ANHB2214 Oral Cavity, Teeth and Gingiva
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
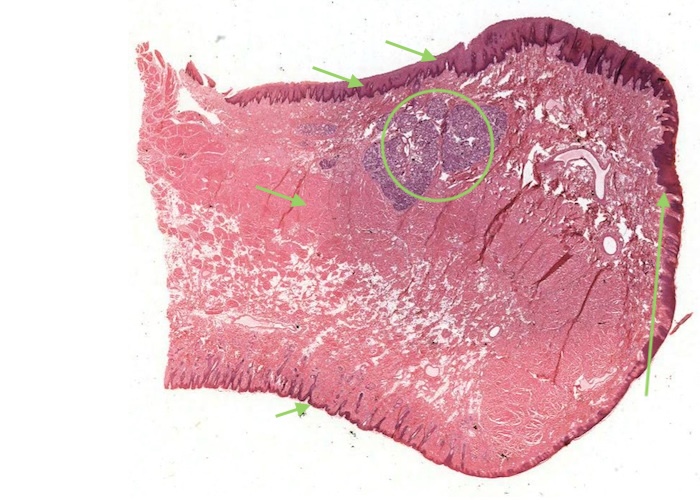
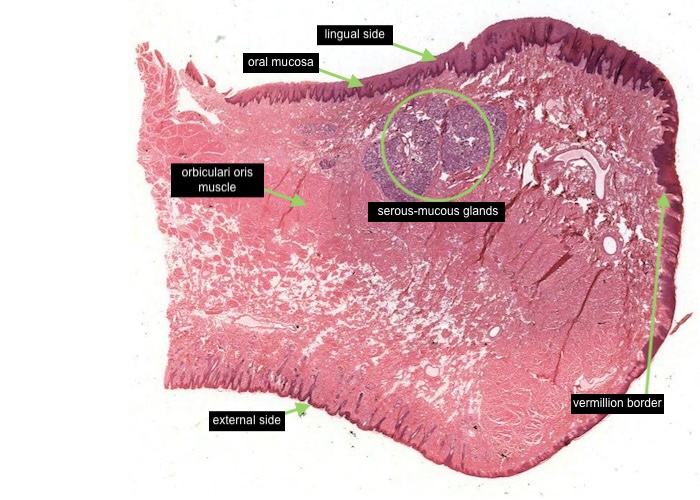
Most of the oral cavity is lined with an "oral mucosa", characterized by non-keratinized stratified squamous epithelium. Mixed serous-mucous glands underlie it in most places. The inside of the lip exemplifies this oral lining.
Figure out how this transverse section of the lip was cut. Distinguish the lingual side (with the thicker epithelial layer) from the external side with a thin epidermal layer and hairs. The upper surface in between is the vermilion border. Note where it is at low magnification because its boundaries with the skin and oral mucosa are somewhat gradual.
The centre of the lip is composed of the orbicularis oris muscle cut in cross section.
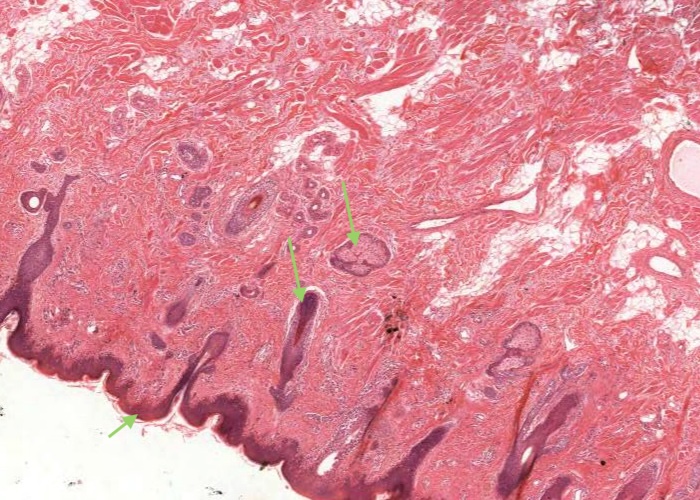
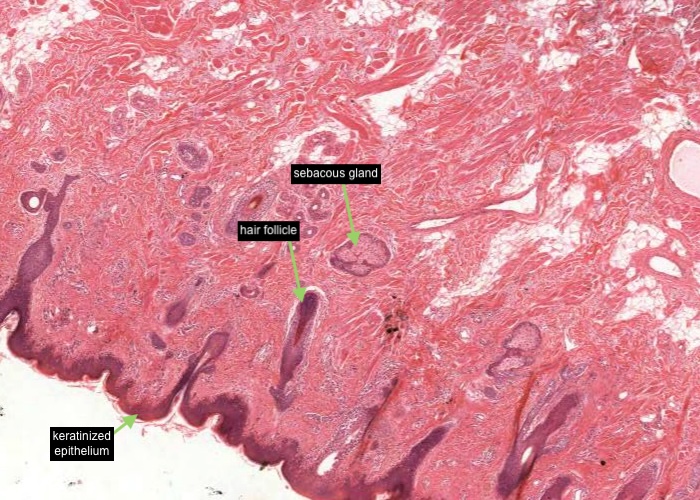
Under low magnification examine the external cutaneous part. Identify a hair follicle, sebaceous gland and keratinized epithelium. Follow the transition of the well keratinized epithelium into the vermilion area of the lip.
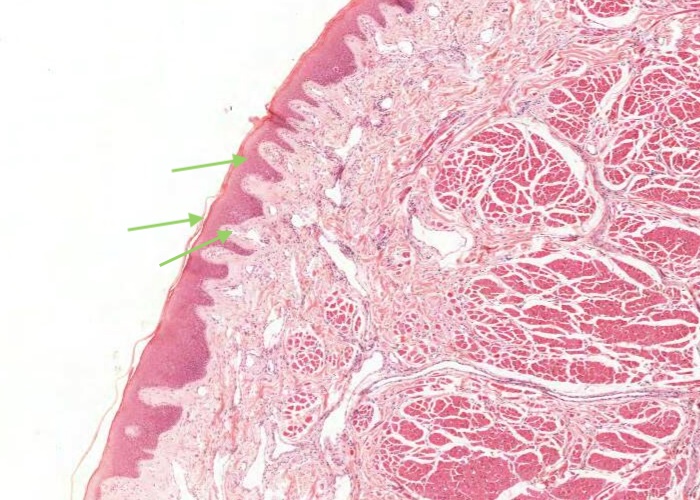

Follow the transition of the well keratinized epithelium into the vermilion area of the lip. The mucosa here has no hair follicles or glands. The dermal papillae are long and extend far up in the epithelium. They contain a particularly large number of blood vessels which impart the red color to the lips. The thinness of epithelium over them maximizes their effect. Observe that the epithelium over the vermilion border is very lightly keratinized.


Most of the oral cavity is lined with an "oral mucosa", characterized by non-keratinized stratified squamous epithelium. Mixed serous-mucous glands underlie it in most places. The inside of the lip exemplifies this oral lining.
Note the generalization that stratified squamous epithelium usually is substantially thicker when it is not keratinized than when it has a dense protective layer of keratin on its surface. This is obvious even without magnification.
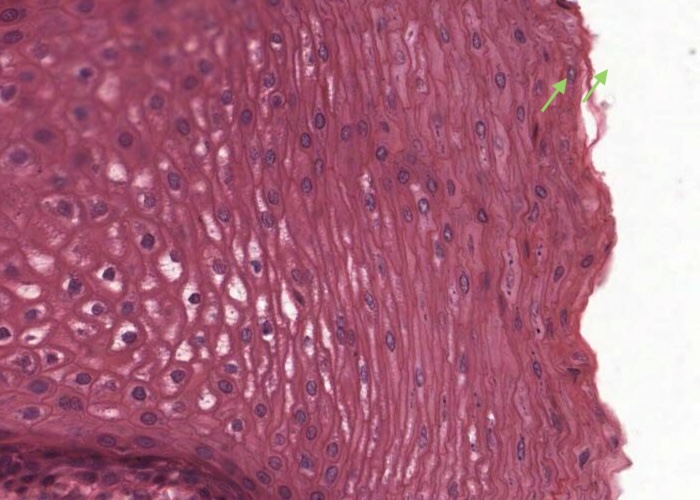
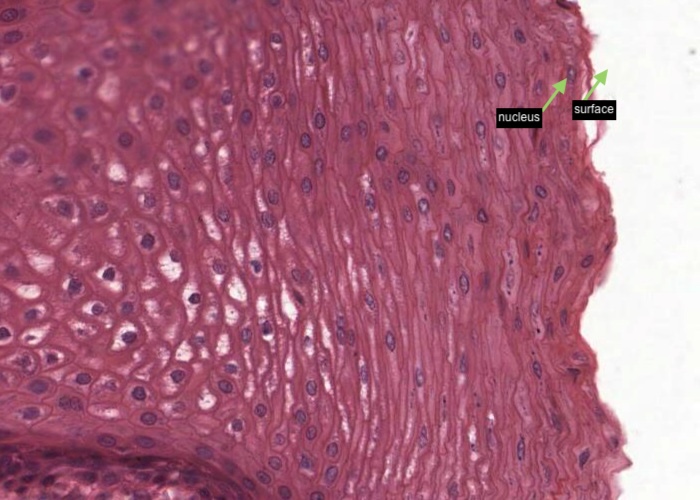
On the oral surface, a nucleus (albeit many are "pyknotic") can be seen in the each cell all the way to the surface. This is typical of areas where the epithelium may be parakeratinized.
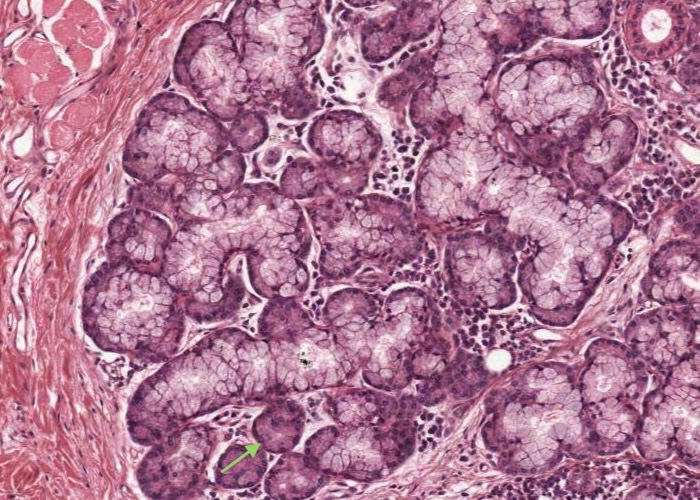
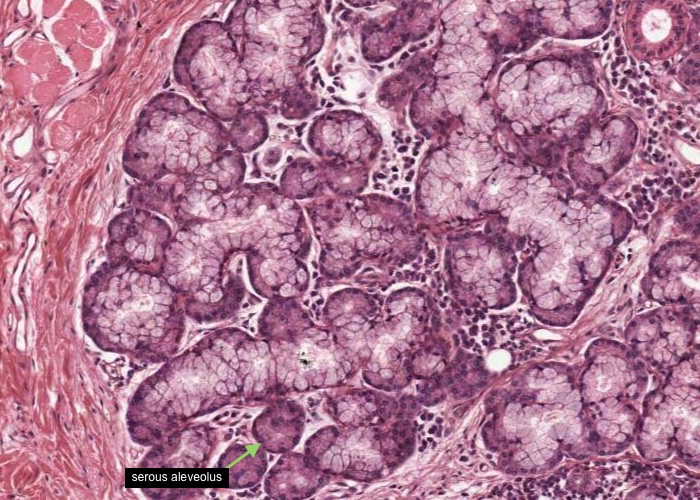
Find the labial glands in the lamina propria ("labial" refers to the lip). They are mixed serous and mucous, but the ones caught here are predominantly the latter. Hunt around for the odd serous alveolus here and there in the glands.
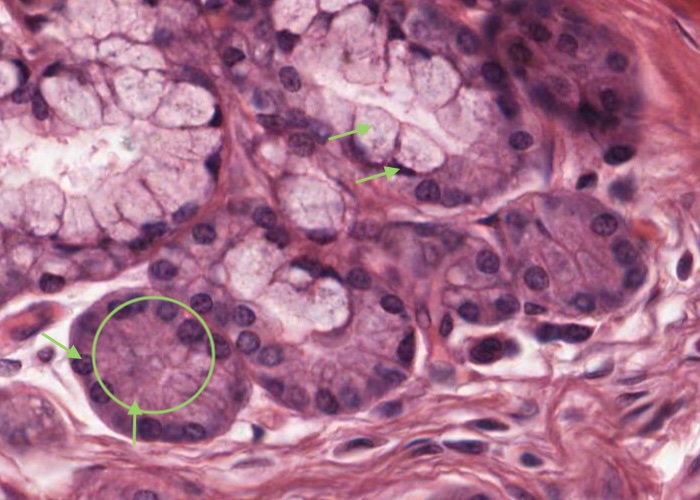
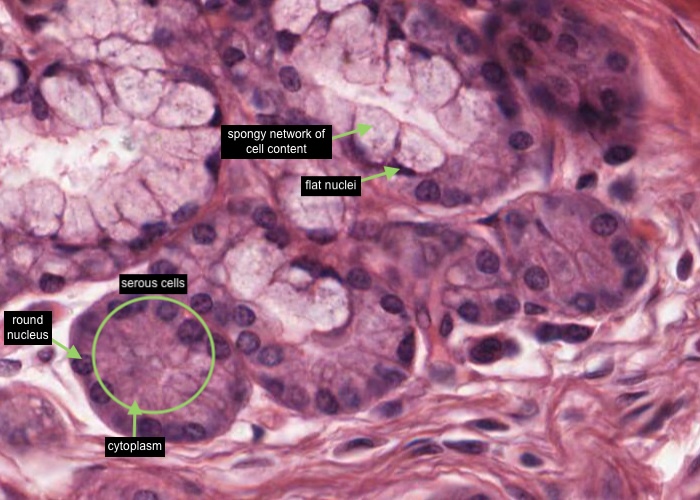
The serous cells are pyramidal, with a round nucleus in the basal part of the cell where the cytoplasm stains darker due to stores of ribosomes. Their apical cytoplasm is pink in H&E and contains zymogen granules, precursors of salivary amylase. Cell boundaries are indistinct. The mucous cells appear pale blue with the nuclei scrunched flat against the base of the cells. They produce a viscid fluid consisting mainly of mucin. This material is usually extracted during tissue preparation, leaving only a spongy network of cell content.

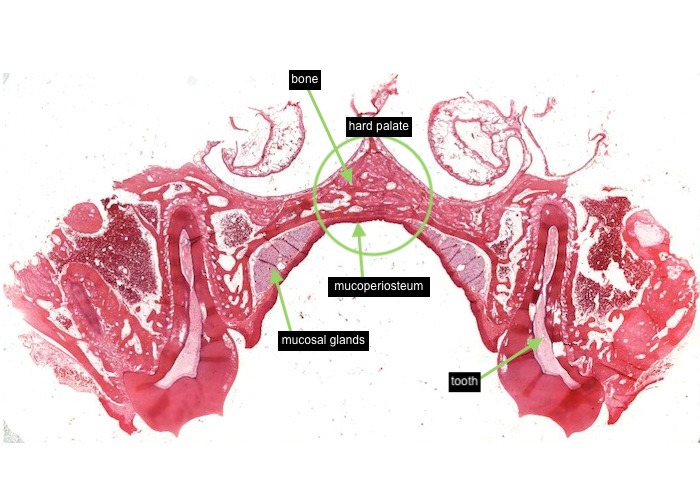
This image of the section you can view (see link below) shows the hard palate with a tooth on either side. Bone underlies this part of the roof of the mouth.
The mucosa of the hard palate has two structural distinctions. Firstly, the mucosa is firmly fused with the periosteum along the midline, forming a so-called mucoperiosteum. Second, the epithelium is keratinized, due to continual rubbing against the keratinized tongue. In areas that receive abrasion the epithelium is keratinized and called "masticatory mucosa. This is the case for the gingiva around each tooth and the hard palate. Anywhere else, the epithelium may become converted to a keratinized form if stressed, for example by a dental prosthesis.
The soft palate is unkeratinized. You can feel the difference in texture between it and the keratinized hard palate if your tongue is nimble enough to reach the back of your oral cavity. The hard palate has a series of left to right ridges that you can easily feel with your tongue. They keep the tongue from slipping and sliding when you talk, chew or when you sucked on a nipple as a baby. Finally, the palate has extensive mucosal glands located laterally.
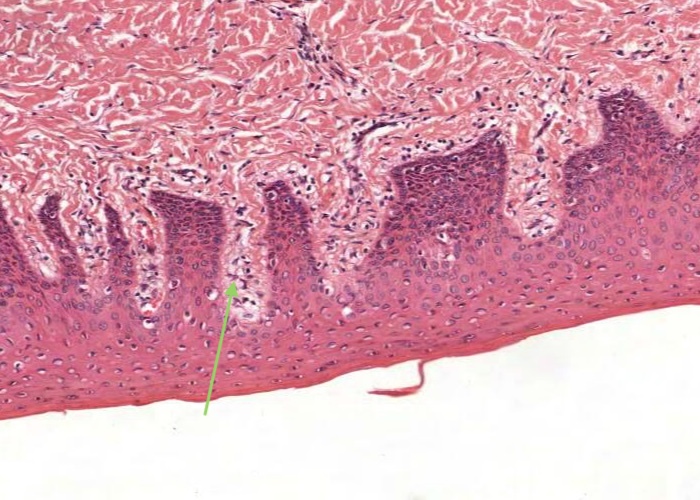
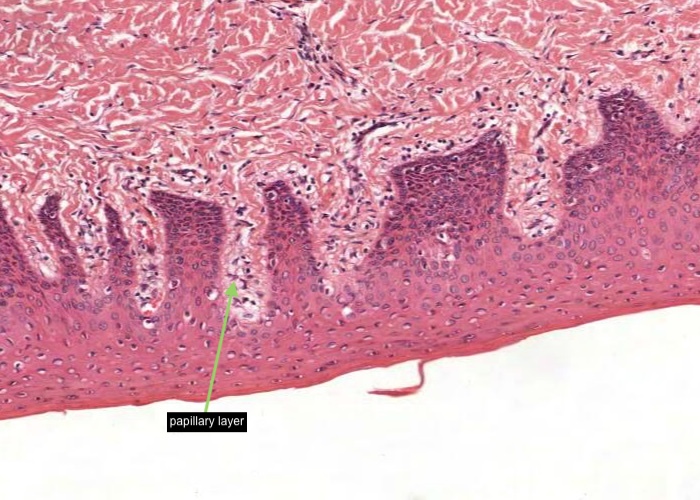
Masticatory mucosa is similar to that of skin but lacks a stratum lucidum. There is a papillary layer of lamina propria which is loose connective tissue but deeper the connective tissue becomes more dense and binds the mucosa firmly to underlying structures and so prevents a lot of mobility of the masticatory mucosa.
MAJOR SALIVARY GLANDS:
All the major salivary glands have ducts that deliver salivary secretions into the oral cavity. Minor salivary glands are located in the submucosa of the oral cavity in specific locations.
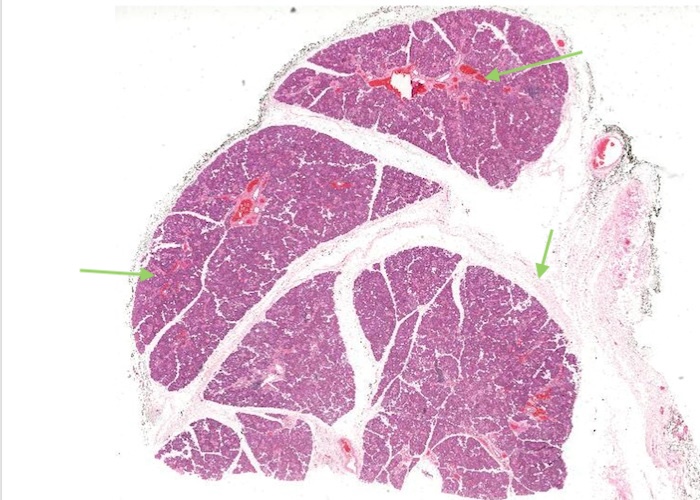
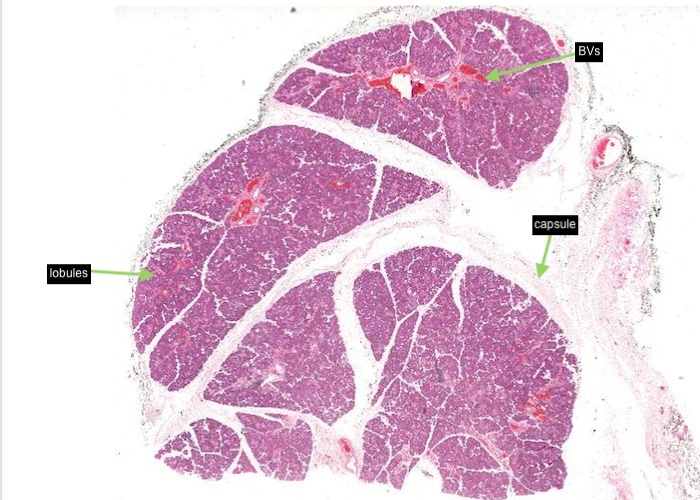
Each gland has a capsule of dense connective tissue with septa, carrying blood vessels and the excretory ducts, penetrating the parenchyma and dividing it into a lobe and lobules.
MAJOR SALIVARY GLANDS - Parotid Gland:
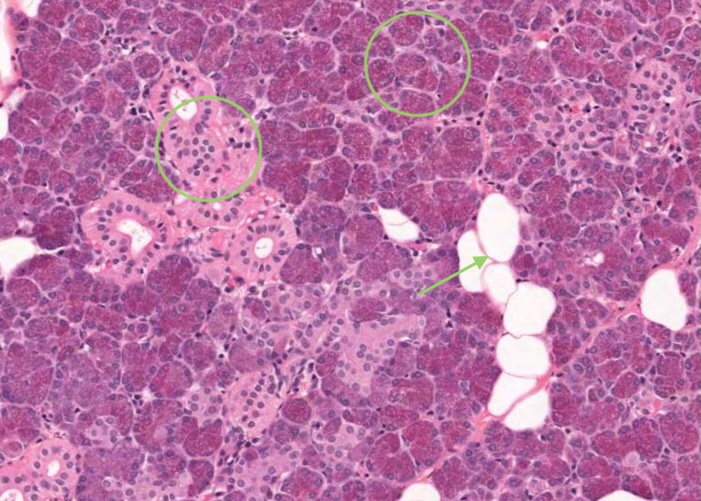
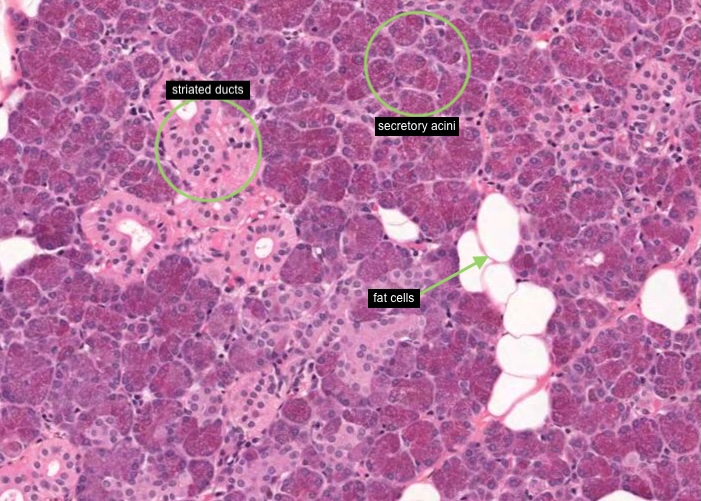
The parotid is a branched acinar (actually tubulo-acinar) all-serous gland. Under low magnification its lobular divisions are clearly visible and within the lobules the secretory acini are easily distinguished from the striated ducts. The many round open spaces are scattered fat cells. Fat cells happen to be characteristic of the parotid gland. Do not mistake them for mucous acini in this purely serous gland.
MAJOR SALIVARY GLANDS - Parotid Gland - serous acinus:
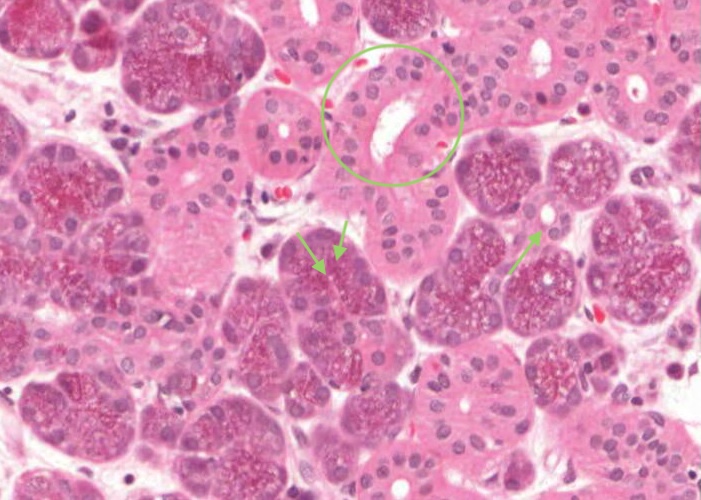
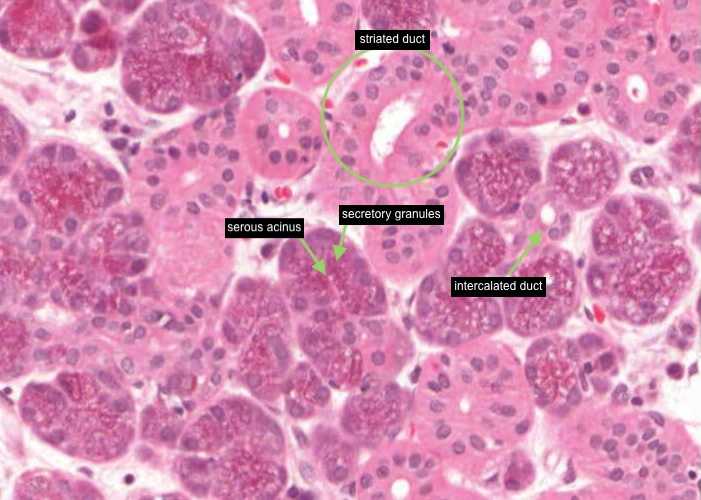
Examine the serous acinus under high magnification. They have round, basally located nuclei and basophilic cytoplasm, as you have come to expect for serous-secreting cells. The apical half of the cell is filled with secretory granules. These should be acidophilic as they contain secretory proteins but the granules have been dissolved out in many places leaving just a foamy cytoplasm. This is not unusual for routine histology. Look around for acini which retain their secretory granules. Note an example of a striated duct and look carefully for an intercalated duct.
MAJOR SALIVARY GLAND - Submandibular:
Scan this compound, branched tubuloacinar mixed gland at low magnification. It has a substantial proportion of both mucous and serous acini.
The submandibular gland has both striated and intercalated ducts. Most of the intralobular duct system is made up of the striated variety. Short segments of intercalated ducts run into striated ducts. This is readily apparent on your section. Thus, the large number of obvious ducts in sections is one way to distinguish the submandibular gland from the other compound glands of the body.
The interlobular ducts are very nicely preserved here and I have enjoyed looking at their epithelia, seeing some cases of the elusive stratified columnar variety and even epithelia that cannot decide whether to be simple or stratified. I hope that you also have the joy of finding this interesting.
MAJOR SALIVARY GLAND - Submandibular - mixed acinus:
The mucous-secreting cells are palely stained, with nuclei flattened against the cell bases. They are closely related to the goblet cell. The serous-secreting cells stain vigorously with hematoxylin. Their basophilia suggests vast quantities of ribosomes and, indeed, this cell type makes enzymes for export in a watery secretion. Note that small groups of serous cells often cap the end of mucous acini. These half-moon-like figures are called serous demilunes.
MAJOR SALIVARY GLAND - Sublingual:
Scan this example of a compound, branched tubuloacinar gland. Note that the sublingual gland is predominantly mucous.
You see mainly large light blue mucous acini with only the occasional darker staining serous demilune. Again, find interlobular ducts surrounded by a large amount of connective tissue that ramifies to surround and define the lobules.
You may need to look carefully to find an intralobular duct in this gland. One reason is that the secretory units are very elongate and so fewer ducts are needed. The ducts that are present are mainly excretory, that is, they are just passive pipes for conducting secretions. They are undistinguished looking and surrounded by a fair amount of connective tissue.
You may come across an occasional striated duct if you are lucky. An intercalated duct are rare in this organ so please don't worry if you can't find one!
MAJOR SALIVARY GLAND - Sublingual - tubular secretory unit:
There are not many intralobular ducts in this gland. One reason is that the secretory units are very elongate and so fewer ducts are needed.
MAJOR SALIVARY GLAND - Salivary gland ducts:
Salivary gland ducts consist of large excretory ducts (interlobular), intralobular ducts (striated) and intercalated ducts (not visible at the magnification of this image).
MAJOR SALIVARY GLAND - Salivary gland ducts -intercalated duct:
To find them, slowly scan around the lobule, looking between acini for a circle of 3-5 elongated low cuboidal cells. An intercalated duct is smaller than the surrounding alveolus or acinus. They are more obvious associated with serous secreting acini so in the sublingual gland they are very short and so rather difficult to see.
MAJOR SALIVARY GLAND - Salivary gland ducts - striated duct:
Move to the purple-staining parenchyma within a lobule. Scan around for cross-sections of acidophilic intralobular ducts lined with a simple cuboidal/columnar epithelium. They may have some small amounts of associated connective tissue supporting them. Note the eosinophilic cells which line them. Their staining characteristic comes from their large numbers of mitochondria (for pumping ions into and out of their lumen) and also basal infoldings of the cell membrane.
They are called both "striated ducts" and "secretory" ducts. These ducts have the important physiological function of regulating the ion content of the saliva. They are not just passive pipes to the surface, as the excretory ducts are. Striated ducts are connected to the purple-staining secretory acini by much smaller intercalated ducts.
MAJOR SALIVARY GLAND - Salivary gland ducts - interlobular duct:
Scan this section at low magnification. Note how the connective tissue divides the gland into lobules of various sizes. You may see a medium-sized blood vessel in this connective tissue. Find a cross-section of an interlobular duct. This is an excretory type of duct, whose function is simply to carry away the secretion to the oral cavity. The duct will be surrounded by interlobular connective tissue and lined by an epithelium that can be simple columnar, pseudostratified, or stratified columnar depending on the size of the duct. Unfortunately, the epithelium in these large ducts is sometimes too poorly preserved to warrant lots of study.
TONGUE:
This is a nice section of tongue to begin with. It is a transection through the tongue of a rabbit and has been stained with Masson stain. The organ is mainly skeletal muscle surrounded by a stratified squamous mucosa.
Observe the very orderly arrangement of the muscle fibers in three perpendicular directions. This is what makes the tongue so wonderfully dexterous. The Masson stain makes it easy to distinguish the epithelium from the lamina propria. The epithelium lining the ventral surface is unkeratinized. The dorsum is keratinized but formed into special lingual papillae. Do not bother to examine these structures here. They are poorly developed on the soft tongue of a rabbit and better observed in other sections. Anyone who has been licked by a bunny knows how soft its tongue is. To see the various types of lingual papillae go to the following items and histological sections.
TONGUE: - lingual muscles:
Observe the very orderly arrangement of the muscle fibers in three perpendicular directions - fibres are sectioned transversely, longitudinally and obliquely.
These muscles can be "extrinsic" (if they have one attachment to a structure distant to the tongue) or "intrinsic" (if they remain within the tongue).
TONGUE: - lingual muscles - skeletal muscles
Note the skeletal muscle fibres cut transversely with a peripheral nucleus visible and also cut longitudinally showing the striations. The green/blue stained tissue is the perimysium (collagen fibres) surrounding numbers of skeletal muscle fibres forming a bundle or fascicle.
TONGUE - dorsal surface:
The dorsum is keratinized but formed into special lingual papillae. Do not bother to examine these structures here. They are poorly developed on the soft tongue of a rabbit and better observed in other sections.
TONGUE - dorsal surface - filiform papillae:
Filiform papillae are the most numerous type of papillae. To observe them, find areas in which the plane of section is completely perpendicular to the surface of the tongue. Oblique sectioning will give complex artifactual patterns to these structures in the same way that oblique sectioning can make a simple epithelium look stratified.
Observe that papillae are mucosal structures with a core of lamina propria surrounded by epithelium. You should be able to tell that they are highly keratinized structures with "barbs" of keratin which they require to serve their mechanical role.
TONGUE - dorsal surface - fungiform papillae:
These structures are big enough (~ 0.5 mm) to see with your naked eye. Indeed, you can easily see them on your partner's tongue as tiny red spots. They are more numerous near the tip of the tongue. They contain taste buds, although you may not see any if the section skipped them (as is the case in this image). Instead of being pointed each fungiform papilla is rounded, resembling, perhaps, an unopened mushroom.
TONGUE - dorsal surface - circumvallate papillae:
Circumvallate papillae are worth spending a little extra time on. Nine to twelve of them are arranged in a V-shape pointing posteriorly. They are shaped like fungiform papillae, but are much larger (2-3 mm) and surrounded by a trench. First, locate them on your friend's tongue, or your own with a mirror. Then, examine the example on the histological section provided here.
At higher magnification, observe the trench around this papilla, the serous glands (of von Ebner) underneath (see next item), and the taste buds in the walls.
TONGUE - dorsal surface - taste bud:
Search around for a favorable section showing that the taste bud extends the entire thickness of the epithelium. You may be able to see the taste pore on a taste bud and at least imagine the taste "hairs" or microvilli protruding from it.
The taste bud is made up of neuroepithelial (snsory) cells, supporting cells and basal cells.
TONGUE - dorsal surface - lingual salivary (von Ebner’s) glands)
At higher magnification observe the trench around this circumvallate papilla, the serous glands (of von Ebner) underneath, and the taste buds in the walls. The glands empty into the trench via a duct to keep the taste buds washed.
TONGUE - dorsal surface - parasympathetic ganglion
It is not always possible to locate a parasympathetic ganglion in many sections of organs but you can find one in this section. Ganglion cells are often seen in sections of the tongue. They are postsynaptic neurons and will innervate the minor salivary glands in the tongue.
TOOTH (ground section)
This image has been rotated 90 degrees to fit in the anatomical details. Observe the main anatomical landmarks of the tooth. The crown is that part which is exposed above the gums (gingiva). The root of each tooth (there may be more than one) extend into the alveolarsocket. This is the hole in the alveolar bone of the jaw that the root of the tooth fits into. The root is attached to the surrounding alveolar bone by a periodontal ligament.
Most of the substance of the tooth is dentin. This tissue is covered by a layer of enamel over the crown, and a thin layer of cementum over the root. The dentinoenamel junction, (DEJ) where the dentin contacts the enamel is an important landmark in the development, structure and pathology of the tooth. The enamel on the outside of the DEJ usually looks yellowish or brownish. The dentin looks white or gray with fine black stria in some places. The interface of the cementum with dentin is of lesser significance. The enamel meets the cementum at the neck of the tooth.
The pulp chamber occupies the center of the tooth, surrounded by dentin. It is filled with an uncalcified cellular, loose, connective tissue. This dental pulp extends down through the root canal to the apical foramen at the tip of the root. Blood vessels and nerves pass up through this foramen to supply the pulp.
TOOTH (ground section) - enamel rods:
The enamel is seen to consist of vast numbers of mineral "rods" or "prisms." At some places, air has been trapped between individual rods, outlining them with very fine black lines. Where the mounting medium has fully penetrated the substance of the enamel, the rods may be less evident. A rod can extend all the way from the dentino-enamel junction to the surface of the enamel. In some places, rods run parallel to one another (such as along the side of the crown). In other areas of "gnarled enamel", they are interwoven to form an especially hard tissue.
TOOTH (ground section) - gnarled enamel:
In some places, rods run parallel to one another (such as along the side of the crown). In other areas of "gnarled enamel", they are interwoven to form an especially hard tissue.
TOOTH (ground section) - lines of Retzius:
You can see two types of incremental lines in the enamel. Lines of Retzius look brownish and are more evident at low magnification.
TOOTH (ground section) - Circadian (daily) increments:
Looking very carefully at the higher power you can see circadian (daily) increments (they look like striations) along individual prisms. They are about as long as a prism is wide.
TOOTH (ground section) - Dentinal tubules:
The main visible structures within dentin are the dentinal tubules. In life they contain very thin processes of odontoblasts. Here of course, this soft tissue is gone and the tubules are hollow. Where they are filled with air they appear black and are totally obvious, extending from the DEJ to the surface of the pulp chamber in a smooth S shaped curve. Close to the DEJ the tubules and the odontoblastic processes branch as well.
TOOTH (ground section) - Contour lines of Owen:
Dentin grows only by apposition which, once again, leaves behind tell-tale incremental "growth lines" (contour lines of Owen). These are less apparent than the incremental lines in the enamel but may be visible in ground sections when the specimen is oriented and illuminated correctly. In this image they appear as shadowy lines running perpendicular to the dentinal tubules.
TOOTH (ground section) - Cementum:
A layer of cementum covers the exterior surface of the dentin in the root, in place of enamel in the crown. In many respects cementum is a form of bone. The first cementum that is laid down on a root is called primary cementum and is acellular. It is only one or two micrometers thick and, as its name implies is without cells or cell processes in it.
Later, under the stimulation of tension on the periodontal ligament secondary or cellular cementum is further deposited. Especially near the apex of the root, where the cementum is thickest, cementocytes are embedded in the extracellular matrix. This cellular cementum exhibits lacunae and canaliculi, similar to bone.
The cementum lining the upper 1/3 of the roots usually remains much thinner, and without embedded cementocytes. Favorable circumstances of orientation, staining and illumination, often allow one to see that cementum has a lamellar structure basically comparable with bone.
On many teeth the layer of enamel extends down exactly to where the cementum starts. In a small percentage, the two tissues overlap or there is a tiny gap where the dentin is covered by neither.
Decalcified tooth:
Teeth are conventionally decalcified and so stained sections of teeth in their sockets is possible to view - and complement what you saw in the ground section.
The first thing to do is figure out the geometry of the teeth in the sections so that you will know the orientation of sections through the dentin. Observe the main anatomical landmarks of the tooth.
The crown is that part which is exposed above the gum (gingiva). The root (one or more) extends into the alveolarsocket. This is the hole in the alveolar bone of the jaw that each root of the tooth fits into. Each root is attached to the surrounding alveolar bone by a periodontal ligament.
Most of the substance of the tooth is dentin. This tissue is covered by a layer of enamel (missing) over the crown, and cementum over the root. As stated in an earlier item, the dentino-enamel junction, (DEJ) where the dentin contacts the enamel is an important landmark in the development, structure and pathology of the tooth. The enamel meets the cementum at the neck of the tooth. The pulp chamber occupies the center of the tooth, surrounded by dentin. It is filled with an uncalcified cellular, loose, connective tissue. This dental pulp extends down through the root canal to the apical foramen at the tip of the root. Blood vessels and nerves pass up through this foramen to supply the pulp.
Decalcified tooth - dentinal tubules (LS):
Remember, no enamel is left on these teeth, proof of the almost negligible amount of organic matrix material in that tissue. The empty space where the enamel had been is called the enamel space. In contrast, approximately 30% by weight of dentin is collagen. Each dentinal tubule will be preserved, coursing through the decalcified dentin. Examine them at high magnification in longitudinal and transverse section.
Look for the contour lines of Owen in this transverse section.
Decalcified tooth -Dentinal tubules (TS):
Remember, no enamel is left on these teeth, proof of the almost negligible amount of organic matrix material in that tissue. The empty space where the enamel had been is called the enamel space. In contrast, approximately 30% by weight of dentin is collagen. Each dentinal tubule is preserved, coursing through the decalcified dentin. Examine them at high magnification in longitudinal and transverse section and sectioned obilquely.
Look for the contour lines of Owen in this transverse section.
Decalcified tooth - Odontoblast:
Odontoblasts can continue to slowly deposit dentin even during adulthood, This very gradually reduces the pulp space and lengthens the dentinal tubules as the odontoblastic layer retreats.
Between mature (calcified) dentin and the layer of odontoblasts there is invariably a thin zone known as predentin. Its substance is more acidophilic than that of calcified dentin. Predentin is, in fact, precalcified dentinal matrix and as such, analogous to the osteoid layer found between osteoblasts and calcified bone.
The layer of odontoblasts within the pulp cavity should be examined with some care. These cells do not form a true epithelium, as also is the case for the sheets of osteoblasts which line the surfaces of bone. Neither of these sheets of cells has a basement membrane. Also, the cells are not really tightly lined up with each other, and while they do have junctional complexes, there can be extracellular material between individual cells. Nevertheless, the cells are crammed against one another and elongate just to pack in the vast number of cells.
Decalcified tooth - Pulp cavity:
Lined by odontoblasts, the pulp cavity is filled with a very loose, cellular connective tissue. Its blood vessels are unusually thin-walled for their size, as is feasible in this highly protected environment. As we all know only too well, nerves exist in pulp, but they are finely divided thin fibres and not easily seen except in special preparations.
Decalcified tooth - Cementum:
Turning to the outer surface of the root, can you find acellular and cellular cementum. Again, a thin layer of acellular cementum covers the entire root surface. At the ends of the root this layer is overlain by a thicker deposit of cellular cementum.
Decalcified tooth - Periodontal ligament:
The periodontal ligament attaching the tooth to the alveolar bone of the tooth socket is well seen. This ligament is much more cellular than most ligaments and very much more vascular. The ends of its collagen fibres are embedded in the alveolar bone and in the cementum as so-called Sharpey's fibers. Indeed, the function of cementum is to anchor the periodontal ligament to the tooth. You can see Sharpey's fibers entering into the alveolar bone and into the cementum of the tooth.
Developing Tooth:
Identify the enamel, dentin, ameloblasts and odontoblasts. The enamel at this early stage stains intensely because it contains a high concentration of protein. This is not the case with adult enamel. The tissues have shrunk considerably during fixation so all the white/clear spaces are artefact.
Developing Tooth - odontoblast:
Odontoblasts are in contact with the dentin they have produced. The odontoblasts form a closely packed sheet of cells.
Developing Tooth - Ameloblast:
The ameloblasts are truly epithelial. Just outside of the ameloblasts are other epithelial cells. These cells and the ameloblasts represent two epithelia joined top to top.
Gingiva:
Examine the free gingiva, the sulcular epithelium lining the sulcus, the space between the gingiva and the missing enamel, and the junctional epithelium, with its epithelial attachment. A little line of scum from the enamel lies between the sulcus and the enamel space. Now, follow the epithelium of the attached gingiva the other way and see that it becomes unkeratinized over the attached gingiva. In the early life of an erupted tooth, the gingival epithelium attaches to the enamel at the base of the crown region through the epithelial attachment. The apical surfaces of these cells adhere to the enamel above them. However, with time and a recession of the gums, the epithelium becomes attached to the cementum. Later in life not only the entire crown but even part of the root may be exposed with the attachment entirely to the cementum. This migration keeps the periodontists in business.