Karimi ACD
1/10
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
11 Terms
Define Acute Coronary Syndrome (ACS) and Myocardial Infarction (MI)
Acs is an umbrella term for acute clinical manifestations including unstable angina (UA), non-ST-segment evaluation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction
If unstable angina not treated → often progresses to NSTEMI or STEMI
Unstable angina is the most severe form of angina with increasing intensity, frequency, and duration
A combination of of atherosclerotic plaque formation, platelet aggregation (clot formation), and vasospasm
Usually an immediate precursor to MI
MI (heart attack): occurs when ischemia block blood flow entirely, causing that affected cardiomyocytes to slow down and eventually die, leading to the formation of irreplaceable scar tissue
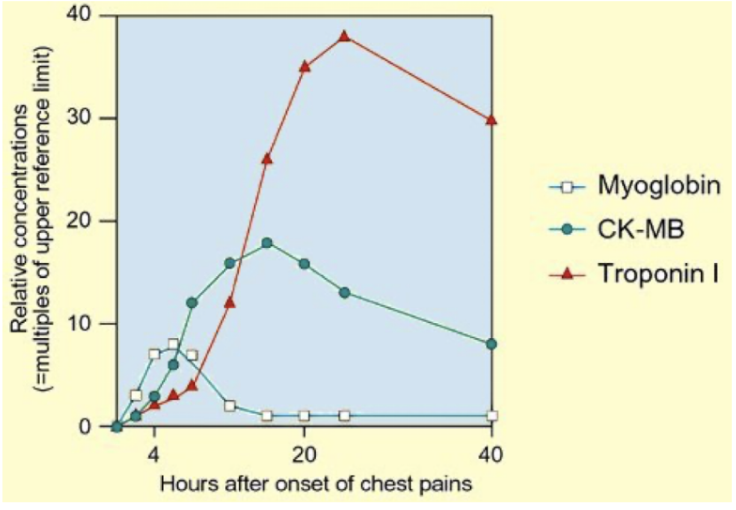
Serum Protein Elevations During MI ?
Troponin T and I
Troponin unique to heart muscle
Creatine Kinase Myocardial Brand (CK-MB)
Semi-specific
Myoglobin
Non-specific
Troponins play an important role in the MI detection as they are part of the contractile apparatus of cardiomyocytes and are released into the circulation upon a myocardial injury
Troponin levels peak = 36 hours after an infarct and may remain high for 7 -10 days
Define MI’s two major types: ST-Segment Elevation (STEMI) and Non-ST-Segment Elevation (NSTEMI)
NSTEMI: a partial thickness (subendocardial) infarct caused by the occlusion of a coronary artery, resulting a partial necrosis of the left ventricular wall (⅓ to ½ of left ventricular wall)
STEMI: a full thickness (transmural) infarct caused by complete occlusion of blood vessel lumen, resulting in necrosis completely through the left ventricular wall
Know the risk factors for ACS
Risk factors for ACS are the same as those that cause CAD/CCD since ACS is the acute progression of plaque buildup and rupture
Describe the pathophysiology of ACS including unstable angina (UA), STEMI and NSTEMI
UA: the plaque ruptures and a thrombus forms, causing partial occlusion. This is a "supply ischemia” without true infarct
NSTEMI: the ruptured plaque thrombus causes a partial occlusion that is severe enough to result in injury and subendocardial infarct
STEMI: complete occlusion of the blood vessels lumen result in a transmural infarct and injury to myocardium
Recall the characteristic biomarker and ECG differences between UA, STEMI and NSTEMI
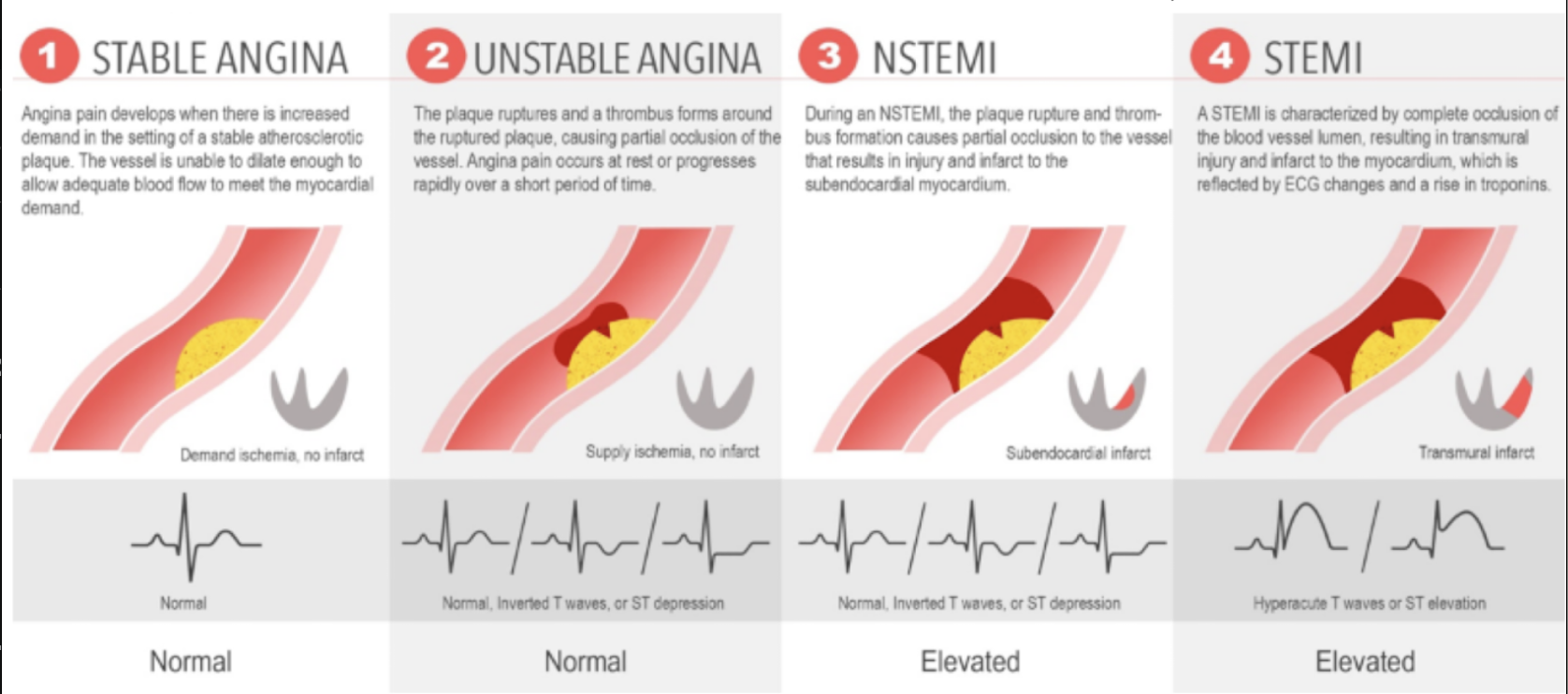
UA: Normal tropons. ECG may be normal, show inverted T waves, or ST depression
NSTEMI: Elevated troponins, ECG is similar to UA (normal, inverted I waves, ST depression)
STEMI: elevated troponins. ECG shows hyperacute T waves or ST elevation (not cardiac troponins peak about 36 hours after infarct)
Aspirin
irreversibly inhibits COX-1, which decreases thromboxane A2 (TXA2) and prevents platelet aggregation
Gives aspirin antiplatelet effect that may be useful for patients at high risk for CV disease
DOA of antiplatelet effect: 7-10 days
Other tissue 6-12 hrs
Avoid normal aspirin dose in children due to link to Reye’s syndrome
P2Y12 inhibitors
inhibit the ADP receptor to decrease platelet aggregation
Agents:
Clopidogrel (Plavix)
Both prodrug and irreversible inhibitor of P2Y12 and thereby inhibits ADP-mediated platelet aggregation
Slow offset of actions (return to baseline after 5 days)
DI: proton pump inhibitor may reduce its effectiveness due to inhibition of CYP2C19
ADE: increase risk of bleeding
Prasugrel
Produrg but activated by hydrolysis in liver
Activation not as variable as clopidogrel, and activated mor efficiently then clop., having a faster onset of action
ADE: Bleeding, more than Clopidogrel
CI: pt with hx of stroke due to bleeding risk
Ticagrelor
More rapid onset and offset than clopidogrel
Also causes greater and more predictable inhibition of platelet aggregation
Metabolized in liver via CYP 3A4 and thus has interactions with potent 3A4 inhibitors or inducers
ADE: Bleeding, dyspnea reported in 17% of patients
Cangrelor (only IV)
Stronger platelet inhibition than aspirin
ADE: Bleeding
Gllb/llla inhibitors
IV biologic agents that inhibits Gllb/llla receptors to decrease aggregation
Agents
Abiximab
Has a long DOA (24 hr after infusion)
Tirofiban
Eptifibatide
ADE: bleeding
Less common: thrombocytopenia
Anticoagulants
Inhibit the coagulation cascade by activating antithrombin III, which inhibits factor Xa, ultimately decreasing fibrin formation and clot formation
Agents
Unfractionated
Heparin
Enoxaparin
Admin: parenterally
ADE: Bleeding (common), Thrombocytopenia (less common)
Fibrinolytics (Tissue Plasminogen Activators): Enzymes that mimic native native tissue plasminogen activator. They increase the formation of plasmin, which directly degrades fibrin and fibrinogen to restore blood flow
Agents:
Alteplase
Tenecteplase
Reteplase
ADE: Bleeding
Describe why agents such as ACE-Inhibitors, Statins, nitroglycerin, and beta blockers are useful in ACS
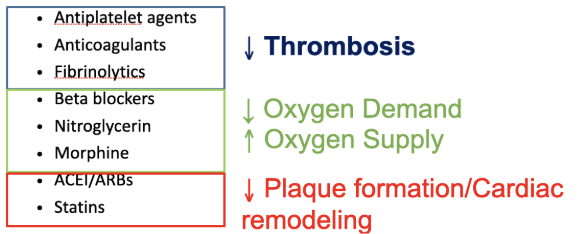
Statins: all patients with UA, STEMI or NSTEMI should be discharged on an intensive statin (atorvastatin 40-80 mg/day), unless contraindicated or patients > 75 years receive a moderate-intensity statine (due to AE)
ACEi/ARBs: treatment with an ACEi is recommended in all patients with MI, if intolerable use ARB
Nitroglycerin: short-acting (sublingual tablets or spray) or long-acting if vasospasms
Beta-Blockers: reduce oxygen demand (by lowering heart rate, contractility, and blood pressure), which helps relieve anxiety and reduce pain. Less oxygen demand means less anaerobic oxidation, reducing lactic acid formation