Advanced Respiratory
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
What are common cases seen on general respiratory ward?
Chronic Obstructive Pulmonary Disease (COPD)
Acute viral pneumonia (including ’Flu and COVID-19)
Bronchiectasis (including pseudomonas colonisation and Cystic Fibrosis)
Pulmonary Fibrosis (Interstitial Lung Disease)
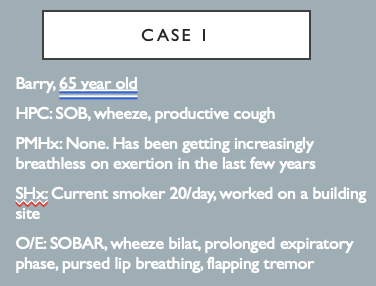
For this case answer the following questions
What’s the likely diagnosis?
What acute treatment does he need?
What longer term tests / management might you suggest?
COPD steroids?
acute exacerbation of undiagnosed COPD give steroids and some nebulisers acutely and possibly abx
monitor O2 levels and blood glucose levels
long term use long acting preventative meds
diagnosing using spirometry with GP
What are the clinical features of COPD?
Rare in under 35s
Dyspnoea
Chronic cough, may be productive
Wheeze
Advanced disease: fatigue, weight loss and anorexia
Features in history: smoking history, occupational and industrial exposures.
History of exacerbations
Co-morbidities
Impact on patient’s life
What are the clinical signs of COPD?
Depends on severity / may be normal
High RR
Hyperexpanded / barrel chest
Prolonged expiratory time (>5s), pursed lip breathing
Use of accessory muscles
Quiet breath sounds +/- wheeze
Quiet heart sounds
Can have basal crepitations
Signs of cor pulmonale / RHF and CO2 retention: ankle oedema, raised JVP, warm, plethoric conjunctivae, bounding pulse, polycythaemia. Acutely – flapping termor
Define COPD.
Common: ~12% of all general medical admissions
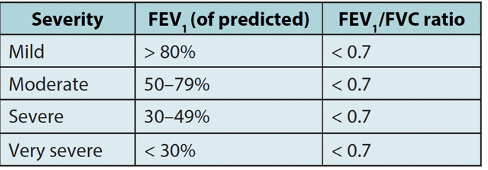
Definition: fixed airflow obstruction (FEV1/FVC <0.7), persistent respiratory symptoms
95% smoking-related (typically >20 pack/years)
Genetic susceptibility.
Environmental and occupational factors
→ Encompasses a number of underlying pathologies including chronic bronchitis and emphysema
→ COPD occurs in 10-20% of smokers
→ Worldwide – biomass fuel exposure. Smoking with marijuana increases risk.
→ Environmental and occupational factors – dusts, chemicals, air pollution
→ Reduced maximal attained lung function due to events during gestation/birth/childhood may also be a risk factor
What is Panacinar emphysema?
dilated airspaces evenly distributed across acini
Centriacinar or proximal emphysema can occur with dilated air spaces in association with respiratory bronchioles
Periacinar or paraseptal emphysema can occur with dilated airspaces at the edge of the acinar unit and abutting a fixed struction such as pleura/vessel
Emphysema
Loss of elasticity, hyper inflammation and increased airspaces
Bronchitis
Mucus overproduction and hyper secretion
Describe and explain the pathology of COPD
Chronic inflammation and fibrosis of small airways: CD8 lymphocyte, macrophage and neutrophil infiltration with release of pro-inflammatory cytokines
Reduction in airway lumen
Airflow limitation leads to gas trapping and static hyperinflation
Recurrent infections may perpetuate airway inflammation
Alveolar wall destruction, causing irreversible enlargement of acinar airspaces, subsequent loss of elastic recoil and hyperinflation
Mucous gland hyperplasia, particularly in large airways
With mucous gland hypersecretion: chronic productive cough
Other mucosal damage:
Squamous metaplasia – replacement of the normal ciliated columnar epithelium by a squamous epithelium
Loss of cilial function: leads to impairment of normal functioning of mucociliary escalator
→ Chronic productive cough → Worsening of sx when quit smoking
→ emphysema (smoking big cause) and chronic bronchitis 9productive more likely) and respiratory symptoms
→ alveoli destruction tripod: assessors muscles
What are the two types of patient see with COPD?
Patient hypoxia and emphysema breathlessness and skinny
Bigger cyanotic chronic bronchitis mucus airways respiratory type 2 respiratory failure more non-invasive ventilation
What are the aims of COPD management?
Smoking cessation
Minimizing symptoms where possible
Maintaining QoL
Minimizing exacerbations
MDT approach
No treatment modifies disease progression (except smoking cessation)
Give examples Non-pharmacological management used in COPD.
Smoking cessation
Education
Pulmonary Rehabilitation
Diet
Self-management plan
Psychosocial support
→ Pulmonary rehab: MDT. RCT evidence that it improves ET, QOL, reduces hospital admissions.
→ Muscle mass, esp LL, reduced. Independent predictor of mortality and disability, independent of lung disease. May reflect systemic nature.
→ Graded exercise to improve muscle function, also includes breathing techniques and education.
→ Usually OP basis over several weeks.
→ Wt loss (concurrent OSA/OHS), but also if very breathless, calorific intake may be low and may be catabolic state.
→ Practical support at home, day centres, car disability badge, signs of anxiety + depression
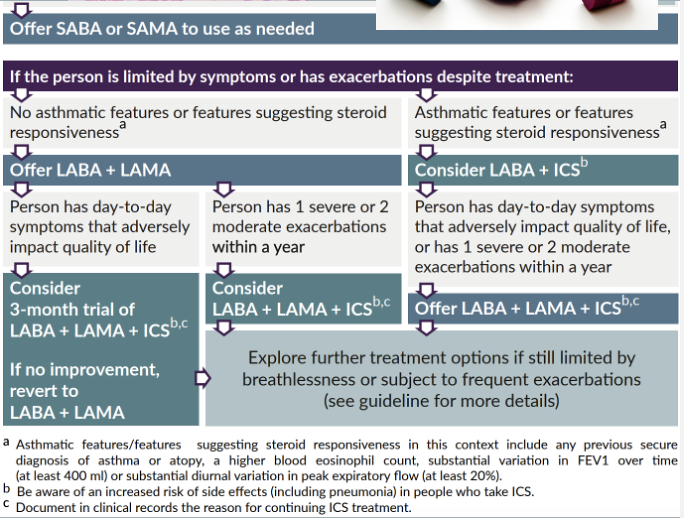
State the Pharmacological management of COPD.
Inhaled therapy:
Short-acting B2 agonists PRN
LABA, LAMA or LABA/LAMA
If 2 exac / year, or one hospital admission – start ICS/LABA. Not ICS monotherapy
If persistent sx / exac – triple therapy
Consider nebulizer therapy
Oral methylxanthines (e.g. theophyllines)
Oral steroids
Mucolytics
→ Nebs – if pt unable to use inhalers / disabled or distressed with SOB despite maximal inhaler therapy. Significant placebo effect
→ Theophyllines – only continue if sx improve. Method of action is unclear – may have anti-inflammatory effect. Care regarding therapeutic/toxic levels (esp in elderly)
→ Carbocisteine: 4 week trial period. Meta-analyses – cause significant decrease in number of COPD exac and decrease number of days of disability (may only apply if not on ICS). Worth trying in mod to severe COPD with severe / prolonged exac, or those repeatedly hospitalized. Caution in peptic ulcer disease
What type of inflammation do COPD patient have?
Chronic worsened by smoke and recurrent infections
Describe how the following thing can occur.
Cor Pulmonale / Pulmonary Hypertension secondary to lung disease
Thickened pulmonary arteriolar wall and remodelling with hypoxia
Leads to increased pulmonary vascular resistance, pulmonary hypertension and impaired gas exchange
→ Also inactivity and deconditioning, muscle weakness and wasting: vicious cycle
How is COPD diagnosed?
Spirometry: FEV/FVC <0.7 post bronchodilation
With respiratory symptoms
Minimal bronchodilator reversibility (<15%) and minimal steroid reversibility
Raised TLC, FRC and RV
Decreased TLco and KCO (emphysema reduces surface area available for gas diffusion)
Imaging is not necessary for dx but CXR will show hyperinflation
Consider: alpha1-Antitrypsin levels, FBC, TFT, CRP, ECG/Echo
→ FEV1 measurement of choice to assess progression / prognosis but it correlates weakly with degree of dyspnoea and changes in FEV1 do not reflect decline in pt’s health
→ CXR: hyperinflated lung fields, attenuation of peripheral vasculature ‘black lung sign’: >7 posterior ribs. Flattened diaphragms. More horizontal ribs. May see bullae – can look like pneumothoraces
→ Symptom based
What other pharmacological managements are available for COPD?
Prophylactic antibiotics: Azithromycin (no evidence in current smokers). 250mg 3x/week if >/= 4 exac despite optimal inhaled therapy. Prior to start – ECG, LFTs, sputum including NTM. Repeat LFTs after 4 weeks. Assess response 3-6 months. Counsel re: hearing loss / tinnitus
Long Term Oxygen Therapy (LTOT)
Vaccination – influenza + pneumococcal
Palliative care / respiratory sedation: morphine / lorazepam / diazepam
Phosphodiesterase-4 inhibitors: Roflumilast (FEV1 <50% and >/= 2 exacerbations in past 12 months despite triple therapy)
MABs/Biologics – watch this space! Dupilumab reduces exacerbations by up to a third in some studies, likely a select patient population
What are COPD exacerbations?
Acute worsening of symptoms resulting in additional therapy
Frequency increases with COPD severity
What are the causes of COPD exacerbations?
mainly viral (rhinovirus, RSV, influenza, parainfluenza, coronavirus, human metapneumonovirus and adenovirus). Others – bacterial (commonly Haemophilus influenzae, streptococcus pneumonia and Moraxella catarrhalis) and environment
What are the symptoms of COPD exacerbations?
cough, increased sputum, SOB, wheeze, worsening RVF
Describe the pathophysiology of COPD exacerbations
increased airway resistance due to bronchospasm, mucosal oedema, increased sputum. Worsens expiratory flow limitation, prolonged expiration (further limited by SOB). Promotes dynamic hyperinflation:causes mechanical compromise. Accessory muscles, thoraco-abdominal dyssynchrony
Describe the general management of AECOPD.
Assess severity
Controlled oxygen
Nebulised bronchodilators (salbutamol 2.5mg and ipratroprium250mcg). With air not O2
Oral steroids (Prednisolone 30mg 5 days – consider wean)
Consider antibiotics
(IV aminophylline)
Consider NIV / ICU
DVT prophylaxis
Early mobilization, nutrition
Consider ‘hospital at home’
What are the Surgical / interventional treatment viable for COPD?
Lung transplant
Bullectomy
Lung volume reduction techniques
Endobronchial valves – bronchoscopic lung volume reduction surgery (bLVR)
Other endobronchial treatments
Lung volume reduction surgery
Based on NICE guidance how should be treat COPD?
Combo B2 agonist CMP pathway and LAMA cGMP pathway both relax smooth muscle in airways
High eosinophils use triple therapy inhalers
small risk using iCS with pneumonia
if baseline COPD bad nebuliser may make it Asia to get drug in
What is NTM?
Non tuberculosis mycobacteria
ensure NTM not here as if use prophylactic drug can be harder to treat in the future
What biologic has best evidence in COPD?
dupilumab
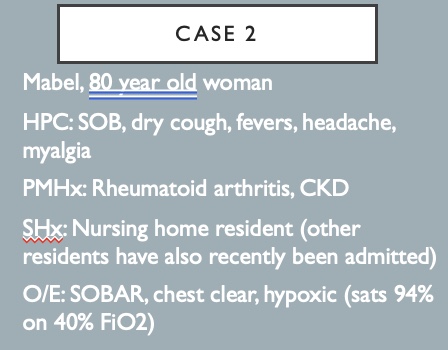
For this case answer the following questions
What’s the likely diagnosis?
What acute treatment does he need?
What longer term tests / management might you suggest?
viral pneumonia
altixamavir as first line for couple of days
Give O2
Make sure patient gets vaccine and jabs
What is Viral pneumonia?
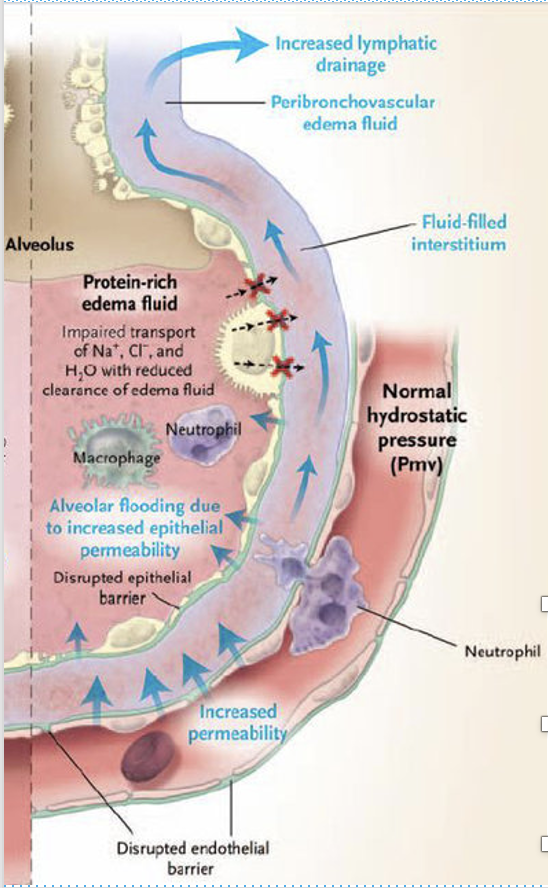
Abnormalities of oxygen and carbon dioxide gas exchange at the level of the alveoli, secondary to viral-mediated and/or immune response-mediated inflammation.
→ virus reduces ability to fight infection so high risk of getting secondary bacterial infection
What are the complications of Viral pneumonia?
Superadded bacterial infection / abscess/empyema/pleural effusion
Sepsis with secondary multi-organ failure
Acute respiratory failure
Cardiovascular collapse
Acute respiratory distress syndrome (ARDS)
What are the outcomes for patients with VIRAL PNEUMONIA?
Most healthy people with pneumonia recover well
Prognosis is guarded in immunocompromised/extremes of age
Several viruses cause severe bronchiectasis
10-40% of children suffer irreversible lung damage after adenovirus pneumonia
What populations are at risk of getting viral pneumonia?
Traditionally a disease predominantly of the very young, the elderly, and the immunosuppressed.
Of particular concern in pregnant women
Longer life spans & early infant survivability
Increasing number of people taking immunosuppressive treatments for cancer & auto-immune conditions
HIV
Increased incidence of organ transplantion
Obesity
(COVID-19)
What conditions can predispose someone to viral pneumonia?
Trauma/severe burns
Uncontrolled diabetes
Malnutrition / poverty / Group living
What are the different types of viral pneumonia?
Divided into DNA or RNA as nucleic acid (more useful to divide by clinical syndromes)
COVID-19: RNA.
Influenza A, B & C: RNA. Greatest cause of mortality. Multiple subtypes – e.g. Avian (H5N1), Swine (N1N1)
Respiratory Syncytial virus (RSV): RNA. Most common cause in small children/infants
Rhinovirus: RNA. Common URTI but uncommon cause of viral pneumonia
Parainfluenza: RNA. Young children, seasonal.
Other coronaviruses: RNA. Human bocavirus coronavirus (MERS: initial mortality rate 30%). Human metapneumovirus (SARS).
Adenovirus: DNA. In people with solid organ/haematological transplantation
Measles. RNA: in children (rising since vaccination falling)
Others: Enterovirus, VZV, Hantavirus, EBV, Human Herpesvirus 6&7, HSV, CMV
→ Don’t really need to know
Describe the general pathophysiology of viral pneumonia.
The submucosa of the alveoli is targeted, causing inflammation and secondary oedema, microhaemorrhage, and cellular immune reaction.
Cellular reaction consists of mononuclear lymphocytes and progresses to polymorphonuclear neutrophil recruitment. Fibrin is released.
CD4 and CD8 cells begin a cascade of immune product secretion that can end in increased vascular permeability and oedema.
May lead to intra-alveolar organization and an obliterans clinical picture.
Can develop into interstitial pneumonia, pulmonary oedema, and cardiogenic shock
Describe the pathophysiology of influenza.
3 subtypes: A, B & C. A more virulent & more frequent. C milder/asymptomatic
A&B can be further categorised into subtypes depending on principle H & N antigens:
H = hemagglutinin: protein, causes red blood cell agglutination (sticking together)
N = neuraminidase, enzyme that cleaves glycosidic bonds of monosaccharide sialic acid
There are 18 known types of H and 11 known types of N, so theoretically198 different possible combinations
•Transmission occurs via droplets, aerosols or direct contact with respiratory secretions: usual incubation is 1-3 days.
Rarely causes cardiac or neurological complications.
Usually self-limiting with recovery 2-7 days but can be severe
→ Try and predict
Describe the pathophysiology of Covid 19.
4 structural proteins (Spike, Membrane, Envelope, Neucleocaspid): Binds to ACE-2 & Enters cells
Asymptomatic phase → invasion URT → LRTI → ARDS
Treatment targeted at two stages of infection response – viral replication and then inflammatory response
Postmembrane fusion, virus enters pulmonary alveolar epithelial cells + viral contents are released into host cell – replicates (RNA transcription)
Cytokine storm: inflammatory response to fight virus but causes lung inflammation and lung injury
White cells sequestered in lung tissue
Host cell apoptosis
Diffuse alveolar damage leading to ARDS
→ Binds to ACE2 → why effects lags a lot
ACE 2 prevalent in pulmonary epithelium
How is viral pneumonia diagnosed?
Used to be a diagnosis of exclusion.
No specific history clues. Higher clinical suspicion in certain patients. Clues on exam – sx of URTI, rash, physical exam out of keeping with illness. Bilateral findings.
Blood tests: Generally less rise in WCC. Lymphopenia is common but non-specific. CRP may be raised but less than in bacterial infection.
Chest x-ray/CT: alveolar infiltrates, patchy bilateral interstitial infiltrates. Or normal chest x-ray.
What tests are there for specific viruses?
Polymerase chain reaction (PCR) is replacing viral cultures/titres. Much quicker, no need for invasive sampling techniques, more sensitive and specific
ELISA for specific pathogens e.g. HSV, RSV, ‘flu A&B, CMV. Doesn’t always indicate active disease.
COVID-19: rapid point of care tests (nucleic acid amplification methods, lateral flow/ELISA/CLIA, biosensors) and PCR.
What specific tests need to be carried out in Covid-19?
Bloods:
Poor prognostic signs: neut:lymph >3, thrombocytopenia <100, High D-dimer (3-4x), CRP >125, High troponin
Also see mildly raised PT, transient transaminitis, mild AKI
SARS-COV-2 Spike Antibody
ECG / echo – myocarditis/cardiomyopathy/dysrthymia/MI
What are the treatments for viral pneumonia?
Traditionally, the treatment of viral pneumonia was supportive care:
Supplemental oxygen +/– intubation & ventilation
Fluid management & replacement
Temperature control, cough treatment
Treatment of concomitant bacterial pneumonia
Meet increased calorie needs
Now, there are specific and effective treatments for certain viruses
Ribavirin: RSV, Parainfluenza, adenovirus, measles
Acyclovir: HSV & VZV
Ganciclovir/foscarnet: CMV
Remember isolation/cohort bay and PPE
Look for and treat superadded bacterial pneumonia
Importance of prevention: immunization, education, prophylaxis
What are the treatments for influenza?
Usually managed in the community, doesn’t require treatment in the healthy
For those at risk or pregnant, or complicated infection: Oseltamivir (or zanamivir if resistant strain). Interrupt function of neuroaminidase on virus surface, preventing release of viral particles from infected host cells
Should start within 48 hours of symptom onset: May help even if up to 5 days but unlicensed
Some strains more likely to develop resistance to oseltamivir (e.g. A H1N1 pdm09) – higher in the immunosuppressed
Secondary bacterial infection are a major cause of death: pneumococcus, staph aureus, streptococcus, haemophilus
Prevention: Annual influenza vaccine and Prophylaxis – for contacts in an at risk group: zanamivir or oseltamivir
What are the pharmacological treatments for covid?
Antivirals: Paxlovid
Remdesivir
Sotrovimab
Dexamethasone
Tocilizumab (or Sarilumab)
Baricitinib
What pathogen factors determine whether TREATMENT FOR COVID-19 is needed?
Covid variant. There are no current variants of concern. Omicron = variants of interest
Time course of infection
What risk factors increase the risk for progression to sever disease for Covid 19?
Down’s syndrome
Solid cancers
Haematological diseases, stem cell transplant
Sickle cell disease, thalassaemia
Renal disease (transplant, CKD 4 or 5)
Liver disease
Solid organ transplant
Immune-mediated inflammatory disorders
Asthma – on oral steroids, frequent exacerbation
COPD home NIV / LTOT, moderate or severe disease (EEV1 <50%)
ILD
Immune deficiency
Neurological disorders and dementia
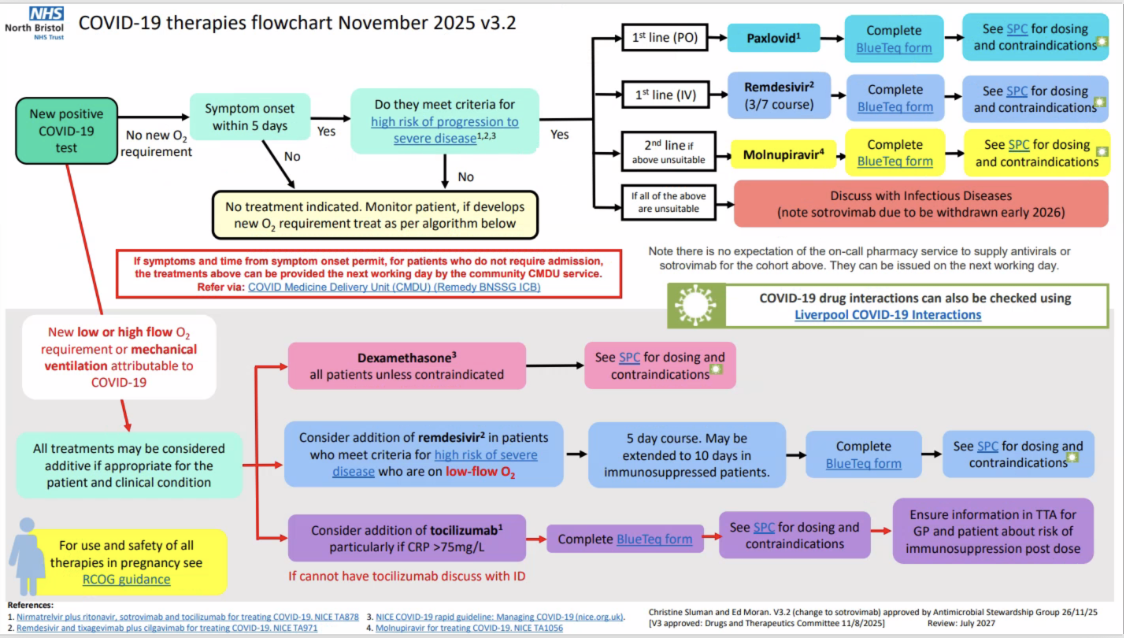
Outline the Covid 19 therapies flowchart
DONT memorise
What are some of the the other pharmacological treatments/adjuncts for Covid 19?
Consider Oseltamivir while influenza/viral swab awaited
Active management of cough and dyspnoea: opioids or benzodiazepines
Additional Adjuncts to consider: Paracetamol, nebulisers may have a limited role in specific cases (0.9% sodium chloride, salbutamol), Carbocisteine, regular medications
Nutrition and bowel management
Many patients with COVID-19 experience diarrhoea).
Ensure adequate calorific intake.
Describe the use of VTE for the treatment and prophylaxis of Covid 19.
High reported prevalence of VTE in COVID-19
Also other coagulopathy e.g. line clots, DIC, high D-Dimers, high target anti-Xa levels
Low threshold for CTPA to look for PE
VTE must be prescribed in absence of CI. Hold if PLT <75 – but consider giving if 50-75 in high risk cases (>25 on ICU)
For conventional supplemental oxygen – therapeutic dose, for 14 days or until discharge
HFNO/CPAP (or not on oxgen) – standard prophylactic dose (unless PE/DVT/other reason for high dose)
Describe the use of antibiotics for the treatment of Covid 19.
ONLY if evidence of superadded bacterial infection (majority will not require) e.g. lobar pneumonia, neutrophilia, productive cough
CRP can be raised in severe disease which can make it difficult – clinical judgement
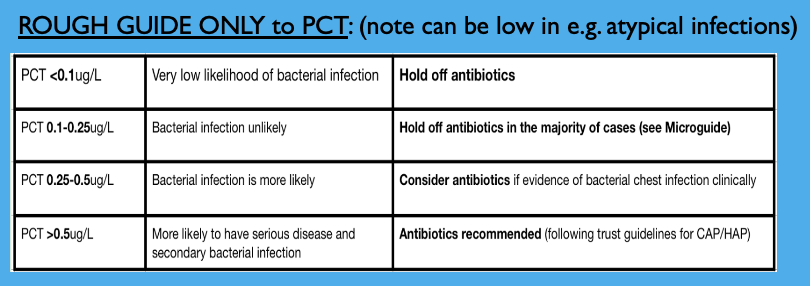
PCT therefore used as an additional aid. Repeat if deteriorates & after 3 days.
What is BRONCHIECTASIS?
Irreversible abnormal dilatation of one or more bronchi, with chronic airway inflammation.
What are the clinical features of BRONCHIECTASIS?
chronic sputum production, recurrent chest infections and airflow obstruction.
Describe the pathophysiology of BRONCHIECTASIS.
Initial (usually infectious) insult – damage to the airway. Disordered anatomy leads to secondary bacterial colonization, perpetuating inflammatory change and damaging mucociliary escalator. Prevents bacterial clearances, leads to further airway damage. Mucosal oedema, inflammation, ulceration. Chronic host inflammatory response
Bronchial neovascularization (hypertrophy and tortuosity of bronchial arteries) may lead to intermittent haemoptysis
Describe and explain the aetiology of BRONCHIECTASIS.
Many and varied causes
Idiopathic in c. 50%
Congenital: pulmonary sequestration
Post-infective (TB, whooping cough, severe pneumonia, ?NTM)
Immunodeficiency: primary (e.g. CVID), secondary (HIV, CLL, nephrotic syndrome)
Mucociliary clearance abnormalities:
Airway diseases: cystic fibrosis, primary ciliary dyskinesia, COPD, asthma, ABPA
Toxic insults: aspiration, inhalation (toxic gases, chemicals)
Mechanical insults: foreign body aspiration, extrinsic lymph node compression, intrinsic obstructing tumour
Associated diseses: rheumatoid arthritis / other connective tissue disease, ulcerative colitis and Crohn’s, chronic sinusitis, yellow nail syndrome, Marfan’s
Describe the management of BRONCHIECTASIS
Treatment of underlying medical condition / associated airflow obstruction
Daily physiotherapy / airway clearance
Optimize nutrition
Pulmonary rehabilitation if breathless
Surgery – rare, localized resection
Lung transplantation
Antimicrobials: intermittent for exacerbations, or long term prophylaxis. Based on sputum results (in vivo sensitivity may be different to in vitro). Higher abxdose and for 10-14 days
Describe the management of BRONCHIECTASIS for Pseudomonas colonized patients
More frequent exacerbations, worse CT appearances, faster decline in lung function
First isolate of Pseudomonas aeruginosa:
Initial rx 2/52 PO Ciprofloxacin 500-750mg BD (counsel re: photosensitivity and tendonitis risk, long QT / known vascular aneurysm)
If fails – IV abx (min 2/42) and nebulized colistin, gentamicin or tobramycin for 3 months
Combination IV abx (anti-pseudomonal penicillin and aminoglycoside) are only needed if lack of clinical response and/or resistance
Consider long-term therapy with daily nebulized colistin or gentamicin in colonized patients with frequent exacerbations (may be in combination with macrolide).
Challenge testing required prior to starting neb abx – risk of bronchoconstriction
Describe and explain the use of Prophylactic Macrolide antibiotics in BRONCHIECTASIS.
Both antibacterial and immunomodulatory properties
Decrease mucous production, alter inflammatory mediator release and inhibit pseudomonas virulence factors and biofilm formation
Reduce exacerbation rates and improve lung function and symptoms
Counsel re: hearing loss.
LFTs at 1 months then 8 weekly.
Avoid if CrCl <30ml/min.
Avoid concomitant nephrotoxics
Baseline ECG – QTc
Exclude NTM
Azithromycin 25—500mg 3 x/week or 500mg twice weekly
Antibiotic holiday’ may be taken
What are some of the further managements used in the treatment of BRONCHIECTASIS?
Self-management plan
Treatment of associated airflow obstruction / wheeze
B2 agonists may enhance airway clearance
Nebulized 7% hypertonic saline – but NB bronchospasm
Acetylcysteine
Vaccinations
Rx reflux and associated rhinosinusitis
Nutrition
Immunoglobulin replacement therapy
Oxygen
Surgery / transplant
What is Cystic Fibrosis?
CF is a genetic cause of bronchiectasis. Recessive.
Multi-system disease due to mutations in the gene encoding the CF transmembrane conductance regulator (CFTR) – a complex chloride channel. Causes inadequate hydration of mucous secretions. Different gene mutations exist which effect different parts of the CFTR and correlate with varying severity – commonest=F508 deletion
Lungs – causes defective mucociliary clearance, mucus obstruction and colonization with pathogenic bacteria. Recurrent infection leads to bronchiectasis.
Pancreas – exocrine ducts blocked by secretions, leading to pancreatic destruction, pancreatic enzyme insufficiency, and CF diabetes
Respiratory management acutely and chronically is largely as for other forms of bronchiectasis
BUT recent advances with CFTR modulators have transformed the disease
Now, c. 95% of all patients with CF in the UK are eligible for…
modulator therapy
Pricing and access have been controversial
Future: gene therapy for cystic fibrosis…(watch this space!)
Describe the use of CFTR modulators in the management of cystic fibrosis.
Directly target the basic defect underlying CF
Orally bioavailable drugs, effective in specific mutations
Small molecule CFTR modulators increase CFTR channel opening at cell surface (’potentiators’), or increase the amount of cell surface CFTR protein (‘correctors’)
Ivacaftor (Kalydeco) was first - CFTR potentiator effective in patients with gating mutation (c. 5% of CF patients). Then combined to form other drugs:
Tezacaftor-Ivacaftor (Symkevi/Symdeko) works in patients hetero-zygousfor F508del (or heterozygous with residual function mutation) – the most common mutation
Lumacaftor-Ivacaftor (Orkambi) – homozygous F580del (c. 50% of CF patients)
What triple therapies are available for the treatment of cystic fibrosis?
Elexacaftor/tezacaftor/ivacaftor (Kaftrio) the first triple therapy. Demonstrated significant improvements in lung function & QoL & reduction in sx. Must have at least one F580del to qualify
Vanzacaftor/tezacaftor/deutivacaftor (Alyftrek). At least one F508del variant. As good as Kaftrio maybe better
Newer triple therapies are often also effective in other, rarer CFTR variants and use is being expanded
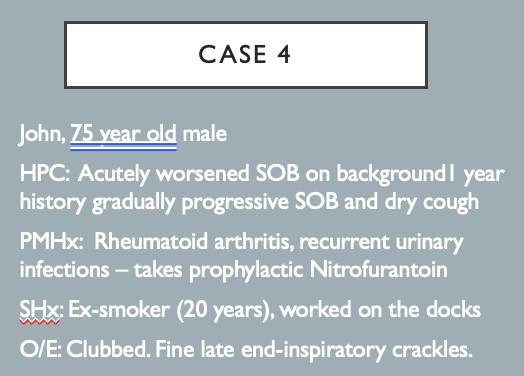
For this case answer the following questions
What’s the likely diagnosis?
What acute treatment does he need?
What longer term tests / management might you suggest?
acute exacerbation of PF
possibly try and allude bacterial infection
If survive educate on PF and give Abx if eligible
What are PULMONARY FIBROSIS?
A group of diffuse lung diseases that involve the pulmonary interstitium(hence also called interstitial Lung Disease / ILD). Interstitium=area between alveolae and capillary as well as the fibrous lung framework.
What are the subtypes of PULMONARY FIBROSIS?
Commonest=Idiopathic pulmonary fibrosis (IPF). Other subtypes are rarer, include e.g. non-specific interstitial pneumonia (NSIP), cryptogenic organizing pneumonia (COP).
What are the clinical features of PULMONARY FIBROSIS?
Can vary slightly with subtype but generally slow and progressive onset, dry cough, sometimes systemic symptoms (e.g. weight loss) over months to years. Inspiratory crackles and squeaks, sometimes clubbing, when advanced can show cyanosis and signs of right heart failure
What things are normally associated to PULMONARY FIBROSIS?
Vary by subtypes but include: smoking; connective tissue diseases (e.g.RA); asbestos exposure; certain drugs e.g. Nitrofurantoin, Amiodarone, Bleomycin; some infections e.g. HIV/PCP
Describe the pathophysiology of PULMONARY FIBROSIS
Largely unknown. Each subtype has its own triggers and pathways but the underlying process of all is one of varying degrees of inflammation and fibrosis.
How is Idiopathic Pulmonary Fibrosis (IPF) diagnosed?
MDT diagnosis – using clinical features, PFTs, HRCT chest and (if biopsy taken) histological features / features from broncho-alveolar lavage
What is the variable prognosis of Idiopathic Pulmonary Fibrosis (IPF)?
Many are stable/decline slowly
A subgroup decline more rapidly (usually male smokers)
5-20% have rapid progression after an acute exacerbation (often inpatient admission)
State the general principles of the management of Idiopathic Pulmonary Fibrosis (IPF)
In context of clinical condition, co-morbidities and patient wishes
Pulmonary rehabilitation
Supportive treatment E.g. home oxygen, opioids
Anti-fibrotics – covered on next slides
Clinical trials
Lung transplantation if eligible and meets criteria
Describe the use of Anti-fibrotics: Slow progression of fibrosis in PULMONARY FIBROSIS
Initiation by specialist ILD centres with MDT.
Initially for those with FVC 50-80%, now FVC >50%
Initially only for IPF but use is expanding in other forms of ILD
Exclusions include inability to tolerate side effects (e.g. intolerable diarrhoea / weight loss), interaction with other medications and bleeding risk
Stop if progression of disease (>10% FVC decline over 12 months)
What Anti-fibrotics are available for PULMONARY FIBROSIS?
Two drugs currently available:
Pirfenidone: inhibits collagen synthesis, reduces fibroblast proliferation
Nintedanib: tyrosine kinase inhibitor
Both drugs associated with GI side effects (diarrhoeaalmost always present)
Both can cause LFT derangement. LFT and FBC monitoring monthly for the first 6 months and 3 monthly after.
Available on a commercial arrangement with drug companies. Nintedanib more expensive - £2,151.10 per pack of 60 capsules, vs £501.92 for 63 capsules (c. £75/day)
Compare Anti-fibrotics: Nintedanib vs Pirfenidone
Bleeding risk with Nintedanib: Common but usually mild (e.g., epistaxis/bruise), but can be serious, sometimes fatal. Due to inhibition of vascular endothelial growth factor (VEGF). Caution is advised with full-dose anticoagulation
Drug interactions may dictate choice
Nintedanib contraindicated in peanut/soya allergy
Pirfenidone: Increased sensitivity to sunlight (caution with concurrent Doxycycline and must use factor 50 and cover up)
Religious/vegetarian considerations – some Nintedanib formulations contain gelatin/ porcine products
Describe and explain the management for the acute exacerbations in PULMONARY FIBROSIS.
An otherwise unexplained acute worsening of dyspnoea in someone with pulmonary fibrosis
Mechanism is poorly understood, viral infections may act as a trigger.
Important cause of death in otherwise apparently stable IPF and increasingly recognized in other forms of ILD such as CTD-associated and NSIP
Inpatient mortality is >60%, rising to 90% within 6 months of discharge
Outcomes for patients with fibrotic lung disease who undergo intubation and ventilation is poor (mortality approaches 100%) – ICU not usually appropriate
HRCT typically shows extensive “ground glass” (reflects inflammation) and/or consolidation on a background of fibrotic changes
Important to exclude/consider/treat for other causes of exacerbation e.g. superimposed bacterial or opportunistic infection, pulmonary embolism, pneumothorax, cardiac dysfunction
Treatment usually with high dose steroids (e.g. IV Methylprednisolone 750mg-1g for 3 days)
In practice, infection is often difficult to exclude and often treat with broad-spectrum antibiotics as well
ANTIVIRALS: NIRMATRELVIR AND RITONAVIR (PAXLOVID)
Nirmatrelvir is a peptidomimetic inhibitor of coronavirus 3C-like protease which prevents multiplication of SARS-CoV-2. Ritonavir inhibits CYP3A-mediated metabolism of nirmatrelvir thereby increasing the plasma concentration of nirmatrelvir.
300mg (2 pink) and 100mg (one white) BD for 5 days
Evidence suggests it reduces hospitalisation and mortality in at risk patients
£513 for course
Eligibility: <5 days of symptoms. Not on oxygen. Increased risk for progression, or age >70, BMI >35, diabetes or heart failure.
Cautions/CI: Hepatitis, liver disease, uncontrolled HIV
Adverse effects: diarrhoea, altered taste, vomiting. Reduced efficacy contraception
REMDESIVIR
Adenosine nucleotide prodrug. RNA polymerase inhibitor – prevents viral multiplication
200mg IV loading, maintenance 100mg IV for total 5-10 days (5 on ward, up to 10 on ICU)
Probably reduces mortality for non-ventilated patients, with or without oxygen. Unclear benefit in those already ventilated. Effectiveness in omicron uncertain.
Expensive (£1773 for a 5 day course)
Eligibility: <10 days from symptom onset, requires supplemental oxygen, 40kg and over, eGFR >30ml/min, ALT <5x lower limit of normal.
Risk assessment: only for use in patients at high risk of progression to severe disease
Reassess daily: Consider stopping if improves and no longer requires O2 72 hours after rx started/continues to deteriorate despite 48 hours of mechanical ventilation.
Monitor renal & liver function – stop if ALT >5x ULN (can be restarted when drops), liver inflammation or eGFR<30
Cautions/CI: (Pregnancy)
Adverse effects: headache, transaminase elevations, infusion reactions (hypotension, n&v, diaphoresis), hypersensitivity.
SOTROVIMAB
Engineered human immunoglobulin monoclonal antibody that binds to the spike protein receptor binding domain of SARS-CoV-2, which prevents the virus from entering human cells.
Evidence: reduced mortality (OR 0.4) and hospitalisation (OR=0.53), mechanical ventilation (OR=0.57), ICU admission (OR=0.33).
500mg for 1 dose
Costs £2209 for one dose
Eligibility: Within 5 days of onset. Do not need supplemental oxygen. Increased risk of progression to severe disease. Weight >40kg. Paxlovid contraindicated / unsuitable.
Adverse effects: Bronchospasm, hypersensitivity, infusion related reaction, skin reaction
DEXAMETHASONE
6mg PO/NG/IV OD for 10 days (or until discharge)
Evidence: Recovery, REMAP-CAP. 28 day mortality lower (OR 0.66)
For all patients with severe COVID-19 who require supplementary oxygen to maintain saturations >94%
Monitor blood sugars at least OD in all patients and QDS in people with diabetes.
PPI
Cautions: Uncontrolled hyperglycaemia, pt already receiving regular oral corticosteroids
Adverse effects: Hyperglycaemia, mood/sleep disturbance, hypernatraemia
TOCILIZUMAB
IL-6 inhibitor used in RA
Evidence: improved 28 day survival (RR mortality 14% & 24%) & reduced time on ICU by a week
8mg/kg IV (total dose not >800mg) single dose over an hour, via Blueteq
Costs c. £1,000 for one 800mg dose
Eligibility: CRP >/=75, Sats <92% RA/requires oxygen, or within 24-48 hrs of starting NHF/CPAP/IMV
CI: Known hypersensitivity to Toci, pregnancy (contraception 3/12 after rx).
PLT <50, Neut <1, liver enzymes 10x normal
Cautions: Co-existing infection, ALT >5x ULN, immunosuppression
Note: CRP levels may be depressed for some time after Toci(missed infeections/atypical presentations of e.g. GI perforation)
Adverse effects: URTI, nasopharyngitis, headache, HTN, raised ALT
SARILUMAB
IL-6 inhibitor used when Tocilizumab not available
Dose: 400mg one off dose via Blueteq
Eligibility: CRP >/=75, Sats <92% RA/requires oxygen, or within 24-48 hrs of starting NHF/CPAP/IMV
CI: Known hypersensitivity to Sari, pregnancy (contraception 3/12 after rx).
PLT <150, Neut <1, liver enzymes 5x normal
Cautions: Co-existing infection, immunosuppression
Note: CRP levels may be depressed for some time after (missed infeections/atypical presentations of e.g. GI perforation)
BARICITINIB
Inhibits JAK1 and JAK2 tyrosine kinases
Evidence: Lower mortality (OR=0.62), lower mechanical ventilation (OR=0.61)
Costs £805 for one tablet
Eligibility: Need supplemental oxygen, are receiving corticosteroids, no evidence of bacterial infection and who cannot have tocilizumab or are deteriorating despite tocilizumab
CI: Lympocytes <0.5, neutrophils <1, haemoglobin <80, active tuberculosis
Cautions: Active, chronic or recurrent infection, age >65, cardiovascular risk factors, risk factors for VTE, malignancy, diverticulitis or viral reactivation. Live vaccines not recommended during rx
Adverse effects: abdo pain, dyslipidaemia, headache, herpes zoster, nausea, skin reactions, thrombocytosis, VTE, facial swelling, cardiovascular event, weight gain, GI perforation, hypersensitivity, malignancy