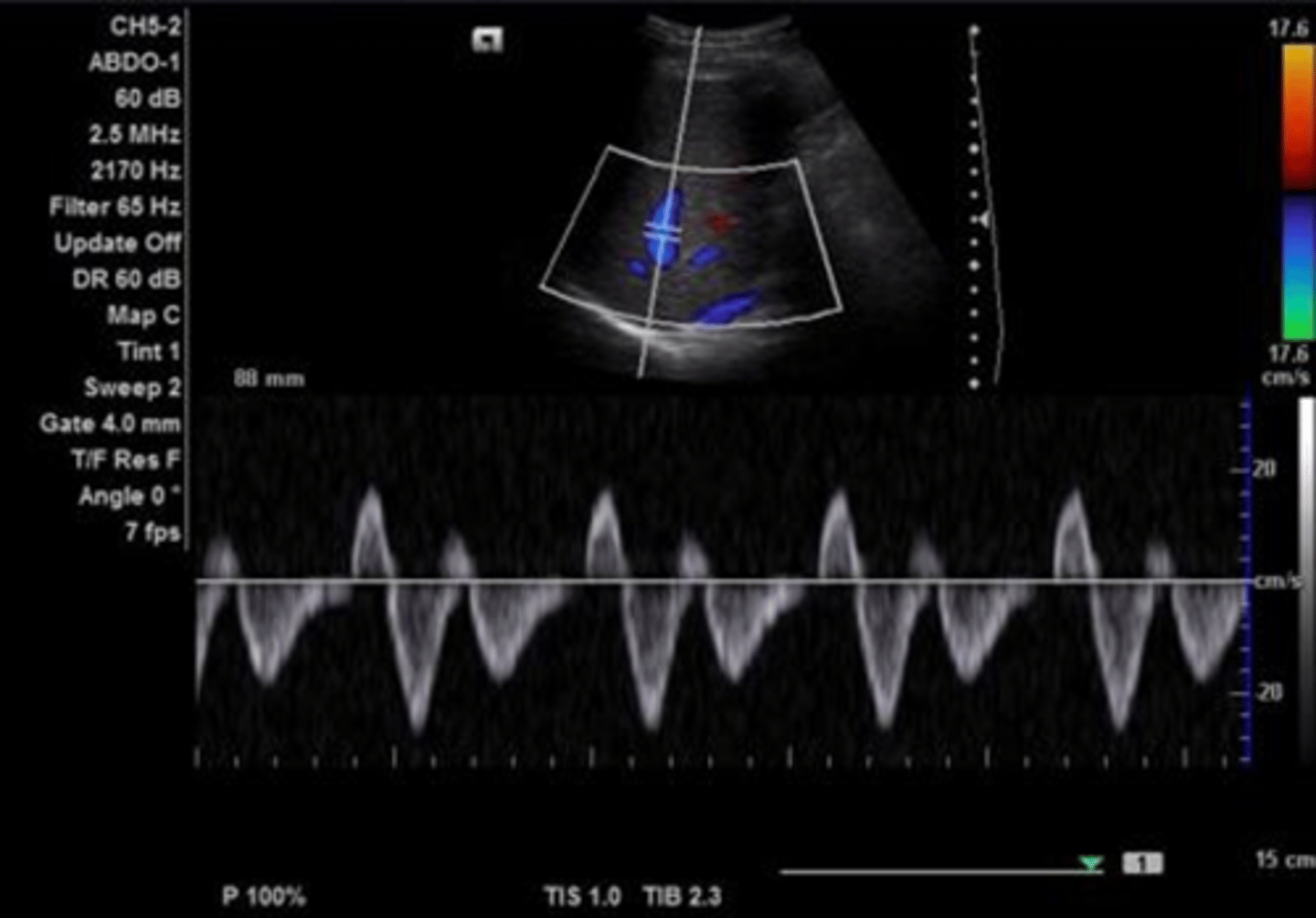
Hepatic Artery Doppler Waveform
Hepatopetal
Low resistant monophasic pan-diastolic forward flow
Hepatic Buffer Response
When PV flow increases, HA flow decreases (post-prandial)
Splenic Vein Doppler Waveform
Hepatopetal flow
Continuous monophasic with slight respiratory variation
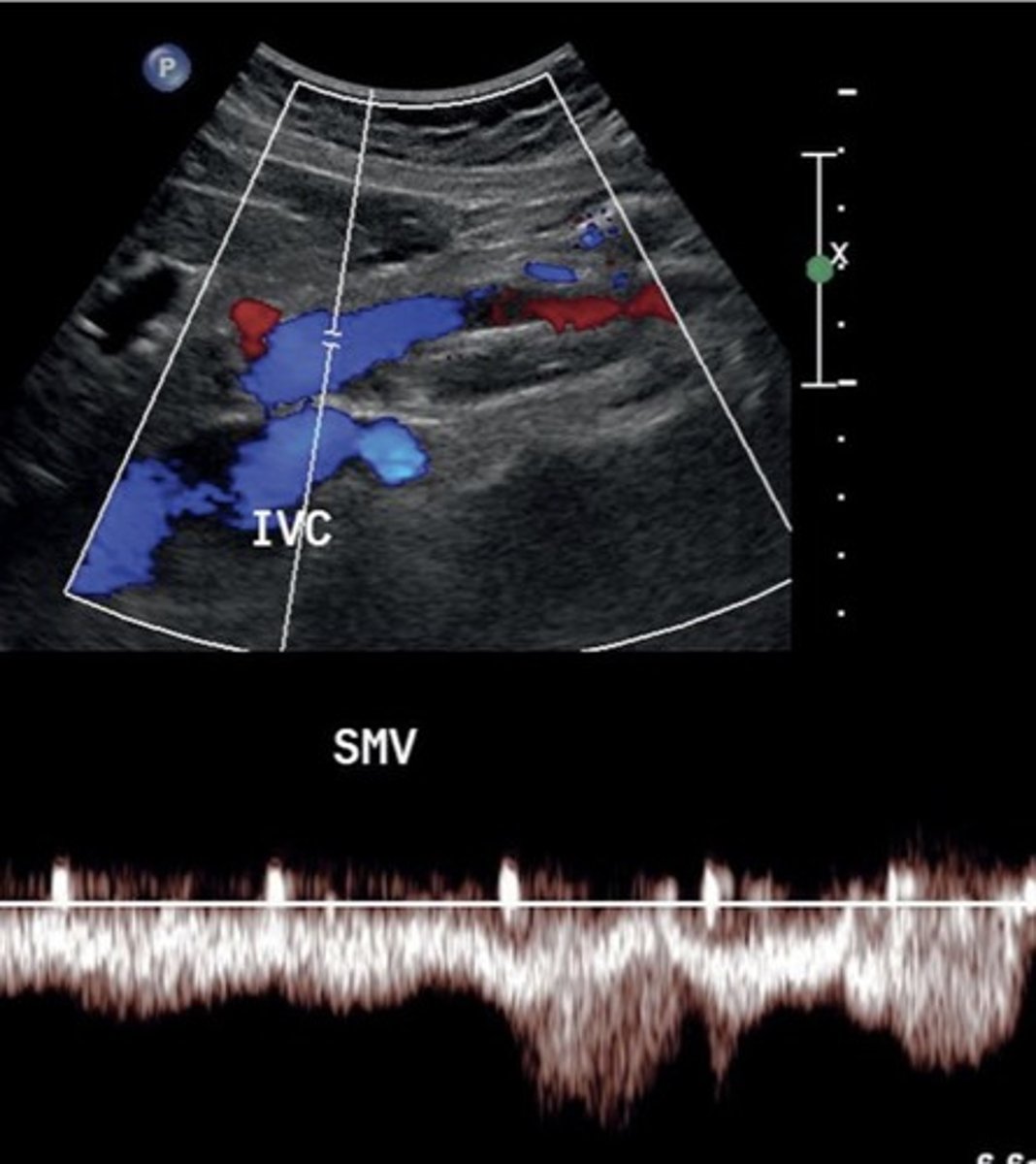
SMV Doppler Waveform
Hepatopetal flow
Continuous monophasic with slight respiratory variation
Portal HTN
Increased pressure in portal venous system
Not diagnosed with spectral Doppler -> diagnosed with gray scale & color
Causes of Portal HTN
Hepatitis C
Hepatitis B
Alcoholic cirrhosis
Primary Biliary Cirrhosis
Autoimmune Hepatitis
Hereditary Hematochromatosis
Schistosomiasis
Portal HTN 2D Findings
Large pulmonary vein
Collaterals
Splenomegaly
Ascites
Enlarged hepatic artery
Portal HTN Doppler Findings
Slow, hepatofugal flow in portal vein
Cirrhosis
End-stage liver disease
Cirrhosis Findings
Portalization of hepatic veins
Collaterals
Hepatofugal flow in portal vein & splenic vein
Coronary Vein Collateral
Can lead to esophageal varices
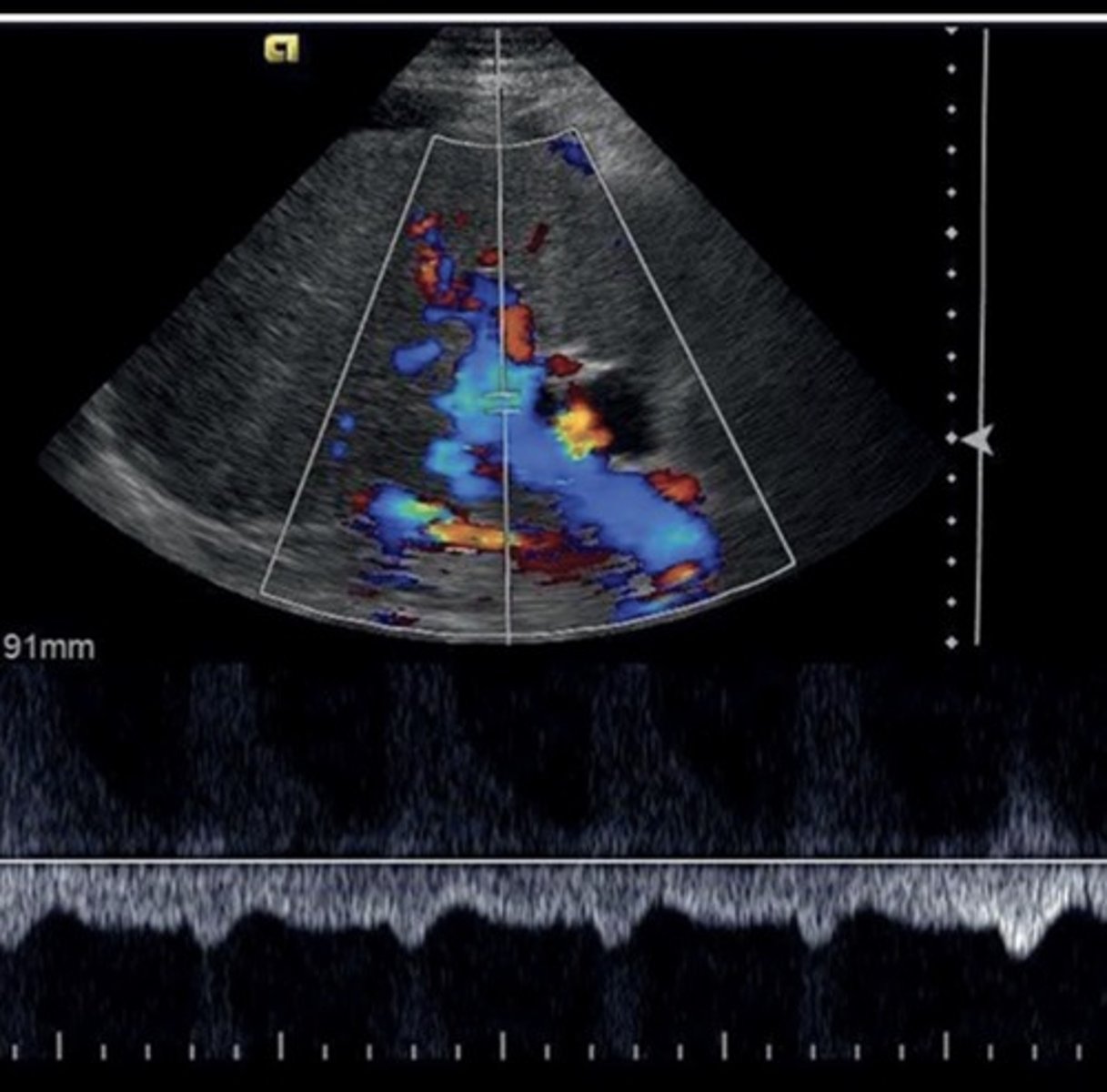
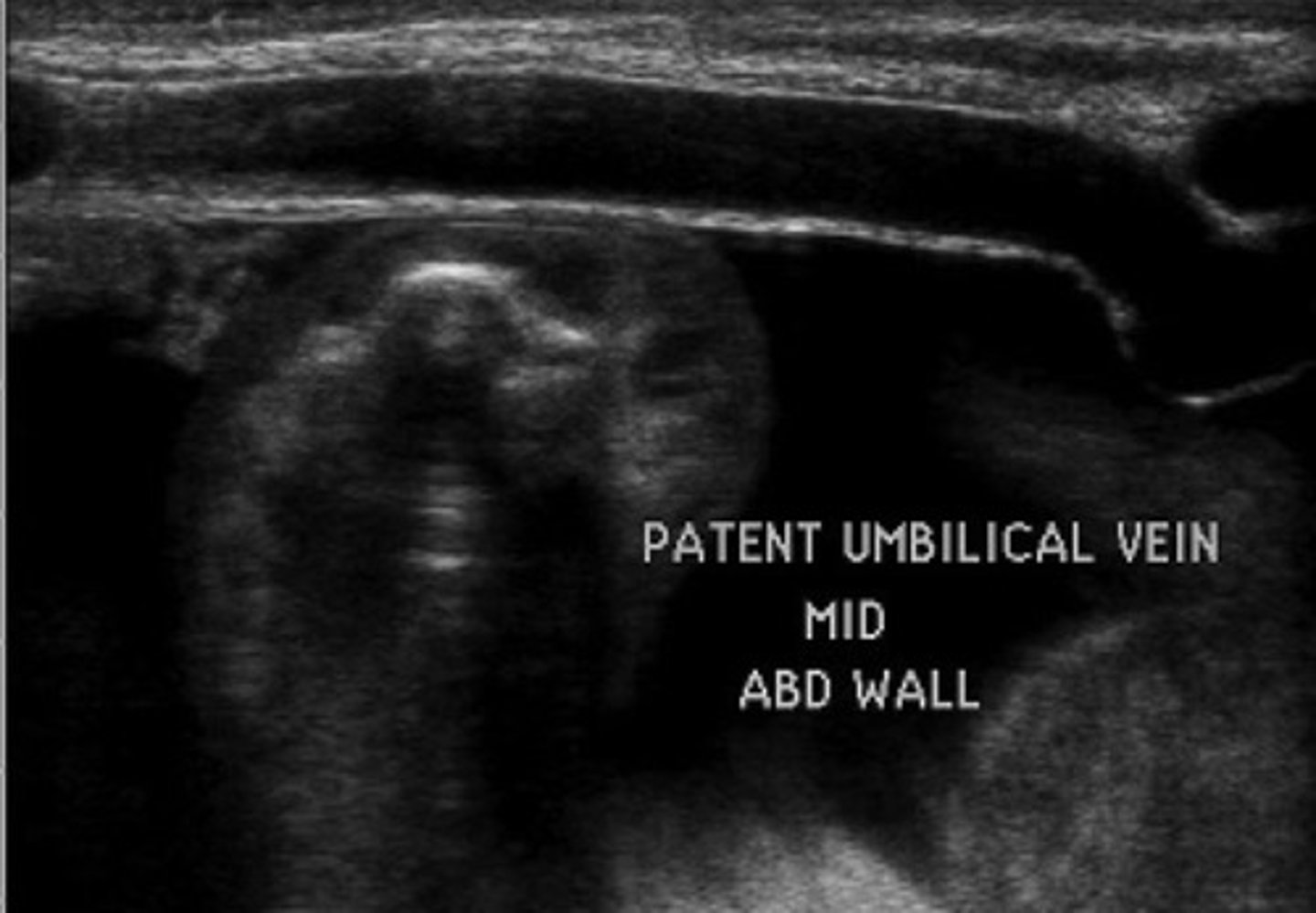
Recanalized Paraumbilical Vein
Ligamentum teres recanalizes
Courses from left portal vein to anterior abdominal wall
Hepatofugal flow
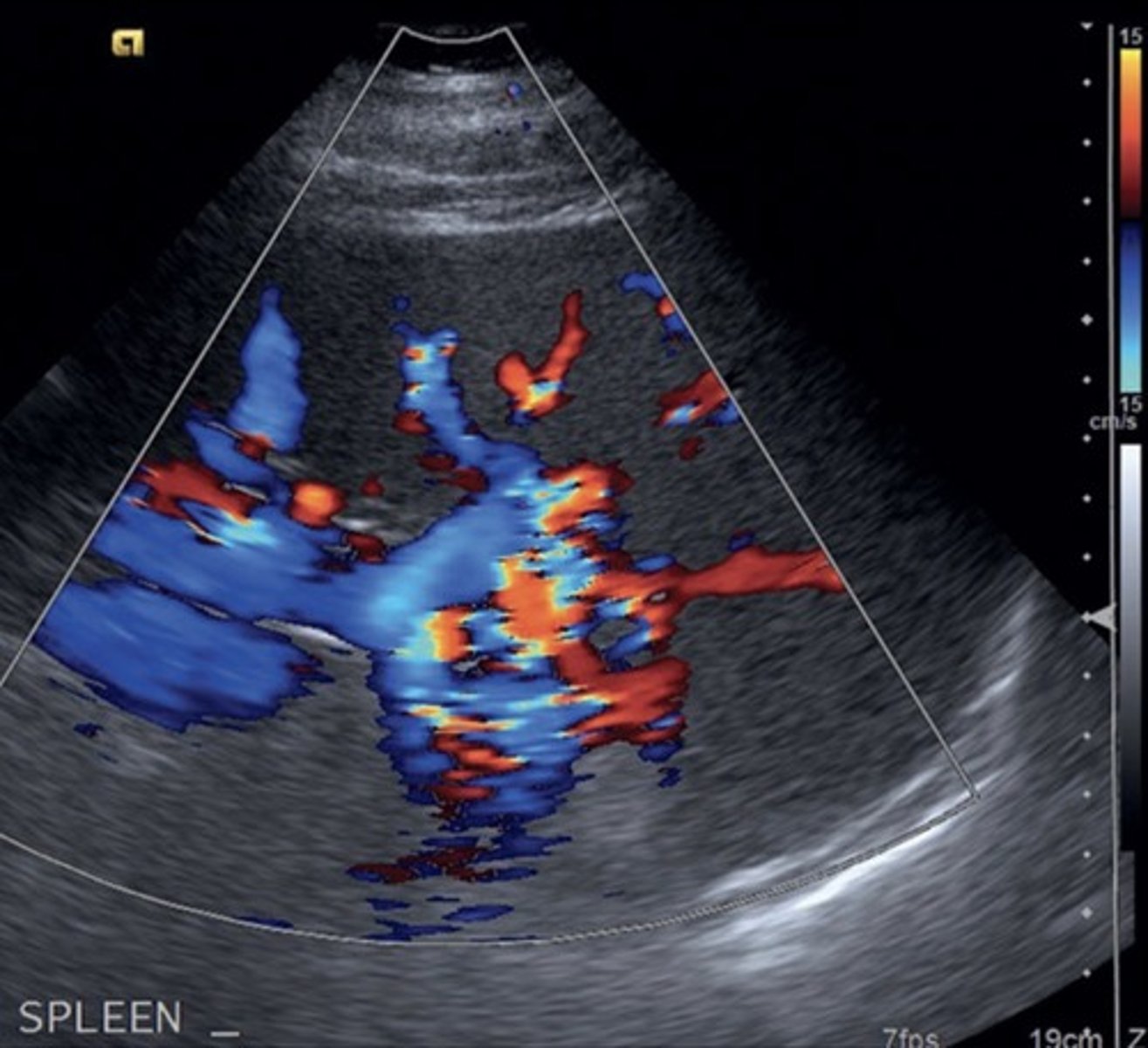
Splenorenal Shunt
Prominent veins at splenic hilum
Hepatofugal flow in splenic vein
Gastroesophageal Veins/Esophageal Varices
Originate from gastroesophageal junction posterior to left liver lobe
Due to hepatofugal flow in coronary vein shunt
High risk of rupture
AV Fistula
Arterialized portal vein flow - hepatic artery to portal vein shunting
Leads to portal HTN
AV Fistula Findings
Large anechoic spaces
Increased portal vein pulsatility & velocities
Aterialization of the Liver
Max portal vein pressure leads to increased hepatic artery flow
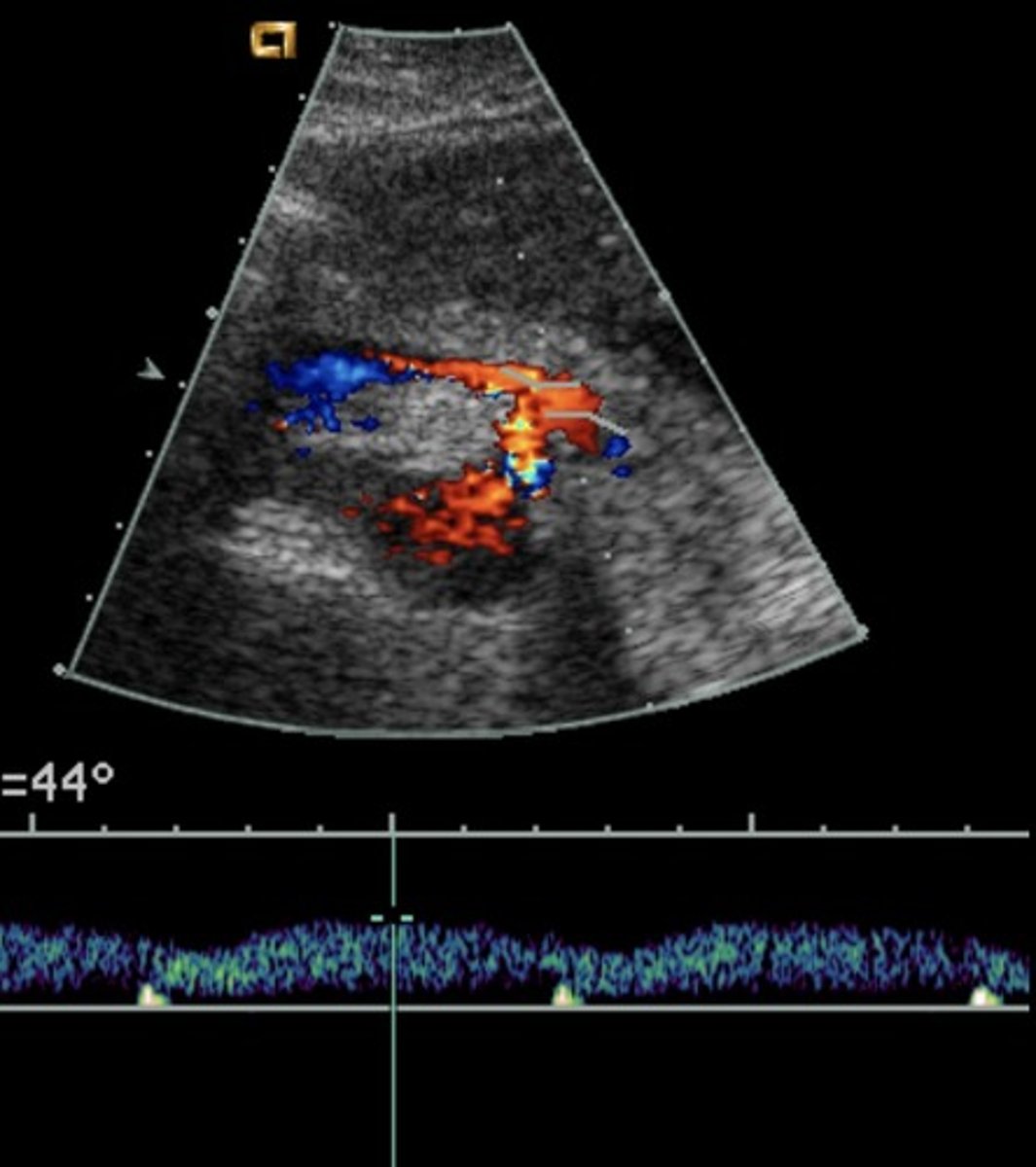
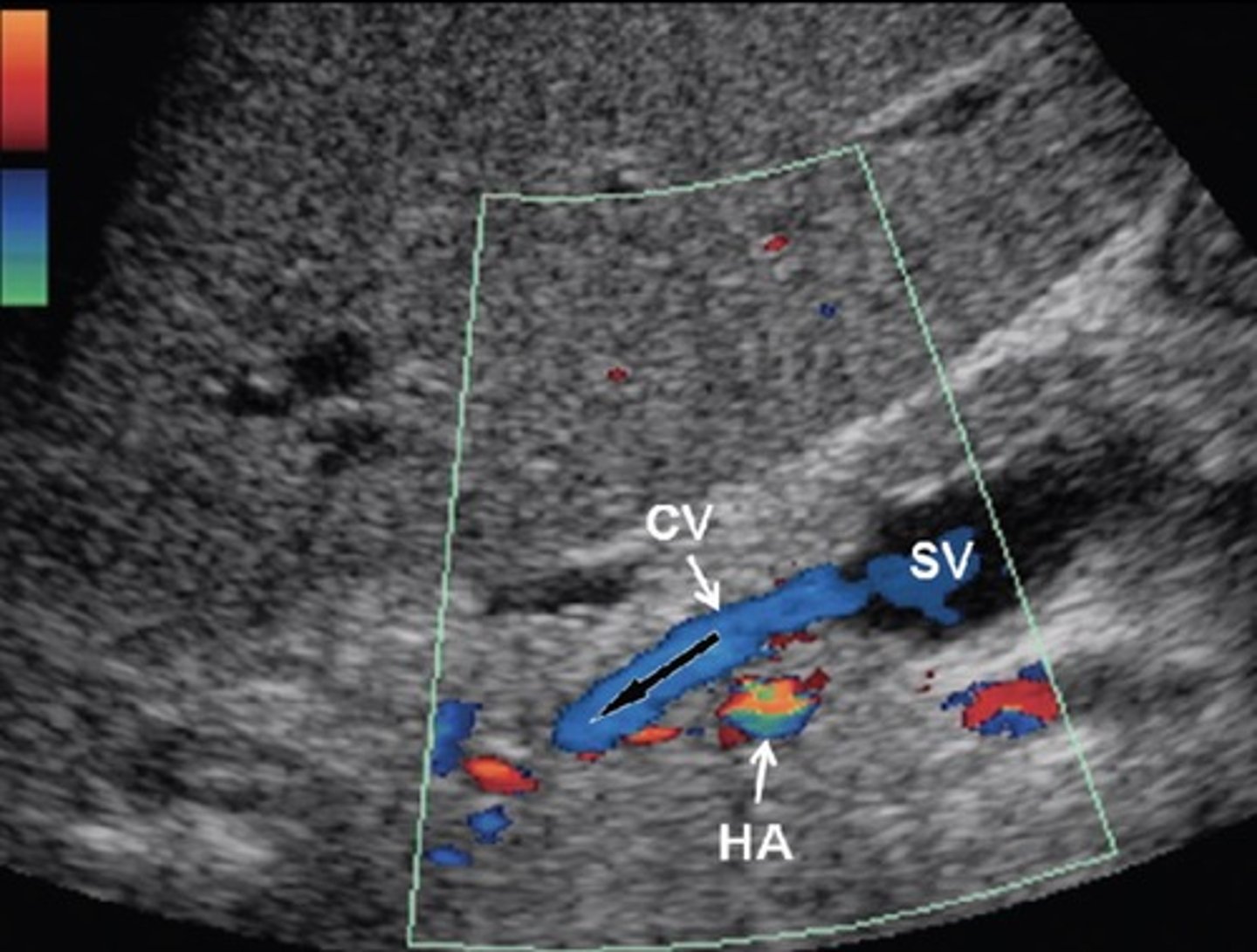
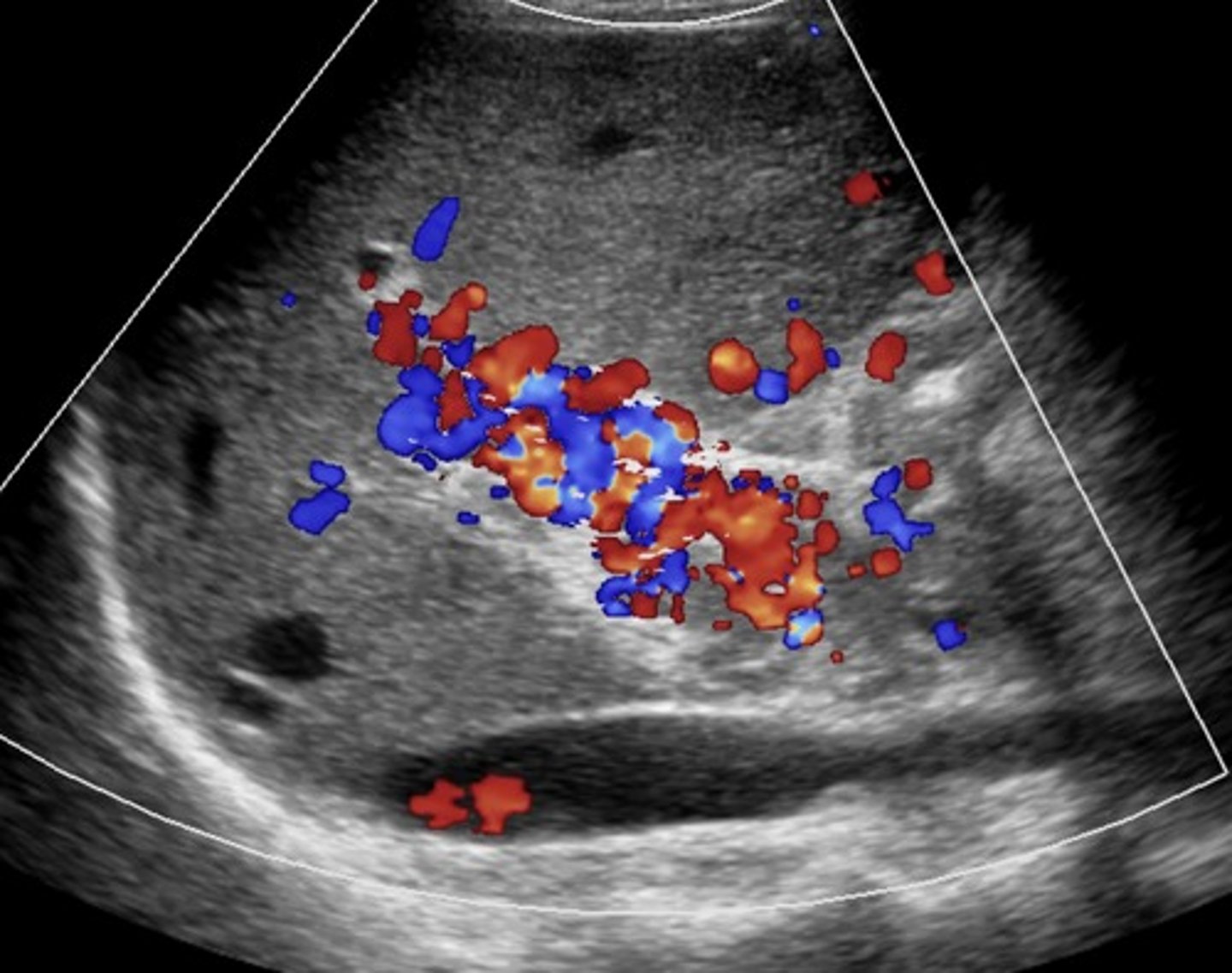
Cavernous Transformation
Due to chronic portal vein thrombosis
Occurs within 6 days after thrombotic event
Absent portal vein flow
Formation of new peri-portal vessels around portal vein
Hepatopetal flow within serpentine vessels
Budd-Chiari Syndrome
Hepatic vein/liver outflow obstruction
Causes increased sinusoidal pressure
Budd-Chiari Syndrome Findings
Hepatic vein thrombosis/post-sinusoidal thrombosis
Monophasic, reduced/reversed flow in portal vein
Enlarged caudate lobe
Ascites
Splenomegaly

Cardiac Cirrhosis
Liver edema caused by congestive heart failure
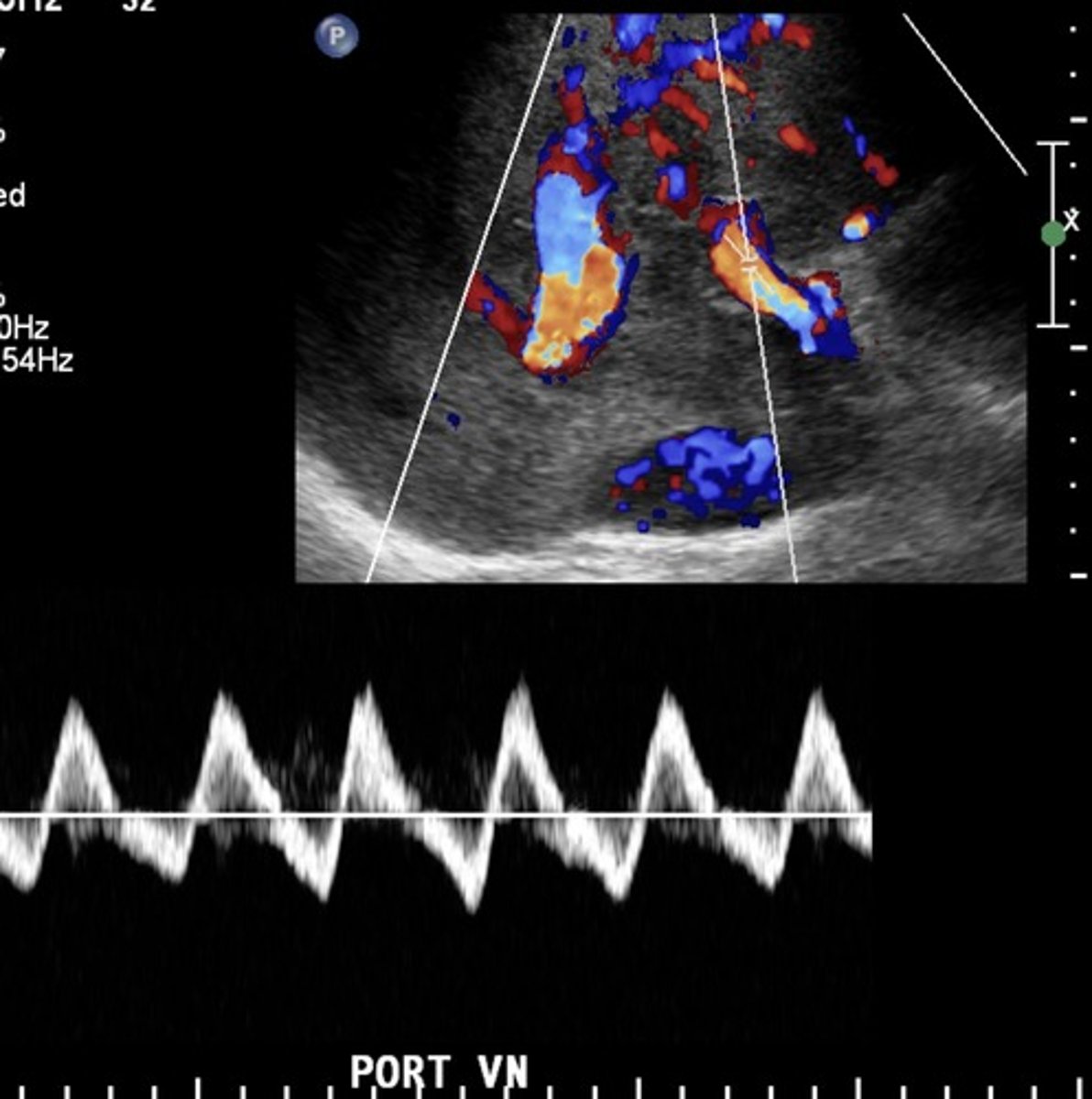
Portal Vein with Cardiac Cirrhosis
Pulsatile
Biphasic
Hepatic Veins with Cardiac Cirrhosis
Compromised flow - over congestion
"w" pattern
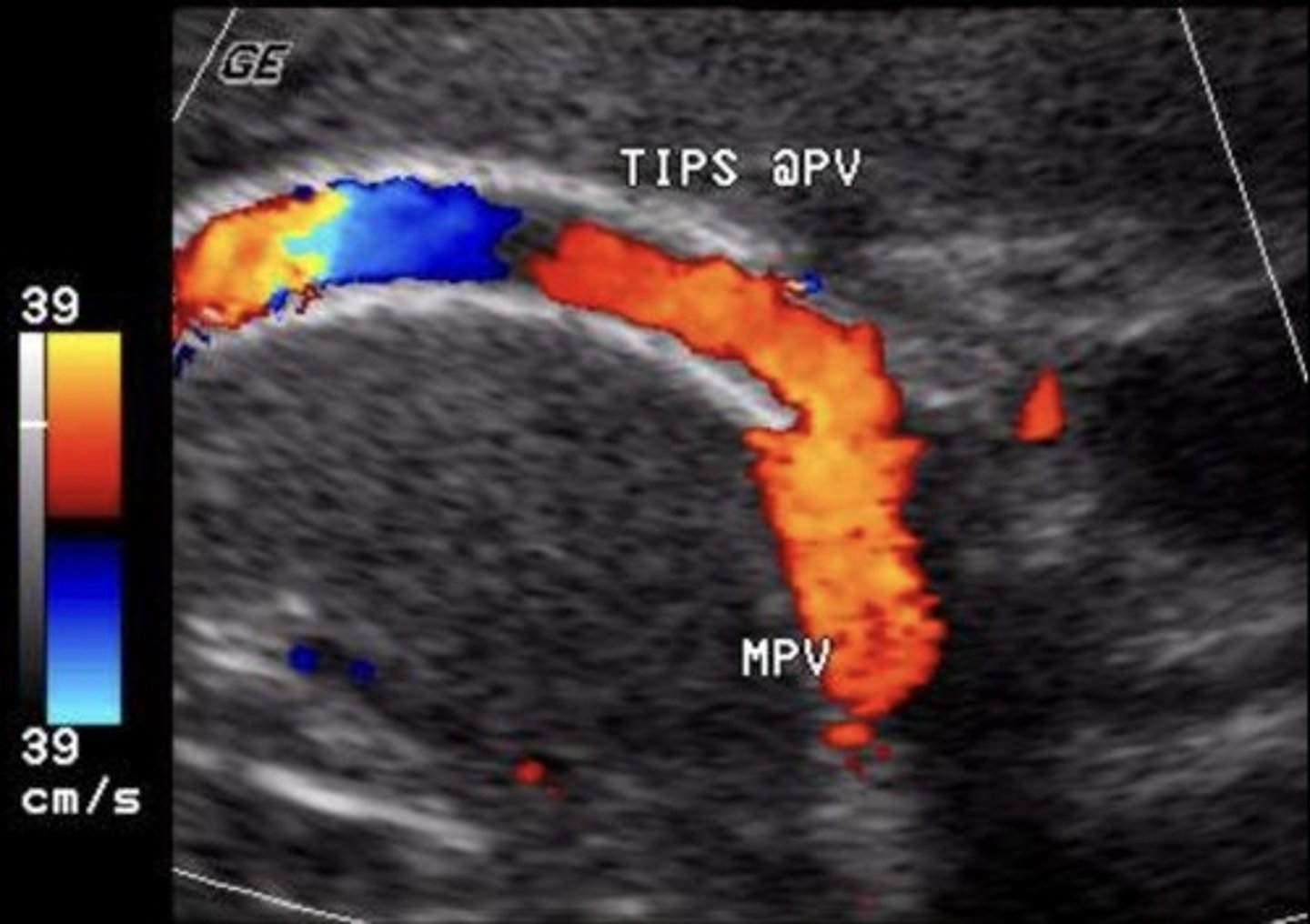
TIPS Shunt
Stent between portal vein & hepatic vein
(commonly right portal vein and right hepatic vein)
TIPS Shunt Normal Findings
No focal aliasing
Hepatofugal flow in portal veins beyond stent
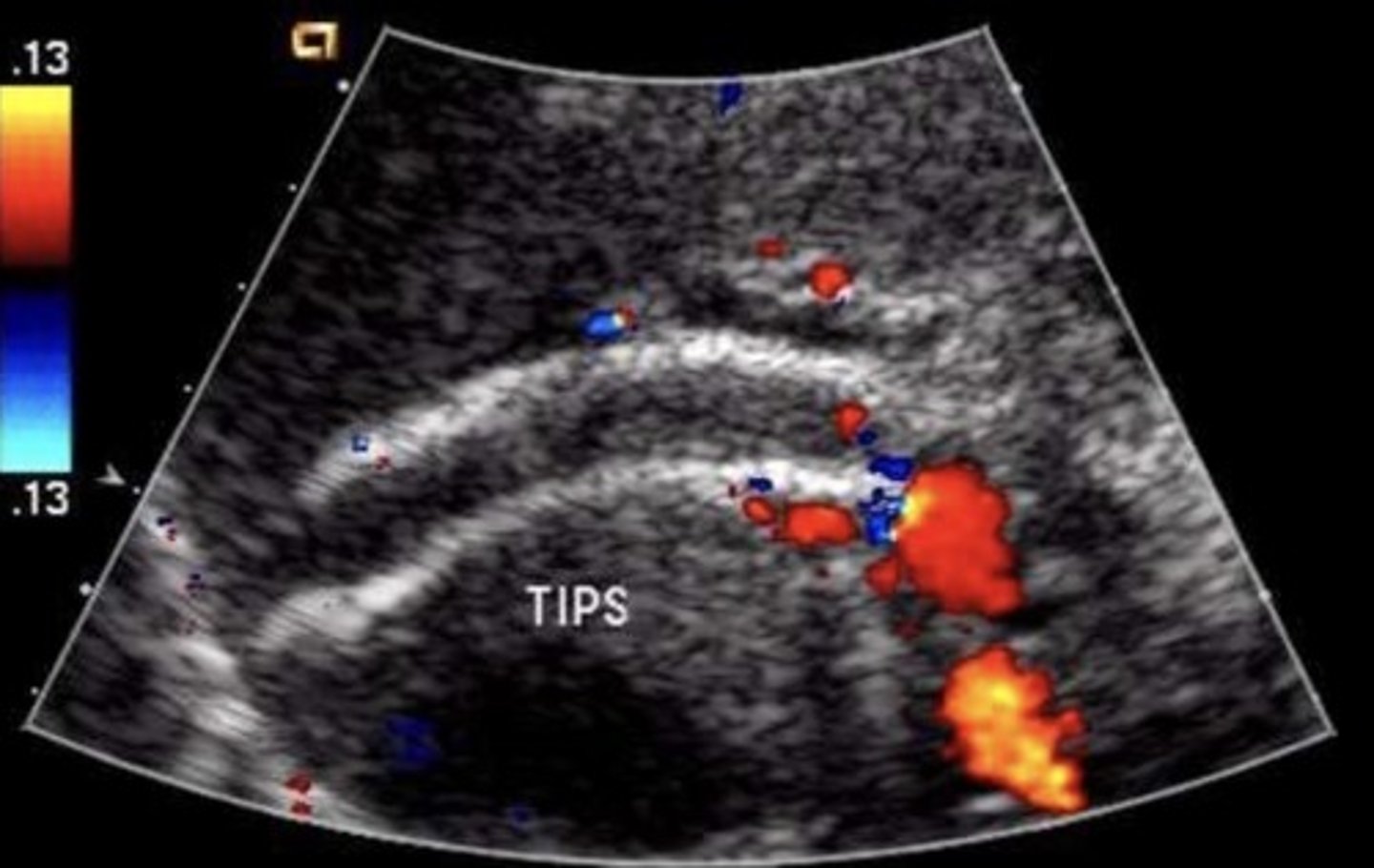
TIPS Shunt Abnormal Findings
Focal aliasing
Velocity changes
Antegrade flow in right & left portal veins
Retrograde flow in hepatic vein
Developing ascites or collaterals
TIPS Shunt Occlusion Findings
Hepatopetal flow in right & left portal veins
Hepatofugal flow in main portal vein
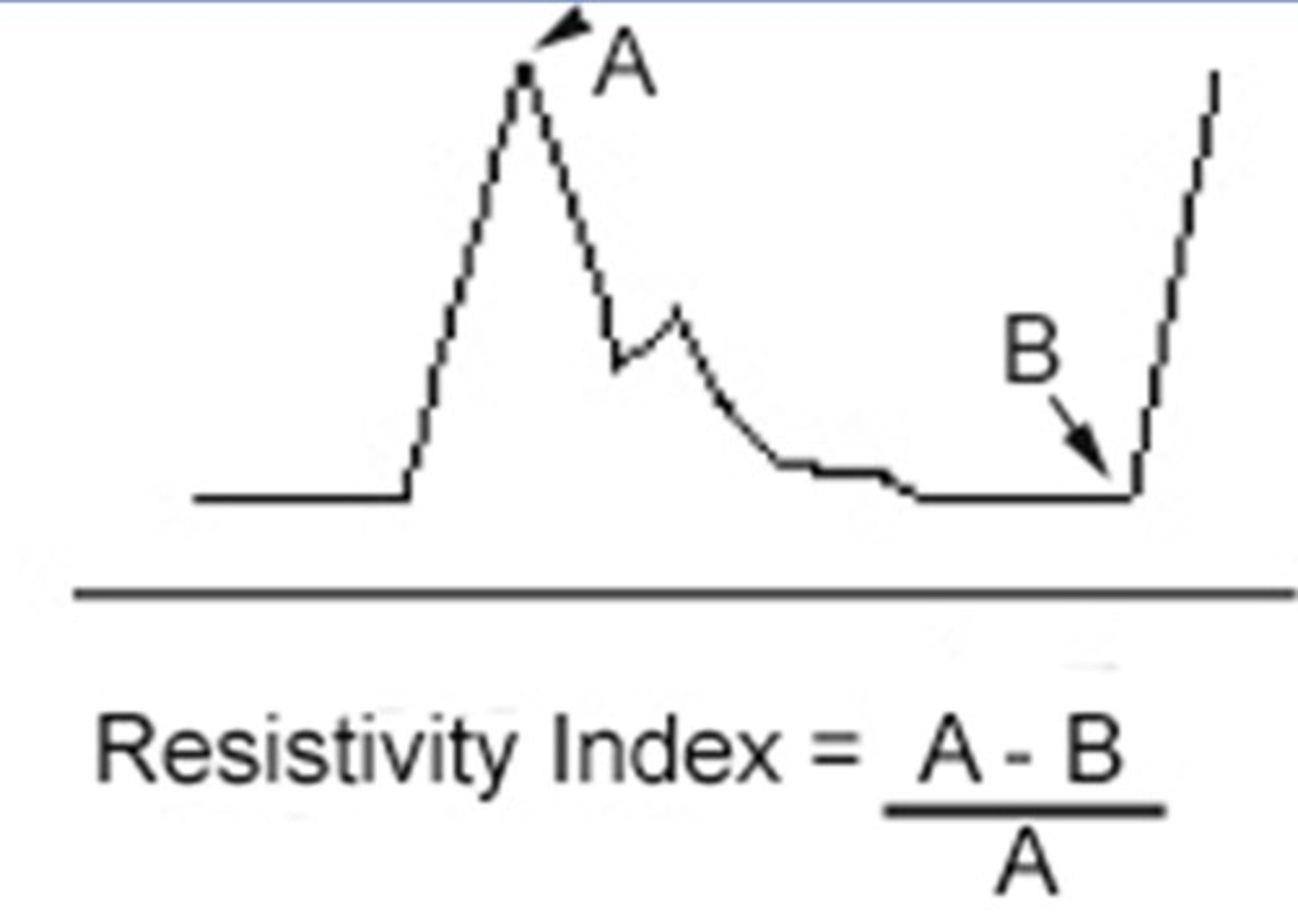
Resistive Index
Resistance of the end/target organ
Orthotopic Liver Transplant
Whole liver is transplanted from a deceased donor
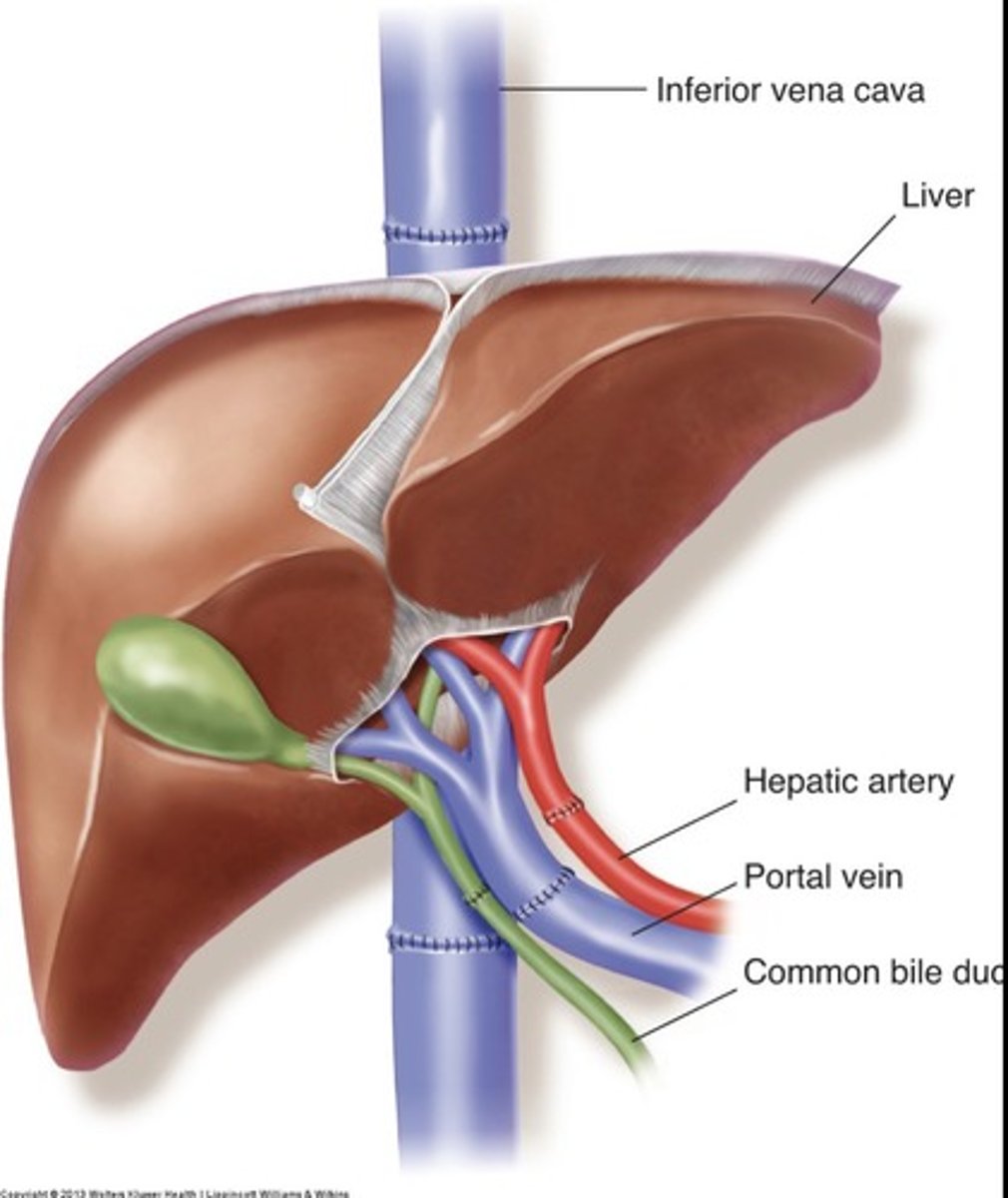
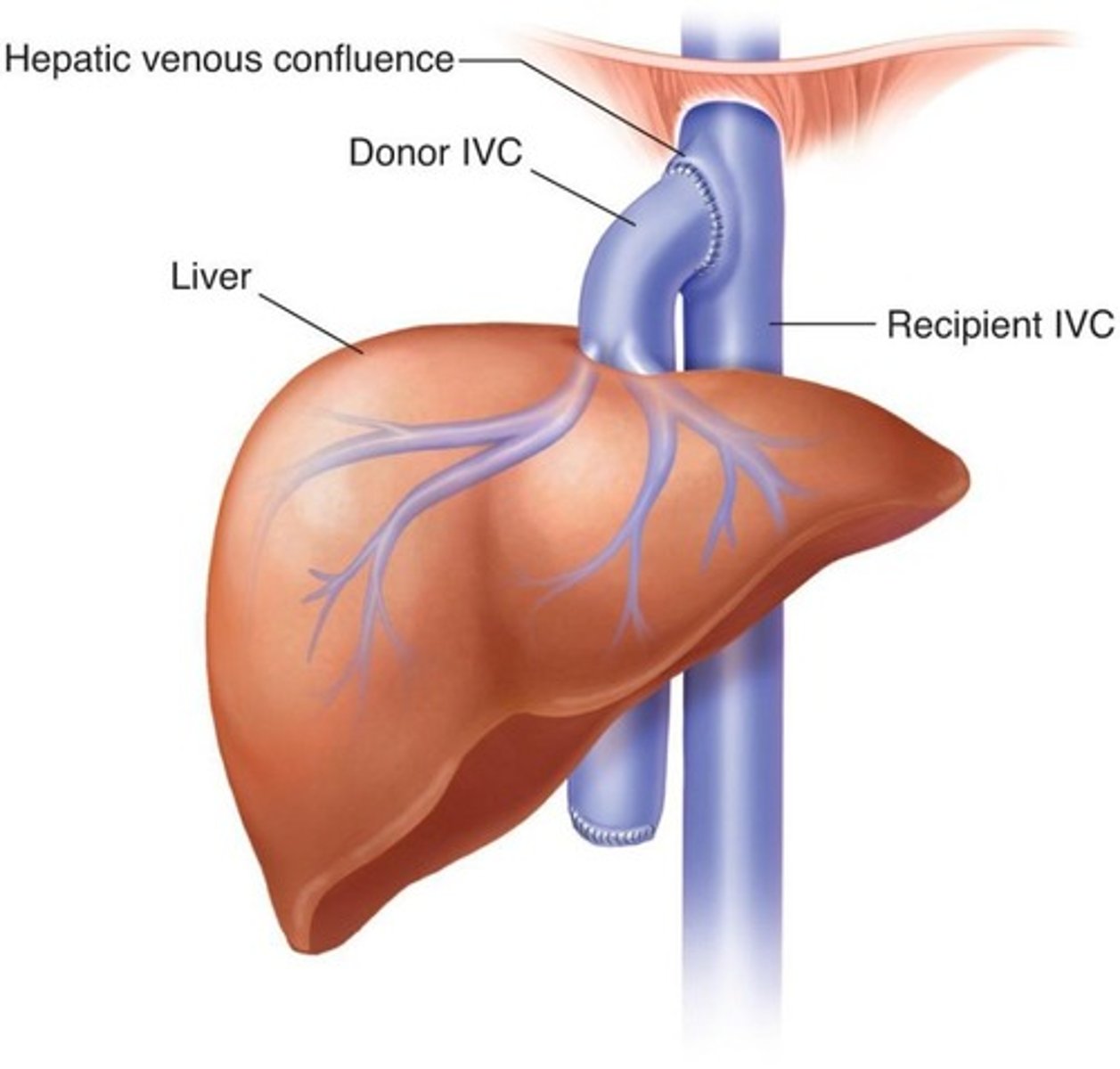
Piggyback IVC Anastomosis
Donor supra hepatic IVC attached to recipients hepatic venous confluence
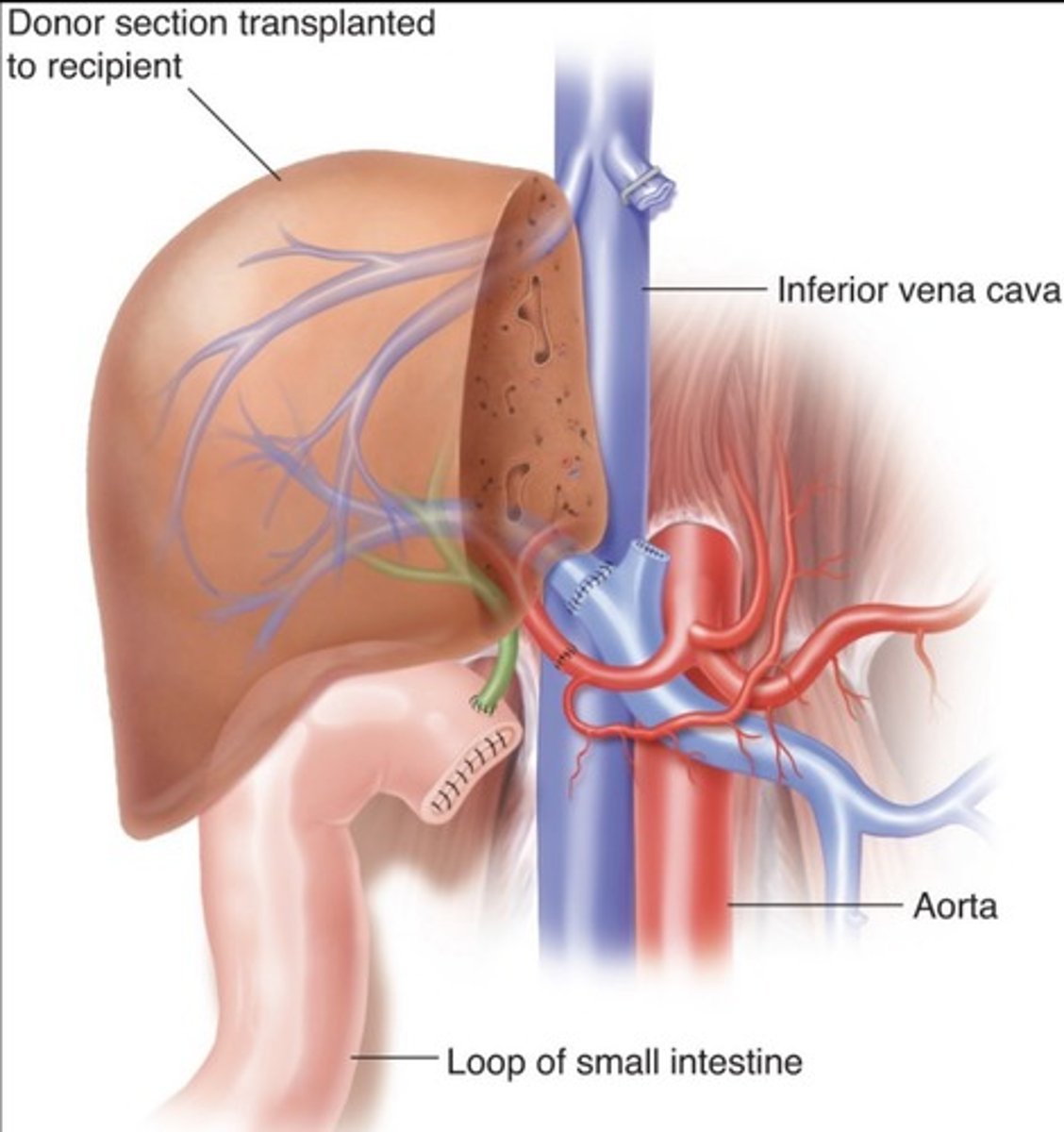
Partial Liver Transplant
Right lobe for adults
Left lobe for children
Normal Post-Transplant Findings
Parenchymal changes
Biliary ducts mat appear thicker - pneumobilia
Hematoma/pleural effusion
Increased RI of hepatic artery
Hepatic Artery Thrombus
Most common vascular complication of liver transplants
Second leading cause of graft failure
Occurs within 2 weeks post-transplant
Hepatic Artery Stenosis
Common at site of anastomosis
Leads to biliary ischemia & hepatic failure - must be treated
Hepatic Artery Pseudoaneurysm
Abnormal dilation due to disruption of intimal lining
Most found at sites of anastomosis
Often mycotic
Most commonly extrahepatic due to arterial wall weakening
Can be intrahepatic due to biopsy or biliary procedures
Anastomotic Biliary Stricture
Due to donor size mismatch or fibrosis
Dilated intrahepatic ducts
Prox CBD dilation
Non-Anastomotic Biliary Stricture
Multiple, long, focal ducts
Due to ischemia, hepatic artery thrombus, chronic rejection, or sclerosing cholangitis
Signs of Liver Transplant Rejection
Abnormal liver function tests
Ascites/pleural effusions
Varices
Sepsis, fever, infection
Biliary obstruction, leakage
Splenomegaly
Right Renal Artery
Posterior to IVC and RRV
Left Renal Artery
Accessory Arteries
Branch off main renal artery or aorta
Supply small portions of renal parenchyma.
Can be single/multiple and unilateral/bilateral
If stenotic, can result in HTN
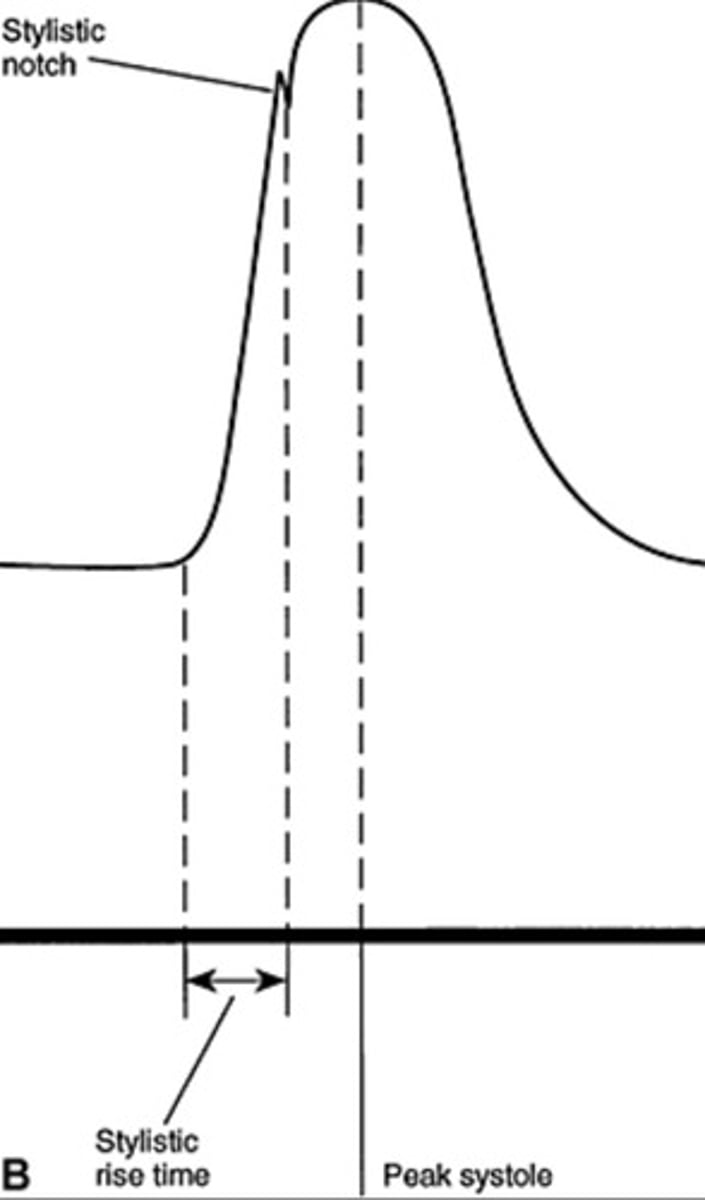
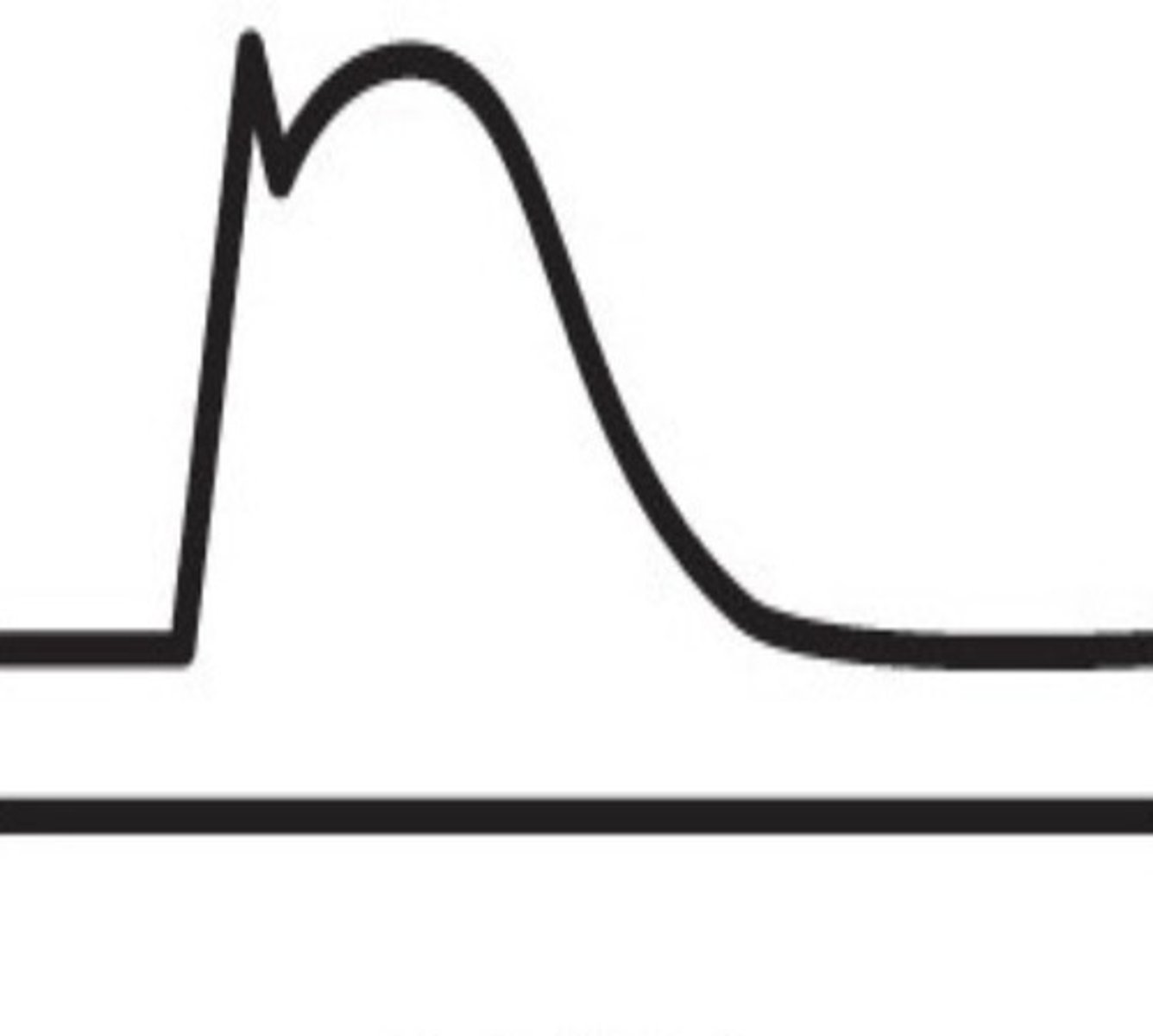
Normal Renal Artery Spectral Waveform
Rapid upstroke
Early systolic peak
2nd most common cause of renal artery stenosis
Fibromuscular dysplasia
0-59% Stenosis Waveform
60-70% Stenosis Waveform

> 80% Stenosis Waveform
Direct Renal Artery Exam
Uses velocities & RAR
Indirect Renal Artery Exam
Uses acceleration time, acceleration index, and waveform assessments
Acceleration Time (AT)
Time it takes for the to reach early systolic peak
Acceleration Index
Change in velocity divided by acceleration time
Tardus Parvus Flow
Rounded/delayed upstroke - indicates high grade stenosis proximally
100% indicative of RAS, but not always seen in RAS patients
Measured by acceleration time or acceleration index
Normal Renal Vein Doppler
Continuous pattern with mild respiratory variations
Sonographic Appearance of Renal Vein Thrombosis
Enlarged kidney
Enlarged vein with internal echoes
Lack of color fill
Biphasic/high resistant arterial signal
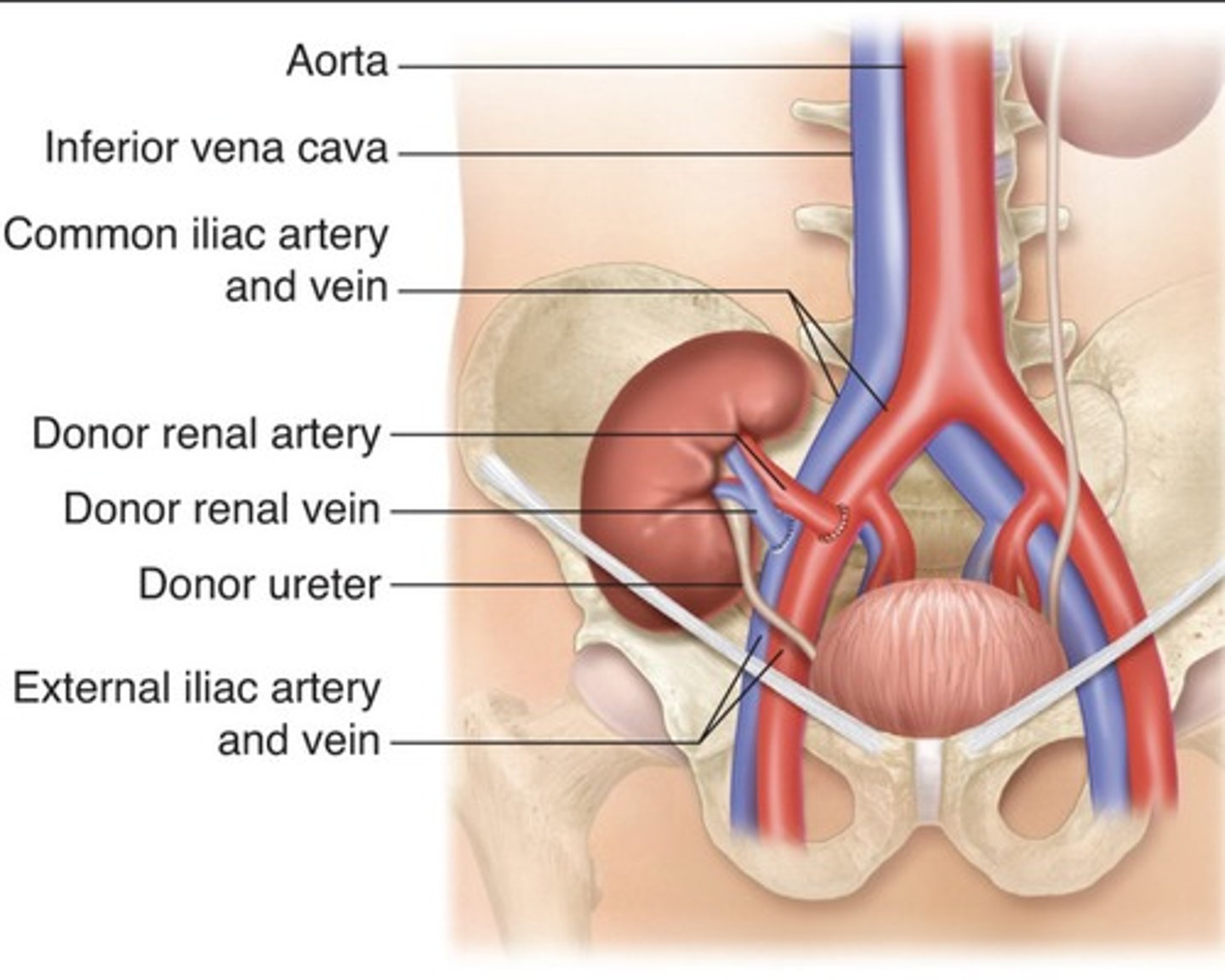
Indications for Renal Transplant
Diabetes mellitus (most common)
Autosomal dominant polycystic kidney disease
Glomerulonephritis
Hypertension
Atherosclerosis
Systemic lupus erythematous
Renal Artery Transplant Placement
Superficially located
Runs with the axis of incision
Hilum oriented inferiorly and posteriorly
Acute Tubular Necrosis (ATN)
Due to ischemia that develops between recipient removal to donor transplant
Common with cadaver donor kidneys
Occurs early post-op
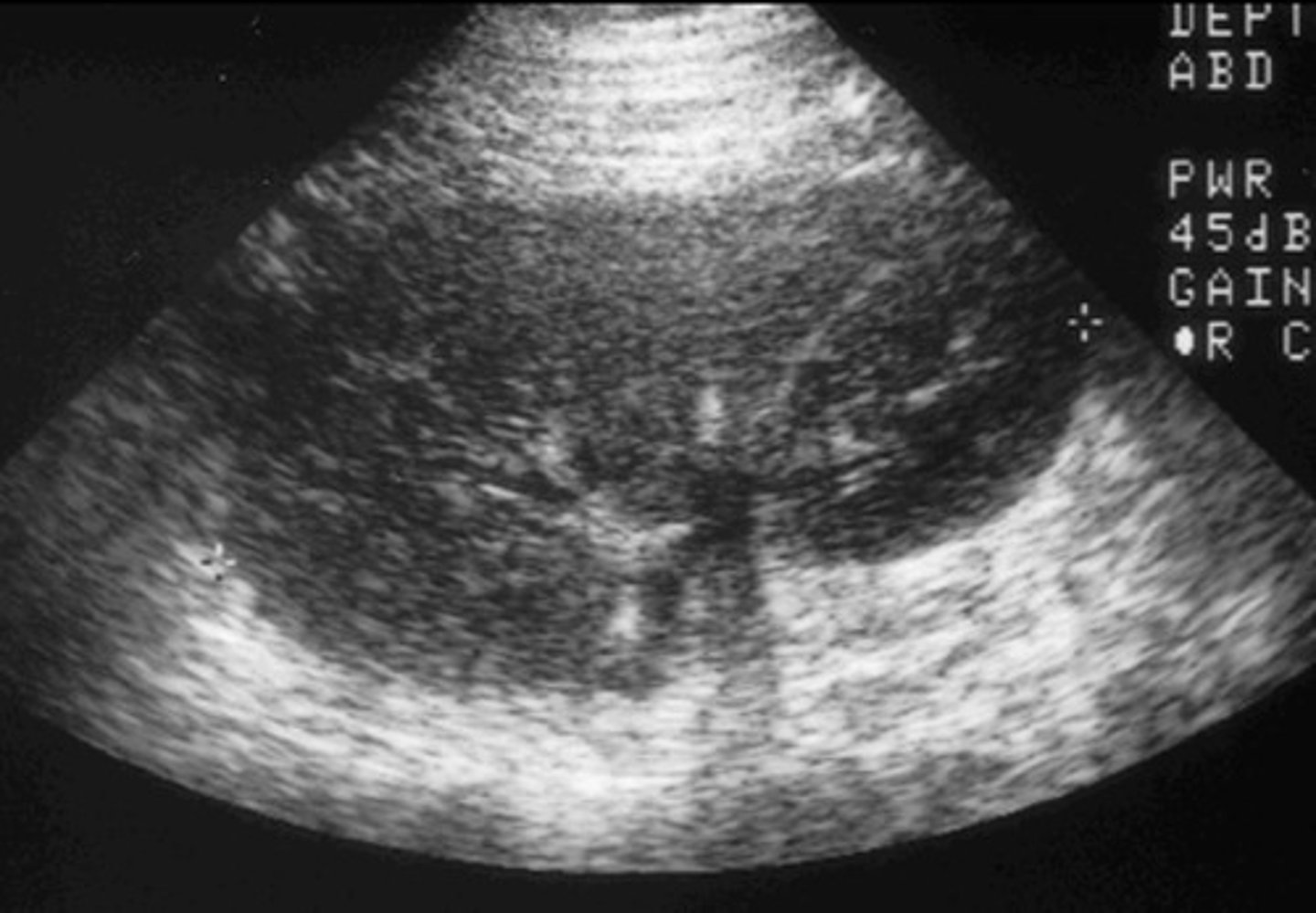
Appearance of Acute Tubular Necrosis (ATN)
Enlarged kidney
Loss of corticomedullary boarders
Parenchymal Graft Failure Causes
Acute tubular necrosis (ATN)
Rejection
Cyclosporin toxicity
Vascular Transplant Failure Causes
Thrombosis
Stenosis
Urological Transplant Failure Causes
Obstruction
Extrinsic compression
Fluid collections
Symptoms of Renal Transplant Rejection
Sudden cessation of urine output (anuria)
Decreased urine output (oliguria)
Increased serum creatinine, protein, or lymphocytes in urine
Hypertension
Swelling or tenderness of the graft
Hyperacute Transplant Rejection
Minutes to hours
Rare
Due to faulty crossmatching tests
Completely destroys graft
Removed immediately
Acute Transplant Rejection
2 weeks - 3 months
Common in cadaver donor kidneys
Appearance of Acute Transplant Rejection
Enlarged kidney
Loss of corticomedullary boarder
Decrease in diastolic flow or flow reversal
RI > 0.8
Chronic Transplant Rejection
3 months - years
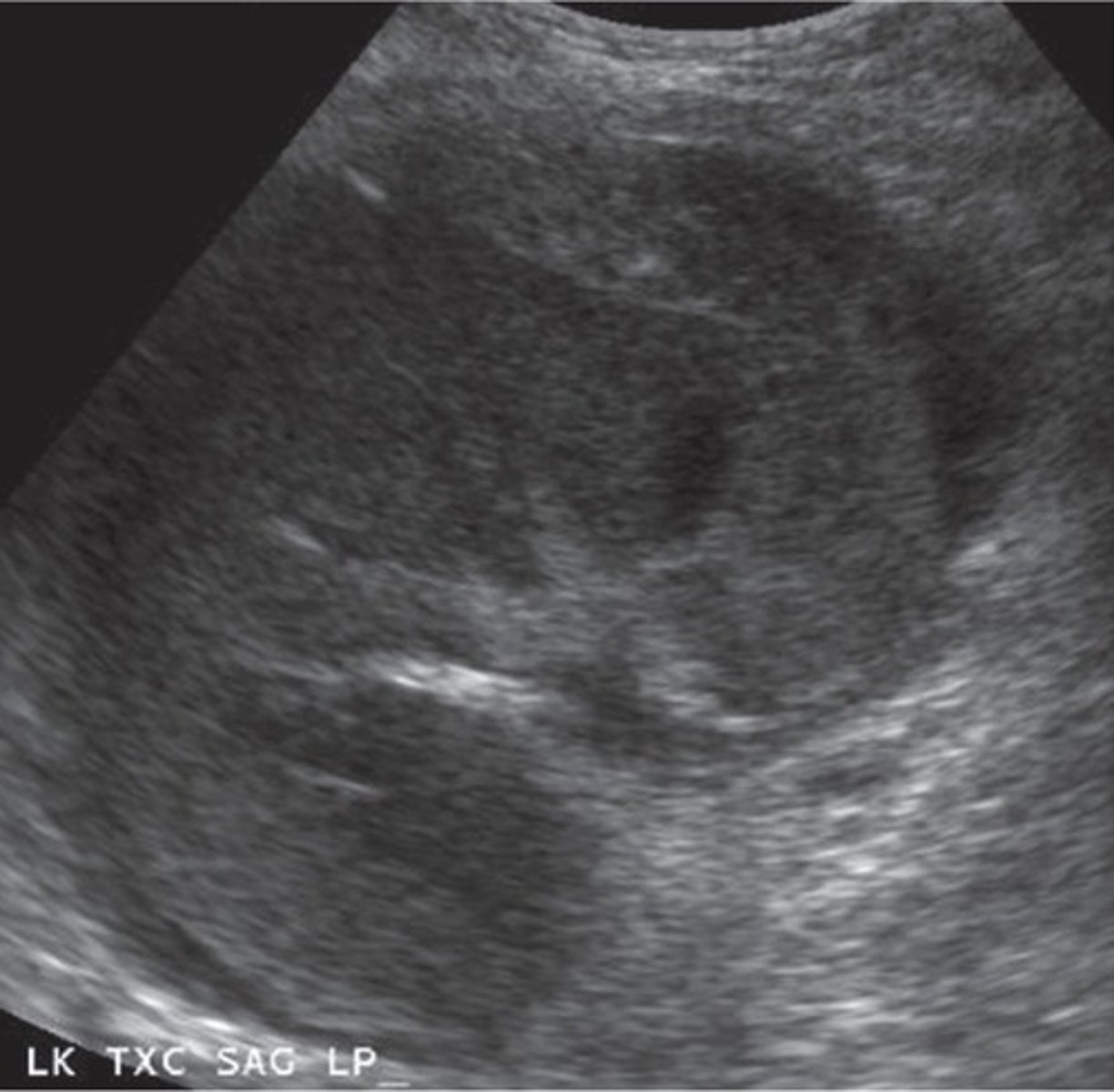
Appearance of Chronic Transplant Rejection
Echogenic kidney
Loss of corticomedullary boarders
Solid material in renal pelvis
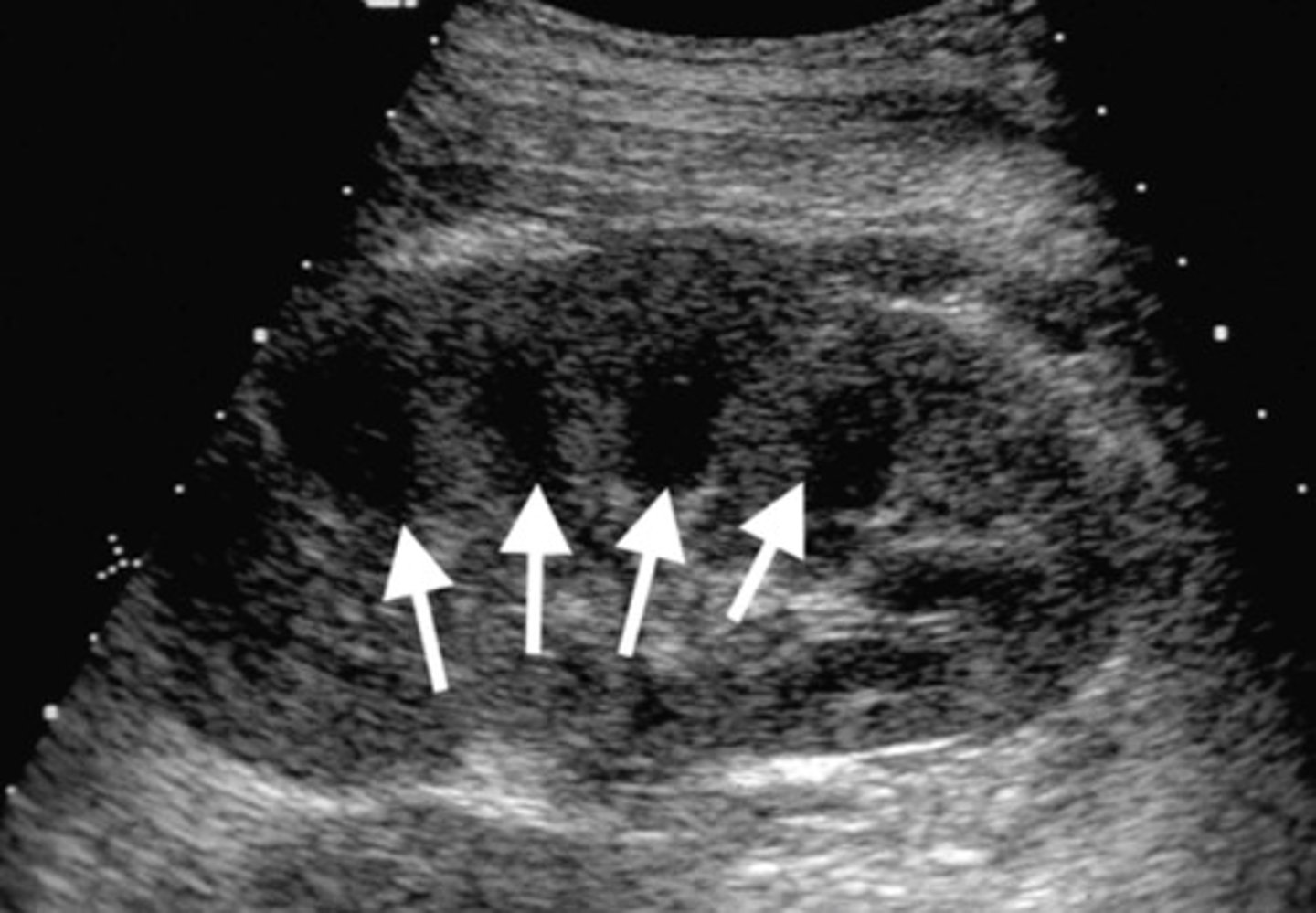
Hydronephrosis Post-Transplant
Due to ureteral narrowing from surgery
Compresses ureter and parenchyma
Increased RI

Perinephric Hematoma
Variable echogenicity - depends on time since hemorrhage occurred
Urinoma
Urine leaking from ureteral anastomosis
Seen in first weeks post-transplant
Suspected when urine output decreases
Risk for rupture - increase quickly
Lymphocele
Surgical nick in lymphatic system
Seen 4-8 weeks post-op
Complex appearance
Can compress the kidney

Page Kidney
Compression of kidney by fluid collections
Longlasting HTN
Blunted waveforms
Increased resistance