L1: Responses to fasting
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
What is metabolism
chemical procosses required to sustain life
Unit of ernegy
calories
heat energy required to raise the temperature of 1 gram of water from 14.5-15.5
One calorie is how many joules
4.186 joules
1 Calorie (capitalized)= one kilocalorie
Aim of the lecture
see how long you could last without eating by considering
Rate of energy expenditure of the body
measure our fat reserves
How hormones guide fasting metabolism
Consequences of long-term malnutrition
Metabolic rate
rate at which energy is consumed by the body
Average requirement of energy used
8500 kJ day-1
rising to 30,000 kJ day-1 with very hard labour
What is metabolic rate affected by
Sleep→ 10% decrease
Fasting (up to 40% decrease, due to lower thyroid hormone level)
Post-prandial thermogenesis→ up to 40% increase
after eating
when food is processed in the liver
Nitrogen metabolism→ heat
Temperature
Thermoregulation demands energy
body temp itself directly affects rate of metabolic reactions
Muscle: fat ratio
Differs in men and women
muscle uses more energy
Exercise
metabolic rate can typically be increased to x10 BMR or up to 20x in trained athletes
Growth, gestation and lactation
Pathologies
Hormone imbalances
variations in levels of thyroid hormone
can alter BMR from 40-200% of normal
Growth hormone and testosterone have similar effects
hypothydroi→ ½
hyper→ x2
How to compare metabolic rates: Basal metabolic rate BMR
Energy consumptin in the resting , post absoprtive state
12-14 hours after last meal
thermoneurtral environment
no shiver or sweat
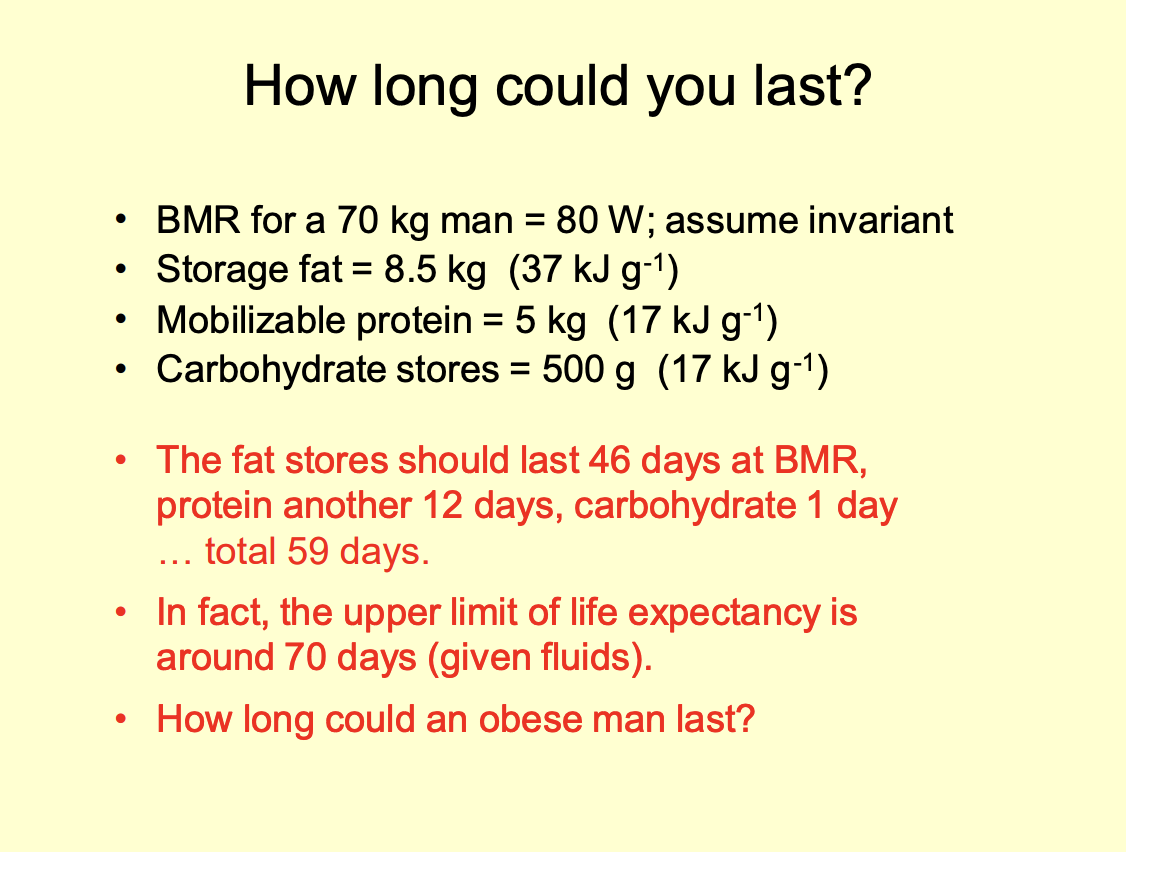
What is the average BMR
80W in a 70kg man
What is BMR due to
activities including
ionic pumping
necessary muscle function
protein metabolism
basal secretion of glands
How is BMR assessed
Indirect calorimetry
Measure rate of oxygen consumption in STP
estimate energy production as 20.2 kJ litre -1 O2 consumed
assumes that metabolism is based on 40% carb and 60% fat (RQ=0.82)
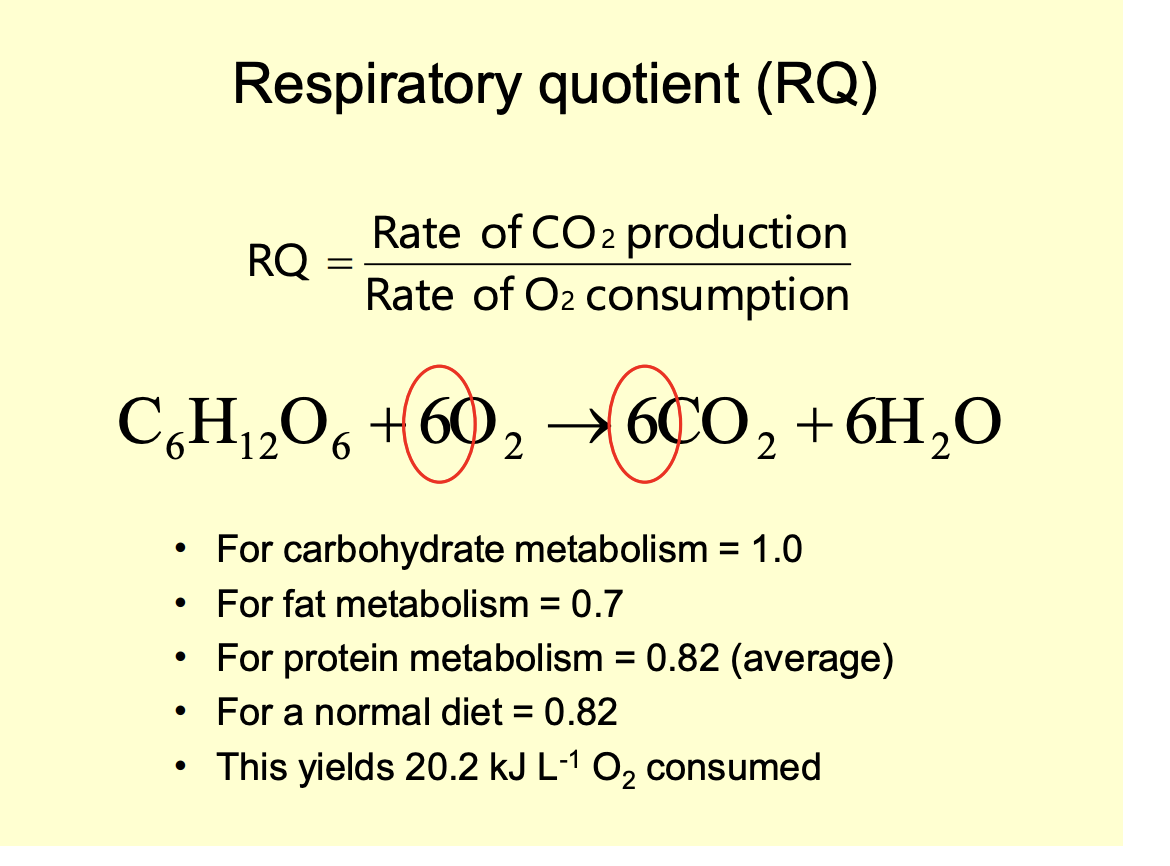
Note on respiratory questions
Normal→ 0.82
never really fully one fuel used or the other
metabolism is like dials→ not an on and off switch
RQ= Rate of CO2 production/ rate of O2 consumption
Respiratory question: average diet
45% carbs→ 17 kJg-1
40% from fats→ 37kJ g-1
15% from proteins→ 17kK g-1
given losses from incomplete metabolism
When may RQ exceeed 1
when rate of fat synthesis from glucose is unsually high
Next thing to measure: Energy stores→ fat: different types of fat
Essential fat→ cannot be used/broken down→ 2kg in 70kg man
CNS (myelin sheath)
Lipid membranes
Storage fat→ 8.5 kg in 70 kg man
can be used for energy
Average fat % in man vs women
Man: 15% body mass
Essential→ 2 kg
Storage→ 8.5 kg
Woman: 27% body mass
Essential→ 7 kg
Storage→ 8.5 kg
What is Visceral fat
found in the abdominal cavity
Why is this fat assoicated with great risk of disease
Broken down
goes to the liver
changes metabolism
great predisposition to metabolic disease:
Type II diabetes
hypertension
atheroscleosis
comapres to subcutaneous fat
Android vs gynoid districubtuion of subcutaneous fat
Android→ ‘manlike’
around abdomen
apple shaped
more dangerous
Gynoid→ ‘woman like’
hips and thighs
Pear shaped
Ways to measure body fat
Body mass index
Underwater weighing
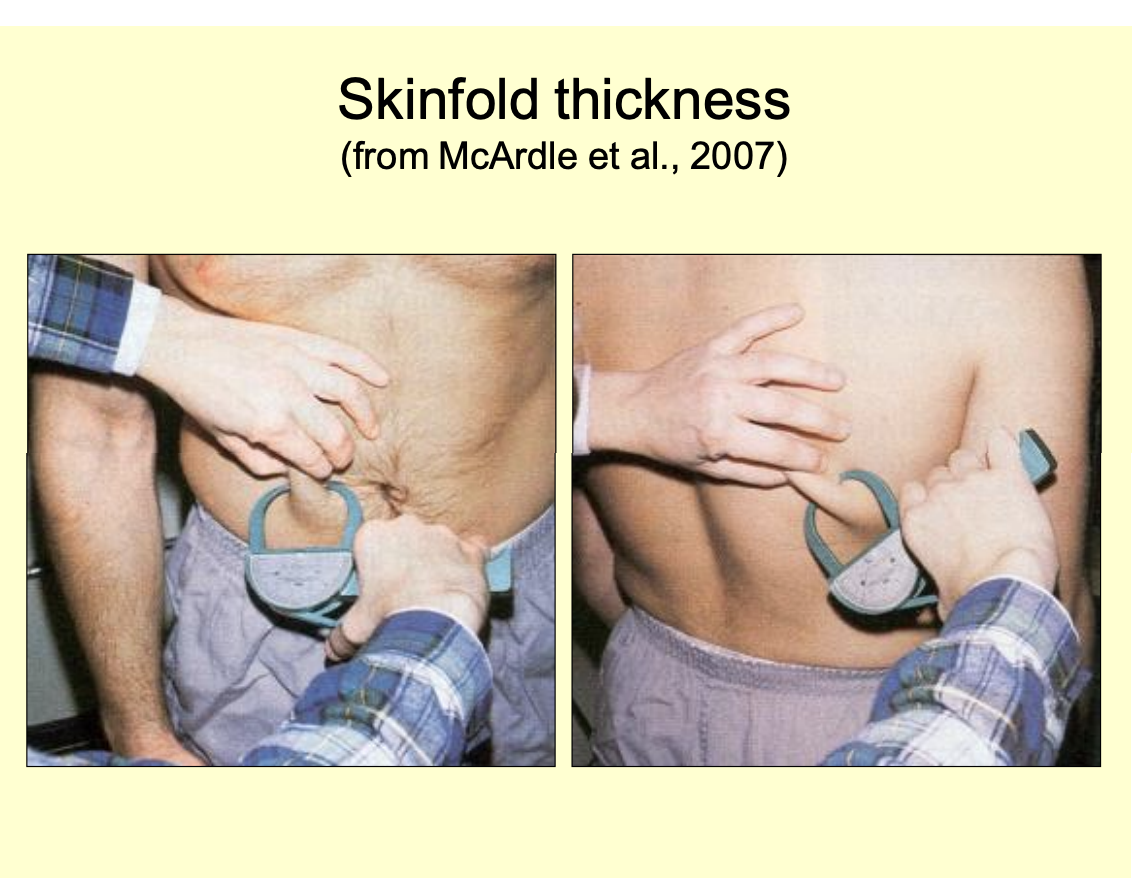
Skin-fold thickness
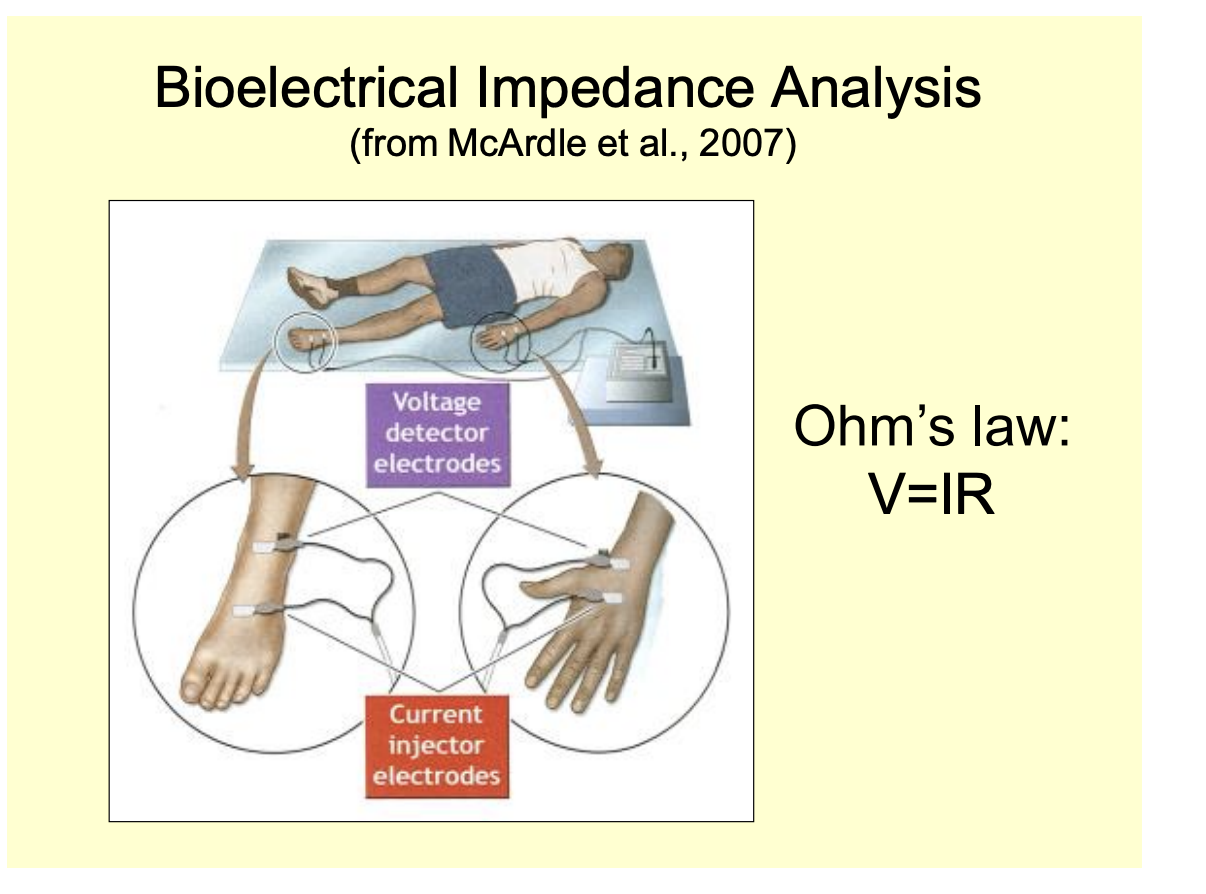
Bioelectrical impedance analysis
Others
Body Mass index (BMI)
BMI= Mass in kg/ Height²
Crude measure of ‘fatness’
Forms different risk categories of diseases
these categories are different for different populations
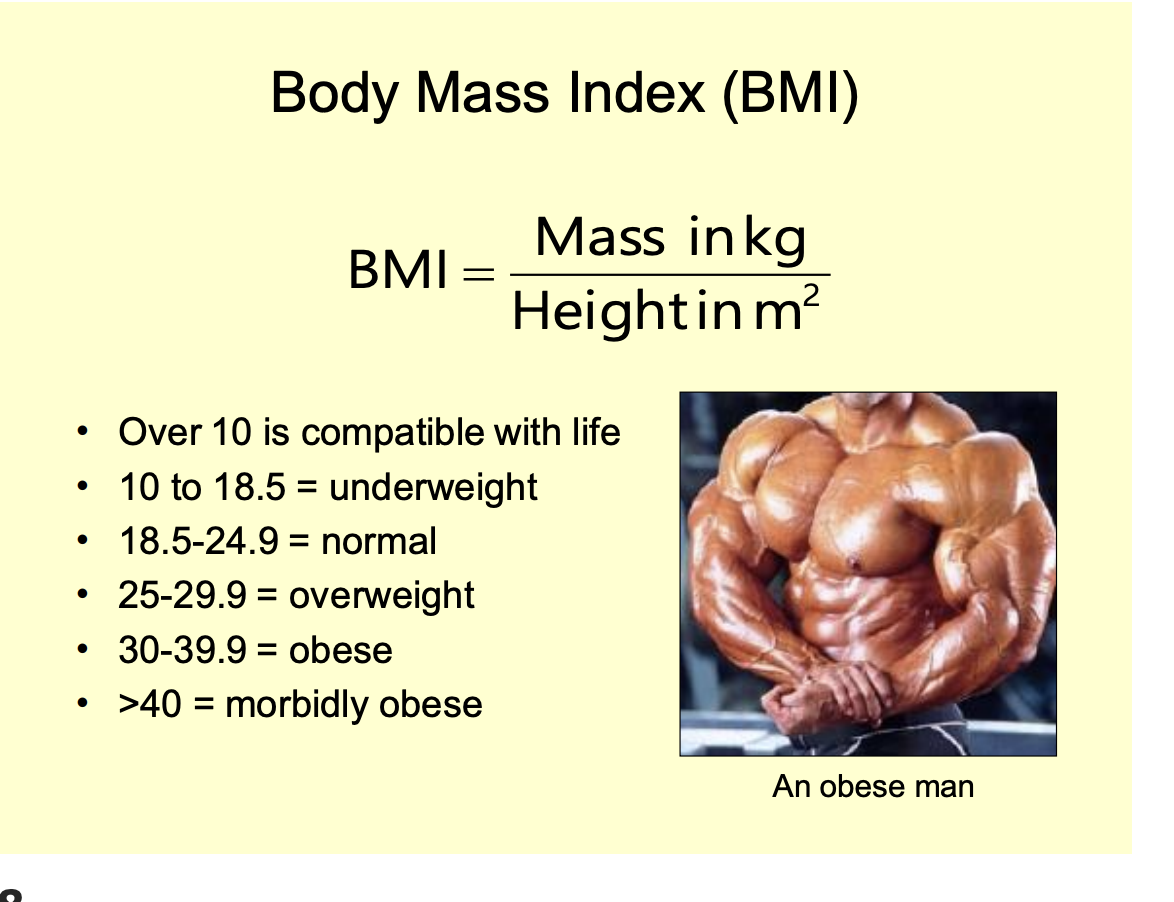
Problems with BMI
Cannot distinguish between muscle and fat (or odema)
risk categories differ between populations
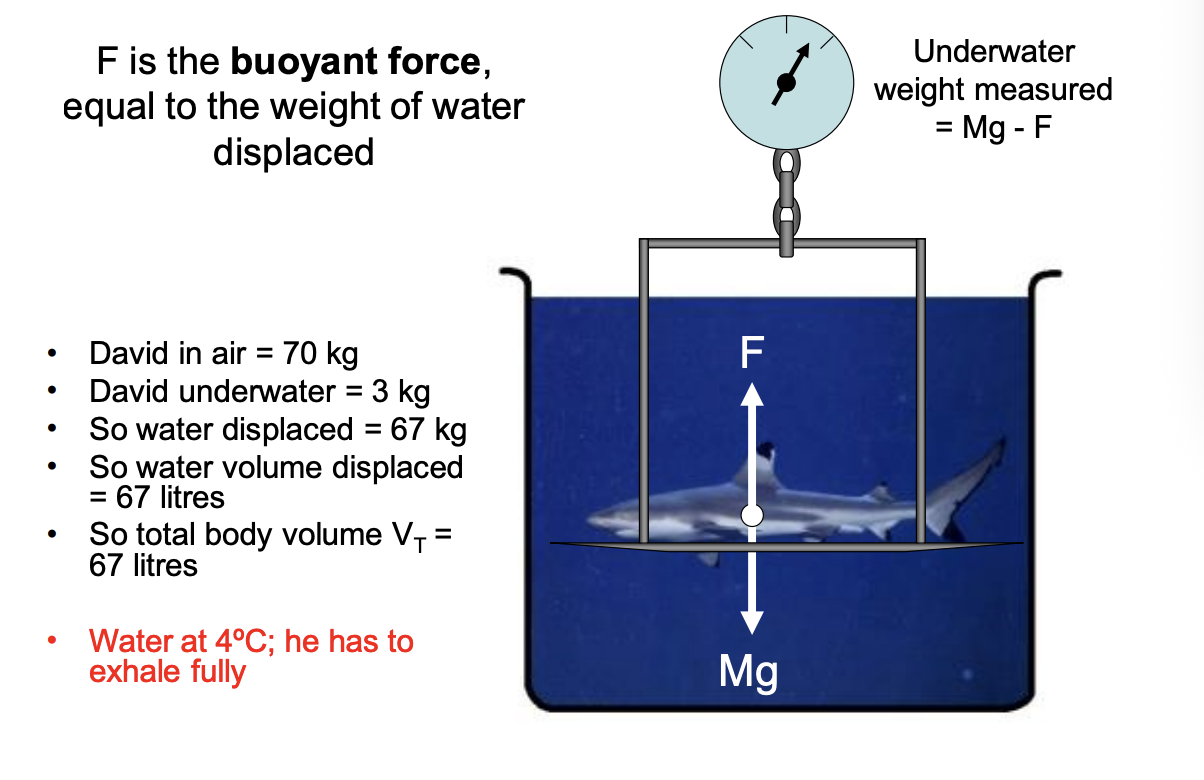
Underwater weighing
One of the most accurate wats to assess body fat percentage
How does this work?
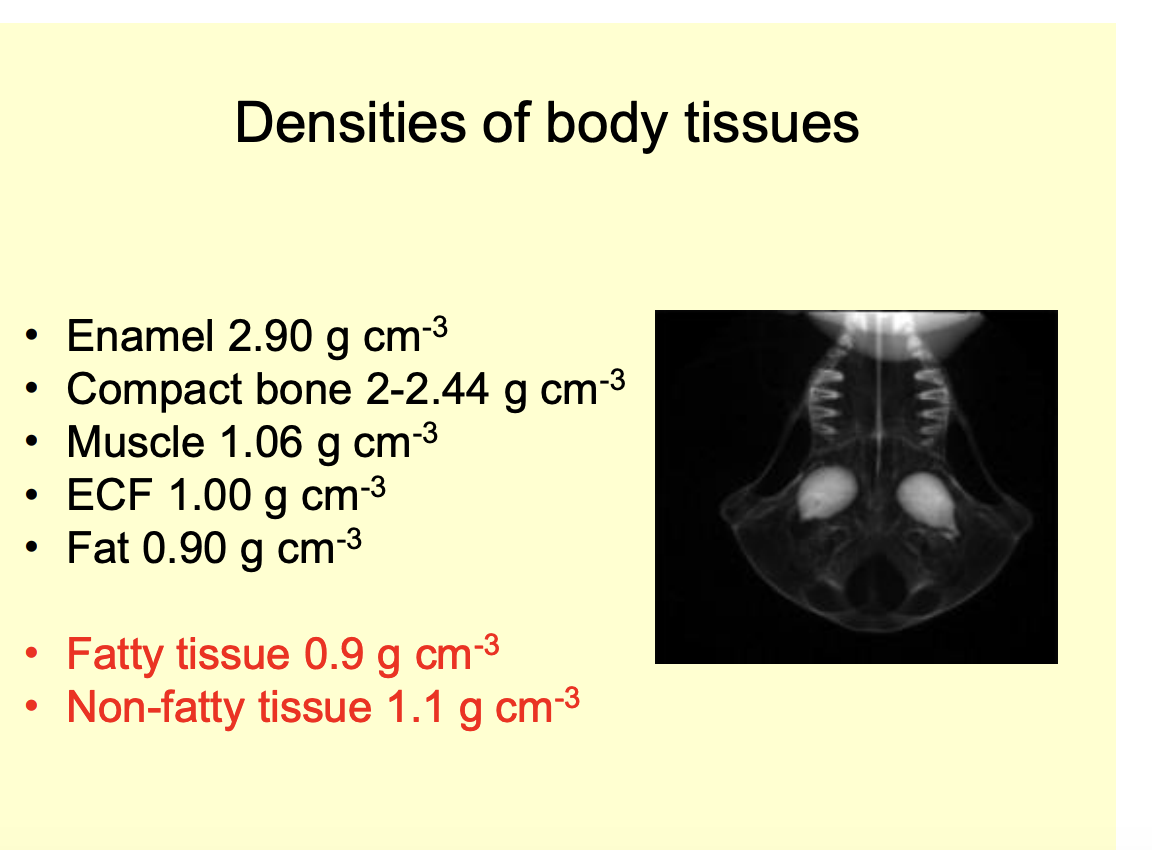
Note that different body tissues have different densities
Fatty tissue: 0.9 gcm-3
non-fatty→ 1.1 gcm-3 (desnser than water)
Weight underwater is equal to normal g force - buyoant force F upwards
F= the weight of water displaced by the body
correction must be made for residual lung volume
must be in 4 degree water (for desnsity of water to be 1 gcm-3) but can just use different density for different temp
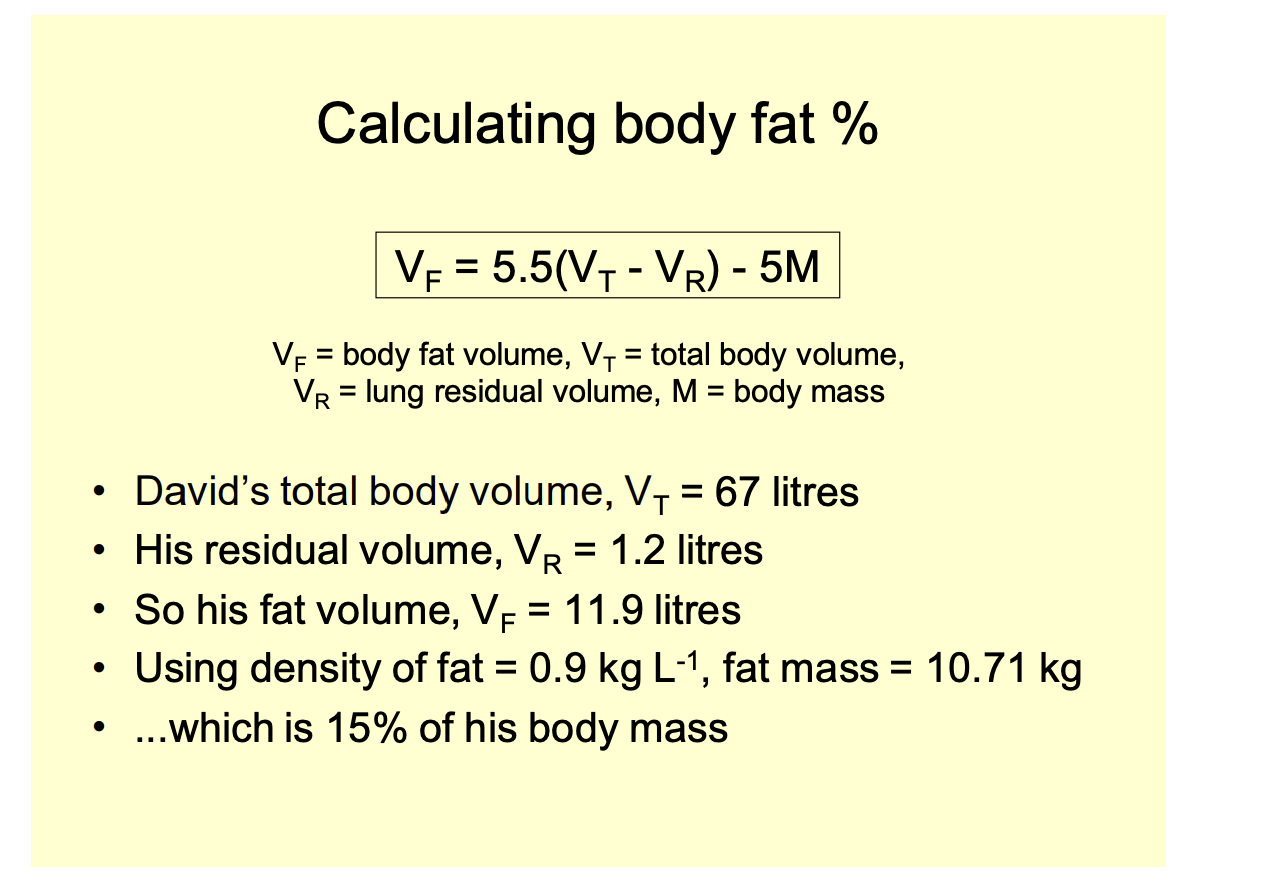
Calculating body fat % from this data

Skin fold thickness
skin fold thickness measured with callipers
at different places
Bioelectrical impedance analysis
Uses V=IR
sends a current through the body
measure the voltage
calculate the resistance
more fat→ high the resistance
Dual energy X-ray Absoprtiometry (DEXA)
Two xrays at different energy
One absorbed through bone
one absorbed through soft tissue
Computer analysis:
puts them together to estimate body composition
note: still less accurate than underwater weighing
Now that we have measured the energy consumption rate and stores, what else if needed to understand what is happening in fasting?
Endrocrine response to fasting
no point in havng the energy stores if they cannot be regulated properly to be used for survival of fasting
Endocrine response to fasting: what is fasting defined as
absence of food intake
strictly from 24 hours after the last meal
What is starvation?
the effects of this on the body
What directly affects metabolic pathways
the relative changes in glucose and FFA availability
This control mechanism being referred to as the RANDLE cycle
These loacl effects are regulated in a whole bdy context by what
Hrormonal Milieu
What hormones affect blood sugar levels
Decrease
Insulin
Increase
Glucagon
Cortisol
growth hormone
Adrenaline (fight-or-flight; exercise)
Why only one hormone to decrease it but many to increase it?
May be more reason/ different types of input needed to increase blood sugar
only need one way to decrease it because it is just about lowering it in the blood????
Which of these are short and long term
Short term→ minute to minute
Insulin
Glucagon
adrenaline
Long term→ adaptive rather than reactive
cortisol
GH
note: adrenline is more for exercise and fight or flight tahn fasting
FDF21 when released
by the liver
during longer-term fasting in humnas
What does FGF21 do
glucagon-like effects in promoting gluconeogenesis from proteins
ketogenesis by the liver
promote resistance to the growth-driving effects of growth hormone
What is glucagon
29 amino acid peptide
Where is glucagon released
alpha cells of Islets of Langerhans
Helps to maintain blood sugar levels between meals

What is glucagon release stimualted and augmented by
Stimulation
lower glucose: hypoglycaemia
lower insulin
Agumentated
ANS
high Amino acids
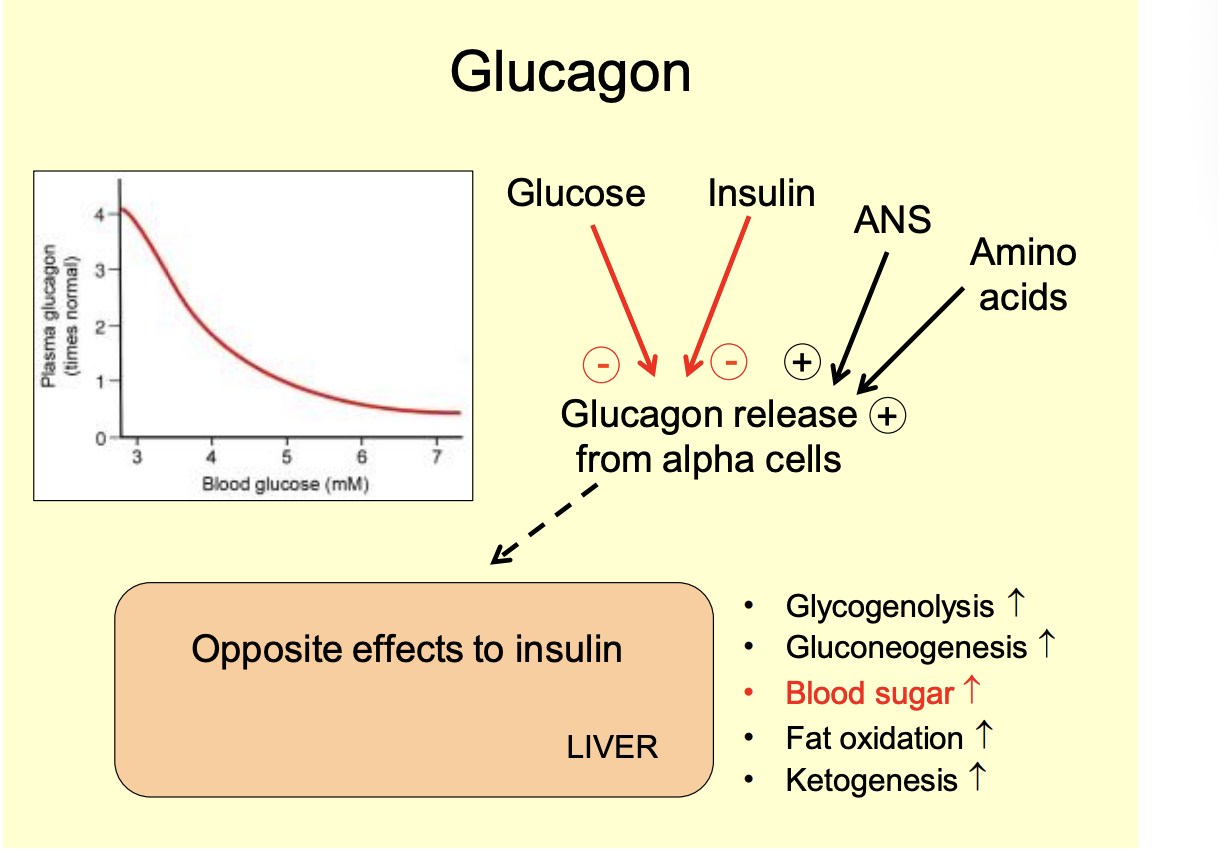
Effects of glucagon
Opposite effects to insulin
Glycogenolysis increases
Gluconeogenesis increase
blood sugar increase
Fat oxidation increase
Keogenesis increase

How does it do this effect
binds to plasma membrane recetpor
stimulates glycogenolsysis
amino acid uptake and gluconegogenesis
hepatic glucose output is increased
stimualtes fat oxidation and ketogenesis
Half life of Glucagon
degraded by liver and kidney
has a short half life in the blood→ 3-4 mins
Metabolism following a meal
Postprandial period
Post-absorptive period
Postprandial period
5 hours of a meal
cabrs are oxidised for exergy
RQ approaches 1 (but does not reach it)
Glycogen and fat are syntehsized and stores
amino acids are made into proteins
INSULIN dominates
although note this isn’t really what hormones do
Post absoprtive
Within 24 hours of a meal
Insulin drops
Glucagon levels rise
note the ratio
Glucose for fuel drops
Hepatic output of glucose many initially by 75% from glycogenolysis
25% from gluconeogenesis during the period
proportion arising from glycogen falling as supplies are diminished
Free fatty acids and amino acids are mobilized
What hormone change is most responsible?
Aruged that it is more to do with the drop in sinuslin than the rsie in glucagon
glucagon being more important in extending fasting
Metbaolism during fasting
Phase I
Phase II
Phase III

Phase I: within days of a meal
Lasts for a weak
Plasma glucose levels drop from 5-3mM after about 3 days
Further drops being prevented by enhanced gluconeogeneesisfrom protein (in both liver and kidney)
Glucose uptake by peripheral tissues is inhibited→ sparing it for the brain
Fat metabolism and ketogenesiincrease
Metabolic rate starts to drop (lower T3)
Hormone changes
Glucagon high, insulin low
GH rises;
Cortisol increase only a little
T3 Drops
Fasting phase II (after a week or so)
Can last for weeks or months
Initially high rate of protein usage as gluconeogenic source slows down
note: NOT TO ZERO
gluconeogenesis declines
Metabolism moves further towards the use of fats→ reaching something approaching a stead-state
Liver glucogen levels are low
but small labile pool remaining
Brain account for 70-80% of total glucose use
the rest= RBC
After a few weeks→ brain can derive up to 75% of its energy from ketone bodies
RQ= 0.7
Hormonal controls in phase II
Insuline low
Glucagon return to normal
Growth hormone??
maybe: but levels are difficult to measure because it pulsates throughout the day
different literature suggest it might increase or decrease
FGF21 from the liver
released in fasting
helps move GH into metabolism mode
Phase III
Lasts a few days before death
fat reserves nearly exhausted
protein catabolism must increase to meet glucose demands
RQ risees from 0.7 to around 0.8
Death: when protein levels about ½ of the body’s protein
Hormone control at this stage
Cortisol finally start to rise significantly
What eventually kills you?
last of muscle strength in the respiratory muscles
can still breath
cannot cough
build up of debris in the lungs
infections
pneumonia kills you
Three phases of fasting graph
note:
the protein metabolism never fully levels off in phase II
the phases are not strict phase→ gradually moves from one phase to another

Why should you not flash diet?
yes you may still have more fat to lose but the continual loss of proteins will continue
the body has no way to sense the amount of protein left
so may still have fat but not enough protein
you will die
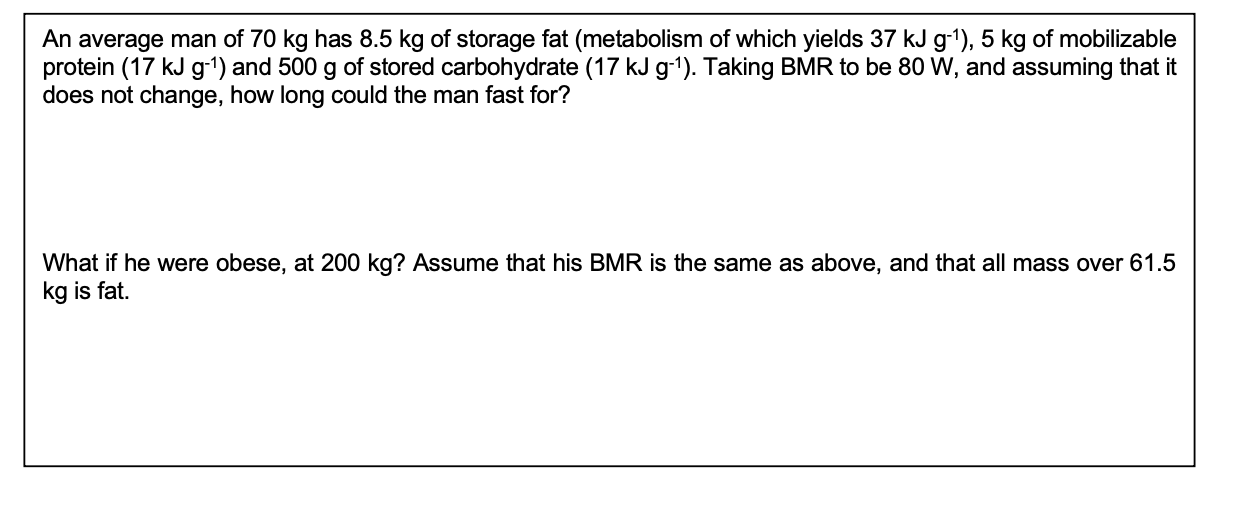
Calculating how long you would last
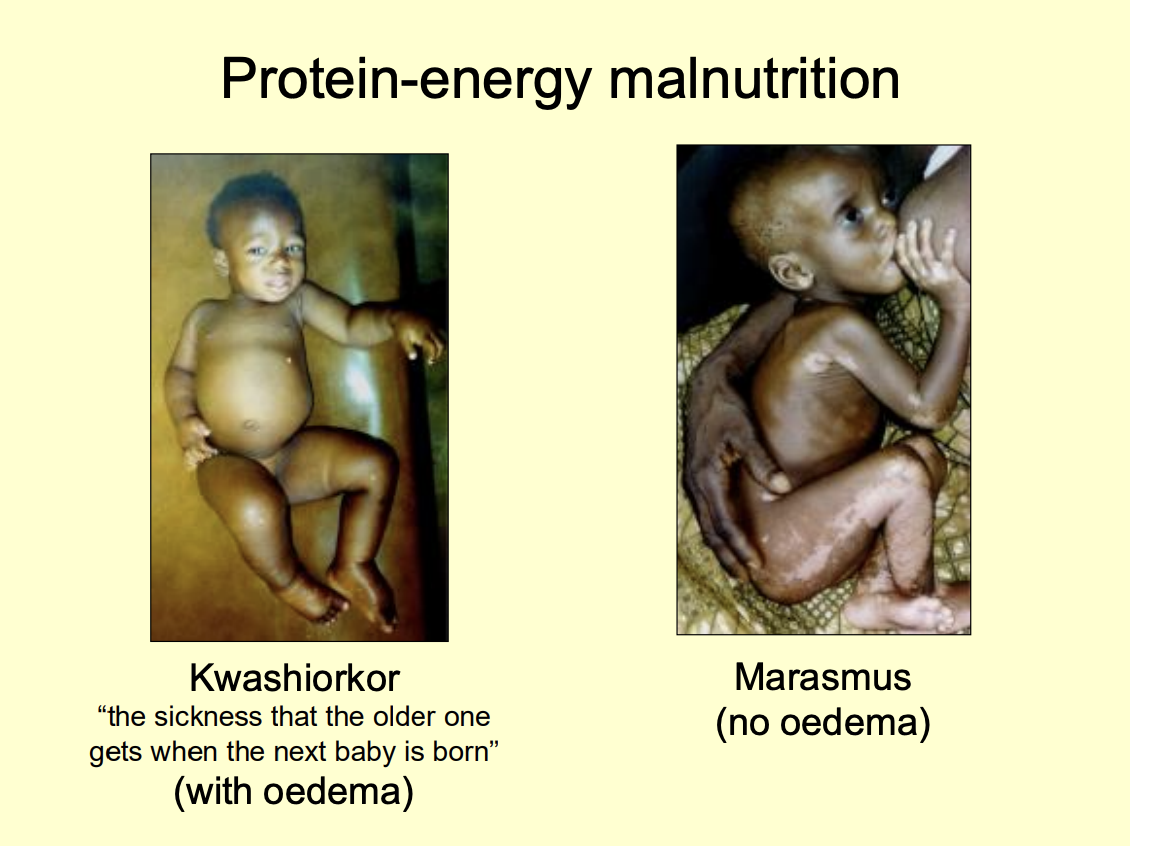
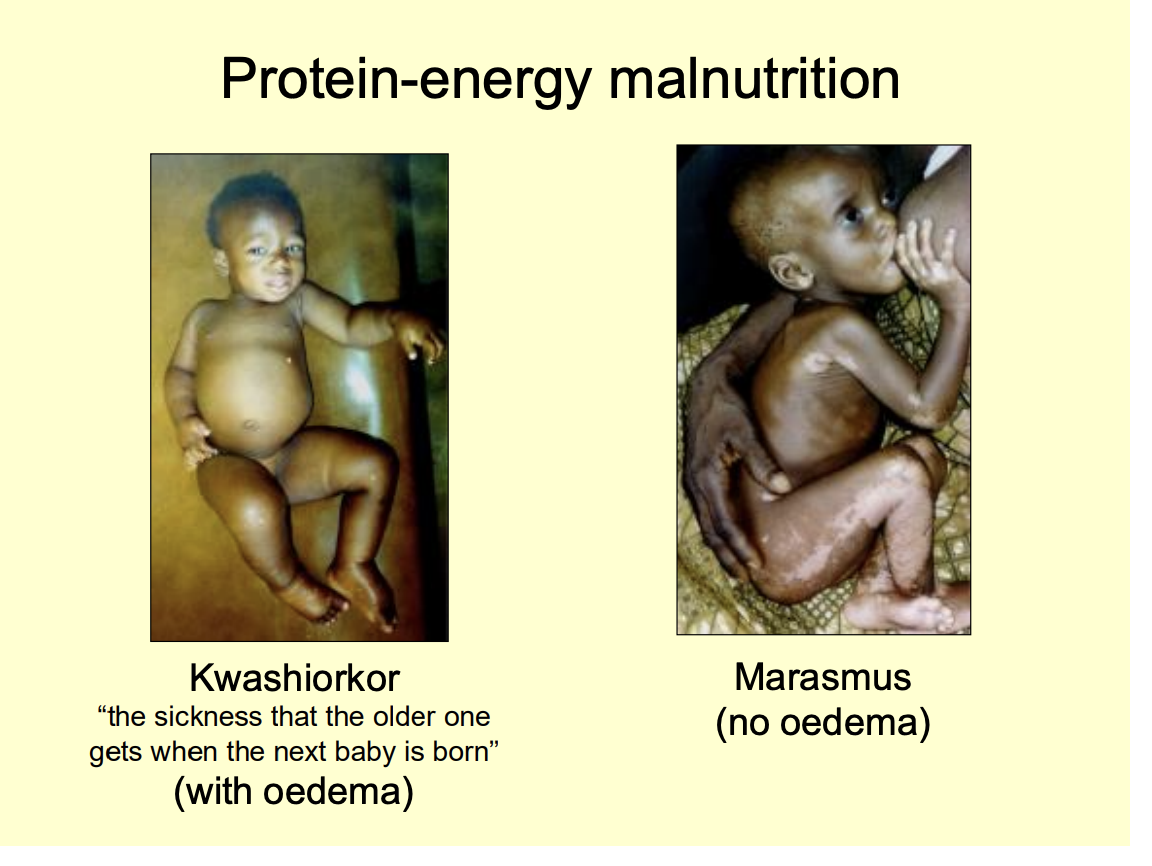
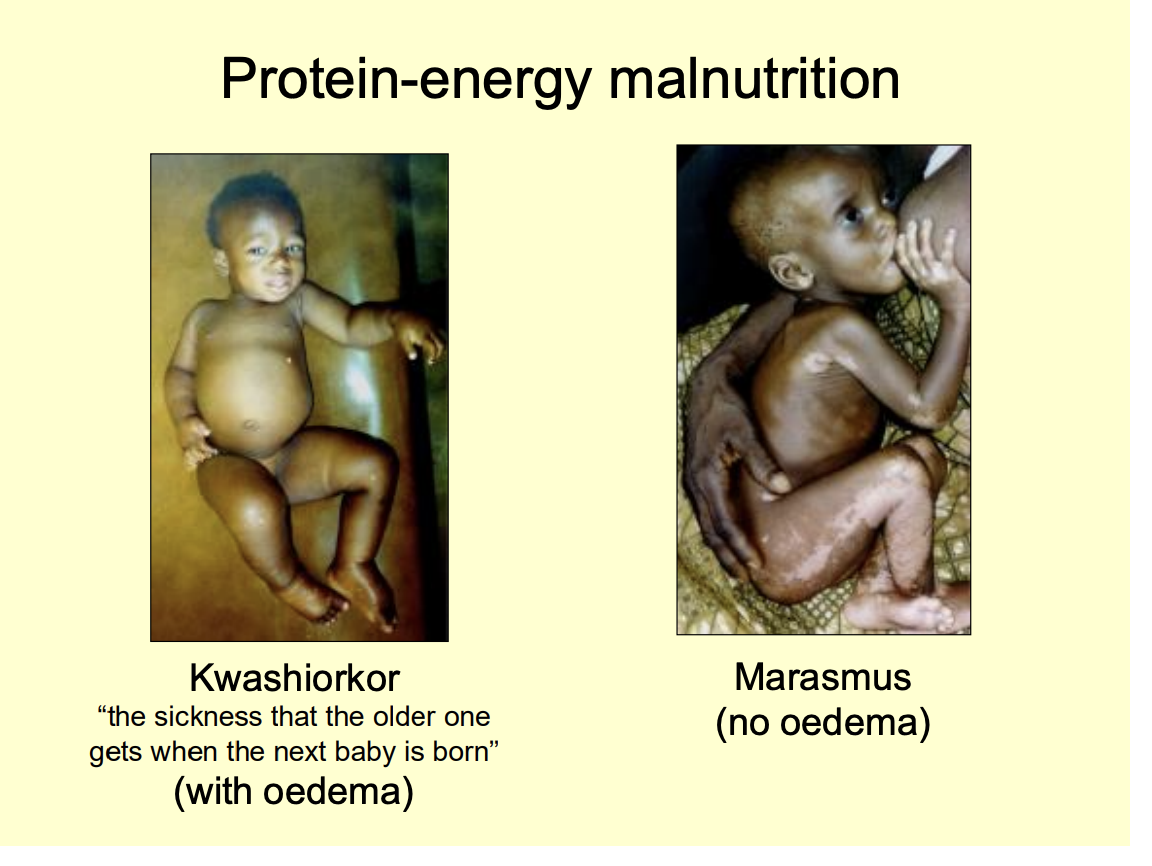
Protein-energy malnutrition: malnutrition contributes to how many deaths a year
3 million child death per year
but very poorly understood
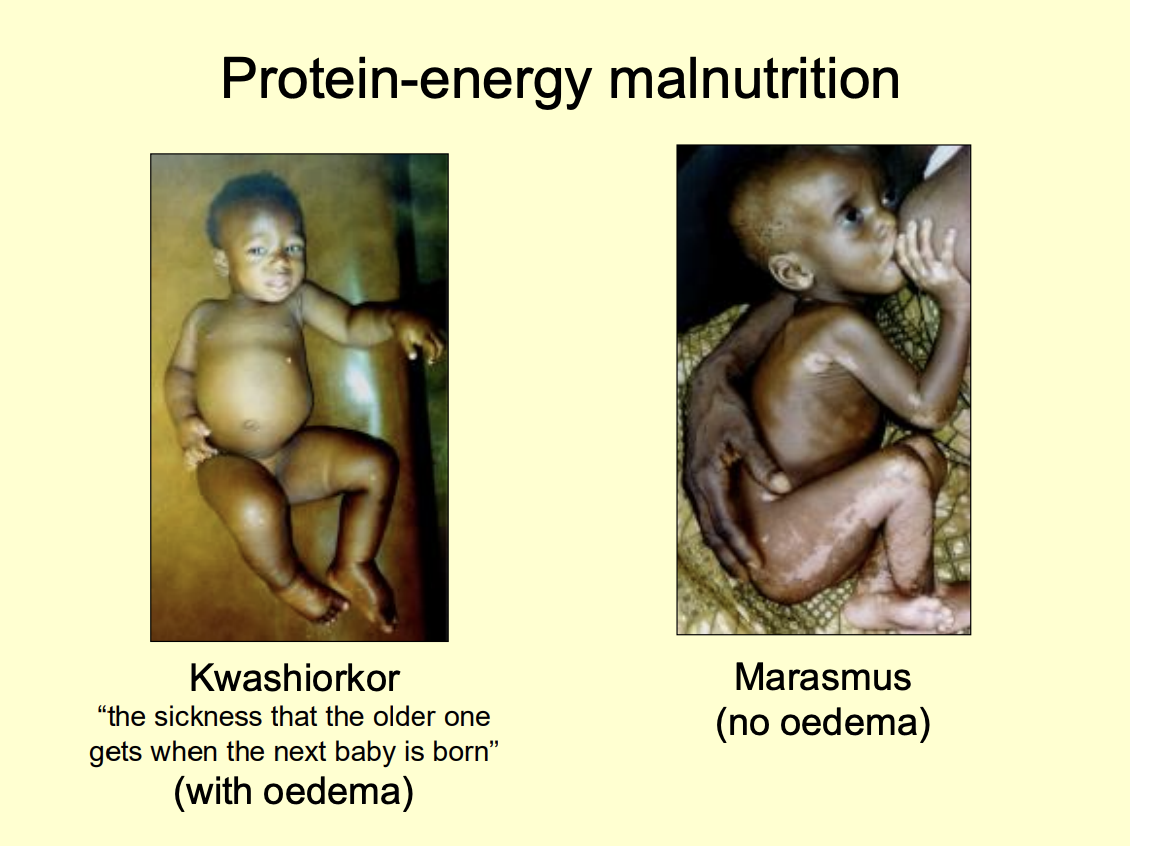
Two examples of protein-energy malnutrition
Kwashiorkor (the sickness that the older one gets when the next baby is born)
After weaning→ from protein rich to low protein diet
peripheral oedma
Marasmus
no oedma
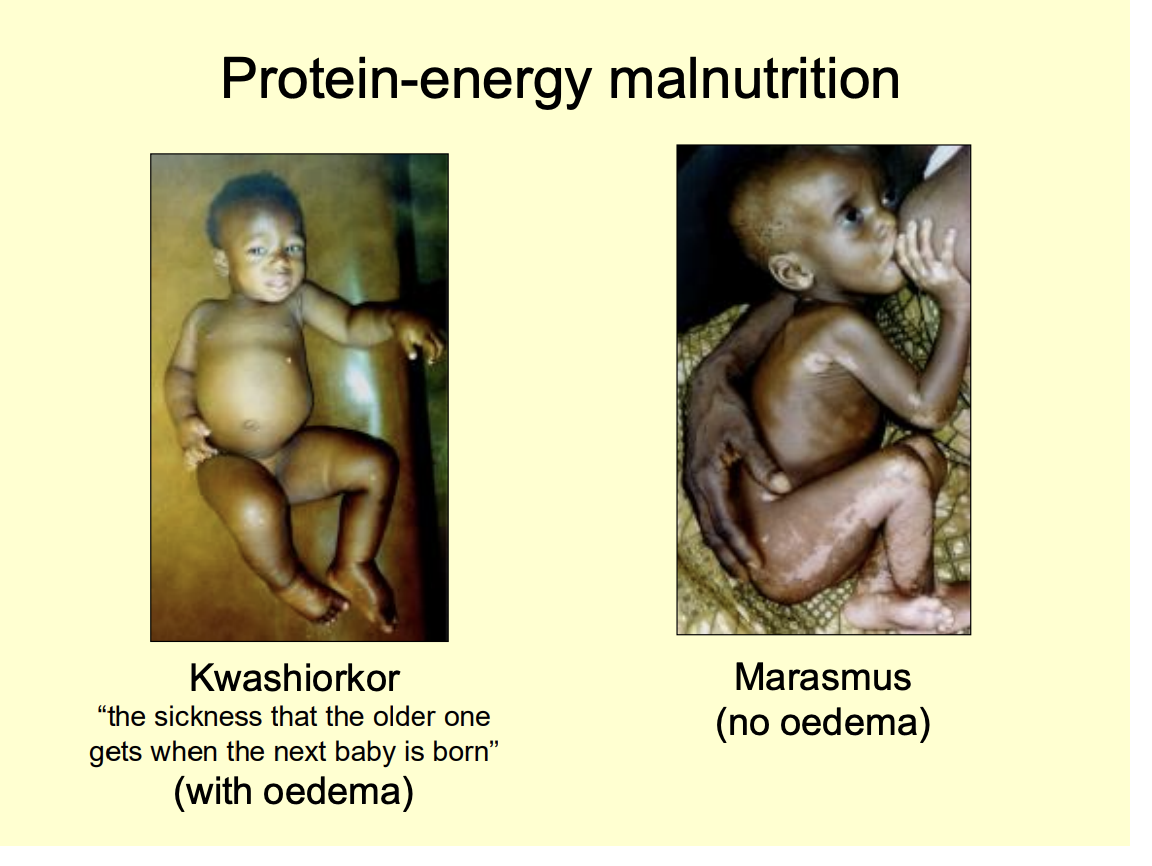
Why does kwashiorkor cause oedema
not getting enough protein
low plasma albumin
low pi c
lots of tissue fluid out
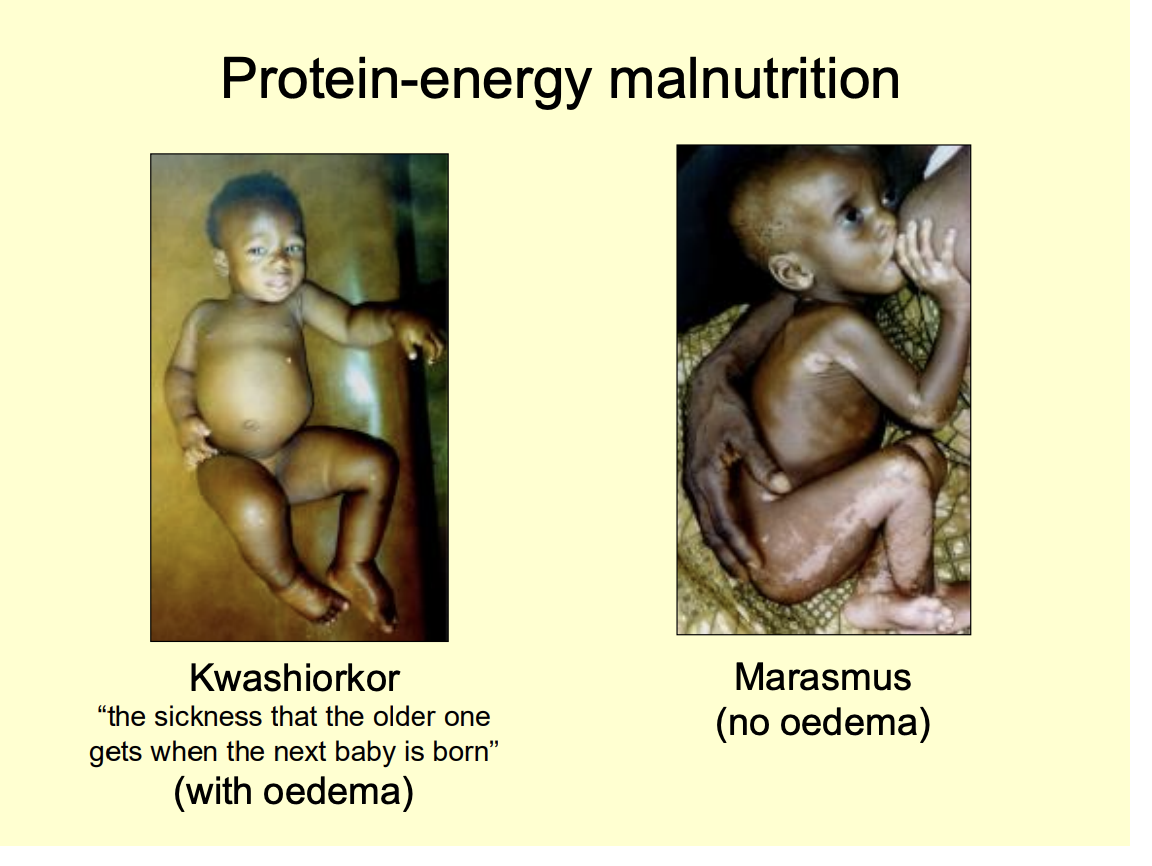
Kwashiorkor characterised by waht
peripheral oedema
hypopigmented
loose hair
flaky paoint dermatitis
Wyh does it happen
Protein deficieny
despire sufficient calorie intake
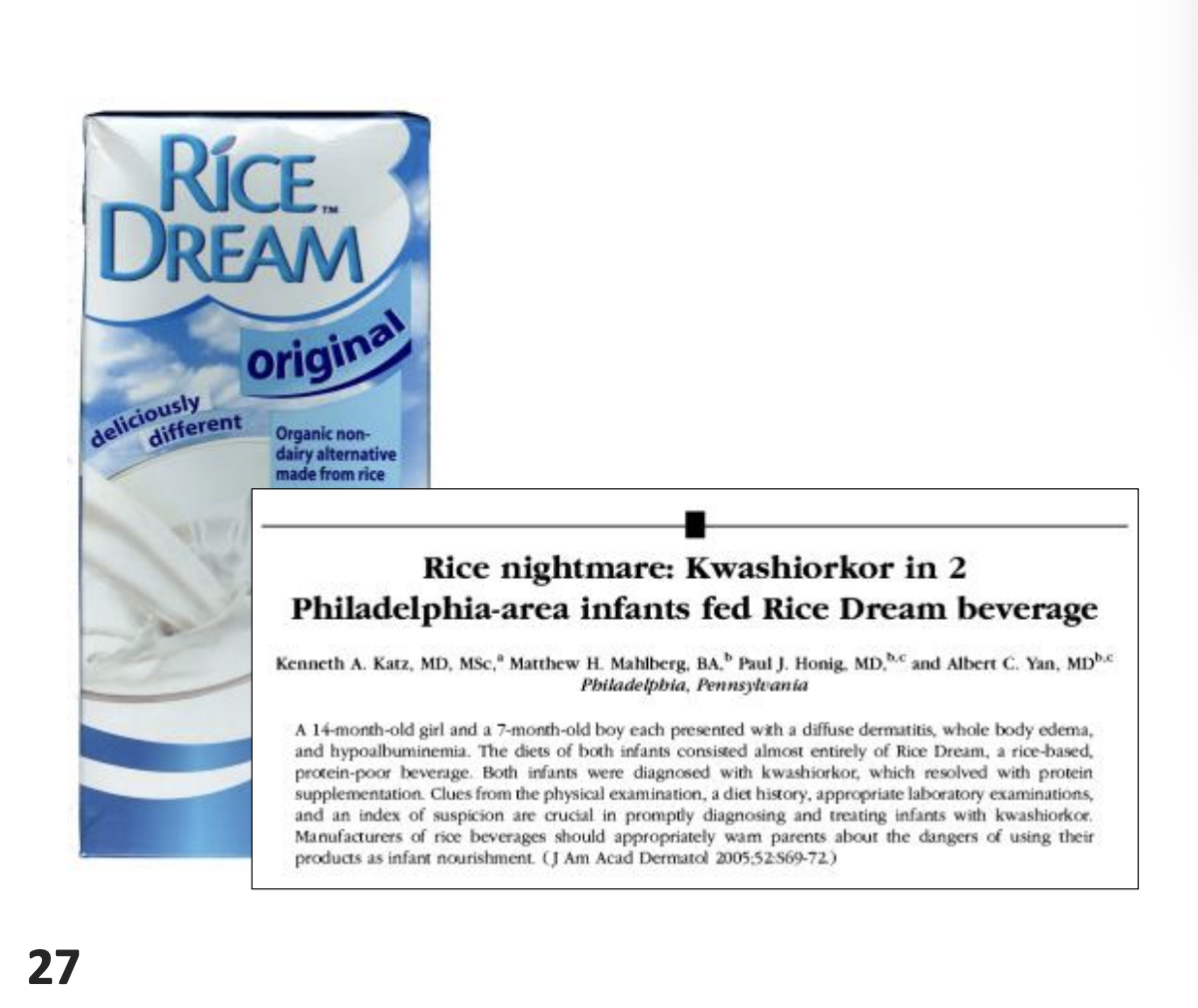
Alternative cause of this disease?
Oxidative stress
imbalance between free radical generation and disposal
perhps as a result of cysteine deficiency?
Evidence of this in the USA
using plant milk for vegan babies
not enough protein
now more reserching going in because of interest in the west
Marasums features
‘wasting away’
less dangerous
due to calorie deficiency alone
Why are these not completely understood?
children on identical diets can develop either of these diseases
v
some studies of why get marasmus in some instead of kwashiorkor
children with natrually lower rate of endogenous protein catabolsim
can be sustained at the same low level even when malnourished
Exams questions
Discuss the endocrine response to fasting.
Discuss why there is only one hypoglycaemic hormone (insulin) but several hyperglycaemic mechanisms.
What methods can be used to assess whether or not you are overweight, and what are the advantages and shortcomings of each method?